
Well-Balanced Lunch Reduces Risk of Lifestyle-Related Diseases in Middle-Aged Japanese Working Men

Abstract
1. Introduction
2. Materials and Methods
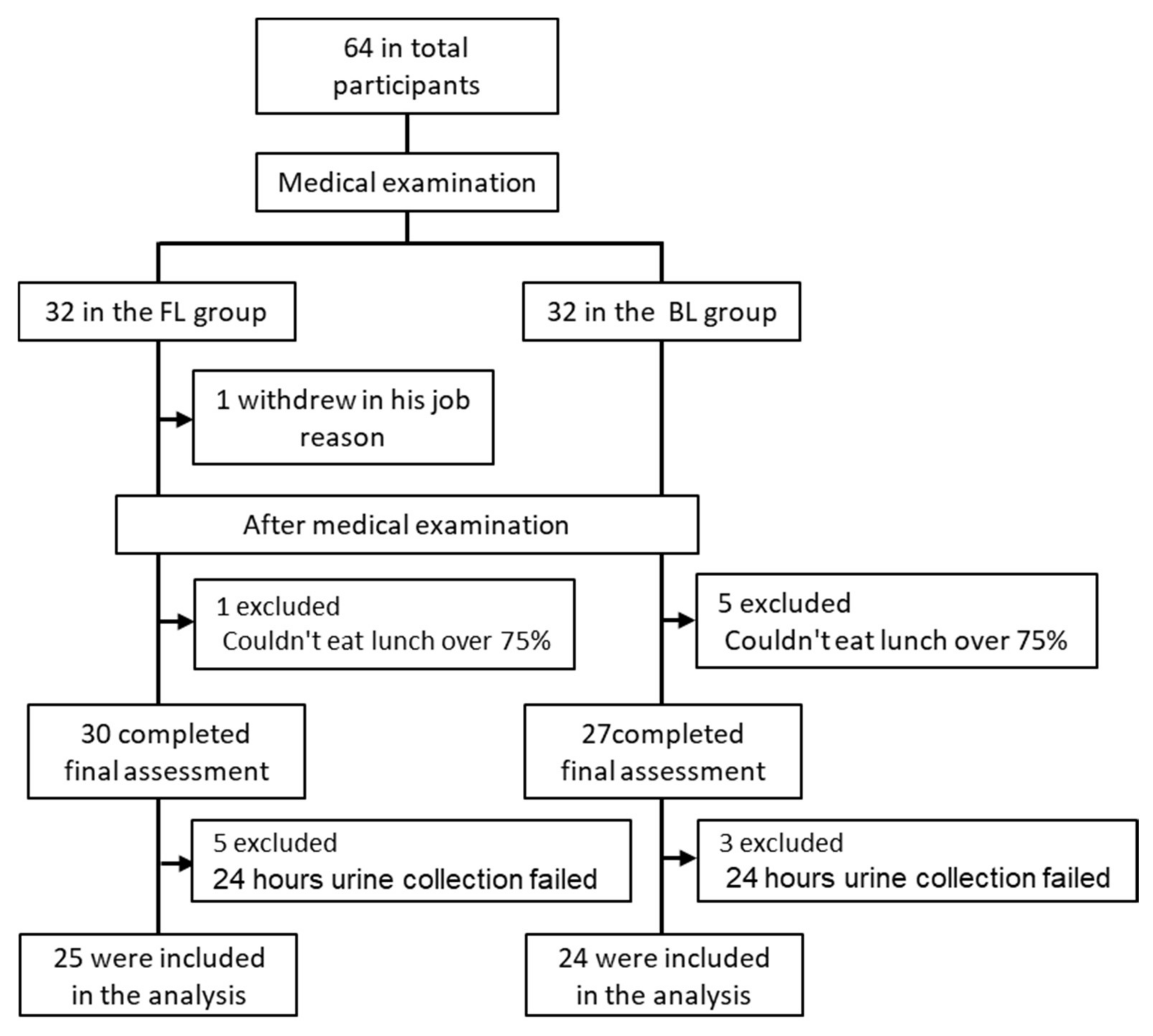
2.1. Participants and Methods
2.2. Study Design
2.3. Test Meals
2.4. Medical Examination
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
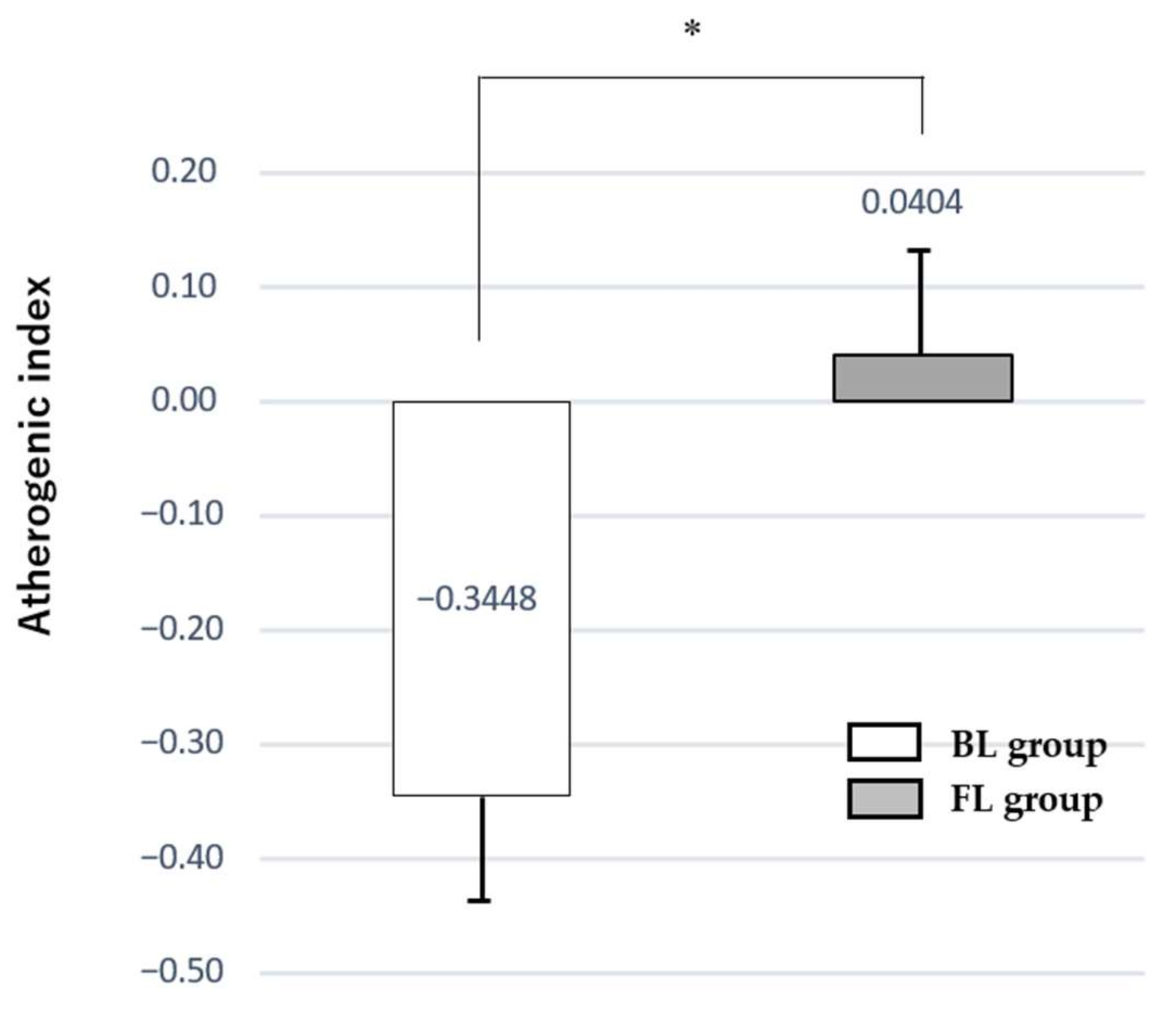
3.2. Changes in BMI, Blood Pressure, and Blood Sampling Test
3.3. Changes in Nutrition Biomarker of 24-h Urine Sampling
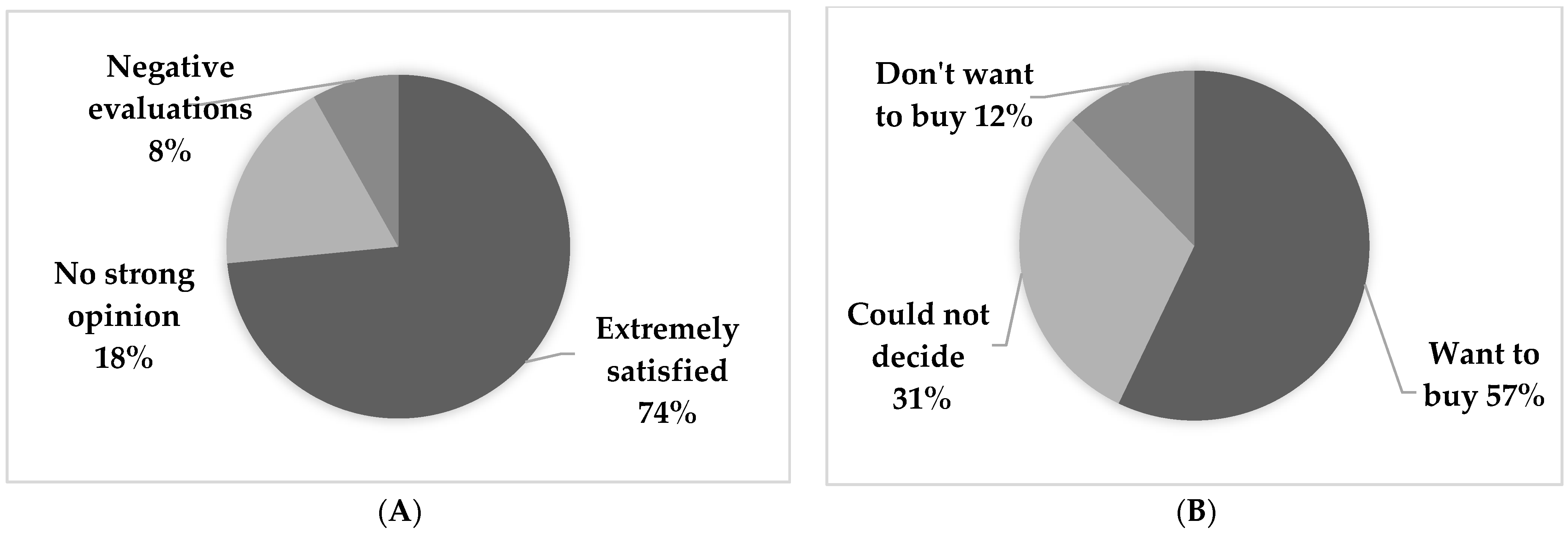
3.4. Impressions of Participation in the Study and Evaluation of Optimal Salt Diet
4. Discussion
4.1. Optimized Lunch and Its Effects
4.2. Changes in Nutritional Biomarkers by 24-h Urine Collection
4.3. Strengths and Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Yamori, Y.; Liu, L.; Ikeda, K.; Miura, A.; Mizushima, S.; Miki, T.; Nara, Y.; on behalf of the WHO Cardiovascular Diseases and Alimentary Comparison (WHO-CARDIAC) Study Group. Distribution of 24-hour Urinary Taurine Excretion and Association with Ischemic Heart Disease Mortality in 24 Populations of 16 Countries: Results from the WHO-CARDIAC Study. Hypertens. Res. 2001, 24, 453–457. [Google Scholar] [CrossRef]
- Yamori, Y.; Liu, L.; Mizushima, S.; Ikeda, K.; Nara, Y. Male Cardiovascular Mortality and Dietary Markers in 25 Population Samples of 16 Countries. J. Hypertens. 2006, 24, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Yamori, Y. Food Factors for Atherosclerosis Prevention: Asian Perspective Derived from Analyses of Worldwide Dietary Biomarkers. Exp. Clin. Cadiol. 2006, 11, 94–98. [Google Scholar]
- Yamori, Y.; Sagara, M.; Arai, Y.; Kobayashi, H.; Kishimoto, K.; Matsuno, K.; Mori, H.; Mori, M. Soy and Fish as Features of the Japanese Diet and Cardiovascular Disease Risks. PLoS ONE 2017, 12, e0186533. [Google Scholar] [CrossRef]
- Uesugi, T.; Fukui, Y.; Yamori, Y. Beneficial Effects of Soybean Isoflavone Supplementation on Bone Metabolism and Serum Lipids in Postmenopausal Japanese Women: A Four-week Study. J. Am. Coll. Nutr. 2002, 2, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.A.; Burke, V.; Puddey, I.B.; Watts, G.F.; O’Neal, D.N.; Best, J.D.; Beilin, L.J. Purified Eicosapentaenoic and Docosahexaenoic Acids have Differential Effects on Serum Lipids and Lipoproteins, LDL Particle Size, Glucose, and Insulin in Mildly Hyperlipidemic Men. Am. J. Clin. Nutr. 2000, 5, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Sagara, M.; Kanda, T.; Njelekera, M.; Armitage, L.; Birt, N.; Birt, C.; Yamori, Y. Effects of Dietary Intake of Soy Protein and Isoflavones on Cardiovascular Disease Risk Factors in High Risk: Middle-Aged Men in Scotland. J. Am. Coll. Nutr. 2003, 23, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Yamori, Y.; Sagara, M.; Mori, H.; Mori, M. Nutrition: Soy and Fish. In The Encyclopedia of Cardiovascular Research and Medicine; Elsevier Inc.: Amsterdam, The Netherlands, 2018; Volume 3, pp. 538–545. [Google Scholar]
- Tanaka, N.; Irino, Y.; Shinohara, M.; Tsuda, S.; Mori, T.; Nagao, M.; Oshita, T.; Mori, K.; Hara, T.; Toh, R.; et al. Eicosapentaenoic Acid-Enriched High-Density Lipoproteins Exhibit Anti-Atherogenic Properties. Circ. J. 2018, 82, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Yamori, Y.; Sagara, M.; Arai, Y.; Kobayashi, H.; Kishimoto, K.; Matsuno, I.; Mori, H.; Mori, M. Cross-Sectional Inverse Association of Regular Soy Intake with Insulin Resistance in Japanese Elderly. J. Nutr. Gerontol. Geriatr. 2018, 37, 282–291. [Google Scholar] [CrossRef]
- Gorety, J.M.; Roxana, V.R.; Ana, L.G.; Rosa-Virgen, P.M.; Beatriz, E.M.; Laurence, S.H. Effect of n-3 Polyunsaturated Fatty Acid Supplementation on Metabolic and Inflammatory Biomarkers in Type 2 Diabetes Mellitus Patients. Nutrients 2017, 9, 573. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Mori, H.; Yamori, Y. Nutritional Biomarker Analyses for Hypertension-Related Risk Assessment and Control. World J. Cardiovasc. Dis. 2014, 4, 268–276. [Google Scholar] [CrossRef][Green Version]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. DASH Sodium Collaborative Research Group. Effects on Blood Pressure of Reduced Dietar y Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, A.; Kajiya, K.; Kishi, H.; Inagaki, J.; Mitarai, M.; Oda, H.; Umemoto, S.; Kobayashi, S. Effects of the DASH-JUMP Dietary Intervention in Japanese Participants with High-Normal Blood Pressure and Stage 1 Hypertension. Hypertens. Res. 2016, 39, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Shintomi, T.; Motoi, S.; Miura, K.; Tomoe, M. Pilot Study to Examine Blood Pressure Improvement Effects of DASH Diet Boxed Meals. J. Nutr. Diet. 2019, 77, 133–144. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Test Group (n = 32) | Control Group (n = 32) | |
|---|---|---|
| Age (years old) | 47.2 ± 5.6 | 47.2 ± 5.5 |
| Height (cm) | 171.0 ± 5.6 | 169.6 ± 5.7 |
| Weight (kg) | 73.5 ± 9.9 | 72.1 ± 10.1 |
| BMI (kg/m2) | 25.1 ± 2.7 | 25.1 ± 3.2 |
| SBP (mm Hg) | 126.5 ± 15.6 | 125.5 ± 11.3 |
| DBP (mm Hg) | 80.3 ± 11.3 | 79.5 ± 9.1 |
| Menu | Nutritional Value | Menu | Nutritional Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| FL | BL | FL | BL | ||||||
Hamburger vegitable sauce |
| Energy (kcal) | 708 | 713 | Ground Meat Cutlet |
| Energy (kcal) | 717 | 723 |
| Protein (g) | 24 | 20 | Protein (g) | 22 | 17 | ||||
| Lipid (g) | 24 | 21 | Lipid (g) | 25 | 20 | ||||
| Carbohydrate (g) | 80 | 109 | Carbohydrate (g) | 100 | 118 | ||||
| K (mg) | 760 | 713 | K (mg) | 907 | 790 | ||||
| Dietary fiber (g) | 11.1 | 7.4 | Dietary fiber (g) | 11.6 | 8.0 | ||||
| NaCl (g) | 0.9 | 1.2 | NaCl (g) | 2.0 | 2.2 | ||||
| DHA (mg) | 980 | - | DHA (mg) | 882 | - | ||||
| Isoflavone (mg) | 40 | - | Isoflavone (mg) | 40 | - | ||||
Deep-fried lotus root |
| Energy (kcal) | 718 | 720 | Hamburger tomato sauce |
| Energy (kcal) | 740 | 744 |
| Protein (g) | 24 | 21 | Protein (g) | 25 | 20 | ||||
| Lipid (g) | 21 | 14 | Lipid (g) | 24 | 22 | ||||
| Carbohydrate (g) | 105 | 124 | Carbohydrate (g) | 104 | 117 | ||||
| K (mg) | 970 | 942 | K (mg) | 938 | 842 | ||||
| Dietary fiber (g) | 10.8 | 7.8 | Dietary fiber (g) | 12.3 | 8.6 | ||||
| NaCl (g) | 1.8 | 2.3 | NaCl (g) | 2.5 | 2.8 | ||||
| DHA (mg) | 827 | - | DHA (mg) | 980 | - | ||||
| Isoflavone (mg) | 40 | - | Isoflavone (mg) | 40 | - | ||||
Tsukune |
| Energy (kcal) | 727 | 735 | Deep-fried lotus root |
| Energy (kcal) | 720 | 723 |
| Protein (g) | 26 | 22 | Protein (g) | 23 | 20 | ||||
| Lipid (g) | 23 | 17 | Lipid (g) | 20 | 14 | ||||
| Carbohydrate (g) | 101 | 121 | Carbohydrate (g) | 110 | 128 | ||||
| K (mg) | 1258 | 1136 | K (mg) | 867 | 839 | ||||
| Dietary fiber (g) | 8.9 | 10.0 | Dietary fiber (g) | 11.0 | 8.0 | ||||
| NaCl (g) | 2.8 | 3.0 | NaCl (g) | 2.2 | 2.6 | ||||
| DHA (mg) | 1157 | - | DHA (mg) | 827 | - | ||||
| Isoflavone (mg) | 40 | - | Isoflavone (mg) | 40 | - | ||||
Pepper stuffed with meat |
| Energy (kcal) | 651 | 649 | Tsukune sweet and sour sauce |
| Energy (kcal) | 725 | 718 |
| Protein (g) | 23 | 22 | Protein (g) | 24 | 21 | ||||
| Lipid (g) | 19 | 11 | Lipid (g) | 24 | 16 | ||||
| Carbohydrate (g) | 94 | 107 | Carbohydrate (g) | 102 | 122 | ||||
| K (mg) | 791 | 841 | K (mg) | 1448 | 1326 | ||||
| Dietary fiber (g) | 10.5 | 6.8 | Dietary fiber (g) | 14.4 | 11.5 | ||||
| NaCl (g) | 2.2 | 2.1 | NaCl (g) | 2.1 | 2.3 | ||||
| DHA (mg) | 892 | - | DHA (mg) | 1157 | - | ||||
| Isoflavone (mg) | 40 | - | Isoflavone (mg) | 40 | - | ||||
Chicken balls with tomato |
| Energy (kcal) | 711 | 718 | Pepper stuffed with meat |
| Energy (kcal) | 684 | 678 |
| Protein (g) | 25 | 21 | Protein (g) | 22 | 22 | ||||
| Lipid (g) | 20 | 18 | Lipid (g) | 19 | 14 | ||||
| Carbohydrate (g) | 106 | 119 | Carbohydrate (g) | 107 | 120 | ||||
| K (mg) | 958 | 940 | K (mg) | 780 | 831 | ||||
| Dietary fiber (g) | 12.1 | 8.6 | Dietary fiber (g) | 11.1 | 7.4 | ||||
| NaCl (g) | 2.1 | 2.4 | NaCl (g) | 2.6 | 2.5 | ||||
| DHA (mg) | 700 | - | DHA (mg) | 892 | - | ||||
| Isoflavone (mg) | 40 | - | Isoflavone (mg) | 40 | - | ||||
| Fortified Lunch Group (n25) | Balanced Lunch Group (n24) | |||||
|---|---|---|---|---|---|---|
| Baseline | 4 Weeks | p-Value | Baseline | 4 Weeks | p-Value | |
| Physical examination and blood pressure | ||||||
| Age (years old) | 47.1 ± 6.1 | 46.0 ± 4.3 | ||||
| Height (cm) | 170.3 ± 5.5 | 170.4 ± 5.9 | ||||
| Weight (kg) | 73.3 ± 8.8 | 72.2 ± 8.7 | <0.001 | 72.4 ± 10.7 | 71.5 ± 10.7 | <0.001 |
| BMI (kg/m2) | 25.2 ± 2.6 | 24.9 ± 2.5 | <0.001 | 25.0 ± 3.5 | 24.7 ± 3.5 | <0.001 |
| SBP (mm Hg) | 125.6 ± 12.5 | 125.6 ± 14.4 | 0.99 | 126.3 ± 12.3 | 122.4 ± 14.4 | 0.06 |
| DBP (mm Hg) | 79.6 ± 10.8 | 76.1 ± 12.0 | 0.02 | 80.5 ± 9.9 | 77.0 ± 11.8 | 0.002 |
| Blood sampling test | ||||||
| Triglyceride (mg/dL) | 150.4 ± 63.2 | 139.3 ± 71.0 | 0.20 | 157.7 ± 95.5 | 167.2 ± 87.8 | 0.66 |
| T- cholesterol (mg/dL) | 197.2 ± 31.0 | 192.8 ± 26.5 | 0.21 | 202.0 ± 18.4 | 200.8 ± 19.5 | 0.74 |
| HDL- cholesterol (mg/dL) | 49.4 ± 11.3 | 53.5 ± 11.9 | 0.01 | 53.1 ± 11.0 | 52.5 ± 12.8 | 0.64 |
| AI | 3.1 ± 0.8 | 2.8 ± 1.0 | 0.003 | 3.0 ± 1.0 | 3.0 ± 0.9 | 0.72 |
| Glucose (mg/dL) | 96.6 ± 16.7 | 102.3 ± 14.4 | 0.13 | 96.8 ± 9.8 | 96.2 ± 8.1 | 0.77 |
| Insulin (μU/mL) | 10.8 ± 7.6 | 10.9 ± 13.7 | 0.97 | 17.6 ± 24.4 | 10.7 ± 9.8 | 0.19 |
| HOMA-IR | 2.7 ± 2.7 | 3.0 ± 4.6 | 0.81 | 4.3 ± 6.0 | 2.7 ± 2.8 | 0.22 |
| HBA1C (%) | 5.0 ± 0.5 | 4.9 ± 0.5 | 0.03 | 5.0 ± 0.4 | 4.9 ± 0.3 | <0.001 |
| 24-h urinary sampling | ||||||
| NaCl (g/day) | 14.1 ± 3.7 | 11.2 ± 3.8 | <0.01 | 14.1 ± 5.3 | 11.0 ± 4.8 | 0.03 |
| K (g/day) | 2.0 ± 0.5 | 1.95 ± 0.7 | 0.74 | 1.9 ± 0.4 | 1.9 ± 0.5 | 0.96 |
| Na/K | 4.8 ± 1.2 | 4.0 ± 1.4 | 0.01 | 4.9 ± 1.9 | 4.0 ± 2.1 | 0.11 |
| Mg (mg/day) | 101.0 ± 34.6 | 90.0 ± 53.8 | 0.22 | 95.5 ± 32.0 | 81.1 ± 25.6 | 0.01 |
| Protein (g) | 73.5 ± 15.0 | 70.7 ± 16.7 | 0.34 | 74.2 ± 15.8 | 67.6 ± 14.9 | 0.04 |
| Isoflavoneds (µmol/day) | 25.2 ± 19.1 | 53.0 ± 35.0 | <0.001 | 19.1 ± 13.9 | 21.0 ± 23.9 | 0.70 |
| Taurine (µmol/day) | 1279.9 ± 595 | 1254.6 ± 547 | 0.79 | 1567.4 ± 1141 | 1773.1 ± 228 | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, M. Well-Balanced Lunch Reduces Risk of Lifestyle-Related Diseases in Middle-Aged Japanese Working Men. Nutrients 2021, 13, 4528. https://doi.org/10.3390/nu13124528
Mori M. Well-Balanced Lunch Reduces Risk of Lifestyle-Related Diseases in Middle-Aged Japanese Working Men. Nutrients. 2021; 13(12):4528. https://doi.org/10.3390/nu13124528
Chicago/Turabian StyleMori, Mari. 2021. "Well-Balanced Lunch Reduces Risk of Lifestyle-Related Diseases in Middle-Aged Japanese Working Men" Nutrients 13, no. 12: 4528. https://doi.org/10.3390/nu13124528
APA StyleMori, M. (2021). Well-Balanced Lunch Reduces Risk of Lifestyle-Related Diseases in Middle-Aged Japanese Working Men. Nutrients, 13(12), 4528. https://doi.org/10.3390/nu13124528