
Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population
2.3. Experimental Interventions
- Blended intervention for additional home-based exercise
- 2.
- Dietary protein counselling incorporating e-health/tele-health
2.4. Dietary Behavior Change and Design Considerations
2.5. Dietary Assessment
2.6. Ethics
2.7. Statistics
3. Results
3.1. Study Participants
3.2. Digitally Supported Counselling—Coaching Contacts
3.3. Effectiveness of the Dietary Protein Counselling
3.3.1. Macronutrients
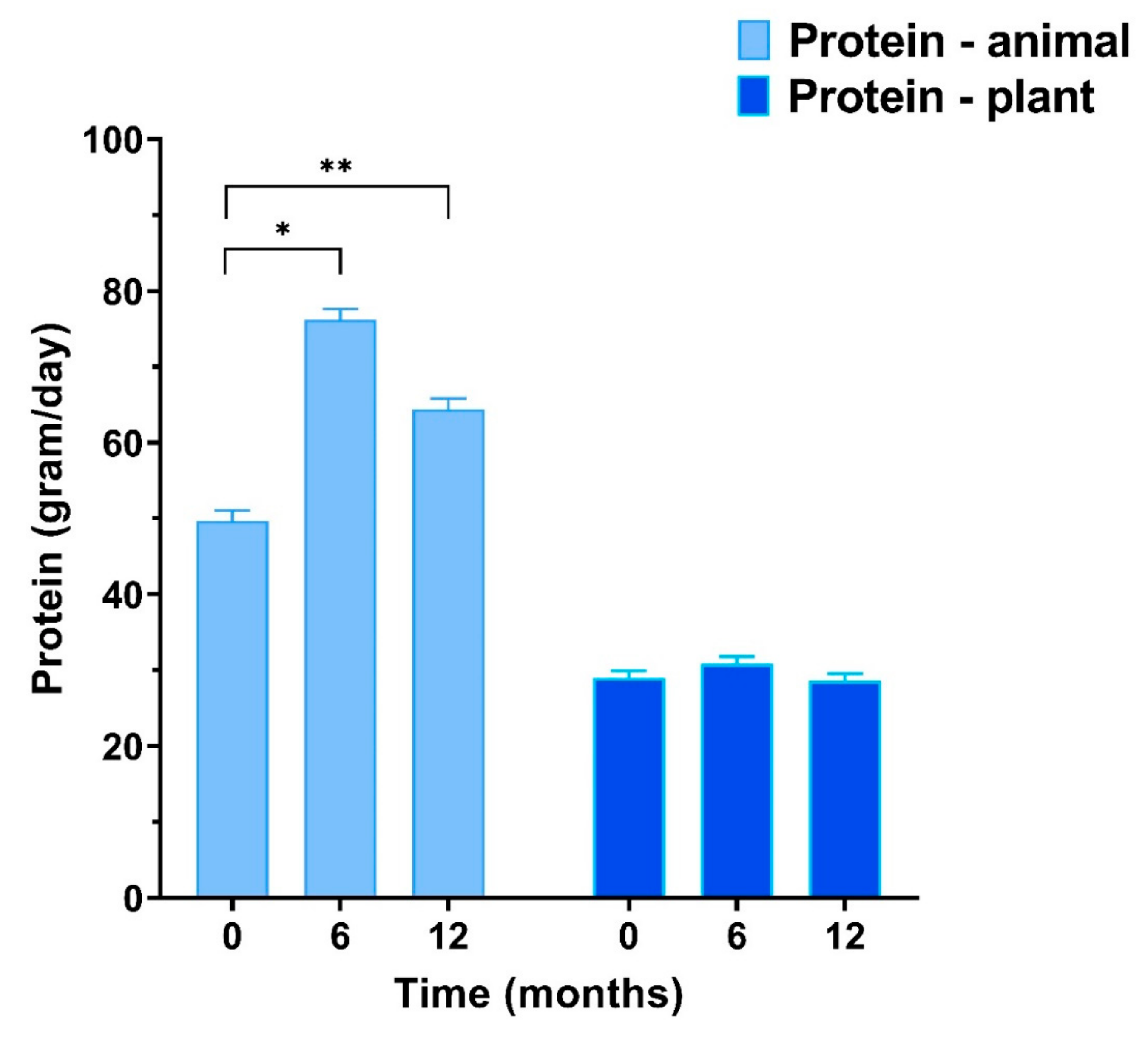
3.3.2. Protein Sources
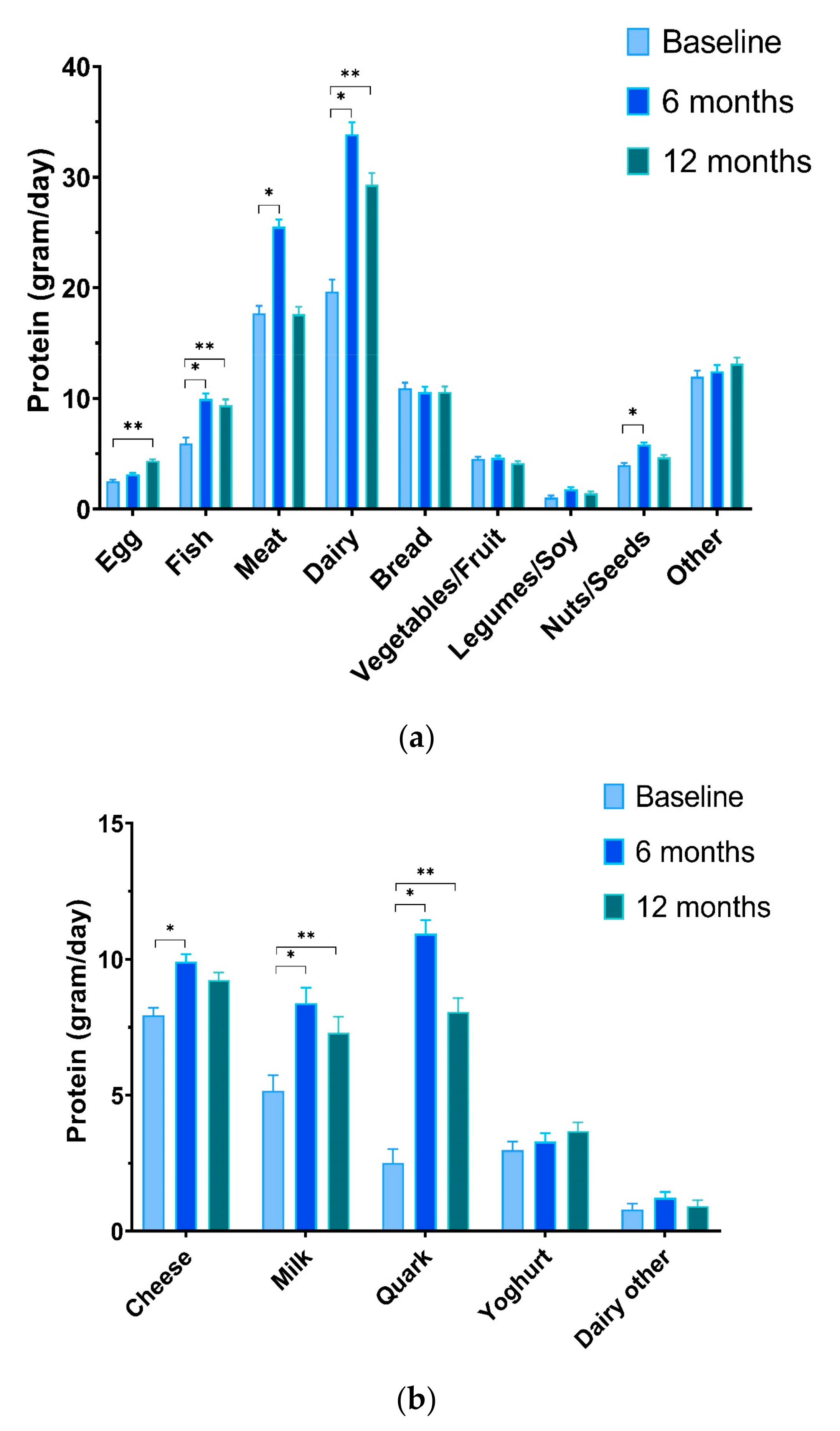
3.3.3. Product Groups
3.3.4. Intake of Amino Acids
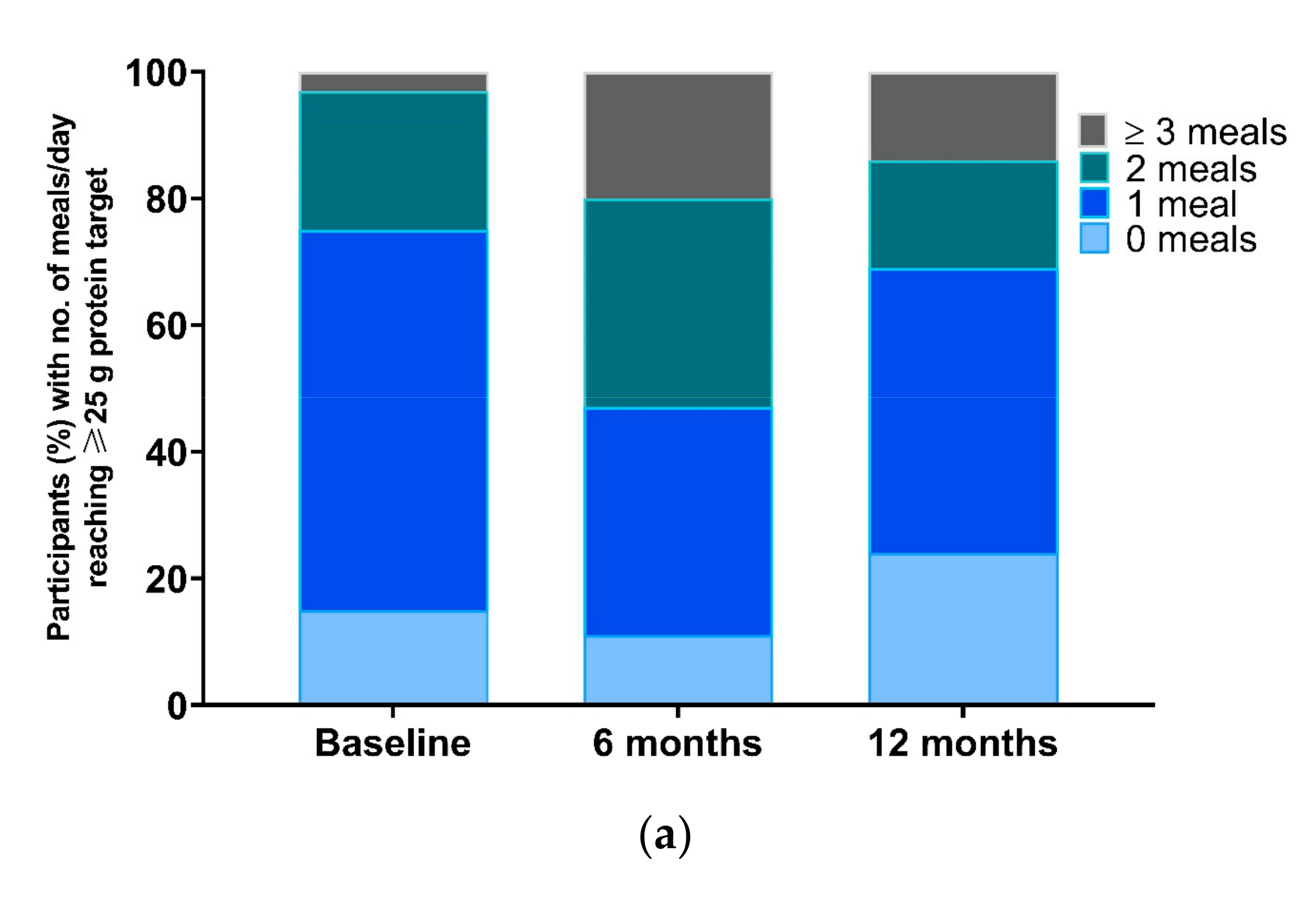
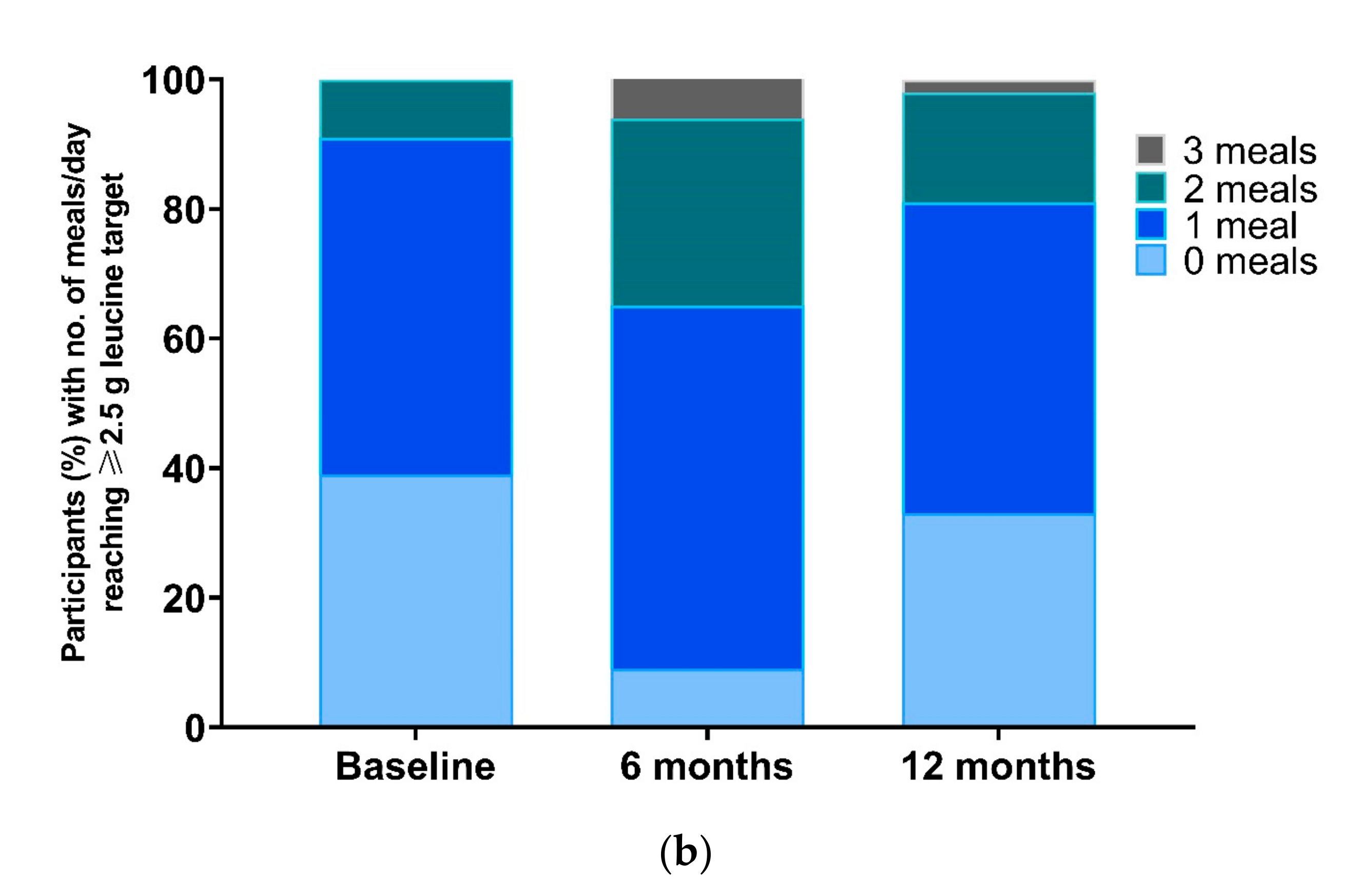
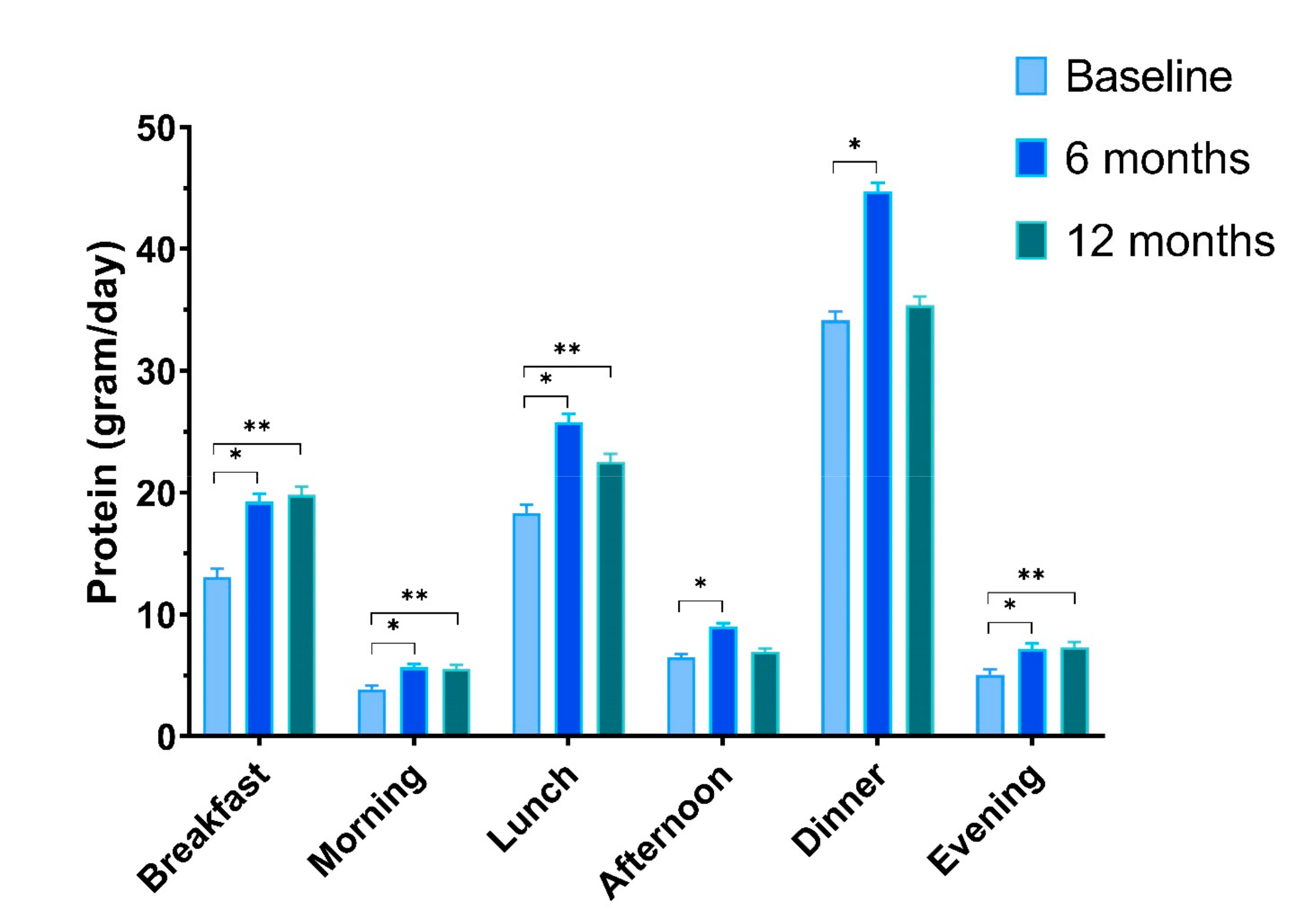
3.3.5. Protein Intake at Different Eating Occasions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beaudart, C.; Dawson, A.; Shaw, S.C.; Harvey, N.C.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; Bruyere, O.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef]
- Cermak, N.M.; Res, P.T.; de Groot, L.C.; Saris, W.H.; van Loon, L.J. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: A meta-analysis. Am. J. Clin. Nutr. 2012, 96, 1454–1464. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P.; The, I.S.G. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 119. [Google Scholar] [CrossRef]
- Wong, S.Y.; Lau, E.M.; Lau, W.W.; Lynn, H.S. Is dietary counselling effective in increasing dietary calcium, protein and energy intake in patients with osteoporotic fractures? A randomized controlled clinical trial. J. Hum. Nutr. Diet. 2004, 17, 359–364. [Google Scholar] [CrossRef]
- Nykänen, I.; Rissanen, T.H.; Sulkava, R.; Hartikainen, S. Effects of individual dietary counseling as part of a comprehensive geriatric assessment (CGA) on nutritional status: A population-based intervention study. J. Nutr. Health Aging 2014, 18, 54–58. [Google Scholar] [CrossRef]
- Ahn, J.A.; Park, J.; Kim, C.J. Effects of an individualised nutritional education and support programme on dietary habits, nutritional knowledge and nutritional status of older adults living alone. J. Clin. Nurs. 2018, 27, 2142–2151. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro-Grillo, I.; Vidal, P.M.; Camilo, M.E. Dietary counseling improves patient outcomes: A prospective, randomized, controlled trial in colorectal cancer patients undergoing radiotherapy. J. Clin. Oncol. 2005, 23, 1431–1438. [Google Scholar] [CrossRef]
- Marx, W.; Kelly, J.T.; Crichton, M.; Craven, D.; Collins, J.; Mackay, H.; Isenring, E.; Marshall, S. Is telehealth effective in managing malnutrition in community-dwelling older adults? A systematic review and meta-analysis. Maturitas 2018, 111, 31–46. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, A.L.; Robinson, S.M.; Sayer, A.A.; Roberts, H.C. An overview of appetite decline in older people. Nurs. Older People 2015, 27, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Berrazaga, I.; Micard, V.; Gueugneau, M.; Walrand, S. The Role of the Anabolic Properties of Plant- versus Animal-Based Protein Sources in Supporting Muscle Mass Maintenance: A Critical Review. Nutrients 2019, 11, 1825. [Google Scholar] [CrossRef]
- Wolfe, R.R.; Baum, J.I.; Starck, C.; Moughan, P.J. Factors contributing to the selection of dietary protein food sources. Clin. Nutr. 2018, 37, 130–138. [Google Scholar] [CrossRef]
- van den Helder, J.; van Dronkelaar, C.; Tieland, M.; Mehra, S.; Dadema, T.; Visser, B.; Krose, B.J.A.; Engelbert, R.H.H.; Weijs, P.J.M. A digitally supported home-based exercise training program and dietary protein intervention for community dwelling older adults: Protocol of the cluster randomised controlled VITAMIN trial. BMC Geriatr. 2018, 18, 183. [Google Scholar] [CrossRef]
- Mehra, S.; Visser, B.; Dadema, T.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Krose, B.J. Translating Behavior Change Principles Into a Blended Exercise Intervention for Older Adults: Design Study. JMIR Res. Protoc. 2018, 7, e117. [Google Scholar] [CrossRef]
- Mehra, S.; Visser, B.; Cila, N.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Krose, B.J. Supporting Older Adults in Exercising With a Tablet: A Usability Study. JMIR Hum. Factors 2019, 6, e11598. [Google Scholar] [CrossRef]
- van den Helder, J.; Mehra, S.; van Dronkelaar, C.; Ter-Riet, G.; Tieland, M.; Visser, B.; Krose, B.J.A.; Engelbert, R.H.H.; Weijs, P.J.M. Blended home-based exercise and dietary protein in community-dwelling older adults: A cluster randomized controlled trial. J. Cachexia Sarcopenia Muscle 2020, 11. [Google Scholar] [CrossRef]
- Kromhout, D.; Spaaij, C.J.; de Goede, J.; Weggemans, R.M. The 2015 Dutch food-based dietary guidelines. Eur. J. Clin. Nutr. 2016, 70, 869–878. [Google Scholar] [CrossRef]
- Twisk, J.; Bosman, L.; Hoekstra, T.; Rijnhart, J.; Welten, M.; Heymans, M. Different ways to estimate treatment effects in randomised controlled trials. Contemp. Clin. Trials Commun. 2018, 10, 80–85. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Hanach, N.I.; McCullough, F.; Avery, A. The Impact of Dairy Protein Intake on Muscle Mass, Muscle Strength, and Physical Performance in Middle-Aged to Older Adults with or without Existing Sarcopenia: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef]
- Symons, T.B.; Sheffield-Moore, M.; Wolfe, R.R.; Paddon-Jones, D. A moderate serving of high-quality protein maximally stimulates skeletal muscle protein synthesis in young and elderly subjects. J. Am. Diet. Assoc. 2009, 109, 1582–1586. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Mamerow, M.M.; Mettler, J.A.; English, K.L.; Casperson, S.L.; Arentson-Lantz, E.; Sheffield-Moore, M.; Layman, D.K.; Paddon-Jones, D. Dietary protein distribution positively influences 24-h muscle protein synthesis in healthy adults. J. Nutr. 2014, 144, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M. The impact of protein quality on the promotion of resistance exercise-induced changes in muscle mass. Nutr. Metab. 2016, 13, 64. [Google Scholar] [CrossRef]
- Munk, T.; Tolstrup, U.; Beck, A.M.; Holst, M.; Rasmussen, H.H.; Hovhannisyan, K.; Thomsen, T. Individualised dietary counselling for nutritionally at-risk older patients following discharge from acute hospital to home: A systematic review and meta-analysis. J. Hum. Nutr. Diet. 2016, 29, 196–208. [Google Scholar] [CrossRef]
- Pölönen, S.; Tiihonen, M.; Hartikainen, S.; Nykänen, I. Individually Tailored Dietary Counseling among Old Home Care Clients - Effects on Nutritional Status. J. Nutr. Health Aging 2017, 21, 567–572. [Google Scholar] [CrossRef]
- Berendsen, A.A.M.; van de Rest, O.; Feskens, E.J.M.; Santoro, A.; Ostan, R.; Pietruszka, B.; Brzozowska, A.; Stelmaszczyk-Kusz, A.; Jennings, A.; Gillings, R.; et al. Changes in Dietary Intake and Adherence to the NU-AGE Diet Following a One-Year Dietary Intervention among European Older Adults-Results of the NU-AGE Randomized Trial. Nutrients 2018, 10, 1905. [Google Scholar] [CrossRef] [PubMed]
- van Doorn-van Atten, M.N.; Haveman-Nies, A.; van Bakel, M.M.; Ferry, M.; Franco, M.; de Groot, L.; de Vries, J.H.M. Effects of a multi-component nutritional telemonitoring intervention on nutritional status, diet quality, physical functioning and quality of life of community-dwelling older adults. Br. J. Nutr. 2018, 119, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, E.J.I.; Haveman-Nies, A.; Doets, E.L.; Dorhout, B.G.; de Groot, L. Effectiveness of a Diet and Resistance Exercise Intervention on Muscle Health in Older Adults: ProMuscle in Practice. J. Am. Med. Dir. Assoc. 2020, 21, 1065–1072.e1063. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.T.; Reidlinger, D.P.; Hoffmann, T.C.; Campbell, K.L. Telehealth methods to deliver dietary interventions in adults with chronic disease: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 104, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Krebs, P.; Shtaynberger, J.; McCabe, M.; Iocolano, M.; Williams, K.; Shuk, E.; Ostroff, J.S. An eHealth Intervention to Increase Physical Activity and Healthy Eating in Older Adult Cancer Survivors: Summative Evaluation Results. JMIR Cancer 2017, 3, e4. [Google Scholar] [CrossRef]
- Kiss, N.; Baguley, B.J.; Ball, K.; Daly, R.M.; Fraser, S.F.; Granger, C.L.; Ugalde, A. Technology-Supported Self-Guided Nutrition and Physical Activity Interventions for Adults With Cancer: Systematic Review. JMIR Mhealth Uhealth 2019, 7, e12281. [Google Scholar] [CrossRef]
- Muller, A.M.; Maher, C.A.; Vandelanotte, C.; Hingle, M.; Middelweerd, A.; Lopez, M.L.; de Smet, A.; Short, C.E.; Nathan, N.; Hutchesson, M.J.; et al. Physical Activity, Sedentary Behavior, and Diet-Related eHealth and mHealth Research: Bibliometric Analysis. J. Med. Internet Res. 2018, 20, e122. [Google Scholar] [CrossRef]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational Interviewing and Self–Determination Theory. J. Soc. Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Carrera, P.M.; Dalton, A.R. Do-it-yourself healthcare: The current landscape, prospects and consequences. Maturitas 2014, 77, 37–40. [Google Scholar] [CrossRef]
- Rollo, M.E.; Burrows, T.; Vincze, L.J.; Harvey, J.; Collins, C.E.; Hutchesson, M.J. Cost evaluation of providing evidence-based dietetic services for weight management in adults: In-person versus eHealth delivery. Nutr. Diet. 2018, 75, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Cradock, K.A.; ÓLaighin, G.; Finucane, F.M.; Gainforth, H.L.; Quinlan, L.R.; Ginis, K.A. Behaviour change techniques targeting both diet and physical activity in type 2 diabetes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef] [PubMed]
- van Rinsum, C.; Gerards, S.; Rutten, G.; Philippens, N.; Janssen, E.; Winkens, B.; van de Goor, I.; Kremers, S. The Coaching on Lifestyle (CooL) Intervention for Overweight and Obesity: A Longitudinal Study into Participants’ Lifestyle Changes. Int. J. Environ. Res. Public Health 2018, 15, 680. [Google Scholar] [CrossRef]
- Arcury, T.A.; Sandberg, J.C.; Melius, K.P.; Quandt, S.A.; Leng, X.; Latulipe, C.; Miller, D.P.; Smith, D.A.; Bertoni, A.G. Older Adult Internet Use and eHealth Literacy. J. Appl. Gerontol. 2020, 39, 141–150. [Google Scholar] [CrossRef]
- Cheng, C.; Beauchamp, A.; Elsworth, G.R.; Osborne, R.H. Applying the Electronic Health Literacy Lens: Systematic Review of Electronic Health Interventions Targeted at Socially Disadvantaged Groups. J. Med. Internet Res. 2020, 22, e18476. [Google Scholar] [CrossRef] [PubMed]
- Mehra, S.; van den Helder, J.; Visser, B.; Engelbert, R.H.H.; Weijs, P.J.M.; Krose, B.J.A. Evaluation of a Blended Physical Activity Intervention for Older Adults: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e16380. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics * | Total (n = 212) | CON (n = 84) | HBex (n = 63) | HBex-Pro (n = 65) | |
|---|---|---|---|---|---|
| Age (years) | 72.2 (6.3) | 73.0 (6.5) | 72.3 (5.5) | 71.0 (6.6) | |
| Female sex n (%) | 148 (70) | 59 (70) | 42 (67) | 47 (72) | |
| Level of education a | Low education n (%) | 93 (44) | 38 (45) | 27 (43) | 28 (43) |
| Ethnicity | Caucasian n (%) | 201 (95) | 81 (96) | 59 (94) | 61 (94) |
| MMSE score | 28.3 (2.0) | 28.3 (1.6) | 28.6 (1.7) | 27.9 (2.6) | |
| Weight | kg | 73.6 (13.9) | 73.3 (12.7) | 72.4 (14.4) | 75.1 (14.9) |
| BMI | kg/m2 | 25.9 (4.2) | 25.7 (3.5) | 25.3 (3.9) | 26.8 (5.1) |
| Sarcopenia b n (%) | No Sarcopenia | 196 (92) | 79 (94) | 59 (94) | 58 (89) |
| Probable | 14 (6) | 4 (5) | 4 (6) | 6 (9) | |
| Confirmed | 2 (1) | 1 (1) | 0 (0) | 1 (2) | |
| Frailty score c n (%) | Non-Frail | 185 (87) | 72 (86) | 58 (92) | 55 (85) |
| Mildly Frail | 24 (11) | 12 (14) | 3 (5) | 9 (16) | |
| Moderately Frail/Frail | 3 (1) | 0 (0) | 2 (3) | 1 (2) | |
| Medical conditions d n (%) | Musculoskeletal | 125 (59) | 49 (58) | 39 (62) | 37 (57) |
| Arthrosis | 49 (23) | 16 (19) | 15 (23) | 18 (28) | |
| Cardiovascular | 115 (54) | 50 (58) | 33 (52) | 32 (49) | |
| Orthopedic implants | 27 (13) | 8 (10) | 12 (19) | 7 (11) | |
| Respiratory | 18 (8) | 4 (5) | 7 (11) | 7 (11) | |
| Diabetes type II | 13 (6) | 3 (4) | 5 (8) | 5 (8) | |
| Comorbidity(≥2 diseases) | 117 (55) | 47 (56) | 35 (56) | 35 (54) | |
| Nutritional intake—Macronutrients | |||||
| Energy | kcal/day | 1880 (472) | 1899 (450) | 1817 (433) | 1918 (533) |
| kcal/kg/day | 26.2 (7.6) | 26.3 (6.4) | 26.2 (8.5) | 26.1 (8.1) | |
| Carbohydrates | g/day | 186 (55.7) | 186 (55.5) | 185 (51.9) | 188 (60.2) |
| Fat | g/day | 75.4 (25.3) | 77.5 (23.6) | 71.7 (22.4) | 76.3 (29.7) |
| Protein | g/day | 77.8 (20.1) | 78.8 (20.1) | 74.6 (19.2) | 79.4 (20.8) |
| g/kg/day | 1.08 (0.3) | 1.09 (0.26) | 1.06 (0.30) | 1.07 (0.31) | |
| Protein—Animal source | g/day | 49.3 (17.1) | 50.4 (18.5) | 46.9 (16.8) | 50.2 (15.7) |
| Protein—Plant source | g/day | 28.5 (8.8) | 28.3 (8.1) | 27.8 (8.5) | 29.3 (10.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van den Helder, J.; Verlaan, S.; Tieland, M.; Scholten, J.; Mehra, S.; Visser, B.; Kröse, B.J.A.; Engelbert, R.H.H.; Weijs, P.J.M. Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults. Nutrients 2021, 13, 502. https://doi.org/10.3390/nu13020502
van den Helder J, Verlaan S, Tieland M, Scholten J, Mehra S, Visser B, Kröse BJA, Engelbert RHH, Weijs PJM. Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults. Nutrients. 2021; 13(2):502. https://doi.org/10.3390/nu13020502
Chicago/Turabian Stylevan den Helder, Jantine, Sjors Verlaan, Michael Tieland, Jorinde Scholten, Sumit Mehra, Bart Visser, Ben J. A. Kröse, Raoul H. H. Engelbert, and Peter J. M. Weijs. 2021. "Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults" Nutrients 13, no. 2: 502. https://doi.org/10.3390/nu13020502
APA Stylevan den Helder, J., Verlaan, S., Tieland, M., Scholten, J., Mehra, S., Visser, B., Kröse, B. J. A., Engelbert, R. H. H., & Weijs, P. J. M. (2021). Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults. Nutrients, 13(2), 502. https://doi.org/10.3390/nu13020502