Hepatorenal Tyrosinaemia: Impact of a Simplified Diet on Metabolic Control and Clinical Outcome

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
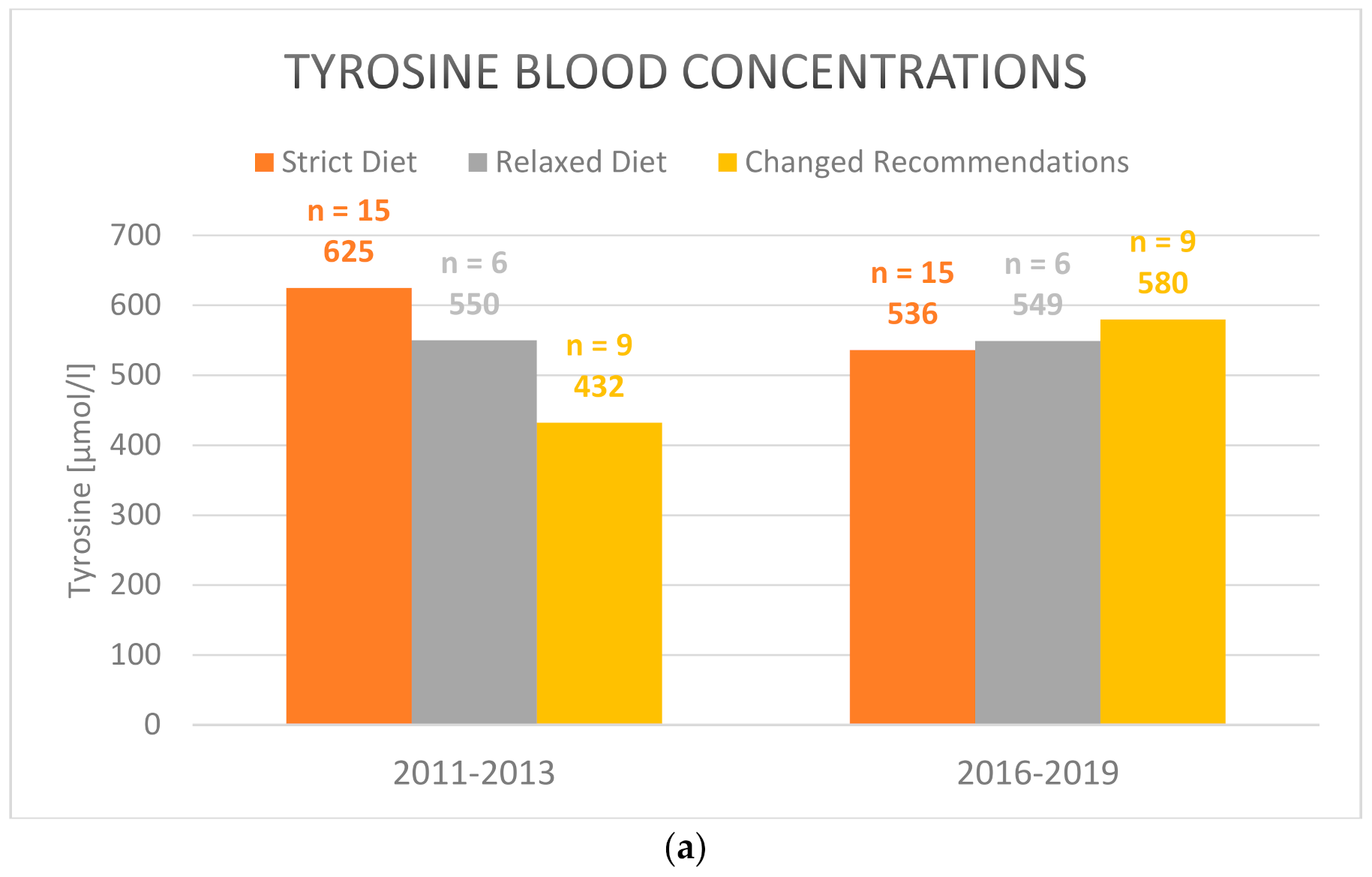
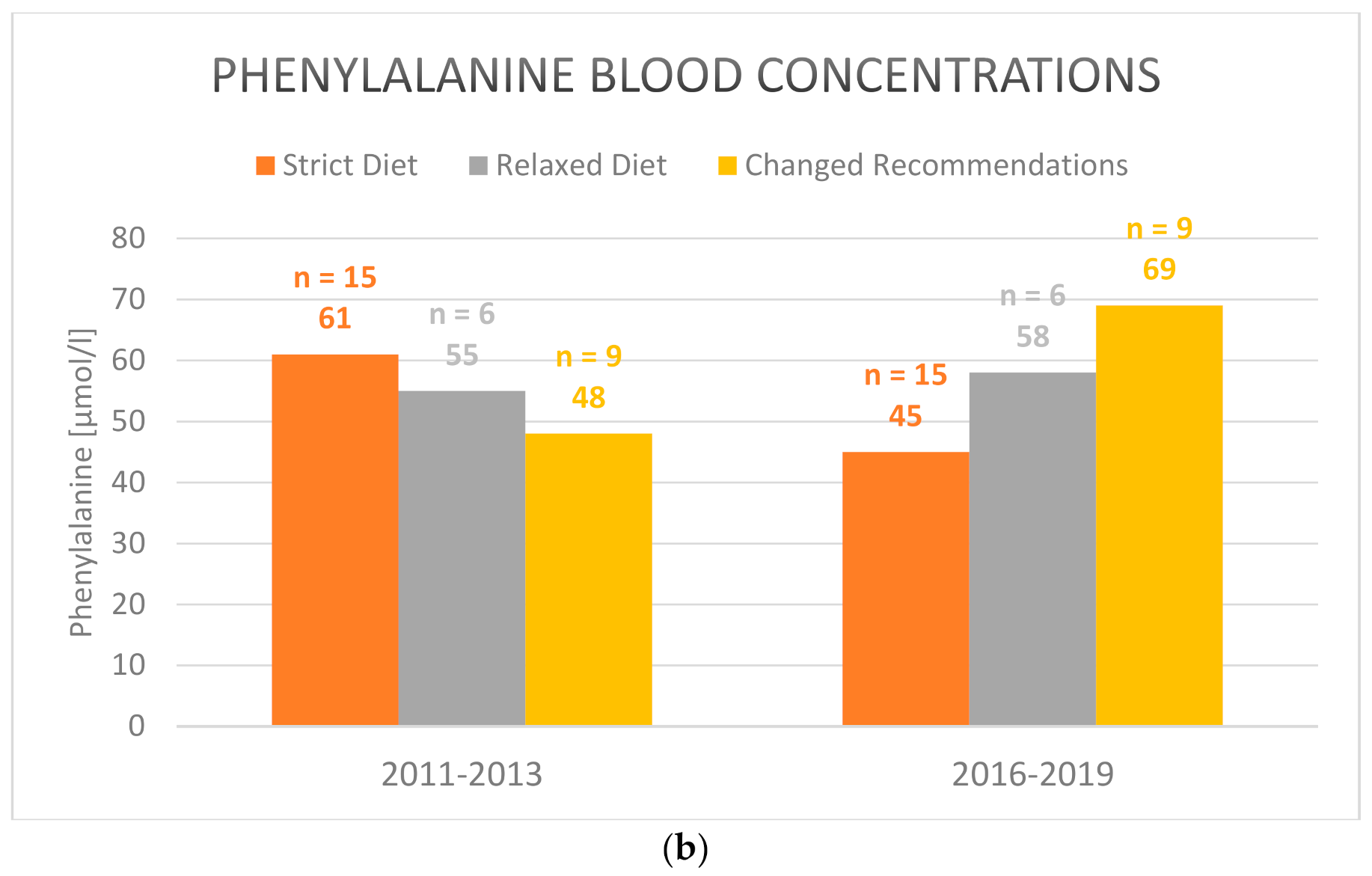
3.1. Dietary Recommendations and Target Parameters
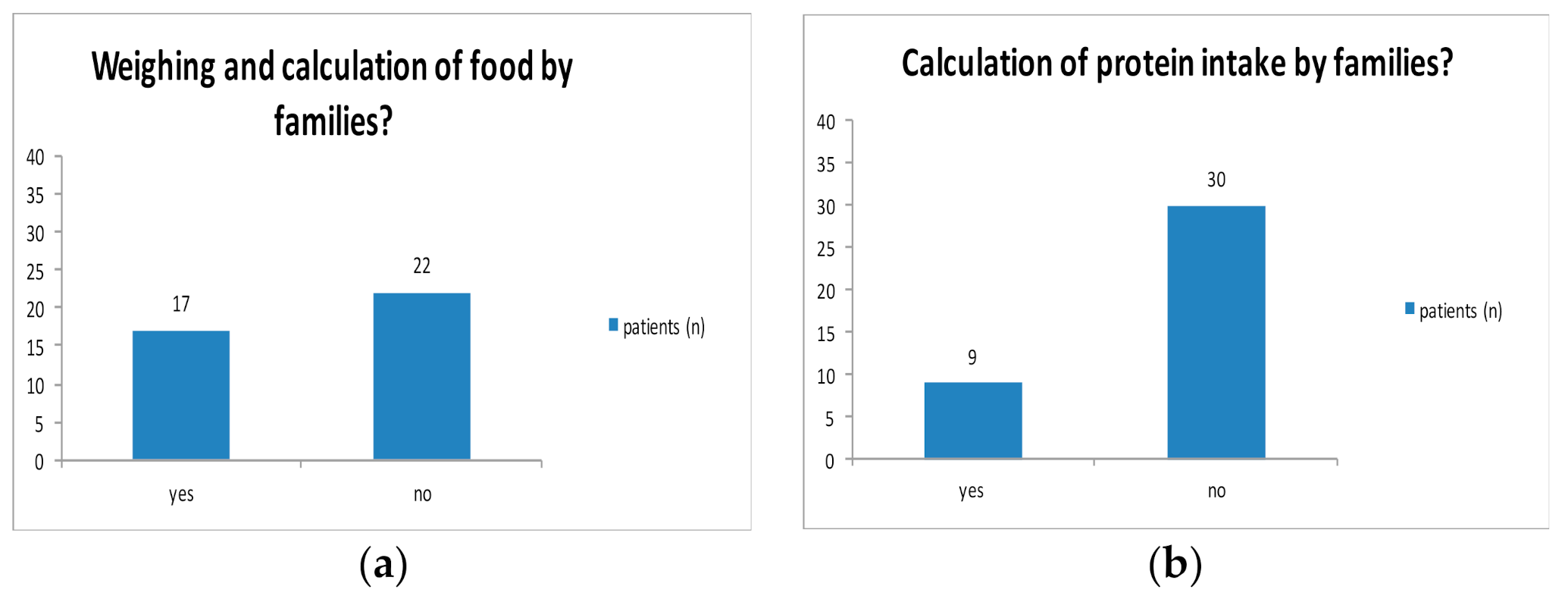
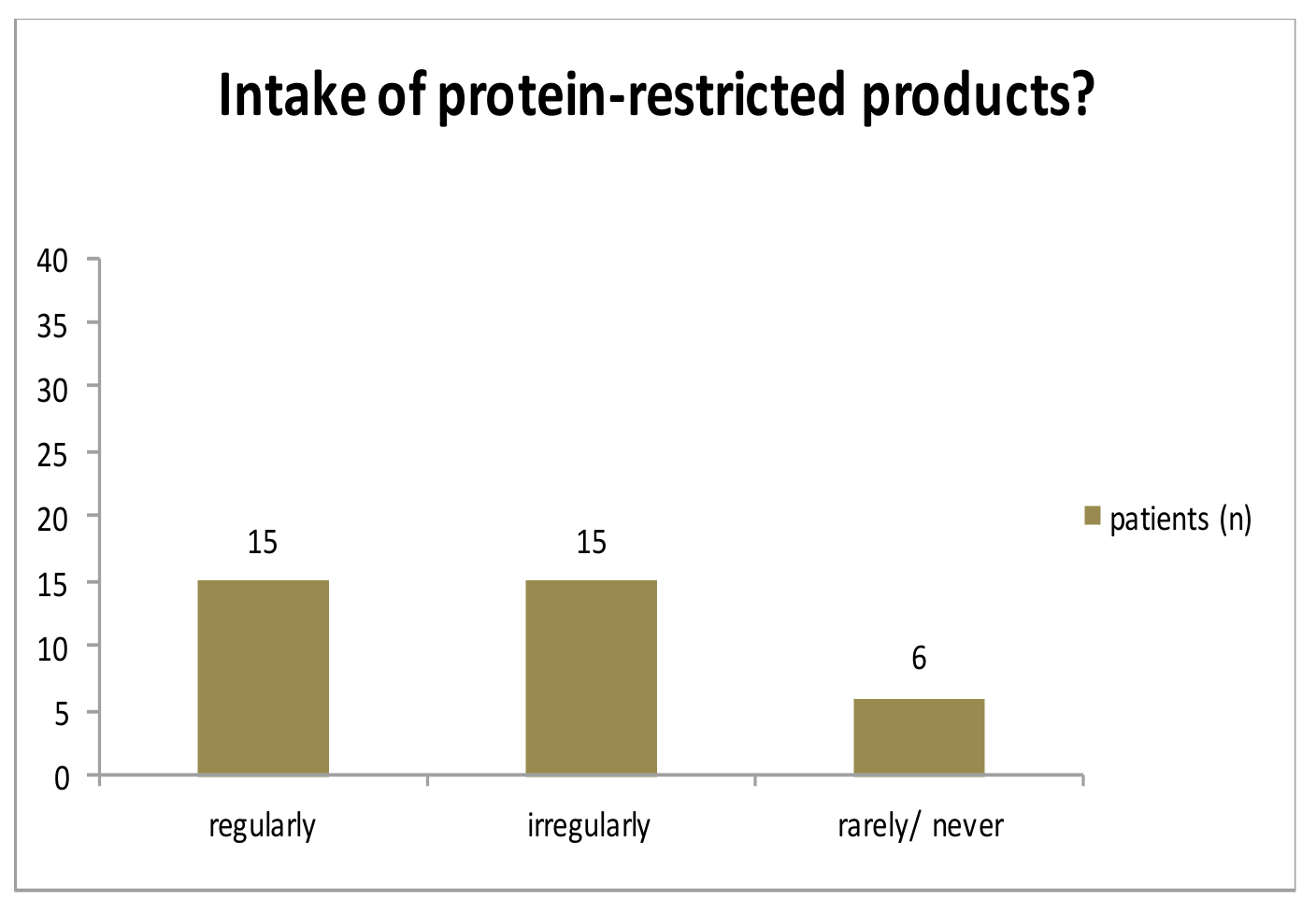
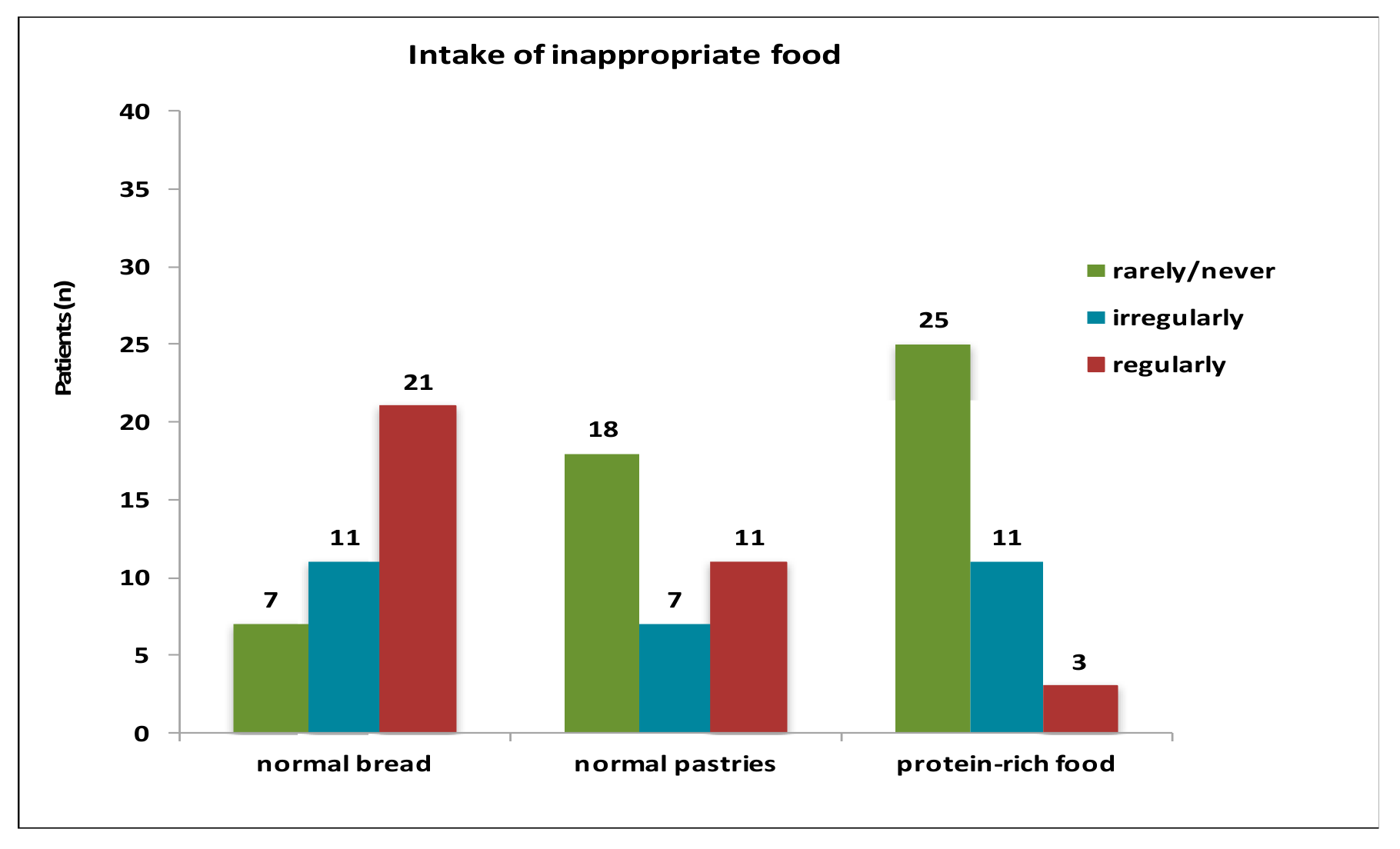
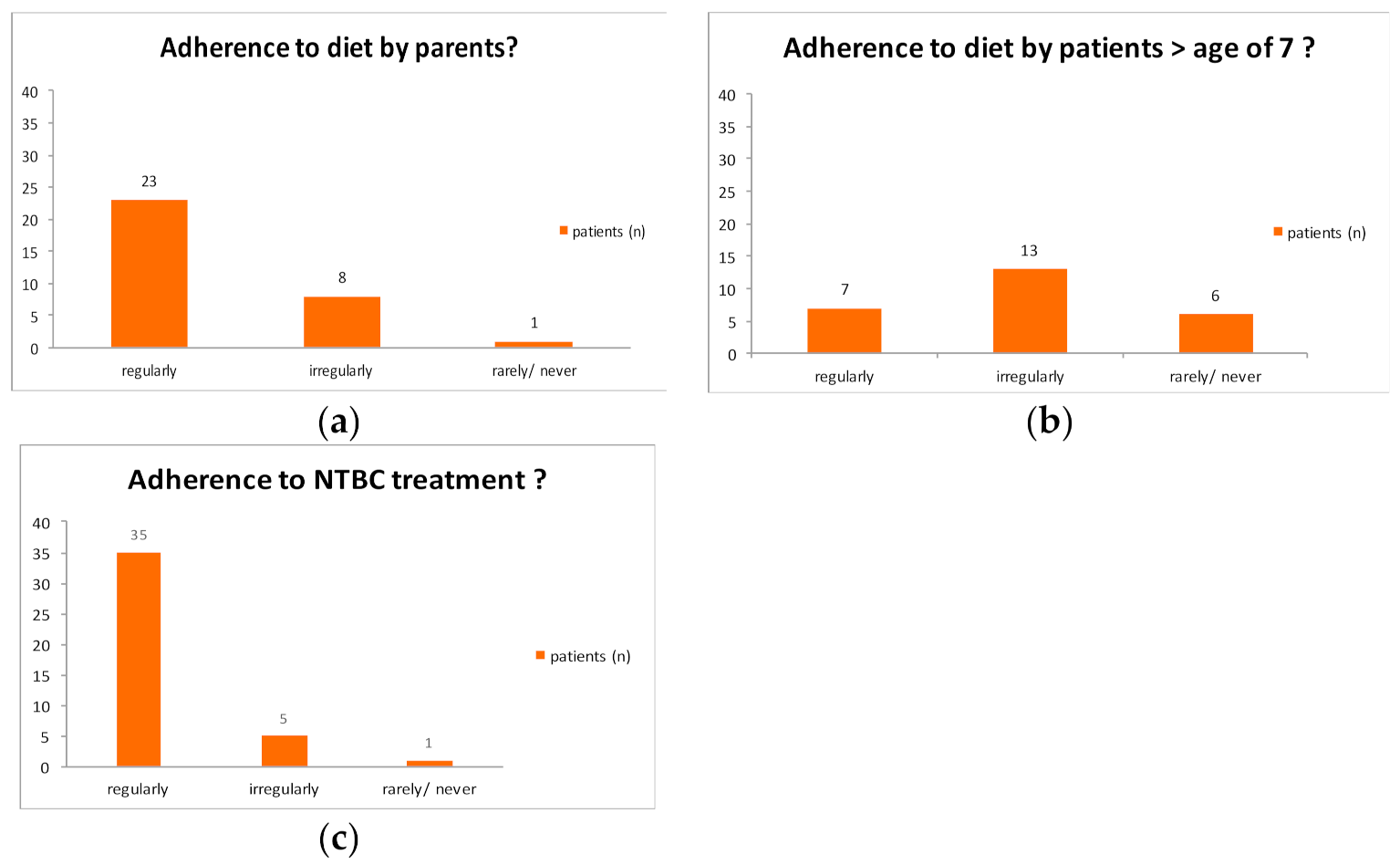
3.2. Medical Formula Intake and Compliance
3.3. Patient Data
Laboratory Findings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Interval | n | Mean Value +/− Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|
| 0–4 months | 11 | 0.84 +/− 0.44 | 0.2 | 1.8 |
| 4–12 months | 35 | 0.90 +/− 0.31 | 0.4 | 1.8 |
| 1–6 years | 30 | 0.76 +/− 0.23 | 0.3 | 1.2 |
| 6–14 years | 19 | 0.72 +/− 0.29 | 0.3 | 1.3 |
| >14 years | 5 | 0.33 +/− 0.11 | 0.2 | 0.5 |
| Age Interval | n | Mean Value +/− Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|
| 0–4 months | 11 | 1.1 +/− 0.27 | 0.8 | 1.7 |
| 4–12 months | 34 | 1.12 +/− 0.44 | 0.2 | 2.38 |
| 1–6 years | 31 | 1 +/− 0.37 | 0.55 | 2.5 |
| 6–14 years | 22 | 0.69 +/− 0.31 | 0.15 | 1.2 |
| >14 years | 7 | 0.45 +/− 0.25 | 0.13 | 0.8 |




References
- Morrow, G.; Tanguay, R.M. Biochemical and Clinical Aspects of Hereditary Tyrosinemia Type 1. Adv. Exp. Med. Biol. 2017, 959, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Lindblad, B.; Lindstedt, S.; Steen, G. On the enzymic defects in hereditary tyrosinemia. Proc. Natl. Acad. Sci. USA 1977, 74, 4641–4645. [Google Scholar] [CrossRef] [PubMed]
- Bendadi, F.; de Koning, T.J.; Visser, G.; Prinsen, H.C.M.T.; de Sain, M.G.M.; Verhoeven-Duif, N.; Sinnema, G.; van Spronsen, F.J.; van Hasselt, P.M. Impaired Cognitive Functioning in Patients with Tyrosinemia Type I Receiving Nitisinone. J. Pediatr. 2014, 164, 398–401. [Google Scholar] [CrossRef]
- van Ginkel, W.G.; Jahja, R.; Huijbregts, S.C.J.; Daly, A.; MacDonald, A.; De Laet, C.; Cassiman, D.; Eyskens, F.; Körver-Keularts, I.M.L.W.; Goyens, P.J.; et al. Neurocognitive outcome in tyrosinemia type 1 patients compared to healthy controls. Orphanet J. Rare Dis. 2016, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- García, M.I.; de la Parra, A.; Arias, C.; Arredondo, M.; Cabello, J.F. Long-term cognitive functioning in individuals with tyrosinemia type 1 treated with nitisinone and protein-restricted diet. Mol. Genet. Metab. Rep. 2017, 11, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Teckman, J.H.; Lueder, G.T. Corneal opacities associated with NTBC treatment. Am. J. Ophthalmol. 2002, 134, 266–268. [Google Scholar] [CrossRef]
- de Laet, C.; Dionisi-Vici, C.; Leonard, J.V.; McKiernan, P.; Mitchell, G.; Monti, L.; de Baulny, H.O.; Pintos-Morell, G.; Spiekerkötter, U. Recommendations for the management of tyrosinaemia type 1. Orphanet J. Rare Dis. 2013, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Chinsky, J.M.; Singh, R.; Ficicioglu, C.; van Karnebeek, C.D.M.; Grompe, M.; Mitchell, G.; Waisbren, S.E.; Gucsavas-Calikoglu, M.; Wasserstein, M.P.; Coakley, K.; et al. Diagnosis and treatment of tyrosinemia type I: A US and Canadian consensus group review and recommendations. Genet. Med. 2017, 19, 1380. [Google Scholar] [CrossRef] [PubMed]
- Mayorandan, S.; Meyer, U.; Gokcay, G.; Segarra, N.G.; de Baulny, H.O.; van Spronsen, F.; Zeman, J.; de Laet, C.; Spiekerkoetter, U.; Thimm, E.; et al. Cross-sectional study of 168 patients with hepatorenal tyrosinaemia and implications for clinical practice. Orphanet J. Rare Dis. 2014, 9, 107. [Google Scholar] [CrossRef] [PubMed]
- van Ginkel, W.G.; van Vliet, D.; Burgerhof, J.G.M.; de Blaauw, P.; Rubio Gozalbo, M.E.; Heiner-Fokkema, M.R.; van Spronsen, F.J. Presumptive brain influx of large neutral amino acids and the effect of phenylalanine supplementation in patients with Tyrosinemia type 1. PLoS ONE 2017, 12, e0185342. [Google Scholar] [CrossRef] [PubMed]
- French-Belgian Study Group for HT-1; Schiff, M.; Broue, P.; Chabrol, B.; De Laet, C.; Habes, D.; Mention, K.; Sarles, J.; Spraul, A.; Valayannopoulos, V.; et al. Heterogeneity of follow-up procedures in French and Belgian patients with treated hereditary tyrosinemia type 1: Results of a questionnaire and proposed guidelines. J. Inherit. Metab. Dis. 2012, 35, 823–829. [Google Scholar] [CrossRef]
- Kienstra, N.S.; van Reemst, H.E.; van Ginkel, W.G.; Daly, A.; van Dam, E.; MacDonald, A.; Burgerhof, J.G.M.; de Blaauw, P.; McKiernan, P.J.; Heiner-Fokkema, M.R.; et al. Daily variation of NTBC and its relation to succinylacetone in tyrosinemia type 1 patients comparing a single dose to two doses a day. J. Inherit. Metab. Dis. 2018, 41, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Schlune, A.; Thimm, E.; Herebian, D.; Spiekerkoetter, U. Single dose NTBC-treatment of hereditary tyrosinemia type I. J. Inherit. Metab. Dis. 2012, 35, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, O.; Daly, A.; Pinto, A.; Ashmore, C.; Evans, S.; Gupte, G.; Santra, S.; Preece, M.A.; Mckiernan, P.; Kitchen, S.; et al. Natural Protein Tolerance and Metabolic Control in Patients with Hereditary Tyrosinaemia Type 1. Nutrients 2020, 12, 1148. [Google Scholar] [CrossRef] [PubMed]


| Unrestricted (Low Protein) | Occasional Consumption Possible (Moderate Protein) | Inappropriate (Protein Rich) |
|---|---|---|
| Fruits, vegetables, potatoes, rice, butter, oil, cream, crème fraiche, sour cream, sugar, sweets, rice/oat drink, special low-protein products | High-fat dairy products (e.g., cream cheese), normal bread, pasta, pastries, nuts, legumes, eggs processed in food | Meat, sausages, eggs, poultry, fish, sea food |
| Center | Protein/Tyrosine Calculation before 2013 | Protein/Tyrosine Calculation after 2013 | Diet before 2013 | Diet after 2013 | Tyr Target values | Phe Target Values |
|---|---|---|---|---|---|---|
| 1 | both | both | strict | strict | <500 | normal |
| 2 | both | both | strict | strict | <400 | <40 |
| 3 | no data 1 | no calculation | no data 1 | strict | <400 | 50 |
| 4 | protein only | protein only | strict | strict | <500 | normal |
| 5 | protein only | no calculation | strict | simplified | <400 | >50 |
| 6 | no calculation | no calculation | strict | simplified | <400 | >30 |
| 7 | tyrosine only | tyrosine only | simplified | simplified | <400 | normal |
| 8 | tyrosine only | tyrosine only | simplified | simplified | <400 | 20–80 |
| 9 | protein only | protein only | simplified | simplified | <800 | 30–80 |
| Center | Number of Patients | Mean Age (std. dev.) | Tyr 2011–2013 | Tyr 2016–2019 | Phe 2011–2013 | Phe 2016–2019 | Diet after 2013 |
|---|---|---|---|---|---|---|---|
| 1 | 9 | 14.3 (+/−6.9) | 645.6 | 599.4 | 58.9 | 54.7 | strict |
| 2 | 10 | 7.2 (+/−5.3) | 555.6 | 447.2 | 42.9 | 35.5 | strict |
| 3 | 3 | 21.3 (+/−4.9) | 680.5 | 640.2 | 42.0 | 45.5 | strict |
| 4 | 2 | 27.5 (+/−5) | 522.8 | 722.1 | 57.7 | 46.1 | strict |
| 5 | 5 | 12.1 (+/−4.3) | 426.7 | 649.1 | 61.9 | 111.2 | simplified |
| 6 | 6 | 13.8 (+/−6.6) | 391.6 | 475.6 | 32.9 | 40.1 | simplified |
| 7 | 5 | 16.7 (+/−6.1) | 523.9 | 542.9 | 60.7 | 64.4 | simplified |
| 8 | 2 | 7.5 (+/−0.7) | - 1 | 463.8 | - 1 | 30.5 | simplified |
| 9 | 2 | 22 (+/−1.4) | 601.4 | 647.5 | 44.0 | 51.8 | simplified |
| total | 44 2 | 13.8 (+/−7.4) | 552.1 | 551.0 | 51.1 | 54.5 |
| Dietary Recommendations | Number of Patients | Tyr 2016–2019 | Phe 2016–2019 |
|---|---|---|---|
| strict diet | 24 | 551 | 44.8 |
| simplified diet | 20 | 552 | 65.5 |
| p | 0.995 | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bärhold, F.; Meyer, U.; Neugebauer, A.-K.; Thimm, E.M.; Lier, D.; Rosenbaum-Fabian, S.; Och, U.; Fekete, A.; Möslinger, D.; Rohde, C.; et al. Hepatorenal Tyrosinaemia: Impact of a Simplified Diet on Metabolic Control and Clinical Outcome. Nutrients 2021, 13, 134. https://doi.org/10.3390/nu13010134
Bärhold F, Meyer U, Neugebauer A-K, Thimm EM, Lier D, Rosenbaum-Fabian S, Och U, Fekete A, Möslinger D, Rohde C, et al. Hepatorenal Tyrosinaemia: Impact of a Simplified Diet on Metabolic Control and Clinical Outcome. Nutrients. 2021; 13(1):134. https://doi.org/10.3390/nu13010134
Chicago/Turabian StyleBärhold, Friederike, Uta Meyer, Anne-Kathrin Neugebauer, Eva Maria Thimm, Dinah Lier, Stefanie Rosenbaum-Fabian, Ulrike Och, Anna Fekete, Dorothea Möslinger, Carmen Rohde, and et al. 2021. "Hepatorenal Tyrosinaemia: Impact of a Simplified Diet on Metabolic Control and Clinical Outcome" Nutrients 13, no. 1: 134. https://doi.org/10.3390/nu13010134
APA StyleBärhold, F., Meyer, U., Neugebauer, A.-K., Thimm, E. M., Lier, D., Rosenbaum-Fabian, S., Och, U., Fekete, A., Möslinger, D., Rohde, C., Beblo, S., Hochuli, M., Bogovic, N., Korpel, V., vom Dahl, S., Mayorandan, S., Fischer, A., Freisinger, P., Dokoupil, K., ... Das, A. M. (2021). Hepatorenal Tyrosinaemia: Impact of a Simplified Diet on Metabolic Control and Clinical Outcome. Nutrients, 13(1), 134. https://doi.org/10.3390/nu13010134