
Changes in Dietary Patterns through a Nutritional Intervention with a Traditional Atlantic Diet: The Galiat Randomized Controlled Trial

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
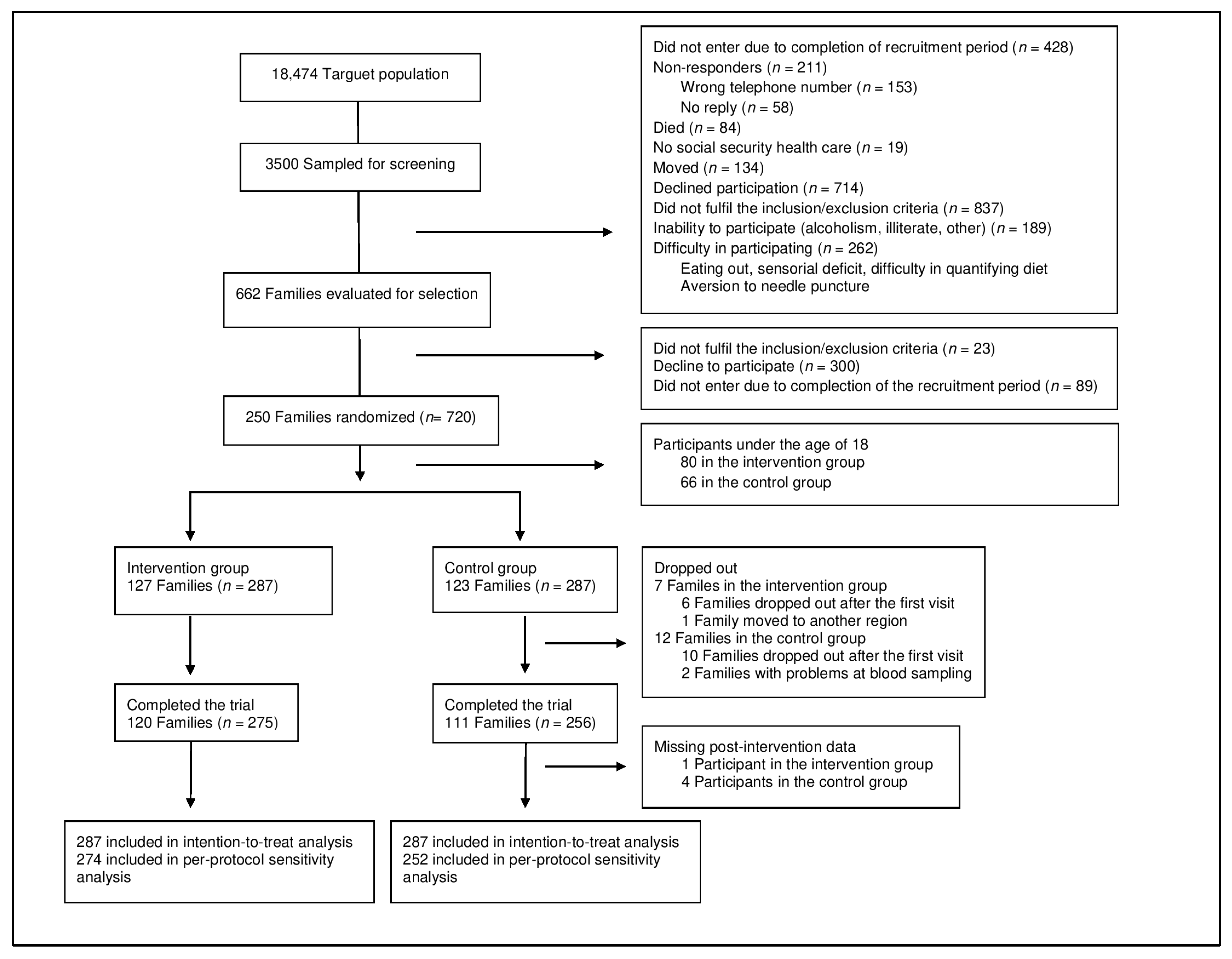
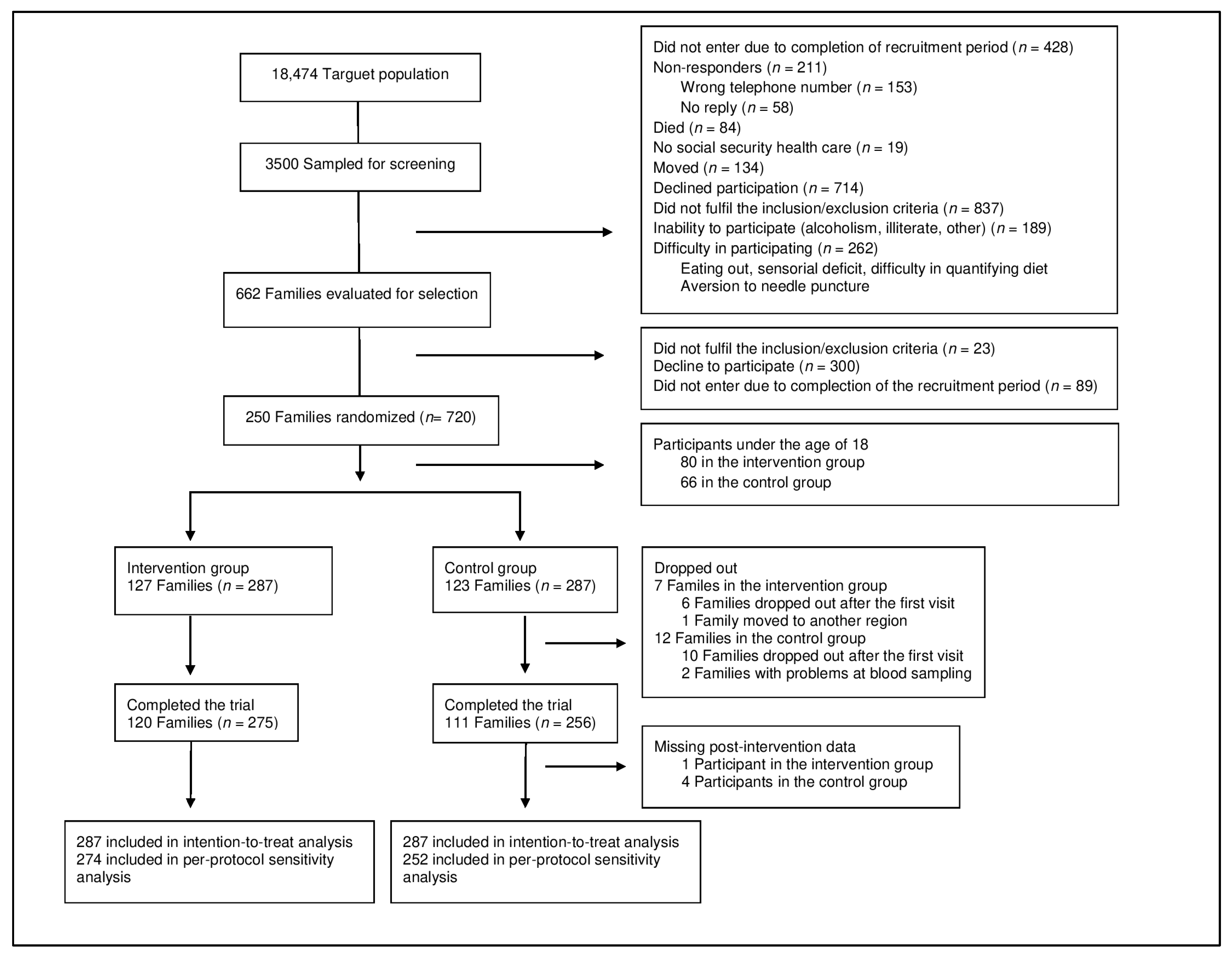
2.1. Study Design
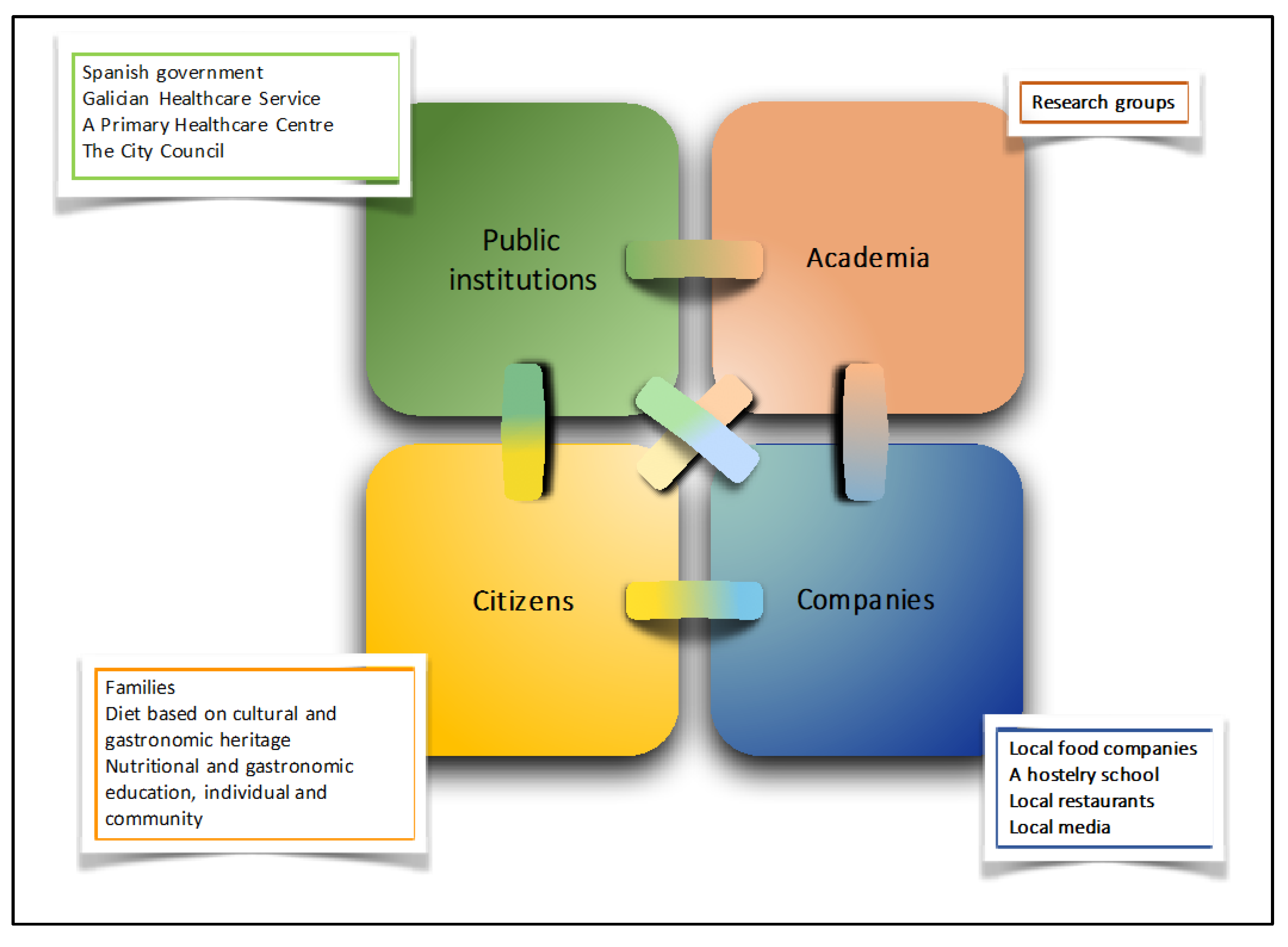
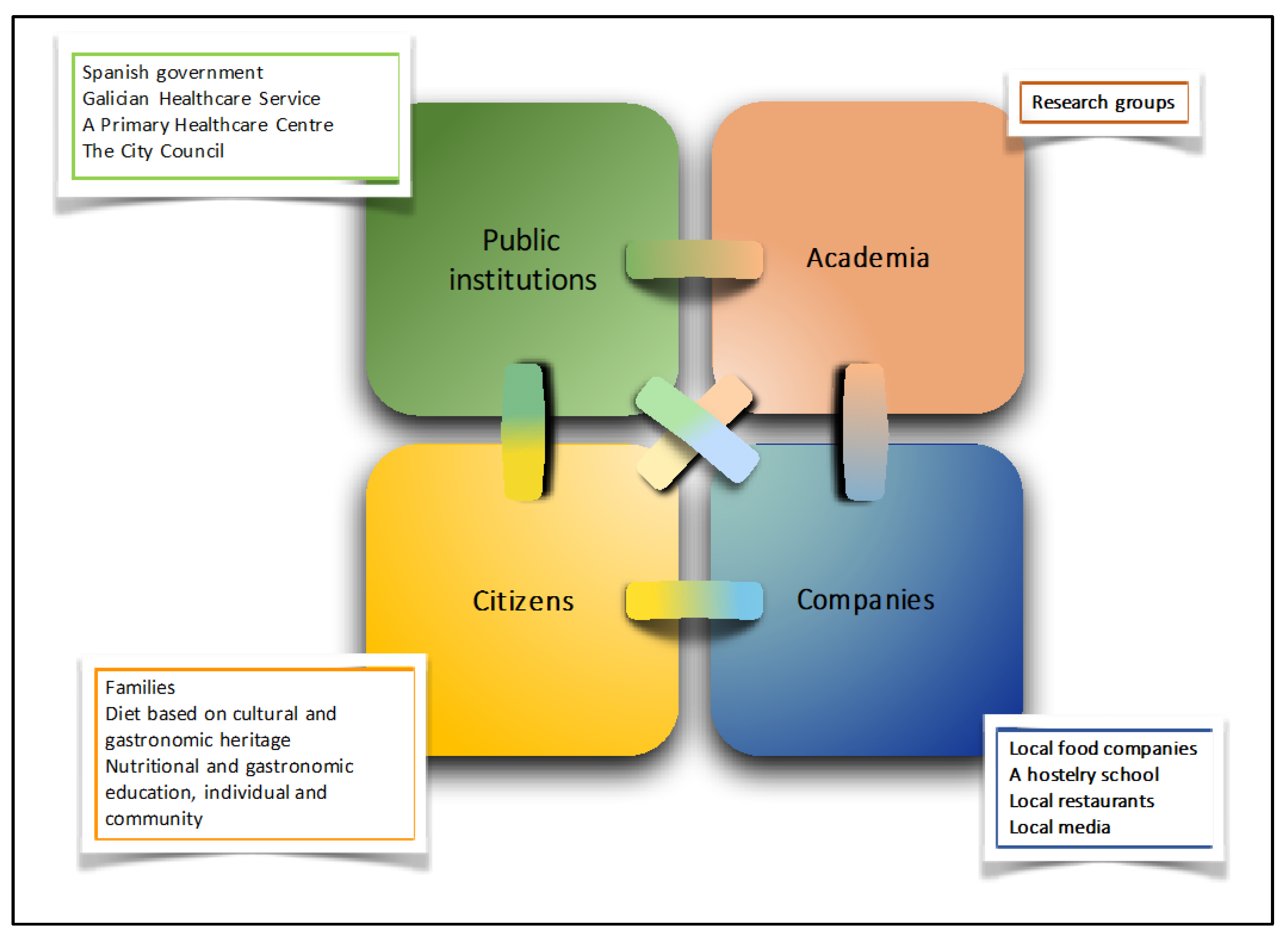
2.2. Theoretical Model
2.3. Dietary Intervention
2.4. Sociodemographic, Health, and Body Weight Data
2.5. Dietary Assessment
2.6. Statistical Analyses
3. Results
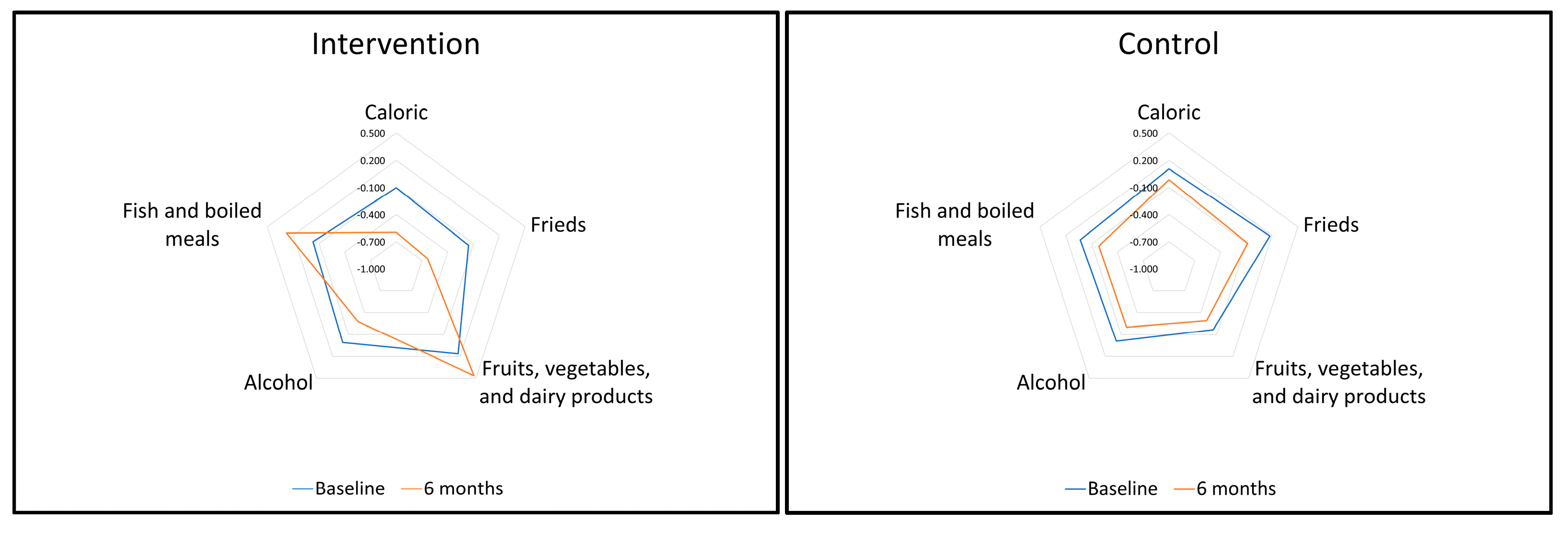
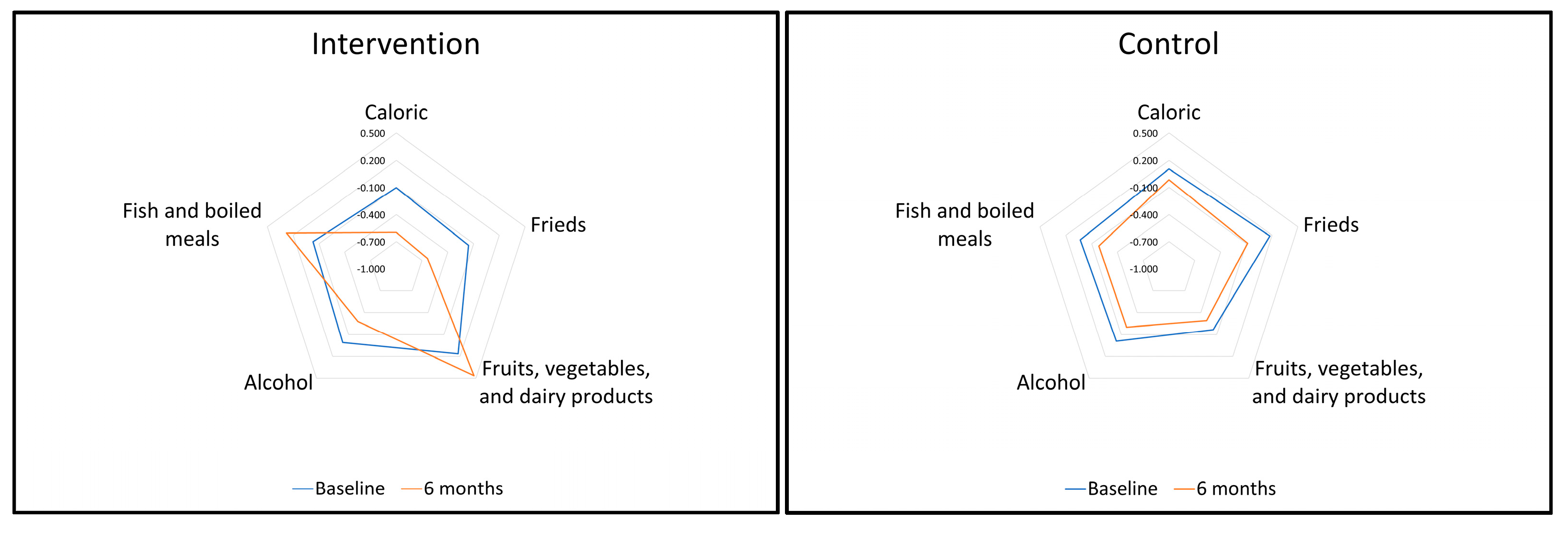
3.1. Effect of the Galiat Intervention on DP Scores
3.2. Association between DP Changes and Body Weight
4. Discussion
4.1. Mechanism and Explanations
4.2. Results in Relation with Other Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FAO; WHO. Sustainable Healthy Diets: Guiding Principles; Sustainable Healthy Diets: Rome, Italy, 2019. [Google Scholar]
- Haddad, L.; Hawkes, C.; Waage, J.; Webb, P.; Godfra, C.; Toulmin, C. Food Systems and Diets: Facing the Challenges of the 21st Century; Global Panel on Agriculture and Food Systems for Nutrition: London, UK, 2016. [Google Scholar]
- Yu, E.; Malik, V.S.; Hu, F.B. Cardiovascular disease prevention by diet modification: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 914–926. [Google Scholar] [CrossRef]
- Carayannis, E.G.; Campbell, D.F.J. ‘Mode 3′ and ‘Quadruple Helix’: Toward a 21st century fractal innovation ecosystem. Int. J. Technol. Manag. 2009, 46, 201–234. [Google Scholar] [CrossRef] [Green Version]
- Carayannis, E.G.; Campbell, D.F.J. Triple Helix, Quadruple Helix and Quintuple Helix and how do knowledge, innovation, and environment relate to each other? Int. J. Soc. Ecol. Sustain. Dev. 2010, 1, 41–69. [Google Scholar] [CrossRef]
- UN. Sustainable Development Goals. Available online: http://sustainabledevelopment.un.org/?menu=1300 (accessed on 2 June 2020).
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Amanda Wood, A.; et al. Food in the anthropocene: The EAT–Lancet commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- González-García, S.; Green, R.F.; Scheelbeek, P.F.; Harris, F.; Dangour, A.D. Dietary recommendations in Spain–affordability and environmental sustainability? J. Clean. Prod. 2020, 254, 120125. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Lopes, C.; Rodríguez-Artalejo, F. Adherence to the Southern European Atlantic diet and occurrence of nonfatal acute myocardial infarction. Am. J. Clin. Nutr. 2010, 92, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillón, P.; Oliveira, A.; Lopes, C.; López-García, E.; Rodriguez-Artalejo, F. The Southern European Atlantic diet is associated with lower concentrations of markers of coronary risk. Atherosclerosis 2013, 226, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Esteve-Llorens, X.; Darriba, C.; Moreira, M.T.; Feijoo, G.; González-García, S. Towards an environmentally sustainable and healthy Atlantic dietary pattern: Life cycle carbon footprint and nutritional quality. Sci. Total Environ. 2019, 646, 70415. [Google Scholar] [CrossRef] [PubMed]
- Hone, T.; Macinko, J.; Millett, C. Revisiting Alma-Ata: What is the role of primary health care in achieving the sustainable development goals? Lancet 2018, 392, 1461–1472. [Google Scholar] [CrossRef]
- Nutting, P.A.; Goodwin, M.A.; Flocke, S.A.; Zyzanski, S.J.; Stange, K.C. Continuity of primary care: To whom does it matter and when? Ann. Fam. Med. 2003, 1, 149–155. [Google Scholar] [CrossRef]
- Barker, I.; Steventon, A.; Deeny, S.R. Association between continuity of care in general practice and hospital admissions for ambulatory care sensitive conditions: Cross sectional study of routinely collected, person level data. BMJ 2017, 356, j84. [Google Scholar] [CrossRef] [Green Version]
- Horstmann, E.; Brown, J.; Islam, F.; Buck, J.; Agins, B.D. Retaining HIV-infected patients in care: Where are we? Where do we go from here? Clin. Infect. Dis. 2010, 50, 752–761. [Google Scholar] [CrossRef]
- Munro, S.A.; Lewin, S.A.; Smith, H.J.; Engel, M.E.; Fretheim, A.; Volmink, J. Patient adherence to tuberculosis treatment: A systematic review of qualitative research. PLoS Med. 2007, 4, e238. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Malvar, M.; Leis, R.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Gude, F. A randomised, family-focused dietary intervention to evaluate the Atlantic diet: The Galiat study protocol. BMC Public Health 2016, 16, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo-Malvar, M.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Leis, R.; Gude, F. Effects of a community-based behavioral intervention with a traditional Atlantic diet on cardiometabolic risk markers: A cluster randomized controlled trial (“The Galiat Study”). Nutrients 2021, 13, 1211. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Kivlihan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaz Velho, M.; Pinheiro, R.; Rodrigues, A.S. The Atlantic diet—origin and features. Int. J. Food Stud. 2016, 5, 106–119. [Google Scholar] [CrossRef]
- The IPAQ-Group International Physical Activity Questionnaire. Available online: http://www.sdp.univ.fvg.it/sites/default/files/IPAQ_English_self-admin_long.pdf (accessed on 14 July 2020).
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latorre-Millán, M.; Rupérez, A.I.; González-Gil, E.M.; Santaliestra-Pasías, A.; Vázquez-Cobela, R.; Gil-Campos, M.; Aguilera, C.M.; Gil, A.M.; Moreno, L.A.; Leis, R.; et al. Dietary patterns and their association with body composition and cardiometabolic markers in children and adolescents: Genobox cohort. Nutrients 2020, 12, 3424. [Google Scholar] [CrossRef]
- Pérez-Gimeno, G.; Rupérez, A.I.; Vázquez-Cobela, R.; Herráiz-Gastesi, G.; Gil-Campos, M.; Aguilera, C.M.; Moreno, L.A.; Trabazo, M.R.L.; Bueno-Lozano, G. Energy dense salty food consumption frequency is associated with diastolic hypertension in Spanish children. Nutrients 2020, 12, 1027. [Google Scholar] [CrossRef] [Green Version]
- Huybrechts, I.; Bornhorst, C.; Pala, V.; Moreno, L.A.; Barba, G.; Lissner, L.; Fraterman, A.; Veidebaum, T.; Hebestreit, A.; Sieri, S.; et al. Evaluation of the children’s eating habits questionnaire used in the IDEFICS study by relating urinary calcium and potassium to milk consumption frequencies among European children. Int. J. Obes. 2011, 35 (Suppl. 1), S69–S78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanfer, A.; Hebestreit, A.; Ahrens, W.; Krogh, V.; Sieri, S.; Lissner, L.; Eiben, G.; Siani, A.; Huybrechts, I.; Loit, H.-M.; et al. Reproducibility of food consumption frequencies derived from the children’s eating habits questionnaire used in the IDEFICS study. Int. J. Obes. 2011, 35 (Suppl. 1), S61–S68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bel-Serrat, S.; Mouratidou, T.; Pala, V.; Huybrechts, I.; Börnhorst, C.; Fernández-Alviraet, J.M.; Hadjigeorgiou, C.; Eiben, G.; Hebestreit, A.; Lissner, L.; et al. Relative validity of the children’s eating habits questionnaire-food frequency section among young European children: The IDEFICS study. Public Health Nutr. 2014, 17, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.O.; Mueller, C.W. Factor Analysis: Statistical Methods and Practical Issues; Sage Publications, Inc.: Newbury Park, CA, USA, 1978. [Google Scholar]
- Northstone, K.; Emmett, P.M. A comparison of methods to assess changes in dietary patterns from pregnancy to 4 years post-partum obtained using principal components analysis. Br. J. Nutr. 2008, 99, 1099–1106. [Google Scholar] [CrossRef]
- Esteve-Llorens, X.; Moreira, M.T.; Feijoo, G.; González-García, S. Linking environmental sustainability and nutritional quality of the Atlantic diet recommendations and real consumption habits in Galicia (NW Spain). Sci. Total Environ. 2019, 683, 71–79. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [CrossRef] [Green Version]
- Newby, P.K.; Muller, D.; Hallfrisch, J.; Andres, R.; Tucker, K.L. Food patterns measured by factor analysis and anthropometric changes in adults. Am. J. Clin. Nutr. 2004, 80, 504–513. [Google Scholar] [CrossRef]
- Newby, P.; Weismayer, C.; Akesson, A.; Tucker, K.; Wolk, A. Longitudinal changes in food patterns predict changes in weight and body mass index and the effects are greatest in obese women. J. Nutr. 2006, 136, 2580–2587. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Nassan, F.L.; Jensen, T.K.; Priskorn, L.; Halldorsson, T.I.; Chavarro, J.E.; Jørgensen, N. Association of dietary patterns with testicular function in young Danish men. JAMA Netw. Open 2020, 3, e1921610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, A.C.; Seed, P.T.; Patel, N.; Barr, S.; Bell, R.; Briley, A.L.; Sian, M.; Godfrey, K.M.; Nelson, S.M.; Oteng-Ntim, E.; et al. Dietary patterns in obese pregnant women; influence of a behavioral intervention of diet and physical activity in the UPBEAT randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lioret, S.; McNaughton, S.; Crawford, D.; Spence, A.; Hesketh, K.; Campbell, K. Parents’ dietary patterns are significantly correlated: Findings from the Melbourne infant feeding activity and nutrition trial program. BJN 2012, 108, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, A.D.; Lioret, S.; Cameron, A.J.; Hesketh, K.D.; McNaughton, S.A.; Crawford, D.; Campbell, K.J. The effect of an early childhood obesity intervention on father’s obesity risk behaviors: The Melbourne InFANT program. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- Pala, V.; Lissner, L.; Hebestreit, A.; Lanfer, A.; Sieri, S.; Siani, A.; Huybrechts, I.; Kambek, L.; Molnar, D.; Tornaritis, M.; et al. Dietary patterns and longitudinal change in body mass in European children: A follow-up study on the IDEFICS multicenter cohort. Eur. J. Clin. Nutr. 2013, 67, 1042–1049. [Google Scholar] [CrossRef]
- Murakami, K.; Shinozaki, N.; Fujiwara, A.; Yuan, X.; Hashimoto, A.; Fujihashi, H. Wang, H.-C.; E Livingstone, M.B.; Sasaki, S. A systematic review of principal component analysis-derived dietary patterns in Japanese adults: Are major dietary patterns reproducible within a country? Adv. Nutr. 2019, 10, 237–249. [Google Scholar] [CrossRef]
- Wirfält, E.; Drake, I.; Wallström, P. What do review papers conclude about food and dietary patterns? Food Nutr. Res. 2013, 57, 20523. [Google Scholar] [CrossRef] [Green Version]
- McEvoy, C.T.; Cardwell, C.R.; Woodside, J.V.; Young, I.S.; Hunter, S.J.; McKinley, M.C. A posteriori dietary patterns are related to risk of type 2 diabetes: Findings from a systematic review and meta-analysis. J. Acad. Nutr. Diet. 2014, 114, 1759–1775.e4. [Google Scholar] [CrossRef]
- Rodríguez-Monforte, M.; Flores-Mateo, G.; Sánchez, E. Dietary patterns and CVD: A systematic review and meta-analysis of observational studies. Br. J. Nutr. 2015, 114, 1341–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Monforte, M.; Sánchez, E.; Barrio, F.; Costa, B.; Flores-Mateo, G. Metabolic syndrome and dietary patterns: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2017, 56, 925–947. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, W.; Siani, A.; Adan, R.; De Henauw, S.; Eiben, G.; Gwozdz, W.; Hebestreit, A.; Hunsberger, M.; Kaprio, J.; Krogh, V.; et al. Cohort Profile: The transition from childhood to adolescence in European children-how I.Family extends the IDEFICS cohort. Int. J. Epidemiol. 2017, 46, 1394–1395j. [Google Scholar] [CrossRef] [Green Version]
- Jilani, H.; Pohlabeln, H.; De Henauw, S.; Eiben, G.; Hunsberger, M.; Molnar, D.; Moreno, L.A.; Pala, V.; Russo, P.; Solea, A.; et al. Relative Validity of a Food and Beverage Preference Questionnaire to Characterize Taste Phenotypes in Children Adolescents and Adults. Nutrients 2019, 11, 1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B. Dietary patterns analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Intervention Components | |
|---|---|
| Basal (time 0) | Nutrition education course (30–40 min) provided to individual families by nutritionists with recommendations for adults and children: information about the Atlantic diet and the food pyramid, benefits of physical activity and eating five meals per day; information on how to prepare food menus, how and why to limit sedentary activity, and how to use the education material provided. Distribute a book with educational material and recipes. Distribute a diary with food delivery dates (every 3 weeks). Start delivery of food packages (adapted for the number of family members in one household). |
| Following the basal visit | Group session (2 h) by researchers and nutritionists to explain the influence of lifestyle on health, how to change to a healthier diet, importance of physical activity, characteristics of the traditional Atlantic diet, and patterns for designing a healthy diet. Cooking class led by teaching chefs; recommendations on portion size. |
| 3 months | Nutrition education course (30–40 min) provided to individual families by nutritionists to strengthen knowledge and messages, use of educational material and recipes; to discuss realistic expectations for behavior change; to develop individual goals, behavior skills, and action plans; and to identify barriers and resolve doubts. Distribute a diary with new food delivery dates (every 3 weeks) and delivery of food packages (adapted for the number of family members). |
| 6 months | End of the intervention. Last nutrition education course (30–40 min) provided to individual families by nutritionists to review progress and renew individual and family action plans for the future. |
| Study Sample | |||
|---|---|---|---|
| Characteristic | Control Arm | Intervention Arm | p-Value |
| Families/study subjects. N | 124/287 | 126/287 | 0.866 |
| Participants per family. Mean ± SD | 2.3 ± 0.8 | 2.3 ± 0.7 | 0.297 |
| Male sex. N (%) | 114 (39.7) | 117 (40.8) | 0.798 |
| Age. Years. Mean ± SD | 45.3 ± 15.4 | 48.2 ± 15.8 | 0.012 |
| Marital status. N (%) | 0.310 | ||
| Married/with partner | 194 (67.8) | 210 (73.4) | |
| Divorced/separated/widowed | 33 (11.5) | 28 (9.8) | |
| Single | 59 (20.6) | 48 (16.8) | |
| Educational level. N (%) | 0.520 | ||
| None | 29 (10.1) | 30 (10.5) | |
| Elementary | 120 (41.8) | 103 (35.9) | |
| Secondary | 91 (31.7) | 103 (35.9) | |
| University or higher | 47 (16.4) | 51 (17.7) | |
| Employment status. N (%) | 0.207 | ||
| Employed | 148 (51.6) | 139 (48.4) | |
| Retired | 40 (13.9) | 56 (19.5) | |
| Other | 99 (34.5) | 92 (32.1) | |
| Smoking status. N (%) | 0.106 | ||
| Never smoker | 128 (44.6) | 120 (41.8) | |
| Ex-smoker | 50 (17.4) | 71 (24.7) | |
| Current smoker | 109 (38.0) | 96 (33.5) | |
| Alcohol intake. N (%) | 0.789 | ||
| Abstainers | 123 (43.5) | 124 (43.2) | |
| Light drinkers (1–140 g/week) | 132 (46.6) | 130 (45.3) | |
| Heavy drinkers (>140 g/week) | 28 (9.9) | 33 (11.5) | |
| Comorbidities. N (%) | |||
| Cardiovascular disease | 42 (16.0) | 49 (18.3) | 0.424 |
| Cerebrovascular accident | 3 (1.1) | 3 (1.1) | 1.000 |
| Diabetes | 16 (5.9) | 16 (5.9) | 1.000 |
| Current medications. N (%) | |||
| Cholesterol-lowering | 23 (8.7) | 32 (12.5) | 0.202 |
| Antihypertensives | 44 (18.1) | 56 (24.2) | 0.187 |
| Health-related quality of life (SF-12). N (%) | |||
| Physical component summary | 48.6 ± 9.3 | 47.3 ± 10.1 | 0.057 |
| Mental component summary | 51.2 ± 10.1 | 52.1 ± 8.8 | 0.120 |
| International Physical Activity Questionnaire. N (%) | 0.182 | ||
| Inactive | 56 (19.8) | 44 (15.3) | |
| Minimally active | 68 (24.6) | 85 (29.6) | |
| Active | 163 (55.6) | 158 (55.1) | |
| Dietary Patterns | Factor Loadings 1 | Assigned Name | Variance Explained (%) | |
|---|---|---|---|---|
| Food Groups | Factor Loadings | |||
| Component 1 | High-energy drinks | 0.37 | Caloric | 7.6 |
| Processed meats | 0.35 | |||
| Precooked food | 0.35 | |||
| Pizza | 0.32 | |||
| Salty snacks | 0.31 | |||
| Mayonnaise and ketchup | 0.26 | |||
| Sweets | 0.26 | |||
| Wine | −0.25 | |||
| Component 2 | Refined grains | 0.39 | Frieds | 6.9 |
| Fried meats | 0.38 | |||
| Fried potatoes | 0.35 | |||
| Fried fishes | 0.28 | |||
| Whole-fat dairy products | 0.27 | |||
| Sunflower oil | 0.20 | |||
| Sweets | 0.20 | |||
| Low-fat dairy products | −0.20 | |||
| Whole grains | −0.37 | |||
| Component 3 | Fruits | 0.45 | Fruits, vegetables, and dairy products | 5.8 |
| Tea, herbal tea | 0.33 | |||
| Honey | 0.32 | |||
| Vegetables | 0.31 | |||
| Nuts | 0.30 | |||
| Olive oil | 0.27 | |||
| Sweets | 0.22 | |||
| Low-fat dairy products | 0.20 | |||
| Whole grains | 0.20 | |||
| Component 4 | Beer | 0.51 | Alcohol | 5.1 |
| Liquors | 0.51 | |||
| Wine | 0.35 | |||
| Coffee | 0.29 | |||
| Olive oil | 0.25 | |||
| Processed meats | 0.23 | |||
| Component 5 | Cooked, steamed, roasted meats | 0.48 | Fish and boiled meals | 4.9 |
| Boiled potatoes | 0.32 | |||
| Legumes | 0.29 | |||
| Vegetables | 0.28 | |||
| Boiled fishes and seafood | 0.27 | |||
| Fried or scrambled eggs | 0.26 | |||
| Boiled or poached eggs | 0.22 | |||
| Sunflower oil | 0.21 | |||
| Fried fishes | 0.20 | |||
| Dietary Pattern | T1 | T2 | T3 |
|---|---|---|---|
| Caloric | |||
| High-energy drinks | 0.47 | 1.61 | 5.08 |
| Processed meats | 1.21 | 2.51 | 4.29 |
| Precooked food | 0.00 | 0.02 | 0.51 |
| Pizza | 0.01 | 0.05 | 0.55 |
| Salty snacks | 0.04 | 0.21 | 1.00 |
| Mayonnaise and ketchup | 0.10 | 0.38 | 1.82 |
| Sweets | 6.96 | 11.74 | 15.94 |
| Wine | 5.48 | 2.68 | 1.36 |
| Frieds | |||
| Refined grains | 12.29 | 17.82 | 21.11 |
| Fried meats | 0.42 | 0.98 | 2.79 |
| Fried potatoes | 0.64 | 1.27 | 2.70 |
| Fried fishes | 0.59 | 1.30 | 1.84 |
| Whole-fat dairy products | 6.68 | 9.48 | 13.94 |
| Sunflower oil | 0.66 | 1.24 | 2.64 |
| Sweets | 8.63 | 10.80 | 15.26 |
| Low-fat dairy products | 11.88 | 8.30 | 6.19 |
| Whole grains | 4.98 | 0.81 | 0.43 |
| Fruits, vegetables, and dairy products | |||
| Fruits | 5.00 | 10.91 | 14.33 |
| Tea. herbal tea | 0.73 | 1.43 | 4.46 |
| Honey | 0.01 | 0.18 | 1.24 |
| Vegetables | 5.19 | 7.24 | 9.92 |
| Nuts | 0.37 | 0.98 | 1.81 |
| Olive oil | 6.75 | 10.09 | 11.26 |
| Sweets | 9.06 | 11.57 | 14.07 |
| Low-fat dairy products | 6.34 | 8.76 | 11.14 |
| Whole grains | 0.91 | 1.65 | 3.58 |
| Alcohol | |||
| Beer | 0.16 | 0.60 | 3.53 |
| Liquors | 0.02 | 0.12 | 0.86 |
| Wine | 0.65 | 2.05 | 6.65 |
| Coffee | 3.22 | 7.01 | 9.16 |
| Olive oil | 7.16 | 10.07 | 10.90 |
| Processed meats | 2.01 | 2.64 | 3.39 |
| Fish and boiled meals | |||
| Cooked, steamed, roasted meats | 2.75 | 4.11 | 6.12 |
| Boiled potatoes | 1.59 | 2.03 | 3.10 |
| Legumes | 0.50 | 0.70 | 1.38 |
| Vegetables | 5.82 | 7.06 | 9.48 |
| Boiled fishes and seafood | 1.56 | 1.83 | 3.00 |
| Fried or scrambled eggs | 1.11 | 1.63 | 1.86 |
| Boiled or poached eggs | 0.64 | 1.05 | 1.24 |
| Sunflower oil | 0.96 | 1.49 | 2.09 |
| Fried fishes | 1.03 | 1.09 | 1.61 |
| Intervention Group | Control Group | Adjusted Mean Differences | p-Value | ICC | |||
|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | Baseline | 6 Months | ||||
| Caloric | −0.104 (−0.274, 0.066) | −0.597 (−0.740, 0.455) | 0.106 (−0.096, 0.307) | −0.015 (−0.189, 0.159) | −0.443 (−0.667, −0.220) | <0.001 | 0.348 |
| Frieds | −0.158 (−0.342, 0.025) | −0.635 (−0.788, 0.482) | 0.174 (−0.342, 0.025) | −0.085 (−0.256, 0.087) | −0.376 (−0.606, −0.146) | 0.001 | 0.389 |
| Fruits, vegetables, and dairy products | 0.165 (−0.006, 0.336) | 0.462 (0.274, 0.650) | −0.168 (−0.321, 0.015) | −0.291 (−0.471, −0.111) | 0.545 (0.297, 0.793) | <0.001 | 0.352 |
| Alcohol | 0.009 (−0.140, 0.159) | −0.278 (−0.390, 0.166) | −0.009 (−0.167, 0.147) | −0.201 (−0.348, −0.054) | −0.106 (−0.271, 0.058) | 0.205 | 0.212 |
| Fish and boiled meals | −0.032 (−0.181, 0.116) | 0.279 (0.120. 0.438) | 0.032 (−0.122, 0.185) | −0.184 (−0.345, −0.023) | 0.491 (0.223, 0.759) | <0.001 | 0.433 |
| Change in Food Pattern Score 1 | Coefficient (95% CI) | p |
|---|---|---|
| Caloric | 0.146 (−0.030, 0.332) | 0.103 |
| Frieds | 0.240 (0.050, 0.429) | 0.013 |
| Fruits, vegetables, and dairy products | −0.184 (−0.379, 0.012) | 0.063 |
| Alcohol | 0.026 (−0.185, 0.237) | 0.812 |
| Fish and boiled meals | −0.099 (−0.262, 0.064) | 0.234 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo-Malvar, M.; Benítez-Estévez, A.J.; Leis, R.; Sánchez-Castro, J.; Gude, F. Changes in Dietary Patterns through a Nutritional Intervention with a Traditional Atlantic Diet: The Galiat Randomized Controlled Trial. Nutrients 2021, 13, 4233. https://doi.org/10.3390/nu13124233
Calvo-Malvar M, Benítez-Estévez AJ, Leis R, Sánchez-Castro J, Gude F. Changes in Dietary Patterns through a Nutritional Intervention with a Traditional Atlantic Diet: The Galiat Randomized Controlled Trial. Nutrients. 2021; 13(12):4233. https://doi.org/10.3390/nu13124233
Chicago/Turabian StyleCalvo-Malvar, Mar, Alfonso J. Benítez-Estévez, Rosaura Leis, Juan Sánchez-Castro, and Francisco Gude. 2021. "Changes in Dietary Patterns through a Nutritional Intervention with a Traditional Atlantic Diet: The Galiat Randomized Controlled Trial" Nutrients 13, no. 12: 4233. https://doi.org/10.3390/nu13124233
APA StyleCalvo-Malvar, M., Benítez-Estévez, A. J., Leis, R., Sánchez-Castro, J., & Gude, F. (2021). Changes in Dietary Patterns through a Nutritional Intervention with a Traditional Atlantic Diet: The Galiat Randomized Controlled Trial. Nutrients, 13(12), 4233. https://doi.org/10.3390/nu13124233