
Differences in Multi-Faceted Lifestyles in Response to the COVID-19 Pandemic and Their Association with Depression and Quality of Life of Older Adults in South Korea: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Questionnaire
2.2.1. Sociodemographic Data
2.2.2. Lifestyle
2.2.3. Depression
2.2.4. Quality of Life
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Data of the Study Participants
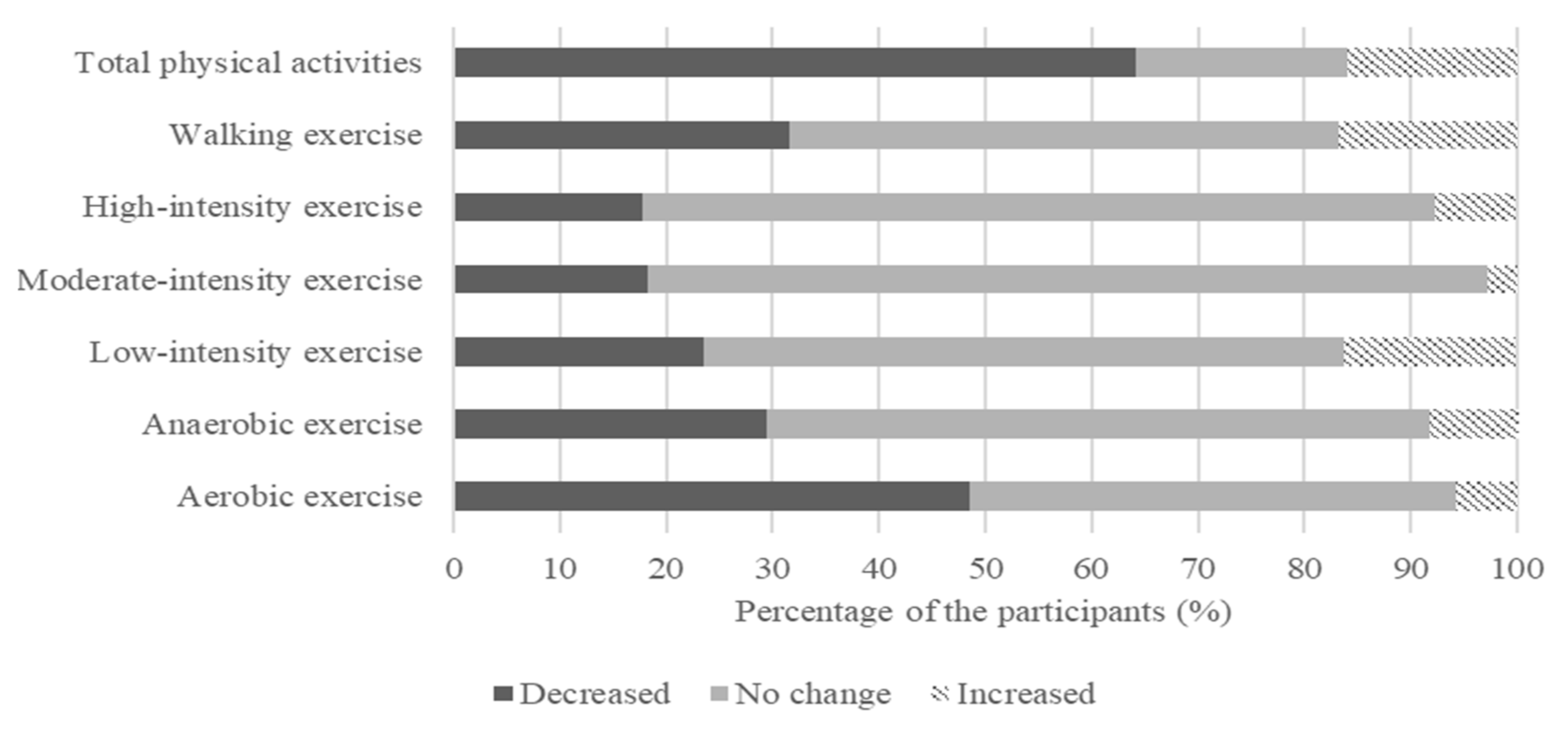
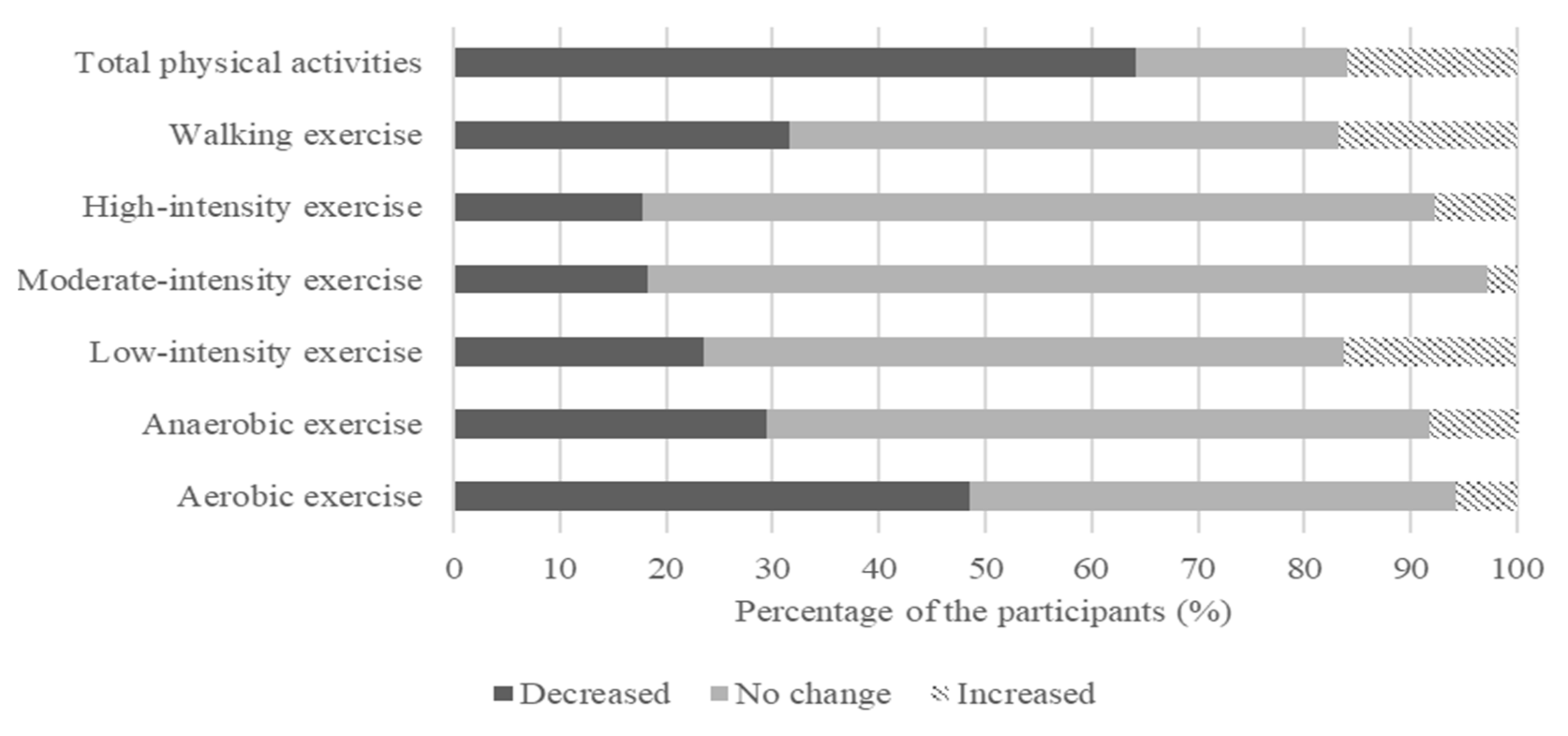
3.2. Effect of the COVID-19 Pandemic on Physical Activity
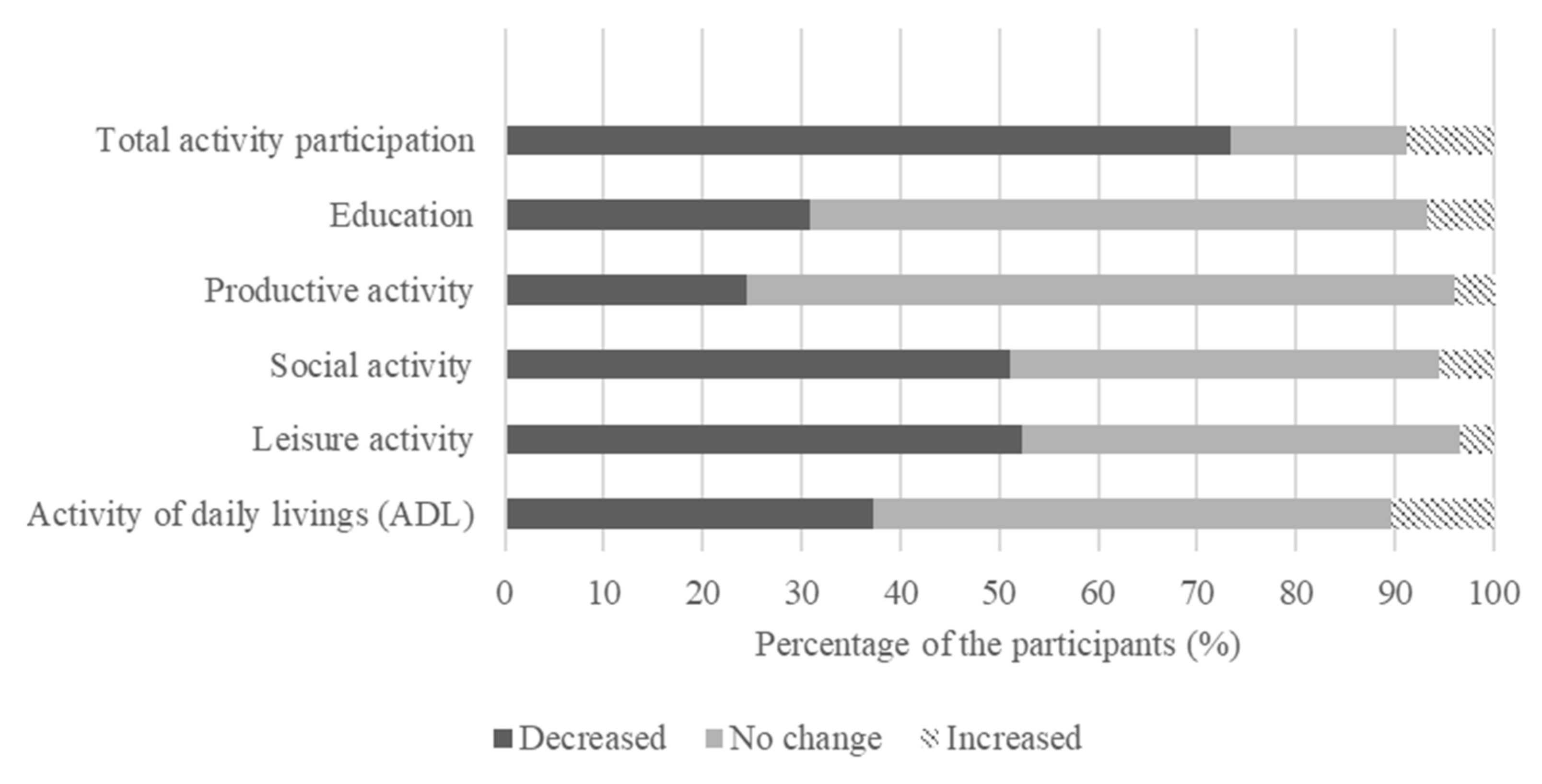
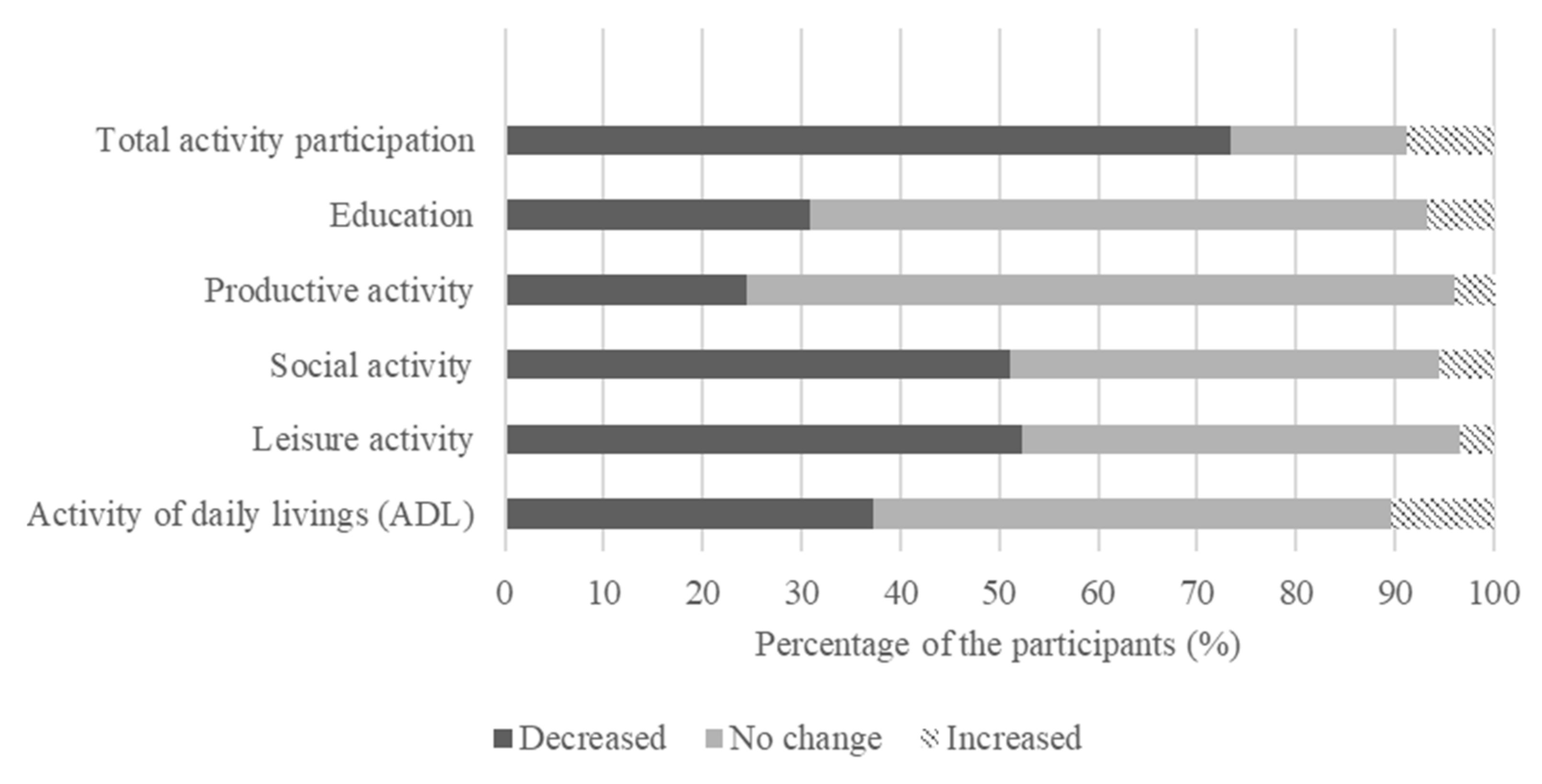
3.3. Effect of the outbreak of COVID-19 Pandemic on Activity Participation
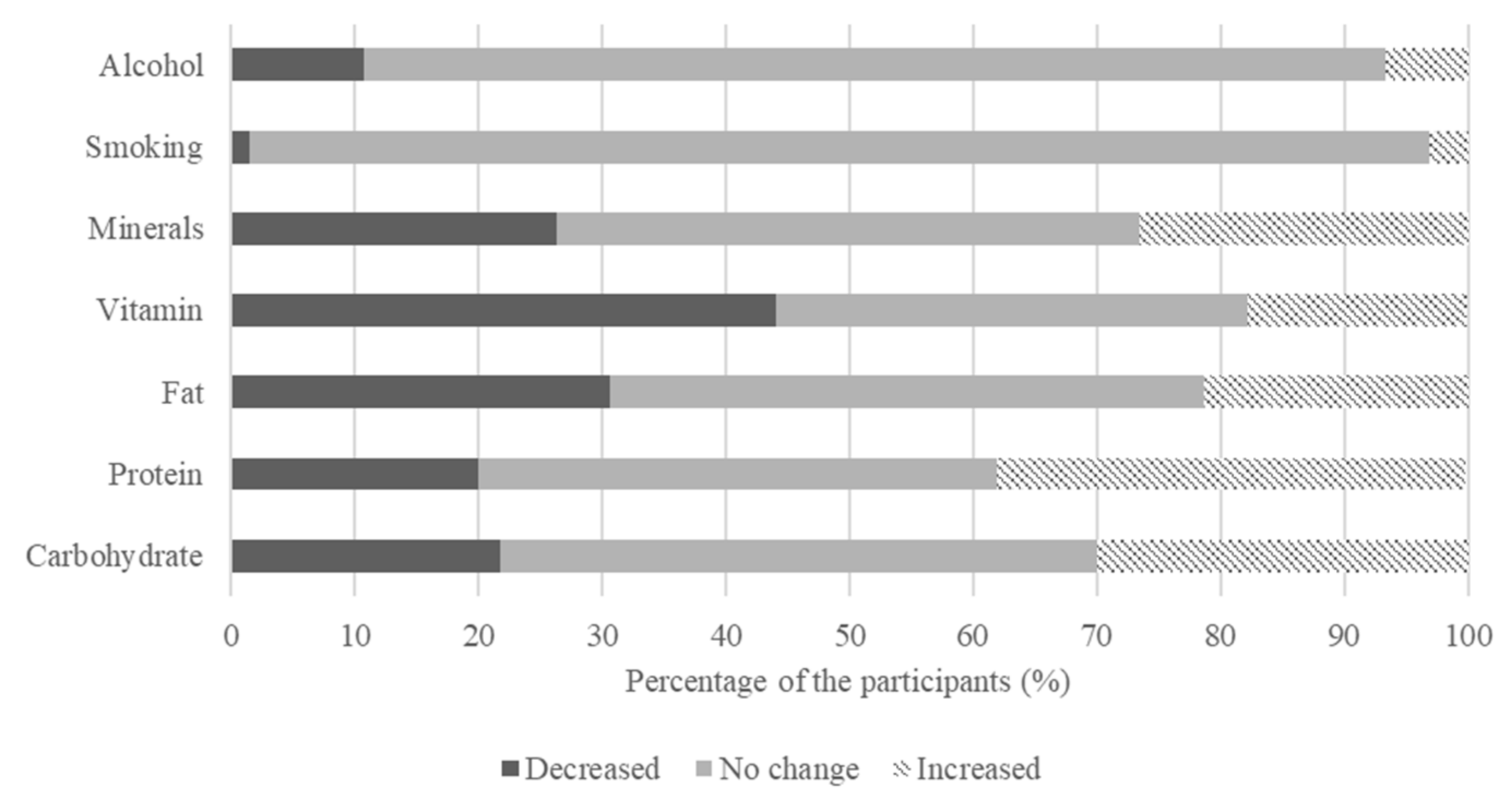
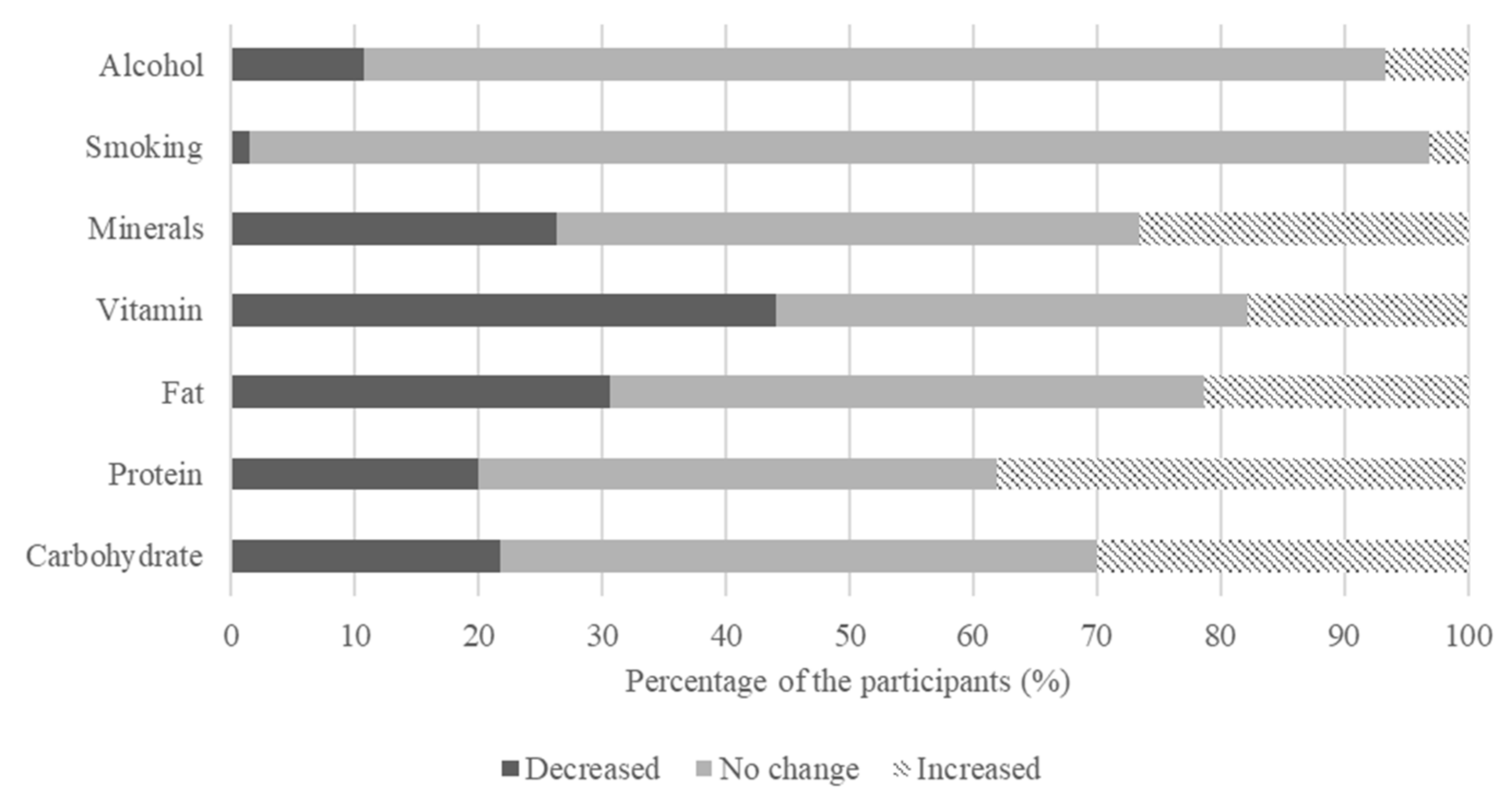
3.4. Effect of the COVID-19 Pandemic on Nutrition
3.5. Associations between Differences in Lifestyle and Psychological Health
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. The Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Bio Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency (KDCA). Coronavirus Disease-19, Confirmed Cases in Republic of Korea. 2021. Available online: http://ncov.mohw.go.kr/ (accessed on 18 August 2021).
- World Health Organization (WHO). Coronavirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/ (accessed on 18 August 2021).
- Celorio-Sardà, R.; Comas-Basté, O.; Latorre-Moratalla, M.L.; Zerón-Rugerio, M.F.; Urpi-Sarda, M.; Illán-Villanueva, M.; Vidal-Carou, M.D.C. Effect of COVID-19 lockdown on dietary habits and lifestyle of food science students and professionals from Spain. Nutrients 2021, 13, 1494. [Google Scholar] [CrossRef]
- Banerjee, D.; Rai, M. Social isolation in Covid-19: The impact of loneliness. Int. J. Soc. Psychiatry 2020, 66, 525–527. [Google Scholar] [CrossRef]
- Yang, X.Y.; Peng, S.; Yang, T.; Cottrell, R.R. Changing trends of mental and behavioral responses and associations during the COVID-19 epidemic in China: A panel study. Health Educ. Res. 2021, 36, 151–158. [Google Scholar] [CrossRef]
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.E.; Sani, G. Will nothing be the same again? Changes in lifestyle during COVID-19 Pandemic and consequences on mental health. Int. J. Environ. Res. Public Health 2021, 18, 8433. [Google Scholar] [CrossRef]
- Balanzá–Martínez, V.; Atienza–Carbonell, B.; Kapczinski, F.; De Boni, R.B. Lifestyle behaviours during the COVID-19–time to connect. Acta Psychiatr. Scand. 2020, 141, 399–400. [Google Scholar] [CrossRef]
- Yang, M.A.; Lim, S.J.; Han, D.S.; Park, J.H. Policy proposal for improving the quality of life for middle-aged people: Focusing on lifestyle. J. Korean Gerontol. Soc. 2020, 40, 351–541. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Healthy Living: What is a Healthy Lifestyle? Copenhagen: WHO Regional Office for Europe. 1999. Available online: https://apps.who.int/iris/handle/10665/108180 (accessed on 19 August 2021).
- Park, K.H.; Han, D.S.; Park, H.Y.; Ha, S.M.; Park, J.H. Pilot research for development of multi-faceted lifestyle profile components affecting health and quality of life: Delphi survey. Korea J. Occup. Ther. 2019, 27, 105–120. [Google Scholar] [CrossRef]
- Lange, K.W.; Nakamura, Y. Lifestyle factors in the prevention of COVID-19. Glob. Health J. 2020, 4, 146–152. [Google Scholar] [CrossRef]
- Chon, K.K.; Rhee, M.K. Preliminary development of Korean Version of CES-D. Korean J. Clin. Psychol. 1992, 11, 65–76. [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Min, S.K.; Kim, K.I.; Jung, Y.C.; Suh, S.Y.; Kim, D.K. Development of Korean version of world health organization quality of life scale abbreviated version (WHOQOL-BREF). J. Korean Neuropsychiatr. Assoc. 2000, 39, 571–579. [Google Scholar]
- WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Goethals, L.; Barth, N.; Guyot, J.; Hupin, D.; Celarier, T.; Bongue, B. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: Qualitative interview study. JMIR Aging 2020, 3, e19007. [Google Scholar] [CrossRef]
- Rodríguez, M.Á.; Crespo, I.; Olm Edillas, H. Exercising in times of COVID-19: What do experts recommend doing within four walls? Rev. Esp. Cardiol. 2020, 73, 527. [Google Scholar] [CrossRef]
- Pizarro-Pennarolli, C.; Sánchez-Rojas, C.; Torres-Castro, R.; Vera-Uribe, R.; Sanchez-Ramirez, D.C.; Vasconcello-Castillo, L.; Rivera-Lillo, G. Assessment of activities of daily living in patients post COVID-19: A systematic review. PeerJ 2021, 9, e11026. [Google Scholar] [CrossRef]
- Tavares, L.M.; Marinho, A. Leisure and COVID-19: Reflections on Brazilian older adults who frequent urban public parks. World Leis. J. 2021, 63, 229–243. [Google Scholar] [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during a strict lockdown: Trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc. Sci. Med. 2020, 265, 113521. [Google Scholar] [CrossRef]
- Richter, L.; Heidinger, T. Caught between two fronts: Successful aging in the time of COVID-19. Work. Older People 2020, 24, 273–280. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and lifestyle changesduring COVID-19 and the subsequent lockdowns among Polish adults: A cross-sectional online survey PLifeCOVID-19 study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Millen, B.E.; Ohls, J.C.; Ponza, M.; McCool, A.C. The elderly nutrition program: An effective national framework for preventive nutrition interventions. J. Am. Diet. Assoc. 2002, 102, 234–240. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Rosenbaum, S.; Richards, J.; Ward, P.B.; Veronese, N.; Stubbs, B. Exercise for depression in older adults: A meta-analysis of randomized controlled trials adjusting for publication bias. Braz. J. Psychiatry 2016, 38, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Heydarnejad, S.; Dehkordi, A.H. The effect of an exercise program on the health-quality of life in older adults. Dan. Med. Bull. 2010, 57, 113–117. [Google Scholar]
- Roh, H.W.; Hong, C.H.; Lee, Y.; Oh, B.H.; Lee, K.S.; Chang, K.J.; Son, S.J. Participation in physical, social, and religious activity and risk of depression in the elderly: A community-based three-year longitudinal study in Korea. PLoS ONE 2015, 10, e0132838. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, M.; Nagasawa, J.; Yoshino, A.; Hiramatsu, K.; Kurashiki, K. Effects of activity participation of the elderly on quality of life. Yonago Acta Med. 2003, 46, 17–24. [Google Scholar]
- Lee, S.J.; Kim, Y.S.; Cho, M.S. A study on dietary habits and food intakes in adults aged 50 or older according to depression status. J. Nutr. Health 2014, 47, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Ju, J.H.; Kim, K.H.; Kim, M.M.; Lim, S.H. Influence of the Eating Attitude and a Well-being Behavior’s Perception of Elderly People on the Subjective Quality of Life and Life Satisfaction. J. Wellness 2017, 12, 15–26. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare Health Plan 2020. 2016. Available online: http://www.mohw.go.kr/react/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=0319&CONT_SEQ=330479&page=1 (accessed on 14 September 2021).
- Shin, H.R.; Yun, T.Y.; Kim, S.K.; Kim, Y.S. An Exploratory Study on Changes in Daily Life of the Elderly amid COVID-19—Focusing on Technology Use and Restrictions on Participation in Elderly Welfare Centers-. Korean J. Gerontol. Soc. Welf. 2020, 75, 207–232. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | N | Percentage or Mean (SD) |
|---|---|---|
| Gender | ||
| Male | 161 | 49.2 |
| Female | 166 | 50.8 |
| Age | 327 | 60.40(4.60) |
| Age group | ||
| 55–59 | 163 | 49.8 |
| 60–69 | 150 | 45.9 |
| >70 | 14 | 4.3 |
| Years of Education | ||
| 0 (no formal education) | 1 | 0.3 |
| 1–6 (elementary) | 1 | 0.3 |
| 7–9 (middle school) | 7 | 2.2 |
| 10–12 (high school) | 74 | 22.6 |
| >13 (college or University) | 244 | 76.6 |
| Retirement status | ||
| Yes | 162 | 49.5 |
| No | 165 | 50.5 |
| Living Alone | ||
| Yes | 25 | 7.6 |
| No | 302 | 92.4 |
| Chronic disease status | ||
| Yes | 174 | 53.2 |
| No | 153 | 46.8 |
| Pre | Post | t (95% CI) | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Aerobic exercise | 2.84 (1.10) | 2.17 (1.15) | 11.60 (0.56–0.79) *** |
| Anaerobic exercise | 2.08 (1.08) | 1.77 (0.98) | 5.59 (0.20–0.42) *** |
| Low-intensity exercise | 2.96 (1.13) | 2.83 (1.16) | 2.62 (0.03–0.23) ** |
| Moderate-intensity exercise | 1.49 (0.82) | 1.24 (0.53) | 6.19 (0.17–0.32) *** |
| High-intensity exercise | 1.66 (0.93) | 1.54 (0.91) | 3.07 (0.04–0.20) ** |
| Walking exercise | 3.23 (1.12) | 2.99 (1.14) | 4.16 (0.12–0.35) *** |
| Total physical activity | 2.38 (0.63) | 2.09 (0.58) | 9.97 (0.23–0.34) *** |
| Pre | Post | t (95% CI) | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Activities of daily living | 3.52 (1.03) | 3.09 (1.16) | 7.52 (0.31–0.53) *** |
| Leisure activity | 1.98 (0.85) | 1.37 (0.72) | 13.92 (0.53–0.69) *** |
| Social activity | 2.03 (0.84) | 1.47 (0.75) | 11.90 (0.46–0.65) *** |
| Productive activity | 2.99 (1.30) | 2.63 (1.38) | 7.23 (0.26–0.46) *** |
| Education | 1.71 (0.81) | 1.42 (0.76) | 6.72 (0.20–0.37) *** |
| Total activity participation | 2.44 (0.53) | 2.00 (0.56) | 15.58 (0.39–0.50) *** |
| Pre | Post | t (95% CI) | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Carbohydrate | 2.88 (0.55) | 2.92 (0.58) | −1.82 (−0.09–0.00) |
| Protein | 2.55 (0.68) | 2.66 (0.66) | −4.45 (−0.15–0.06) *** |
| Fats | 2.29 (0.66) | 2.24 (0.68) | 2.30 (0.01–0.89) * |
| Vitamins | 3.24 (0.76) | 3.06 (0.76) | 6.56 (0.13–0.23) *** |
| Minerals | 2.37 (0.78) | 2.41 (0.78) | −1.51 (−0.80–0.01) |
| Total intake of five nutrients | 2.67(0.50) | 2.66(0.52) | 0.657(−0.02–0.04) |
| Smoking | 1.53 (1.27) | 1.54 (1.28) | −0.60 (−0.05–0.03) |
| Alcohol | 1.74 (0.91) | 1.70 (0.91) | 1.50 (−0.01–0.09) |
| Depression | Quality of Life | |
|---|---|---|
| Logistic Regression-Odd Ratio (95% CI) | ||
| Physical activity | 0.977 (0.955–1.001) | 1.473 (1.033–2.099) * |
| Activity participation | 0.960 (0.934–0.987) ** | 1.847(1.247–2.737) ** |
| Nutrition | 0.974(0.953–0.996) * | 1.684 (1.185–2.392) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.-H.; Kim, A.-R.; Yang, M.-A.; Park, J.-H. Differences in Multi-Faceted Lifestyles in Response to the COVID-19 Pandemic and Their Association with Depression and Quality of Life of Older Adults in South Korea: A Cross-Sectional Study. Nutrients 2021, 13, 4124. https://doi.org/10.3390/nu13114124
Park K-H, Kim A-R, Yang M-A, Park J-H. Differences in Multi-Faceted Lifestyles in Response to the COVID-19 Pandemic and Their Association with Depression and Quality of Life of Older Adults in South Korea: A Cross-Sectional Study. Nutrients. 2021; 13(11):4124. https://doi.org/10.3390/nu13114124
Chicago/Turabian StylePark, Kang-Hyun, Ah-Ram Kim, Min-Ah Yang, and Ji-Hyuk Park. 2021. "Differences in Multi-Faceted Lifestyles in Response to the COVID-19 Pandemic and Their Association with Depression and Quality of Life of Older Adults in South Korea: A Cross-Sectional Study" Nutrients 13, no. 11: 4124. https://doi.org/10.3390/nu13114124
APA StylePark, K.-H., Kim, A.-R., Yang, M.-A., & Park, J.-H. (2021). Differences in Multi-Faceted Lifestyles in Response to the COVID-19 Pandemic and Their Association with Depression and Quality of Life of Older Adults in South Korea: A Cross-Sectional Study. Nutrients, 13(11), 4124. https://doi.org/10.3390/nu13114124