
Stress Responsiveness and Emotional Eating Depend on Youngsters’ Chronic Stress Level and Overweight

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Sample
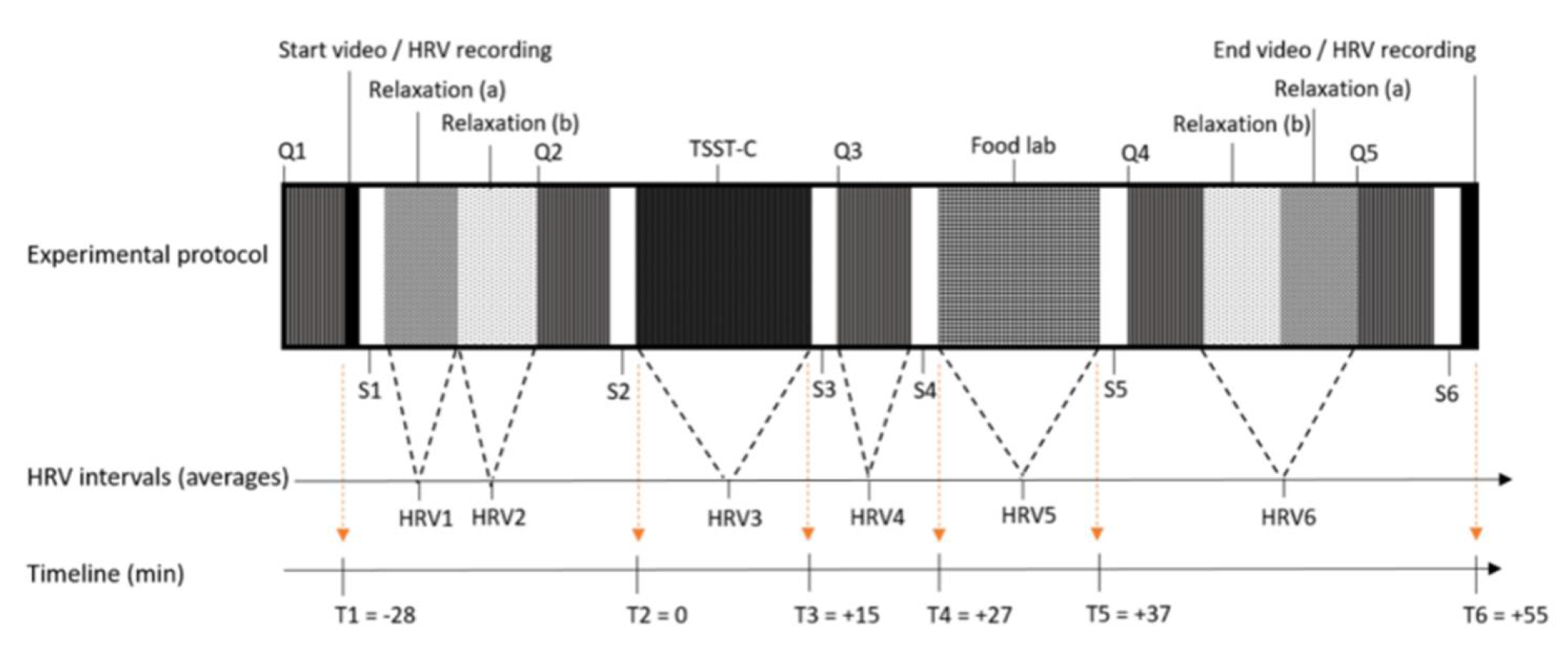
2.2. Experimental Design
2.3. Stress Manipulation
2.4. Response to the Stressor: Overall Responsiveness, Stress Reactivity, and Stress Recovery
2.4.1. Salivary Cortisol and Alpha-Amylase
2.4.2. Heart Rate Variability
2.4.3. Mood and Self-Reported Stress
2.5. Snack Liking/Wanting Score and Snack Buffet Intake during the Food Lab
2.5.1. Snack Categories
2.5.2. Liking and Wanting Score
2.5.3. Snack Buffet Intake
2.6. Weight and Chronic Stress Level as Predictor
2.6.1. Body Composition Measures
2.6.2. Chronic Stress Level
2.7. Trait Emotional Eating
2.8. Statistical Analyses
3. Results
3.1. Descriptive Data and Intervention Check
3.2. Stress Reactivity/Recovery in Relation to Chronic Stress and Weight Status
3.3. Food Lab Responses in Relation to Chronic Stress and Weight Status
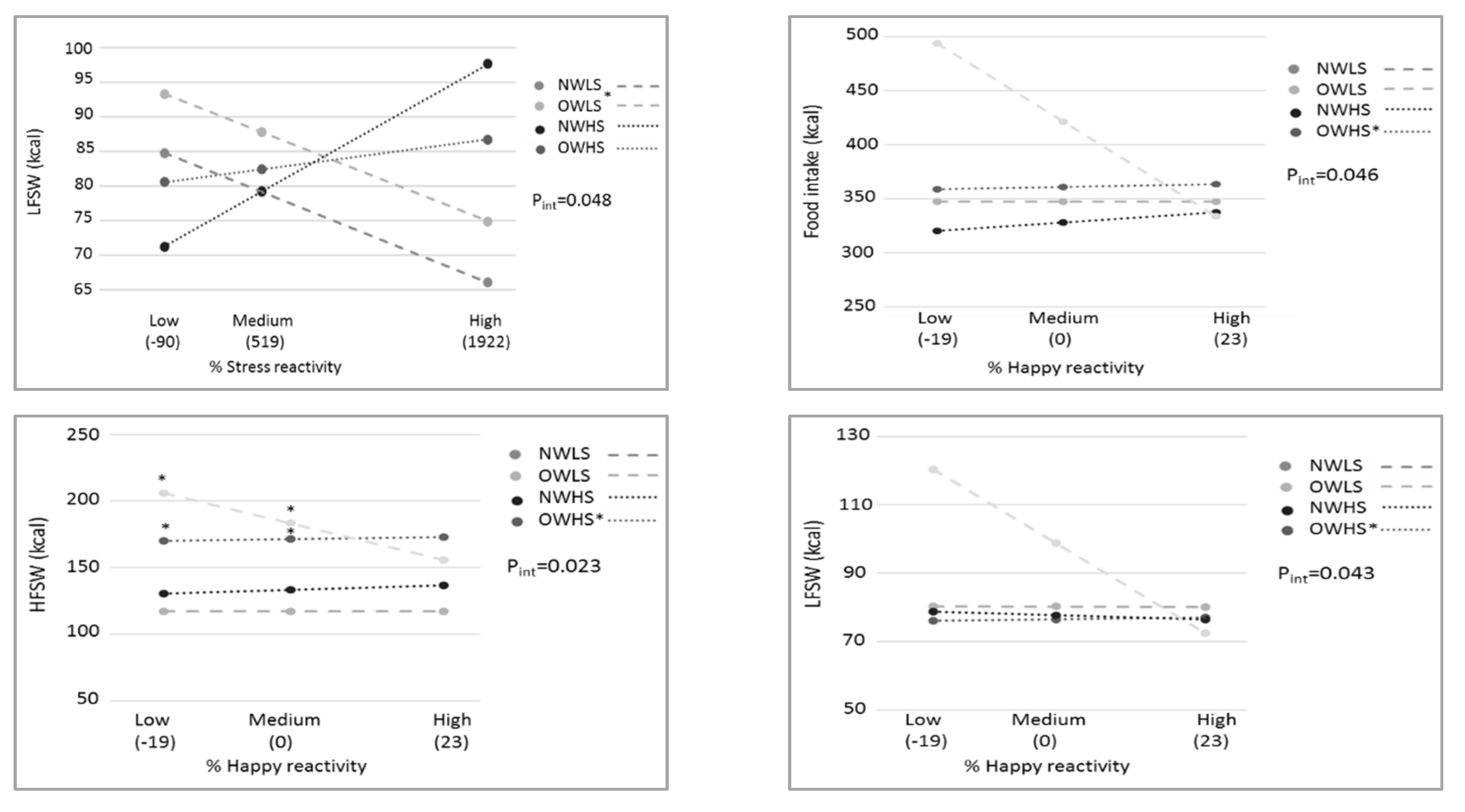
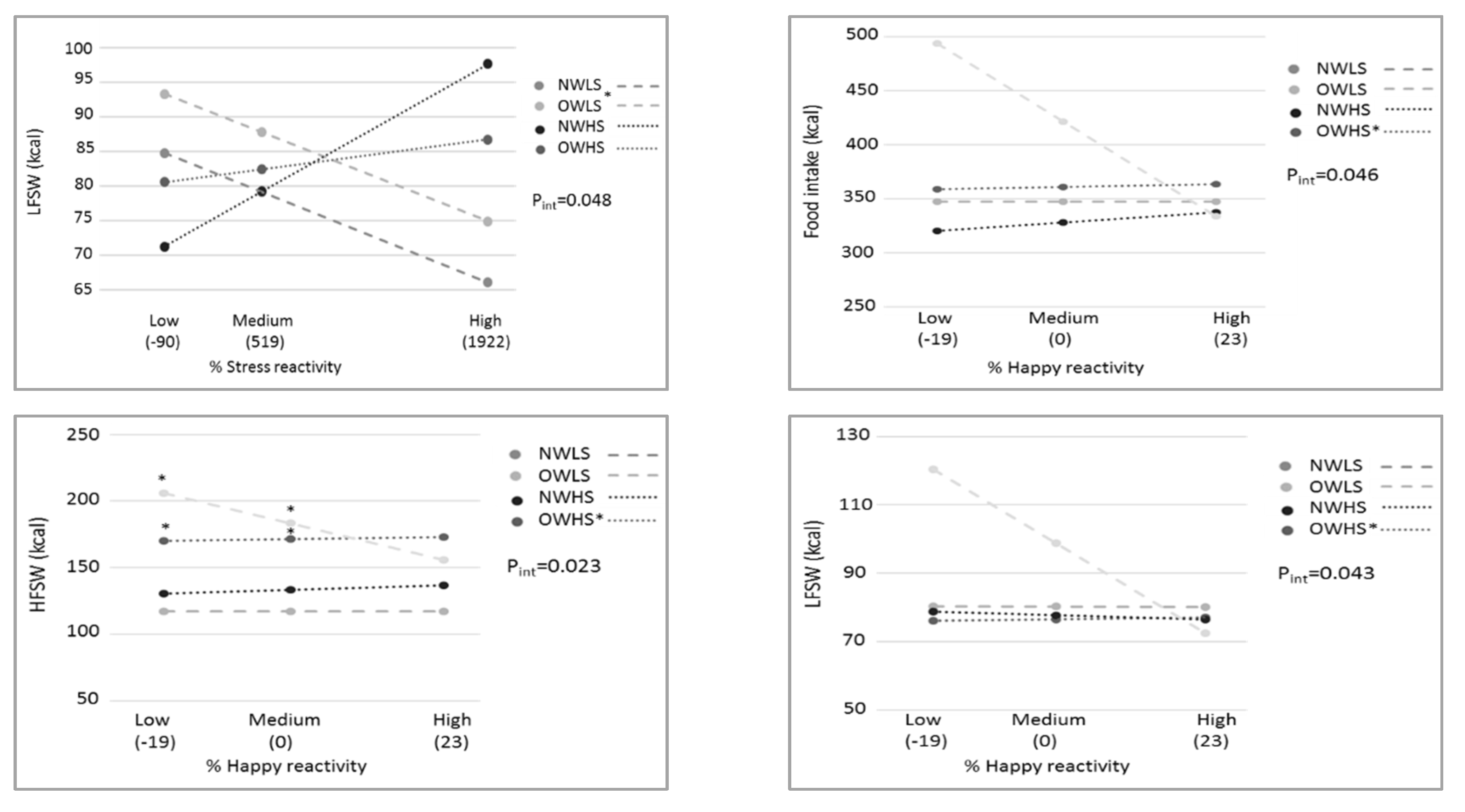
3.4. Stress Responsiveness as Moderator
3.5. Interrelations between Stress Reactivity/Recovery and Food Lab Responses
3.6. The Role of Trait Emotional Eating
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!) Guidance to Support Country Implementation; WHO: Geneva, Switzerland, 2017; Volume 9, 176p. [Google Scholar]
- Childhood Obesity Facts|Overweight & Obesity|CDC. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 19 January 2021).
- Hill, D.C.; Moss, R.H.; Sykes-Muskett, B.; Conner, M.; O’Connor, D.B. Stress and eating behaviors in children and adolescents: Systematic review and meta-analysis. Appetite 2018, 123, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B. The effect of obesity on health outcomes. Mol. Cell. Endocrinol. 2010, 316, 104–108. [Google Scholar] [CrossRef]
- Charmandari, E.; Tsigos, C.; Chrousos, G. Endocrinology of the stress response. Annu. Rev. Physiol. 2005, 67, 259–284. [Google Scholar] [CrossRef]
- Pervanidou, P.; Chrousos, G.P. Metabolic consequences of stress during childhood and adolescence. Metabolism. 2012, 61, 611–619. [Google Scholar] [CrossRef]
- Bae, Y.J.; Stadelmann, S.; Klein, A.M.; Jaeger, S.; Hiemisch, A.; Kiess, W.; Ceglarek, U.; Gaudl, A.; Schaab, M.; von Klitzing, K.; et al. The hyporeactivity of salivary cortisol at stress test (TSST-C) in children with internalizing or externalizing disorders is contrastively associated with α-amylase. J. Psychiatr. Res. 2015, 71, 78–88. [Google Scholar] [CrossRef]
- Pervanidou, P.; Chrousos, G.P. Stress and Pediatric Obesity: Neurobiology and Behavior. Fam. Relat. 2016, 65, 85–93. [Google Scholar] [CrossRef]
- Vainik, U.; Neseliler, S.; Konstabel, K.; Fellows, L.K.; Dagher, A. Eating traits questionnaires as a continuum of a single concept. Uncontrolled eating. Appetite 2015, 90, 229–239. [Google Scholar] [CrossRef]
- Dalton, M.; Blundell, J.; Finlayson, G.S. Examination of food reward and energy intake under laboratory and free-living conditions in a trait binge eating subtype of obesity. Front. Psychol. 2013, 4, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debeuf, T.; Verbeken, S.; Van Beveren, M.L.; Michels, N.; Braet, C. Stress and eating behavior: A daily diary study in youngsters. Front. Psychol. 2018, 9, 2657. [Google Scholar] [CrossRef]
- Rajcani, J.; Solarikova, P.; Turonova, D.; Brezina, I.; Rajčáni, J. Heart Rate Variability in Psychosocial Stress: Comparison Between Laboratory and Real-Life Setting. Act. Nerv. Super. Rediviva 2016, 58, 77–82. [Google Scholar]
- Hofmann, J.; Meule, A.; Reichenberger, J.; Weghuber, D.; Ardelt-Gattinger, E.; Blechert, J. Crave, like, eat: Determinants of food intake in a sample of children and adolescents with a wide range in body mass. Front. Psychol. 2016, 7. [Google Scholar] [CrossRef] [Green Version]
- Michels, N.; Sioen, I.; Boone, L.; Clays, E.; Vanaelst, B.; Huybrechts, I.; De Henauw, S. Cross-lagged associations between children’s stress and adiposity: The children’s body composition and stress study. Psychosom. Med. 2015, 77, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Pervanidou, P.; Chrousos, G.P. Stress and obesity/metabolic syndrome in childhood and adolescence. Int. J. Pediatr. Obes. 2011, 6, 21–28. [Google Scholar] [CrossRef]
- Roemmich, J.N.; Lambiase, M.J.; Lobarinas, C.L.; Balantekin, K.N. Interactive effects of dietary restraint and adiposity on stress-induced eating and the food choice of children. Eat. Behav. 2011, 12, 309–312. [Google Scholar] [CrossRef]
- Blechert, J.; Meule, A.; Busch, N.A.; Ohla, K. Food-pics: An image database for experimental research on eating and appetite. Front. Psychol. 2014, 5, 1–10. [Google Scholar] [CrossRef]
- Klosowska, J.C.; Verbeken, S.; Braet, C.; Wijnant, K.; Debeuf, T.; De Henauw, S.; Michels, N. The Moderating Role of Emotion Regulation in the Association between Stressors with Psychological and Biological Measures in Adolescence. Psychosom. Med. 2020, 82, 495–507. [Google Scholar] [CrossRef]
- Roelants, M.; Hauspie, R.; Hoppenbrouwers, K. References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann. Hum. Biol. 2009, 36, 680–694. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. Br. Med. J. 2007, 335, 194–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, M.H. Tanner Stages. In The SAGE Encyclopedia of Lifespan Human Development; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Debeuf, T.; Verbeken, S.; Boelens, E.; Volkaert, B.; Van Malderen, E.; Michels, N.; Braet, C. Emotion regulation training in the treatment of obesity in young adolescents: Protocol for a randomized controlled trial. Trials 2020, 21, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, L.; Van Durme, K.; Van Beveren, M.L.; Claes, L. Do changes in affect moderate the association between attachment anxiety and body dissatisfaction in children? An experimental study by means of the Trier Social Stress Test. Eat. Behav. 2017, 26, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.P.; Kennedy, P.J.; Dockray, S.; Cryan, J.F.; Dinan, T.G.; Clarke, G. The Trier Social Stress Test: Principles and practice. Neurobiol. Stress 2017, 6, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ‘Trier social stress test’-A tool for investigating psychobiological stress responses in a laboratory setting. Proc. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Fekedulegn, D.B.; Andrew, M.E.; Burchfiel, C.M.; Violanti, J.M.; Hartley, T.A.; Charles, L.E.; Miller, D.B. Area under the curve and other summary indicators of repeated waking cortisol measurements. Psychosom. Med. 2007, 69, 651–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michels, N.; Sioen, I.; Braet, C.; Huybrechts, I.; Vanaelst, B.; Wolters, M.; De Henauw, S. Relation between salivary cortisol as stress biomarker and dietary pattern in children. Psychoneuroendocrinology 2013, 38, 1512–1520. [Google Scholar] [CrossRef]
- Dickerson, S.S.; Kemeny, M.E. Acute Stressors and Cortisol Responses: A Theoretical Integration and Synthesis of Laboratory Research. Psychol. Bull. 2004, 130, 355–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DetectX® CORTISOL Enzyme Immunoassay Kit Dried Fecal Extracts, Saliva, Urine, Serum, EDTA and Heparin Plasma and Tissue Culture Media NCalTM International Standard Kit. Available online: www.ArborAssays.com (accessed on 25 August 2020).
- Sigma Aldrich Amylase Activity Assay Kit Sufficient for 100 Colorimetric Tests|Sigma-Aldrich. Available online: https://www.sigmaaldrich.com/catalog/product/sigma/mak009?lang=en®ion=BE (accessed on 13 August 2020).
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Heal. 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Michels, N.; Sioen, I.; Clays, E.; De Buyzere, M.; Ahrens, W.; Huybrechts, I.; Vanaelst, B.; De Henauw, S. Children’s heart rate variability as stress indicator: Association with reported stress and cortisol. Biol. Psychol. 2013, 94, 433–440. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV--heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- About HRV-Kubios HRV. Available online: https://www.kubios.com/about-hrv/#Summary_of_HRV_parameters (accessed on 25 August 2020).
- Laurent, J.; Catanzaro, S.J.; Rudolph, K.D.; Joiner, T.E.; Potter, K.I.; Lambert, S.; Osborne, L.; Gathright, T. A measure of positive and negative affect for children: Scale development and preliminary validation. Psychol. Assess. 1999, 11, 326–338. [Google Scholar] [CrossRef]
- Oliver, G.; Wardle, J.; Gibson, L. Stress and Food Choice: A Laboratory Study. Psychosom. Med. 2000, 62, 853–865. [Google Scholar] [CrossRef]
- Finlayson, G.; King, N.; Blundell, J.E. Is it possible to dissociate ‘liking’ and ‘wanting’ for foods in humans? A novel experimental procedure. Physiol. Behav. 2007, 90, 36–42. [Google Scholar] [CrossRef]
- Finlayson, G.; King, N.; Blundell, J.E. Liking vs. wanting food: Importance for human appetite control and weight regulation. Neurosci. Biobehav. Rev. 2007, 31, 987–1002. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhao, Y.; Li, J.; Dai, J.; Wang, X.; Wang, S. Factor Structure of the 10-Item Perceived Stress Scale and Measurement Invariance Across Genders Among Chinese Adolescents. Front. Psychol. 2020, 11, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, M. Children’s Depression Inventory (CDI2): Technical Manual, 2nd ed.; Multi-Health Systems Inc.: North Tonawanda, NY, USA, 2011. [Google Scholar]
- Bodden, D.; Braet, C.; Stikkelbroek, Y. CDI-2. Screeningsvragenlijst Voor Depressie Bij Kinderen en Jongeren; Hogrefe Uitgevers B.V.: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Michels, N.; Vanaelst, B.; Vyncke, K.; Sioen, I.; Huybrechts, I.; De Vriendt, T.; De Henauw, S. Children’s Body composition and Stress–the ChiBS study: Aims, design, methods, population and participation characteristics. Arch. Public Heal. 2012, 70, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staufenbiel, S.M.; Penninx, B.W.J.H.; Spijker, A.T.; Elzinga, B.M.; van Rossum, E.F.C. Hair cortisol, stress exposure, and mental health in humans: A systematic review. Psychoneuroendocrinology 2013, 38, 1220–1235. [Google Scholar] [CrossRef] [PubMed]
- Sauvé, B.; Koren, G.; Walsh, G.; Tokmakejian, S.; Van Uum, S.H.M. Measurement of cortisol in human hair as a biomarker of systemic exposure. Clin. Investig. Med. 2007, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis Methodology in the Social Sciences; Guilford Publications, Inc.: New York, NY, USA, 2018. [Google Scholar]
- Volkaert, B.; Wante, L.; Van Beveren, M.L.; Vervoort, L.; Braet, C. Training Adaptive Emotion Regulation Skills in Early Adolescents: The Effects of Distraction, Acceptance, Cognitive Reappraisal, and Problem Solving. Cognit. Ther. Res. 2020, 44, 678–696. [Google Scholar] [CrossRef]
- Bongers, P.; Jansen, A. Emotional eating is not what you think it is and emotional eating scales do not measure what you think they measure. Front. Psychol. 2016, 7, 1932. [Google Scholar] [CrossRef] [Green Version]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef] [Green Version]
- Epel, E.; Lapidus, R.; McEwen, B.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2001, 26, 37–49. [Google Scholar] [CrossRef]
- Herhaus, B.; Ullmann, E.; Chrousos, G.; Petrowski, K. High/low cortisol reactivity and food intake in people with obesity and healthy weight. Transl. Psychiatry 2020, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Newman, E.; O’Connor, D.B.; Conner, M. Daily hassles and eating behaviour: The role of cortisol reactivity status. Psychoneuroendocrinology 2007, 32, 125–132. [Google Scholar] [CrossRef]
- Evers, C.; Dingemans, A.; Junghans, A.F.; Boevé, A. Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neurosci. Biobehav. Rev. 2018, 92, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, E.; Canals, J.; Arija, V.; De Henauw, S.; Michels, N. The role of emotion regulation in childhood obesity: Implications for prevention and treatment. Nutr. Res. Rev. 2016, 29, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Galasso, L.; Montaruli, A.; Jankowski, K.S.; Bruno, E.; Castelli, L.; Mulè, A.; Chiorazzo, M.; Ricceri, A.; Erzegovesi, S.; Caumo, A.; et al. Binge eating disorder: What is the role of physical activity associated with dietary and psychological treatment? Nutrients 2020, 12, 3622. [Google Scholar] [CrossRef] [PubMed]
- Everly, G.S.; Lating, J.M. A Clinical Guide to the Treatment of the Human Stress Response; Springer: New York, NY, USA, 2013. [Google Scholar]

{kind=link}
{kind=link}
| Normal Weight and Low Stress n = 52 | Overweight and Low Stress n = 16 | Normal Weight and High Stress n = 46 | Overweight and High Stress n = 23 | Total Sample n = 137 | p-Value Overall Group Difference | |
|---|---|---|---|---|---|---|
| Body mass index z-score | −0.2 ± 0.6 a,b | 1.9 ± 0.7 a,c | −0.0 ± 0.7 c,d | 1.7 ± 0.6 b,d | 0.4 ± 0.4 | <0.001 |
| Weight category (n; % overweight or obese) | 52; 0% a,b | 16; 100% a,c | 46; 0% c,d | 23; 100% b,d | 137; 28.7% | <0.001 |
| Perceived stress scale (0–40) | 12.8 ± 3.5 a,b | 13.8 ± 4.9 c,d | 20.5 ± 4.0 a,c | 20.0 ± 4.0 b,d | 14.2 ± 2.0 | <0.001 |
| Depressive symptoms (0–56) | 5.0 ± 3.4 a,b | 6.0 ± 4.4 c,d | 12.0 ± 6.2 a,c | 14.1 ± 5.2 b,d | 9.0 ± 6.2 | <0.001 |
| Hair cortisol (pg/mg) | 2.1 (1.6; 2.7) a,b | 1.8 (1.6; 2.2) c,d | 3.1 (2.7; 5.8) a,c | 3.7 (2.5; 5.1) b,d | 2.6 (1.9; 3.7) | <0.001 |
| Background | ||||||
| Sex (n; %women) | 20; 38.5% | 8; 50% | 28; 62.2% | 13; 56.5% | 69; 50.7% | 0.121 |
| Age | 14.0 ± 1.6 | 13.2 ± 2.9 a | 14.8 ± 1.6 a | 13.9 ± 2.4 | 14.2 ± 2.0 | 0.030 |
| Tanner stage (n; % prepubertal) | 1; 1.9% | 2; 12.5% | 3; 6.7% | 4; 17.4% | 10; 7.4% | 0.098 |
| Parental education (n; % post-secondary) | 30; 57.7% | 7; 43.8% | 25; 55.6% | 10; 43.5% | 72; 52.9% | 0.580 |
| Trait emotional eating (13–65) | 26.5 ± 13.5 | 25.4 ± 10.6 | 30.6 ± 10.6 | 26.1 ± 10.5 | 27.7 ± 11.8 | 0.245 |
| Stress Parameters at Start | ||||||
| Stress report (1–100) | 6 (1; 13) | 3 (1; 10) | 10 (1; 20) | 10 (1; 28) | 10 (1; 20) | 0.124 |
| Negative emotions report (3–300) | 3 (3; 12) | 3 (3; 7) | 3 (3; 17) | 8 (3; 24) | 3 (3; 15) | 0.271 |
| Happy report (1–100) | 69.9 ± 25.2 | 71.8 ± 20.0 | 63.3 ± 20.8 | 58.4 ± 27.3 | 66.1 ± 23.7 | 0.209 |
| HRV RMSSD (ms) | 51 (36; 77) | 63 (42; 82) | 53 (41; 69) | 48 (34; 34) | 51 (39; 76) | 0.771 |
| HRV stress index | 8.3 ± 3.2 | 3.2 ± 3.6 | 8.1 ± 3.1 | 9.0 ± 2.9 | 8.3 ± 3.1 | 0.835 |
| Salivary cortisol (pg/mL) | 309 (142; 558) a | 553 (249; 734) b | 441 (160; 816) c | 116 (75; 263) a,b,c | 311 (115; 693) | 0.021 |
| Salivary alpha-amylase (nmol/min/mL) | 46,265 ± 18,284 | 35,549 ± 20,108 | 44,776 ± 21,262 | 40,929 ± 17,851 | 43,903 ± 19,562 | 0.306 |
| Food Parameters at Start | ||||||
| Hunger (1–100) | 19.4 ± 21.7 | 5.8 ± 7.4 | 19.3 ± 21.7 | 8.6 ± 13.2 | 16.4 ± 20.2 | 0.038 |
| Liking (12–1200) | 791.9 ± 129.7 a | 617.5 ± 267.0a | 744.2 ± 144.0 | 698.4 ± 142.5 | 743.9 ± 162.3 | 0.003 |
| Wanting (12–1200) | 454.1 ± 244.2 | 366.2 ± 236.4 | 415.2 ± 242.8 | 303.6 ± 159.2 | 410.0 ± 235.8 | 0.114 |
| Normal Weight and Low Stress n = 52 (Mean ± SE) | Overweight and Low Stress n = 16 (Mean ± SE) | Normal Weight and High Stress n = 46 (Mean ± SE) | Overweight and High Stress n = 23 (Mean ± SE) | |
|---|---|---|---|---|
| Stress | ||||
| % Stress reactivity | 557.8 ± 200.8 | 564.9 ± 394.6 | 378.5 ± 214.7 | 725.6 ± 332.2 |
| % Stress recovery | −32.1 ± 25.8 | −39.3 ± 50.6 | 25.3 ± 27.5 | 26.6 ± 42.6 |
| AUCi stress | −37.4 ± 25.6 | −133.6 ± 50.3 | −76.5 ± 27.4 | −77.6 ± 42.4 |
| % Negative emotions reactivity | 19.9 ± 25.7 | 36.2 ± 50.4 | 54.6 ± 27.4 | 76.2 ± 42.4 |
| % Negative emotions recovery | −0.9 ± 13.8 | −15.3 ± 27.1 | 1.0 ± 14.7 | 21.2 ± 22.8 |
| AUCi negative emotions | −33.5 ± 19.2 | −17.4 ± 37.7 | −37.5 ± 20.5 | −61.1 ± 31.7 |
| % Happy reactivity | 160.6 ± 130.3 | 0.2 ± 256.0 | 50.5 ± 139.3 | 332.4 ± 215.6 |
| % Happy recovery | 409.8 ± 148.4 a | 75.0 ± 95.9 | −8.8 ± 176.2 | −26.6 ± 89.7 a |
| AUCi happy | 22.8 ± 27.6 | 13.6 ± 54.2 | −2.1 ± 29.5 | −22.2 ± 46.6 |
| % Stress index reactivity | 0.2 ± 4.2 | 3.2 ± 8.2 | 3.6 ± 4.6 | 5.6 ± 7.6 |
| % Stress index recovery | 2.2 ± 2.6 | −0.9 ± 5.0 | 3.7 ± 2.8 | 4.4 ± 4.6 |
| AUCi Stress index | −2.06 ± 3.3 | −0.29 ± 6.3 | −2.6 ± 3.6 | 4.1 ± 5.8 |
| % RMSSD reactivity | −2.6 ± 6.5 | −11.6 ± 12 | −0.1 ± 7.1 | −10.8 ± 11.6 |
| % RMSSD recovery | 3.4 ± 3.4 | 8.5 ± 6.6 | 7.0 ± 3.7 | 4.6 ± 6.1 |
| AUCi RMSSD | −66.5 ± 36.8 | −74.7 ± 71.1 | −09.1 ± 39.9 | −110.8 ± 65.7 |
| % Salivary cortisol reactivity | 410.9 ± 1561.5 a | 250.4 ± 3249.3 | 137.7 ± 1636.8 b | 7856.9 ± 2710.9 a,b |
| % Salivary cortisol recovery | −49.4 ± 21.5 | −6.9 ± 40.2 | −27.1 ± 22.5 | 28.9 ± 34.0 |
| AUCi Salivary cortisol | −19,806.6 ± 10,924.7 | −9610.8 ± 22,170.7 | −16,225.8 ± 11,752.7 | −6059.5 ± 18,402.6 |
| % Salivary alpha-amylase reactivity | 4.8 ± 2.2 | −2.4 ± 4.3 | 5.2 ± 2.3 | 5.9 ± 3.6 |
| % Salivary alpha-amylase recovery | −4.7 ± 2.7 | −2.0 ± 5.3 | −3.3 ± 2.9 | −4.1 ± 4.5 |
| AUCi salivary alpha-amylase | −11,443.5 ± 1698.7 | −8397.5 ± 33,667.4 | −13,998.6 ± 18,324.7 | 27,116.6 ± 28,351.8 |
| Food Parameters | ||||
| Increase in hunger (1–100) | 13.0 ± 2.3 | 6.7 ± 4.7 | 14.0 ± 3.8 | 12.3 ± 3.8 |
| Increase in wanting (12–1200) | 89.0 ± 19.8 | 85.2 ± 39.6 | 93.0 ± 20.9 | 147.0 ± 32.4 |
| Trait emotional eating (13–65) | 26.3 ± 1.7 | 26.4 ± 3.4 | 30.2 ± 1.8 | 27.8 ± 2.8 |
| Food intake (kcal) | 347.6 ± 29.1 | 383.5 ± 58.2 | 331.5 ± 30.7 | 393.9 ± 47.7 |
| Energy density intake (kcal/g) | 2.5 ± 0.0 | 2.5 ± 0.1 | 2.4 ± 0.0 | 2.6 ± 0.1 |
| HFSW intake (kcal) | 116.3 ± 13.6 a | 170.6 ± 27.3 | 134.7 ± 22.4b | 189.6 ± 22.4 a,b |
| LFSW intake (kcal) | 78.2 ± 7.7 | 87.9 ± 15.4 | 77.4 ± 8.1 | 83.0 ± 12.6 |
| HFSA intake (kcal) | 125.4 ± 14.7 | 116.2 ± 32.1 | 99.5 ± 16.3 | 99.7 ± 24.2 |
| LFSA intake (kcal) | 30.5 ± 3.8 | 22.3 ± 7.9 | 30.1 ± 4.0 | 20.6 ± 6.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wijnant, K.; Klosowska, J.; Braet, C.; Verbeken, S.; De Henauw, S.; Vanhaecke, L.; Michels, N. Stress Responsiveness and Emotional Eating Depend on Youngsters’ Chronic Stress Level and Overweight. Nutrients 2021, 13, 3654. https://doi.org/10.3390/nu13103654
Wijnant K, Klosowska J, Braet C, Verbeken S, De Henauw S, Vanhaecke L, Michels N. Stress Responsiveness and Emotional Eating Depend on Youngsters’ Chronic Stress Level and Overweight. Nutrients. 2021; 13(10):3654. https://doi.org/10.3390/nu13103654
Chicago/Turabian StyleWijnant, Kathleen, Joanna Klosowska, Caroline Braet, Sandra Verbeken, Stefaan De Henauw, Lynn Vanhaecke, and Nathalie Michels. 2021. "Stress Responsiveness and Emotional Eating Depend on Youngsters’ Chronic Stress Level and Overweight" Nutrients 13, no. 10: 3654. https://doi.org/10.3390/nu13103654
APA StyleWijnant, K., Klosowska, J., Braet, C., Verbeken, S., De Henauw, S., Vanhaecke, L., & Michels, N. (2021). Stress Responsiveness and Emotional Eating Depend on Youngsters’ Chronic Stress Level and Overweight. Nutrients, 13(10), 3654. https://doi.org/10.3390/nu13103654