
Implementing a Transition Program from Paediatric to Adult Services in Phenylketonuria: Results after Two Years of Follow-Up with an Adult Team


 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Follow-Up Care Protocol for Patients with PKU
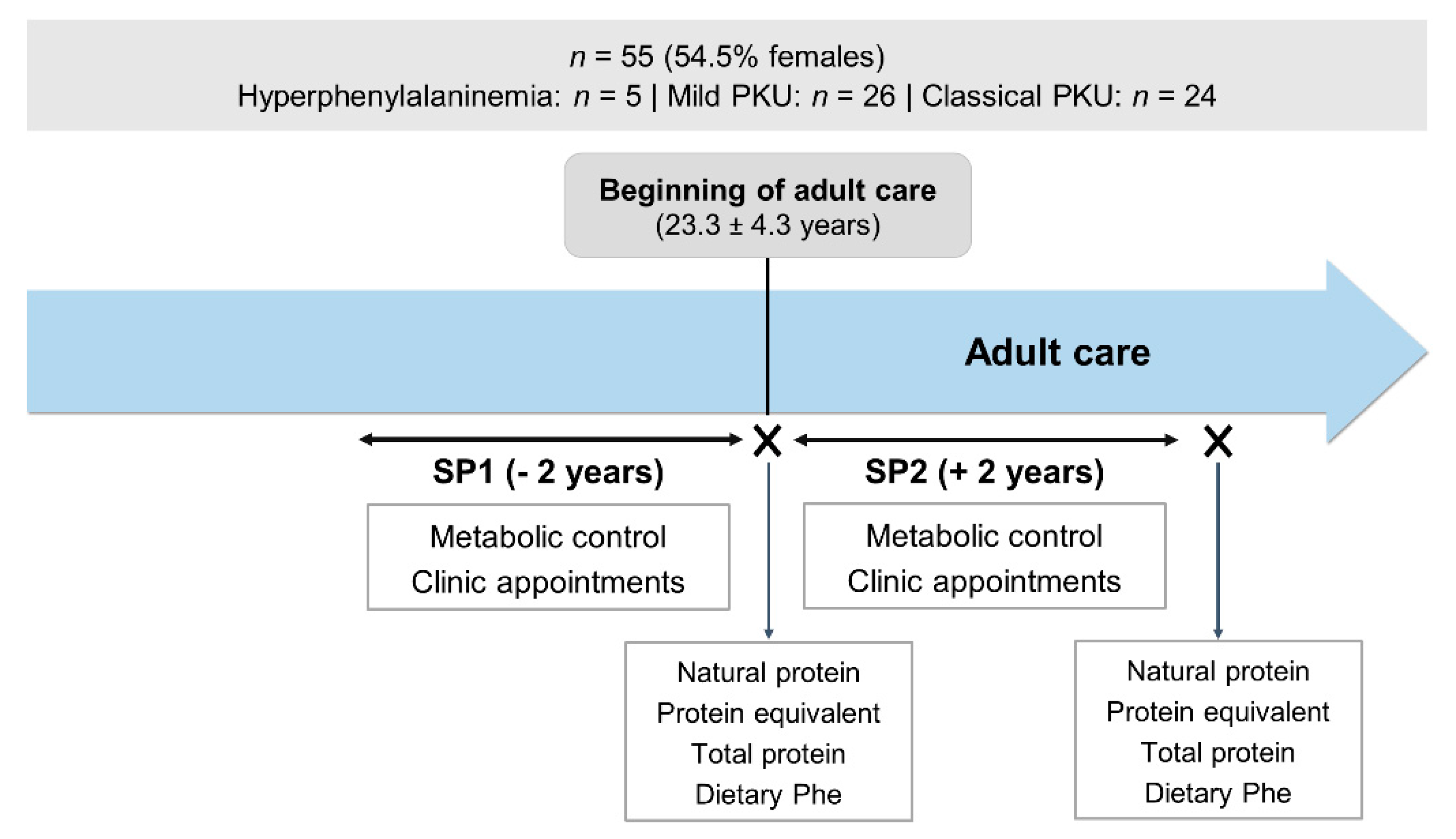
2.2. Participants
2.3. Study Design
2.4. Data Collection
2.4.1. Metabolic Control
2.4.2. Frequency of Clinic Appointments
2.4.3. Protein Intake
2.4.4. Ethical Statement
2.4.5. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Blood Phenylalanine Control
3.3. Follow-Up
3.4. Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blau, N.; van Spronsen, F.J.; Levy, H.L. Phenylketonuria. Lancet 2010, 376, 1417–1427. [Google Scholar] [CrossRef]
- Van Wegberg, A.M.J.; MacDonald, A.; Ahring, K.; Bélanger-Quintana, A.; Blau, N.; Bosch, A.M.; Burlina, A.; Campistol, J.; Feillet, F.; Giżewska, M.; et al. The complete European guidelines on phenylketonuria: Diagnosis and treatment. Orphanet J. Rare Dis. 2017, 12, 1–56. [Google Scholar]
- Vardy, E.; MacDonald, A.; Ford, S.; Hofman, D.L. Phenylketonuria, co-morbidity, and ageing: A review. J. Inherit. Metab. Dis. 2020, 43, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Bilder, D.A.; Kobori, J.A.; Cohen-Pfeffer, J.L.; Johnson, E.M.; Jurecki, E.R.; Grant, M.L. Neuropsychiatric comorbidities in adults with phenylketonuria: A retrospective cohort study. Mol. Genet. Metab. 2017, 121, 1–8. [Google Scholar] [CrossRef]
- Bilder, D.A.; Noel, J.K.; Baker, E.R.; Irish, W.; Chen, Y.; Merilainen, M.J.; Prasad, S.; Winslow, B.J. Systematic review and meta-analysis of neuropsychiatric symptoms and executive functioning in adults with phenylketonuria. Dev. Neuropsychol. 2016, 41, 245–260. [Google Scholar] [CrossRef]
- Burlina, A.P.; Lachmann, R.H.; Manara, R.; Cazzorla, C.; Celato, A.; van Spronsen, F.J.; Burlina, A. The neurological and psychological phenotype of adult patients with early-treated phenylketonuria: A systematic review. J. Inherit. Metab. Dis. 2019, 42, 209–219. [Google Scholar] [CrossRef]
- Burton, B.K.; Jones, K.B.; Cederbaum, S.; Rohr, F.; Waisbren, S.; Irwin, D.E.; Kim, G.; Lilienstein, J.; Alvarez, I.; Jurecki, E.; et al. Prevalence of comorbid conditions among adult patients diagnosed with phenylketonuria. Mol. Genet. Metab. 2018, 125, 228–234. [Google Scholar] [CrossRef]
- Enns, G.M.; Koch, R.; Brumm, V.; Blakely, E.; Suter, R.; Jurecki, E. Suboptimal outcomes in patients with PKU treated early with diet alone: Revisiting the evidence. Mol. Genet. Metab. 2010, 101, 99–109. [Google Scholar] [CrossRef]
- Trefz, K.F.; Muntau, A.C.; Kohlscheen, K.M.; Altevers, J.; Jacob, C.; Braun, S.; Greiner, W.; Jha, A.; Jain, M.; Alvarez, I.; et al. Clinical burden of illness in patients with phenylketonuria (PKU) and associated comorbidities—A retrospective study of German health insurance claims data. Orphanet J. Rare Dis. 2019, 14, 181. [Google Scholar] [CrossRef] [PubMed]
- Macleod, E.L.; Ney, D.M. Nutritional management of phenylketonuria. Ann. Nestle Eng. 2010, 68, 58–69. [Google Scholar] [CrossRef]
- Hoeks, M.P.; den Heijer, M.; Janssen, M.C. Adult issues in phenylketonuria. Neth. J. Med. 2009, 67, 2–7. [Google Scholar]
- Al Hafid, N.; Christodoulou, J. Phenylketonuria: A review of current and future treatments. Transl. Pediatr. 2015, 4, 304–317. [Google Scholar]
- Bilginsoy, C.; Waitzman, N.; Leonard, C.O.; Ernst, S.L. Living with phenylketonuria: Perspectives of patients and their families. J. Inherit. Metab. Dis. 2005, 28, 639–649. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; Gokmen-Ozel, H.; van Rijn, M.; Burgard, P. The reality of dietary compliance in the management of phenylketonuria. J. Inherit. Metab. Dis. 2010, 33, 665–670. [Google Scholar] [CrossRef]
- MacDonald, A.; van Rijn, M.; Feillet, F.; Lund, A.M.; Bernstein, L.; Bosch, A.M.; Gizewska, M.; van Spronsen, F.J. Adherence issues in inherited metabolic disorders treated by low natural protein diets. Ann. Nutr. Metab. 2012, 61, 289–295. [Google Scholar] [CrossRef]
- Walter, J.H.; White, F.J. Blood phenylalanine control in adolescents with phenylketonuria. Int. J. Adolesc. Med. Health 2004, 16, 41–45. [Google Scholar] [CrossRef]
- Ahring, K.; Bélanger-Quintana, A.; Dokoupil, K.; Gokmen-Ozel, H.; Lammardo, A.M.; MacDonald, A.; Motzfeldt, K.; Nowacka, M.; Robert, M.; van Rijn, M. Blood phenylalanine control in phenylketonuria: A survey of 10 European centres. Eur. J. Clin. Nutr. 2011, 65, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.H.; White, F.J.; Hall, S.K.; MacDonald, A.; Rylance, G.; Boneh, A.; Francis, D.E.; Shortland, G.J.; Schmidt, M.; Vail, A. How practical are recommendations for dietary control in phenylketonuria? Lancet 2002, 360, 55–57. [Google Scholar] [CrossRef]
- Trefz, F.K.; van Spronsen, F.J.; MacDonald, A.; Feillet, F.; Muntau, A.C.; Bélanger-Quintana, A.; Burlina, A.; Demirkol, M.; Giovannini, M.; Gasteyger, C. Management of adult patients with phenylketonuria: Survey results from 24 countries. Eur. J. Pediatr. 2015, 174, 119–127. [Google Scholar] [CrossRef]
- Jurecki, E.R.; Cederbaum, S.; Kopesky, J.; Perry, K.; Rohr, F.; Sanchez-Valle, A.; Viau, K.S.; Sheinin, M.Y.; Cohen-Pfeffer, J.L. Adherence to clinic recommendations among patients with phenylketonuria in the United States. Mol. Genet. Metab. 2017, 120, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.A.; Brown, C.; Grant, M.; Greene, C.L.; Jurecki, E.; Koch, J.; Moseley, K.; Suter, R.; van Calcar, S.C.; Wiles, J.; et al. Newborn screening 50 years later: Access issues faced by adults with PKU. Genet. Med. 2013, 15, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Suddaby, J.S.; Sohaei, D.; Bell, H.; Tavares, S.; Lee, G.J.; Szybowska, M.; So, J. Adult patient perspectives on phenylketonuria care: Highlighting the need for dedicated adult management and services. Eur. J. Med. Genet. 2020, 63, 103818. [Google Scholar] [CrossRef] [PubMed]
- Blau, N.; Bélanger-Quintana, A.; Demirkol, M.; Feillet, F.; Giovannini, M.; MacDonald, A.; Trefz, F.K.; van Spronsen, F. Management of phenylketonuria in Europe: Survey results from 19 countries. Mol. Genet. Metab. 2010, 99, 109–115. [Google Scholar] [CrossRef]
- Burton, B.K.; Leviton, L. Reaching out to the lost generation of adults with early-treated phenylketonuria (PKU). Mol. Genet. Metab. 2010, 101, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Chabrol, B.; Jacquin, P.; Francois, L.; Broué, P.; Dobbelaere, D.; Douillard, C.; Dubois, S.; Feillet, F.; Perrier, A.; Fouilhoux, A.; et al. Transition from pediatric to adult care in adolescents with hereditary metabolic diseases: Specific guidelines from the French network for rare inherited metabolic diseases (G2M). Arch. Pediatr. 2018, 25, 344–349. [Google Scholar] [CrossRef]
- Brumm, V.L.; Bilder, D.; Waisbren, S.E. Psychiatric symptoms and disorders in phenylketonuria. Mol. Genet. Metab. 2010, 99 (Suppl. 1), S59–S63. [Google Scholar] [CrossRef]
- Colver, A.; Rapley, T.; Parr, J.R.; McConachie, H.; Dovey-Pearce, G.; Couteur, A.L.; McDonagh, J.E.; Bennett, C.; Maniatopoulos, G.; Pearce, M.S.; et al. Facilitating transition of young people with long-term health conditions from children’s to adults’ healthcare services—Implications of a 5-year research programme. Clin. Med. (Lond.) 2020, 20, 74–80. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, A.; van Wegberg, A.M.J.; Ahring, K.; Beblo, S.; Bélanger-Quintana, A.; Burlina, A.; Campistol, J.; Coşkun, T.; Feillet, F.; Giżewska, M.; et al. PKU dietary handbook to accompany PKU guidelines. Orphanet J. Rare Dis. 2020, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; MacDonald, A. Treatment options and dietary supplements for patients with phenylketonuria. Expert Opin. Orphan Drugs 2018, 6, 667–681. [Google Scholar] [CrossRef]
- Mutze, U.; Roth, A.; Weigel, J.F.W.; Beblo, S.; Baerwald, C.G.; Buhrdel, P.; Kiess, W. Transition of young adults with phenylketonuria from pediatric to adult care. J. Inherit. Metab. Dis. 2011, 34, 701–709. [Google Scholar] [CrossRef]
- Mutze, U.; Thiele, A.G.; Baerwald, C.; Ceglarek, U.; Kiess, W.; Beblo, S. Ten years of specialized adult care for phenylketonuria—A single-centre experience. Orphanet J. Rare Dis. 2016, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Rocha, J.C.; Vilarinho, L.; Cabral, A.; Osório, R.V.; Almeida, M.F. Consensus for the nutritional treatment of phenylketonuria. Acta Pediatr. Port. 2007, 38, 44–54. [Google Scholar]
- Barbosa, C.S.; Almeida, M.F.; Sousa, C.; Rocha, S.; Guimas, A.; Ribeiro, R.; Martins, E.; Bandeira, A.; Oliveira, B.M.P.M.; Borges, N.; et al. Metabolic control in patients with phenylketonuria pre- and post-sapropterin loading test. J. Inborn Errors Metab. Screen 2018, 6, 1–6. [Google Scholar] [CrossRef]
- Cadario, F.; Prodam, F.; Bellone, S.; Trada, M.; Binotti, M.; Trada, M.; Allochis, G.; Baldelli, R.; Esposito, S.; Bona, G.; et al. Transition process of patients with type 1 diabetes (T1DM) from paediatric to the adult health care service: A hospital-based approach. Clin. Endocrinol. (Oxf.) 2009, 71, 346–350. [Google Scholar] [CrossRef]
- Martins, P.; Barreira, S.C.; Melo, A.T.; Campanilho-Marques, R.; Costa-Reis, P.; Fonseca, J.E.; Oliveira-Ramos, F. Transition in a paediatric rheumatology unit—experience from a tertiary unit. Acta Reumatol. Port. 2019, 44, 320–321. [Google Scholar]
- Smith, W.R.; Sisler, I.Y.; Johnson, S.; Lipato, T.J.; Newlin, J.S.; Owens, Z.S.; Morgan, A.M.; Treadwell, M.J.; Polak, K. Lessons learned from building a pediatric-to-adult sickle cell transition program. South. Med. J. 2019, 112, 190–197. [Google Scholar] [CrossRef]
- MacDonald, A.; Ahring, K.; Dokoupil, K.; Gokmen-Ozel, H.; Lammardo, A.M.; Motzfeldt, K.; Robert, M.; Rocha, J.C.; van Rijn, M.; Bélanger-Quintana, A. Adjusting diet with sapropterin in phenylketonuria: What factors should be considered? Br. J. Nutr. 2011, 106, 175–182. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brown, C.S.; Lichter-Konecki, U. Phenylketonuria (PKU): A problem solved? Mol. Genet. Metab. Rep. 2016, 6, 8–12. [Google Scholar] [CrossRef]
- Schulz, B.; Bremer, H.J. Nutrient intake and food consumption of adolescents and young adults with phenylketonuria. Acta Paediatr. 1995, 84, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Crowley, R.; Wolfe, I.; Lock, K.; McKee, M. Improving the transition between paediatric and adult healthcare: A systematic review. Arch. Dis. Child. 2011, 96, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D. Between two worlds: Bridging the cultures of child health and adult medicine. J. Adolesc. Health 1995, 17, 10–16. [Google Scholar] [CrossRef]
- Kemper, A.R.; Brewer, C.A.; Singh, R.H. Perspectives on dietary adherence among women with inborn errors of metabolism. J. Am. Diet. Assoc. 2010, 110, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Rutishauser, C.; Akré, C.; Surìs, J.-C. Transition from pediatric to adult health care: Expectations of adolescents with chronic disorders and their parents. Eur. J. Pediatr. 2011, 170, 865–871. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total (n = 55) | |
|---|---|---|
| Gender, n (%) | Female | 30 (54.5) |
| Male | 25 (45.5) | |
| Disease severity, n (%) | Hyperphenylalaninemia | 5 (9.1) |
| Mild PKU | 26 (47.3) | |
| Classical PKU | 24 (43.6) | |
| Age at the first appointment with an adult physician, years (mean ± SD (range)) | 23.3 ± 4.3 (18–33) | |
| Year of the first appointment with an adult physician, n (%) | 2011 | 1 (1.8) |
| 2012 | 9 (16.4) | |
| 2013 | 31 (56.4) | |
| 2014 | 11 (20.0) | |
| 2015 | 3 (5.5) | |
| BH4 loading test, n (%) | SP1 | 0 (0) |
| SP2 | 24 (43.6) | |
| SP1 (n = 52) | SP2 (n = 52) | p | |
|---|---|---|---|
| Annual number of blood spots, n | 11 (7–15) | 14 (7–20) | 0.002 |
| Median blood (Phe), µmol/L | 525 ± 248 | 552 ± 225 | 0.100 |
| (Phe) measurements < 480 µmol/L, % | 51 (4–96) | 37 (5–85) | 0.041 |
| SP1 (n = 52) | SP2 (n = 52) | p | |
|---|---|---|---|
| Attended appointments, n | |||
| Nutrition | 5 (3–6) | 7 (5–8) | <0.001 |
| Medical | 0 (0–1) | 4 (3–5) | <0.001 |
| Total | 5 (4–6) | 11 (8–13) | <0.001 |
| Missed appointments, n | |||
| Nutrition | 0 (0–1) | 0 (0–1) | 0.014 |
| Medical | 0 (0–0) | 0 (0–1) | 0.001 |
| Total | 0 (0–1) | 1 (0–2) | <0.001 |
| Entering Adult Care (n = 52) | After SP2 (n = 52) | p | |
|---|---|---|---|
| Natural protein, g/kg/day | 0.46 (0.35–0.88) | 0.46 (0.28–0.94) | 0.873 |
| Protein equivalent, g/kg/day | 0.85 (0.47–1.10) | 0.83 (0.43–1.05) | 0.066 |
| Total protein, g/kg/day | 1.51 (1.26–1.66) | 1.34 (1.07–1.54) | 0.194 |
| Phe, mg/day | 1210 (830–2311) | 1318 (763–2935) | 0.278 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peres, M.; Almeida, M.F.; Pinto, É.J.; Carmona, C.; Rocha, S.; Guimas, A.; Ribeiro, R.; Martins, E.; Bandeira, A.; MacDonald, A.; et al. Implementing a Transition Program from Paediatric to Adult Services in Phenylketonuria: Results after Two Years of Follow-Up with an Adult Team. Nutrients 2021, 13, 799. https://doi.org/10.3390/nu13030799
Peres M, Almeida MF, Pinto ÉJ, Carmona C, Rocha S, Guimas A, Ribeiro R, Martins E, Bandeira A, MacDonald A, et al. Implementing a Transition Program from Paediatric to Adult Services in Phenylketonuria: Results after Two Years of Follow-Up with an Adult Team. Nutrients. 2021; 13(3):799. https://doi.org/10.3390/nu13030799
Chicago/Turabian StylePeres, Maria, Manuela F. Almeida, Élia J. Pinto, Carla Carmona, Sara Rocha, Arlindo Guimas, Rosa Ribeiro, Esmeralda Martins, Anabela Bandeira, Anita MacDonald, and et al. 2021. "Implementing a Transition Program from Paediatric to Adult Services in Phenylketonuria: Results after Two Years of Follow-Up with an Adult Team" Nutrients 13, no. 3: 799. https://doi.org/10.3390/nu13030799
APA StylePeres, M., Almeida, M. F., Pinto, É. J., Carmona, C., Rocha, S., Guimas, A., Ribeiro, R., Martins, E., Bandeira, A., MacDonald, A., & Rocha, J. C. (2021). Implementing a Transition Program from Paediatric to Adult Services in Phenylketonuria: Results after Two Years of Follow-Up with an Adult Team. Nutrients, 13(3), 799. https://doi.org/10.3390/nu13030799