
Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland


Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Overview
2.1.1. Baseline Risk of T2D
2.1.2. Risk of T2D with Complications
2.1.3. Risk of Death
2.1.4. Estimating the Effects of Increased Whole Grain Intake in the Reduction of T2D
2.1.5. Cost Data
2.1.6. Utility Weights
2.1.7. Sensitivity Analyses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (Variation) * | Distribution | Distribution Values Used in PSA Mean (SE) | Source |
|---|---|---|---|---|
| Additional health care costs of T2D excluding basic health care | 3315 € (±25%) | Gamma | 3315€ (423€) | [35] |
| Cost of T2D complications | 4401€ (±25%) | Gamma | 4401€ (561€) | [34] |
| Costs from productivity losses due to T2D | 7632€ (±25%) | Gamma | 7632€ (974€) | [36] |
| Additional T2D health care costs for primary health care | Men 562 € (SD 587€) Women 542 € (SD 649 €) | Gamma | Men 562€ (9.53€) Women 542€ (9.82€) | Based on own results |
| Additional medication costs of T2D | 584 € (±25%) | Gamma | 584€ (74€) | [47] |
| Parameter | Value (Variation) * | Distribution Applied in PSA | Distribution Values Used in PSA Mean (SE) | Source | |
|---|---|---|---|---|---|
| T2D-specific mortality risk, Hazard ratio (95% CI) | Women HR 2.47 (2.42–3.06) Men HR 1.93 (1.79–2.07) | Lognormal | 2.47 (0.04) 1.93 (0.05) | [32] | |
| Mortality risk associated with T2D with complications, Hazard ratio (95% CI) | HR 2.36 (1.70–3.29) | Lognormal | 2.36 (0.41) | [31] | |
| All-cause mortality | Based on age and sex | - | - | [30] | |
| Utilities | |||||
| Baseline utilities (EQ-5D-3L) | Beta | Alpha | Beta | [39] | |
| (value) | (value) | ||||
| Women | |||||
| (Age, Utility, SE) | |||||
| 30–44 0.906 (0.003) | 8573 | 889 | |||
| 45–54 0.865 (0.005) | 4040 | 631 | |||
| 55–64 0.810 (0.006) | 3463 | 812 | |||
| 65+ 0.770 (0.008) | 2130 | 636 | |||
| Men | Men | Men | |||
| (Age, Utility, SE) | |||||
| 30–44 0.917 (0.003) | 7755 | 702 | |||
| 45–54 0.876 (0.005) | 3806 | 539 | |||
| 55–64 0.821 (0.006) | 3351 | 731 | |||
| 65+ 0.781 (0.008) | 2087 | 585 | |||
| Disutility of T2D (EQ-5D-3L) (SE) | 0.041 | Beta | Alpha | Beta | [38] |
| (0.012) | 11.19 | 261.9 | |||
| Weighted disutility of T2D complications (EQ-5D-3L) | 0.119 (±25%) | Beta | 0.119 (0.015) | Disutility values of individual complications [40,41,42,43,44] Proportion of complications [45] | |
3. Results
3.1. Population Results
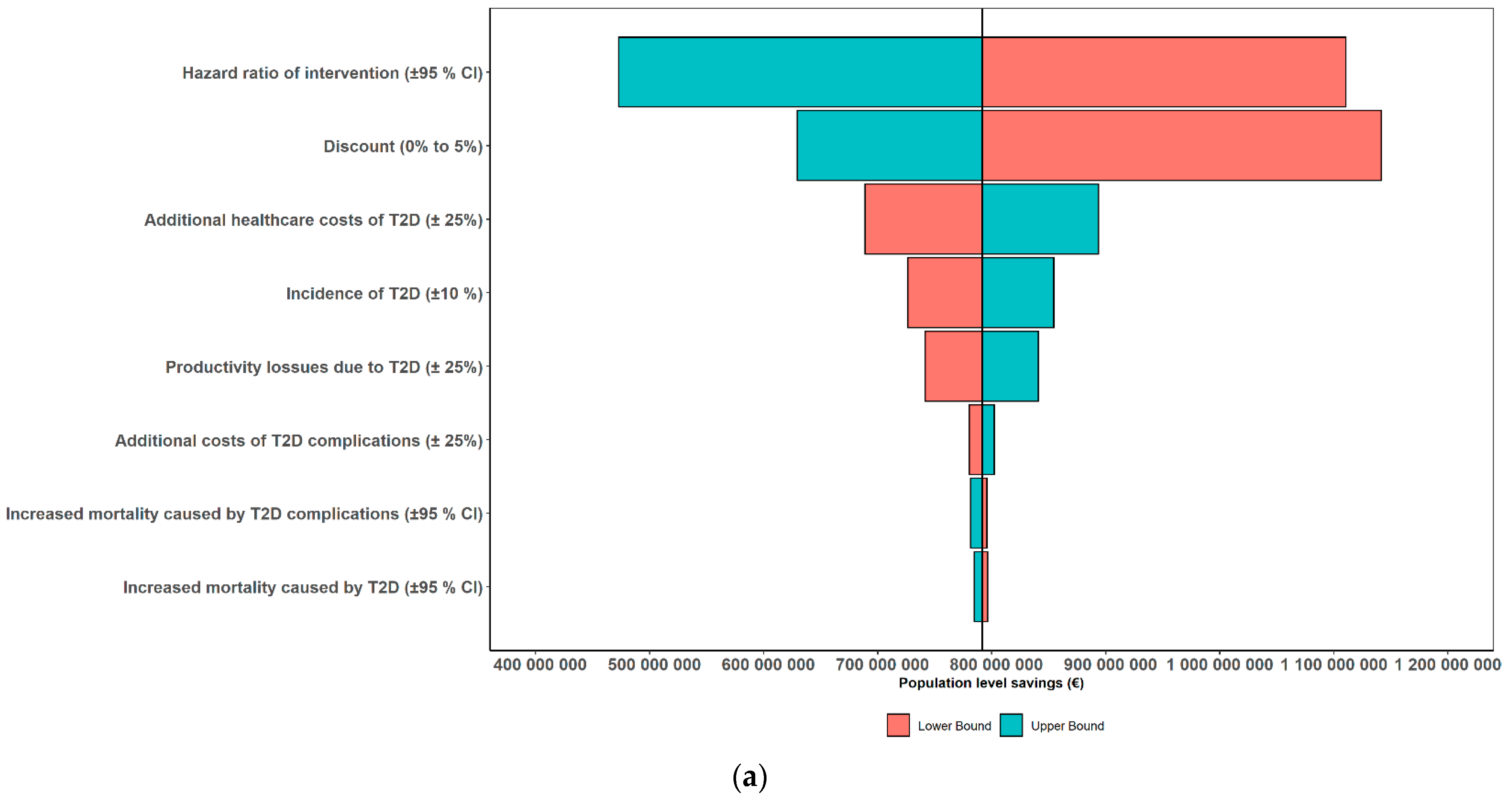
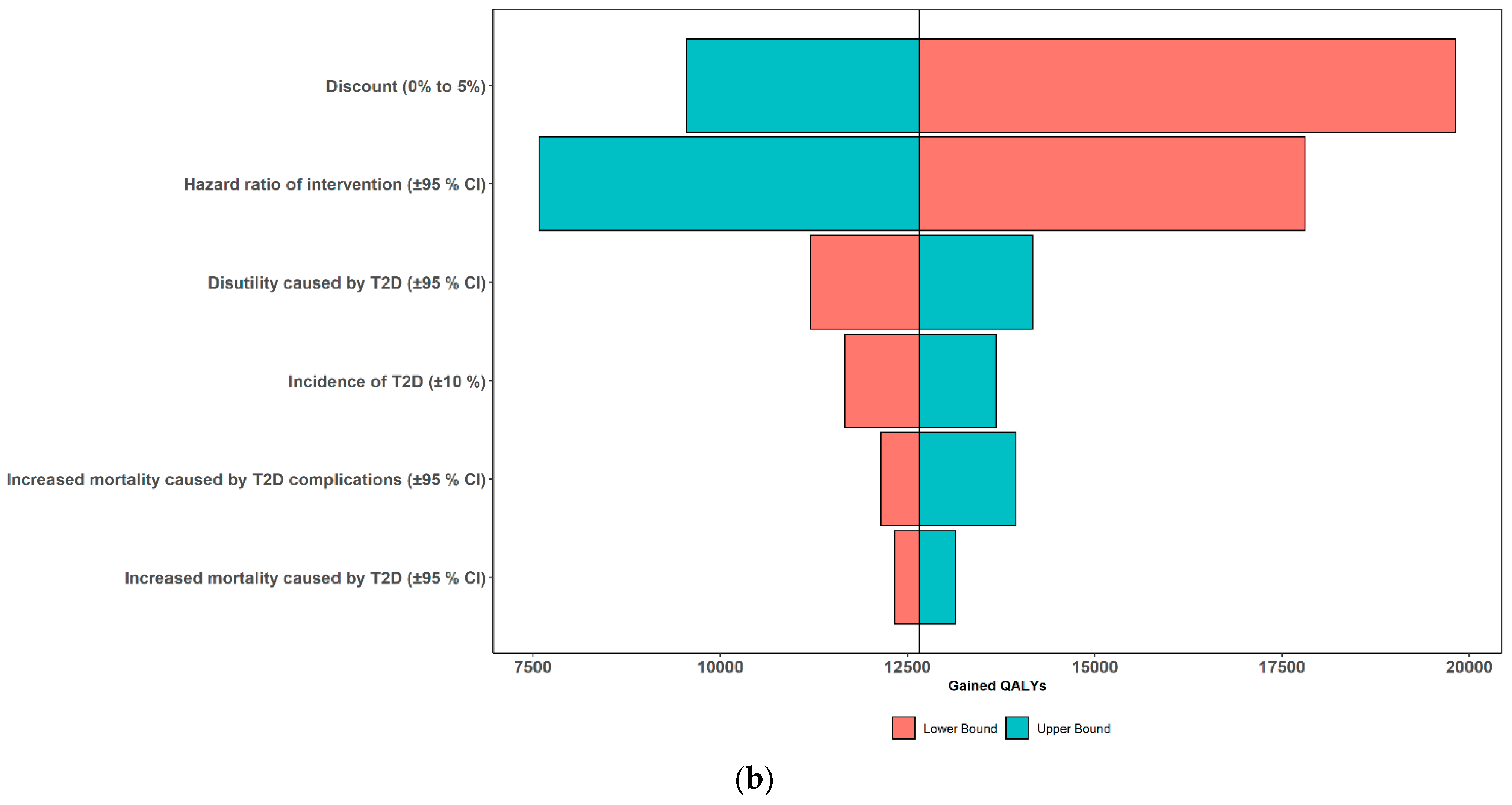
3.2. Results of One-Way Sensitivity Analyses
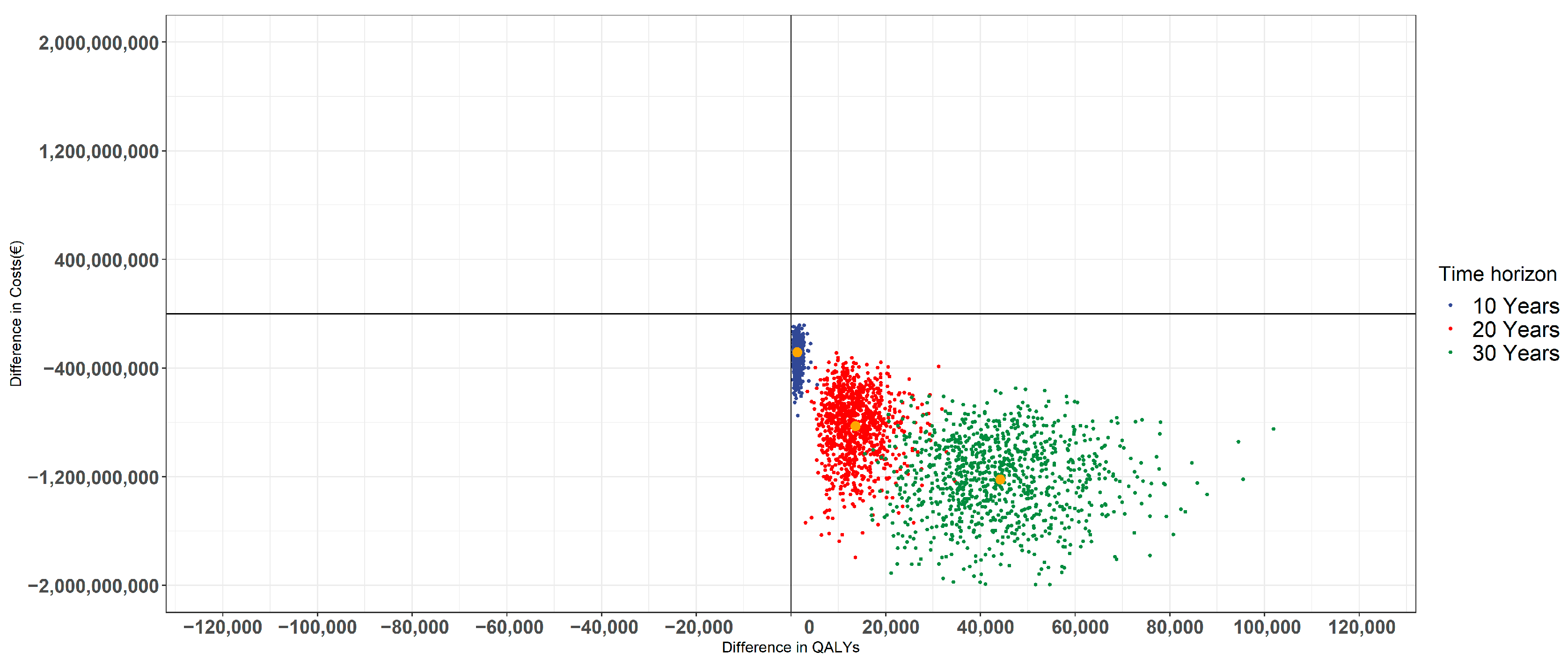
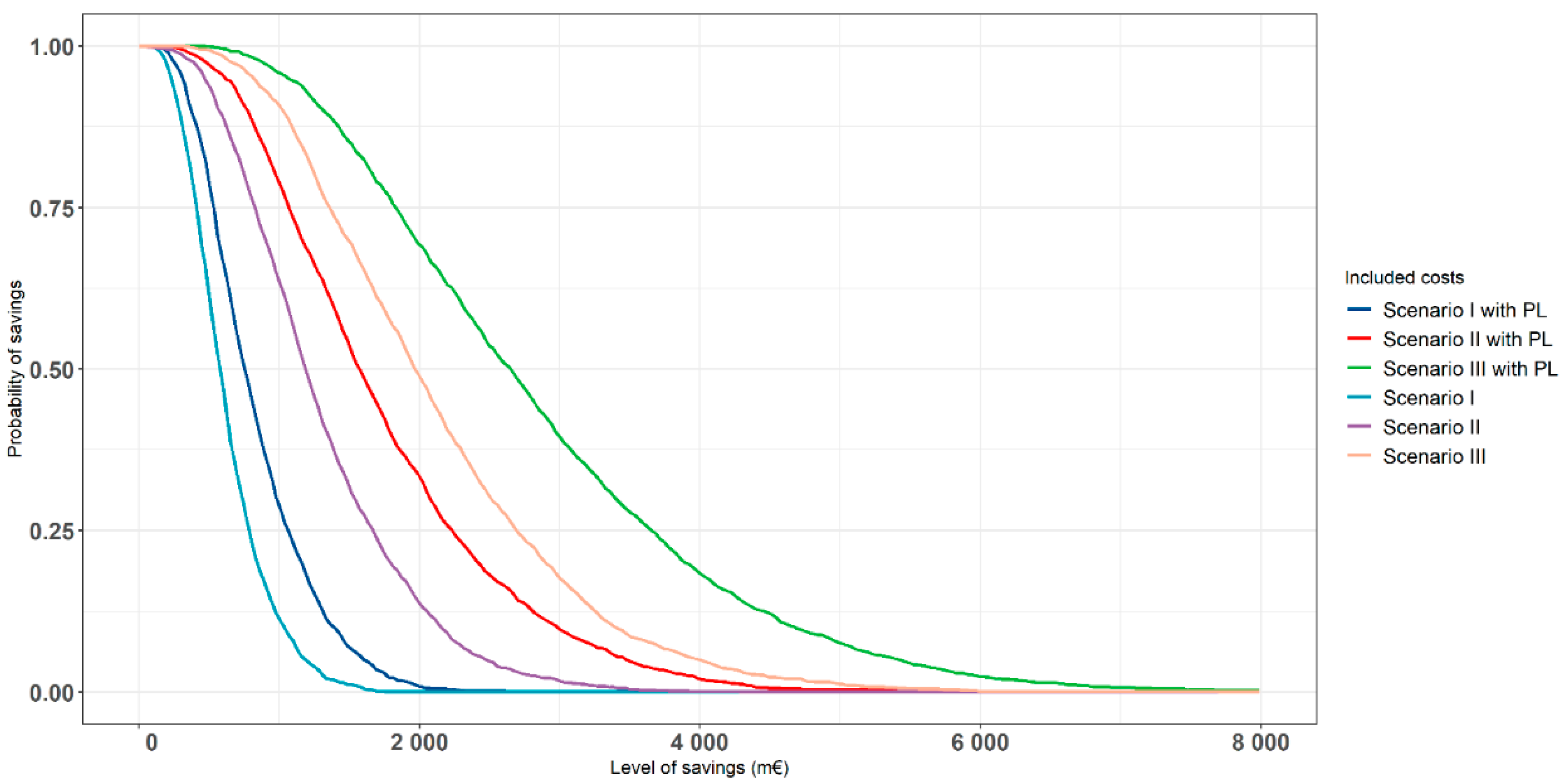
3.3. Results of Probabilistic Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, R.; Karuranga, S.; Malanda, B.; Saeedi, P.; Basit, A.; Besançon, S.; Bommer, C.; Esteghamati, A.; Ogurtsova, K.; Zhang, P.; et al. Global and regional estimates and projections of diabetes-related health expenditure: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The disease burden associated with obesity. J. Am. Med. Assoc. 2013, 282, 1523–1529. [Google Scholar] [CrossRef]
- Brugnara, L.; Murillo, S.; Novials, A.; Rojo-Martínez, G.; Soriguer, F.; Goday, A.; Calle-Pascual, A.; Castaño, L.; Gaztambide, S.; Valdés, S.; et al. Low physical activity and its association with diabetes and other cardiovascular risk factors: A nationwide, population-based study. PLoS ONE 2016, 11, e0160959. [Google Scholar] [CrossRef] [Green Version]
- De Munter, J.S.L.; Hu, F.B.; Spiegelman, D.; Franz, M.; Van Dam, R.M. Whole grain, bran, and germ intake and risk of type 2 diabetes: A prospective cohort study and systematic review. PLoS Med. 2007, 4, e261. [Google Scholar] [CrossRef]
- Chanson-Rolle, A.; Meynier, A.; Aubin, F.; Lappi, J.; Poutanen, K.; Vinoy, S.; Braesco, V. Systematic review and meta-analysis of human studies to support a quantitative recommendation for whole grain intake in relation to type 2 diabetes. PLoS ONE 2015, 10, e0131377. [Google Scholar] [CrossRef]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Norat, T.; Romundstad, P.; Vatten, L.J. Whole grain and refined grain consumption and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of cohort studies. Eur. J. Epidemiol. 2013, 28, 845–858. [Google Scholar] [CrossRef]
- Della Pepa, G.; Vetrani, C.; Vitale, M.; Riccardi, G. Wholegrain intake and risk of type 2 diabetes: Evidence from epidemiological and intervention studies. Nutrients 2018, 10, 1288. [Google Scholar] [CrossRef] [Green Version]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Ding, M.; Sampson, L.; Willett, W.C.; Manson, J.A.E.; Wang, M.; Rosner, B.; Hu, F.B.; Sun, Q. Intake of whole grain foods and risk of type 2 diabetes: Results from three prospective cohort studies. BMJ 2020, 370, m2206. [Google Scholar] [CrossRef]
- Lindström, J.; Louheranta, A.; Mannelin, M.; Rastas, M.; Salminen, V.; Uusitupa, M.; Tuomilehto, J. The Finnish Diabetes Prevention Study (DPS). Diabetes Care 2003, 26, 3230–3236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindström, J.; Peltonen, M.; Eriksson, J.G.; Louheranta, A.; Fogelholm, M.; Uusitupa, M.; Tuomilehto, J. High-fibre, low-fat diet predicts long-term weight loss and decreased type 2 diabetes risk: The Finnish Diabetes Prevention Study. Diabetologia 2006, 49, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Dietary Database Whole Grain Intake across European Countries. Available online: https://knowledge4policy.ec.europa.eu/health-promotion-knowledge-gateway/whole-grain-5_en (accessed on 10 May 2021).
- Valsta, L.; Kaartinen, N.; Tapanainen, H.; Männistö, S.; Sääksjärvi, K. Ravitsemus Suomessa—FinRavinto 2017-Tutkimus. Nutrition in Finland—The National FinDiet 2017 Survey; Terveyden ja hyvinvoinnin laitos (THL). Raportti 12/2018; National Institute for Health and Welfare: Helsinki, Finland, 2018; ISBN 978-952-343-238-3. [Google Scholar]
- Kärkkäinen, O.; Lankinen, M.A.; Vitale, M.; Jokkala, J.; Leppänen, J.; Koistinen, V.; Lehtonen, M.; Giacco, R.; Rosa-Sibakov, N.; Micard, V.; et al. Diets rich in whole grains increase betainized compounds associated with glucose metabolism. Am. J. Clin. Nutr. 2018, 108, 971–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weickert, M.; Möhlig, M.; Schöfl, C.; Arafat, A.; Otto, B.; Viehoff, H.; Koebnick, C.; Kohl, A.; Spranger, J.; Pfeiffer, A. Cereal fiber improves whole-body insulin. Diabetes Care 2006, 29, 773–780. [Google Scholar] [CrossRef] [Green Version]
- Bhathena, S.J.; Velasquez, M.T. Beneficial role of dietary phytoestrogens in obesity and diabetes. Am. J. Clin. Nutr. 2002, 76, 1191–1201. [Google Scholar] [CrossRef] [Green Version]
- Durazzo, A.; Zaccaria, M.; Polito, A.; Maiani, G.; Carcea, M. Lignan Content in Cereals, Buckwheat and Derived Foods. Foods 2013, 2, 53–63. [Google Scholar] [CrossRef]
- Călinoiu, L.; Vodnar, D. Whole Grains and Phenolic Acids: A Review on Bioactivity, Functionality, Health Benefits and Bioavailability. Nutrients 2018, 10, 1615. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, M.M.H.; Hughes, J.; Grafenauer, S. Healthcare cost savings associated with increased whole grain consumption among Australian adults. Nutrients 2021, 13, 1855. [Google Scholar] [CrossRef]
- Abdullah, M.; Gyles, C.; CPF, M.; Carlberg, J.; Jones, P. Cost-of-illness analysis reveals potential healthcare savings with reductions in type 2 diabetes and cardiovascular disease following recommended intakes of dietary fiber in Canada. Front. Pharmacol. 2015, 6, 167. [Google Scholar] [CrossRef] [Green Version]
- Fayet-Moore, F.; George, A.; Cassettari, T.; Yulin, L.; Tuck, K.; Pezzullo, L. Healthcare expenditure and productivity cost savings from reductions in cardiovascular disease and type 2 diabetes associated with increased intake of cereal fibre among Australian adults: A cost of illness analysis. Nutrients 2018, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Koponen, P.; Borodulin, K.; Lundqvist, A.; Sääksjärvi, K.; Koskinen, S. Health, Functioning and Welfare in Finland. The FinHealth 2017 Study; Finnish institute for health and welfare: Helsinki, Finland, 2018. (In Finnish) [Google Scholar]
- Lindström, J.; Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef] [Green Version]
- Zarca, K.; Filipovic-Pierucci, A.; Wiener, M.; Zdenek, K.; Vojtech, F.; Jordan, A.; Yonatan, C.A.; Vince, D. Markov Models for Health Economic Evaluations. Package ‘Heemod’ 2019. Package Guidance. Available online: https://cran.r-project.org/web/packages/heemod/heemod.pdf (accessed on 15 June 2021).
- Statistics of Finland Official Statistics of Finland (OSF): Population Structure [e-Publication]. Statistical Database. Available online: https://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm__vaerak/statfin_vaerak_pxt_11rd.px/ (accessed on 5 May 2021).
- Briggs, A.A.; Claxton, K.; Sculpher, M.M. Decision Modelling for Health Economic Evaluation, 4th ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Borodulin, K.; Tolonen, H.; Jousilahti, P.; Jula, A.; Juolevi, A.; Koskinen, S.; Kuulasmaa, K.; Laatikainen, T.; Männistö, S.; Peltonen, M.; et al. Cohort profile: The national finRiSK study. Int. J. Epidemiol. 2018, 47, 696–696i. [Google Scholar] [CrossRef] [PubMed]
- Wikström, K.; Toivakka, M.; Rautiainen, P.; Tirkkonen, H.; Repo, T.; Laatikainen, T. Electronic Health Records as Valuable Data Sources in the Health Care Quality Improvement Process. Heal. Serv. Res. Manag. Epidemiol. 2019, 6, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Finland Official Statistics of Finland (OSF): Deaths [e-Publication]. Statistical Databse. Available online: https://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm__kuol/statfin_kuol_pxt_12ap.px/ (accessed on 5 May 2021).
- Weir, D.L.; Mcalister, F.A.; Majumdar, S.R.; Eurich, D.T. The interplay between continuity of care, multimorbidity, and adverse events in patients with diabetes. Med. Care 2016, 54, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.S.; Heneghan, C.J.; Farmer, A.J.; Fuller, A.M.; Adler, A.I.; Aronson, J.K.; Stevens, R.J. All-cause and cardiovascular mortality in middle-aged people with type 2 diabetes compared with people without diabetes in a large U.K. primary care database. Diabetes Care 2013, 36, 2366–2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.B.; Kristensen, M.; Seal, C.J.; Jacques, P.; McKeown, N.M. Recommendations for reporting whole-grain intake in observational and intervention studies. Am. J. Clin. Nutr. 2015, 101, 903–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koski, S.; Ilanne-Parikka, P.; Kurkela, O.; Jarvala, T.; Rissanen, P. The cost of diabtes: Reducing comorbidites by half would brings savings of up to hundreds of millions annually. Diabetes ja Lääkäri 2018, 2, 12–17. (In Finnish) [Google Scholar]
- Koski, S.; Kurkela, O.; Ilanne-Parikka, P.; Rissanen, P. The Cost of diabetes in Finland 2002–2011. Finnish Diabetes Association 2017. Available online: https://www.diabetes.fi/yhteiso/vaikuttaminen/tutkimukset_ja_selvitykset/diabeteksen_kustannukset_suomessa#acbe4f4c (accessed on 5 May 2021). (In Finnish).
- Koski, S.; Kurkela, O.; Ilanne-Parikka, P.; Rissanen, P. Diabetes in Numbers. 2018. Finnish Diabetes Association 2017. Available online: https://www.diabetes.fi/yhteiso/vaikuttaminen/tutkimukset_ja_selvitykset/diabeteksen_kustannukset_suomessa#acbe4f4c (accessed on 5 May 2021). (In Finnish).
- Lääkkeiden Hintalautakunta (Pharmaceuticals Pricing Board (HILA)) Preparing a Health Economic Evaluation to Be Attached to the Application for Reimbursement and Wholesale Price for a Medicinal Product. Pharmaceuticals Pricing Board Guideline. 2019, pp. 1–13. Available online: https://www.hila.fi/en/applying-and-notifications/application-forms-and-instructions/ (accessed on 15 June 2021).
- Saarni, S.I.; Harkanen, T.; Sintonen, H.; Suvisaari, J.; Koskinen, S.; Aromaa, A.; Lonnqvist, J. The impact of 29 chronic conditions on health-related quality of life: A general population survey in Finland using 15D and EQ-5D. Qual. Life Res. 2006, 15, 1403–1414. [Google Scholar] [CrossRef]
- Martikainen, J.A.; Soini, E.J.O.; Laaksonen, D.E.; Niskanen, L. Health economic consequences of reducing salt intake and replacing saturated fat with polyunsaturated fat in the adult Finnish population: Estimates based on the FINRISK and FINDIET studies. Eur. J. Clin. Nutr. 2011, 65, 1148–1155. [Google Scholar] [CrossRef] [Green Version]
- Bagust, A.; Beale, S. Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Econ. 2005, 14, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.; Gray, A.; Holman, R. Estimating Utility Values for Health States of Type 2 Diabetic Patients Using the EQ-5D (UKPDS 62). Med. Decis. Mak. 2002, 22, 340–349. [Google Scholar] [CrossRef]
- Kontodimopoulos, N.; Pappa, E.; Chadjiapostolou, Z.; Arvanitaki, E.; Papadopoulos, A.A.; Niakas, D. Comparing the sensitivity of EQ-5D, SF-6D and 15D utilities to the specific effect of diabetic complications. Eur. J. Health Econ. 2010, 13, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Solli, O.; Stavem, K.; Kristiansen, I.S. Health-related quality of life in diabetes: The associations of complications with EQ-5D scores. Health Qual. Life Outcomes 2010, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Beaudet, A.; Clegg, J.; Thuresson, P.O.; Lloyd, A.; McEwan, P. Review of utility values for economic modeling in type 2 diabetes. Value Health 2014, 17, 462–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arffman, M.; Ilanne-Parikka, P.; Keskimäki, I.; Kurkela, O.; Lindström, J.; Sund, R.; Winell, K. The Incidence and Prevalence of Type 1 and Type 2 Diabetes and Their Comorbidities in Finland during the Years 2000–2017. Finnish institute for Health and welfare: Helsnki, Finland, 2020. (In Finnish) [Google Scholar]
- Briggs, A.; Sculpher, M.; Claxton, K. Applied Methods of Cost-effectiveness Analysis in Health Care; Oxford University Press: Oxford, UK, 2006; ISBN 978-0-19-922728-0. [Google Scholar]
- Kela Statistical database Kelasto. Reimbursements of Medicine Expenses Database. Available online: http://raportit.kela.fi/ibi_apps/WFServlet?IBIF_ex=NIT137AL&YKIELI=E (accessed on 3 December 2020).
- Väätäinen, S.; Cederberg, H.; Roine, R.; Keinänen-Kiukaanniemi, S.; Saramies, J.; Uusitalo, H.; Tuomilehto, J.; Martikainen, J. Does future diabetes risk impair current quality of life? A cross-sectional study of health-related quality of life in relation to the Finnish diabetes risk score (FINDRISC). PLoS ONE 2016, 11, e0147898. [Google Scholar] [CrossRef]
- Attema, A.E.; Brouwer, W.B.F.; Claxton, K. Discounting in Economic Evaluations. Pharmacoeconomics 2018, 36, 745–758. [Google Scholar] [CrossRef] [Green Version]
- Andersson, E.; Persson, S.; Hallén, N.; Ericsson, Å.; Thielke, D.; Lindgren, P.; Steen Carlsson, K.; Jendle, J. Costs of diabetes complications: Hospital-based care and absence from work for 392,200 people with type 2 diabetes and matched control participants in Sweden. Diabetologia 2020, 63, 2582–2594. [Google Scholar] [CrossRef]
- Kurkela, O.; Forma, L.; Ilanne-Parikka, P.; Nevalainen, J.; Rissanen, P. Association of diabetes type and chronic diabetes complications with early exit from the labour force: Register-based study of people with diabetes in Finland. Diabetologia 2021, 64, 795–804. [Google Scholar] [CrossRef]
- Zhang, X.F.; Wang, X.K.; Tang, Y.J.; Guan, X.X.; Guo, Y.; Fan, J.M.; Cui, L.L. Association of whole grains intake and the risk of digestive tract cancer: A systematic review and meta-analysis. Nutr. J. 2020, 19, 1–14. [Google Scholar] [CrossRef]
- Mellen, P.B.; Walsh, T.F.; Herrington, D.M. Whole grain intake and cardiovascular disease: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Gaesser, G.A. Whole grains, refined grains, and cancer risk: A systematic review of meta-analyses of observational studies. Nutrients 2020, 12, 3756. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.M.; Schmier, J.K. Cardiovascular healthcare cost savings associated with increased whole grains consumption among adults in the united states. Nutrients 2020, 12, 2323. [Google Scholar] [CrossRef] [PubMed]
- Parikka, S.; Koskela, T.; Ikonen, J.; Kilpeläinen, H.; Hedman, L.; Koskinen, S.; Lounamaa, A. Kansallisen Terveys-, Hyvinvointi ja Palvelututkimus FinSoten Perustulokset 2020 [in Finnish] National FinSote Study Results. Finnish Institute for Health and Welfare. 2018. Available online: http://www.terveytemme.fi/finsote/ (accessed on 5 May 2021).

| Men | Women | Both | |
|---|---|---|---|
| Population (not excl. T2D) (30–79 years) * [26] | 1,673,290 | 1,702,260 | 3,375,550 |
| Prevalence of T2D in whole population (HbA1c ≥ 48 or fasting glucose ≥ 7) (%) ** | 14.6 | 9.4 | 12.0 |
| Estimated population size without T2D (30–79 years) | 1,428,990 | 1,542,248 | 2,971,238 |
| Estimated average age of population at baseline | 53.1 | 54.2 | 53.5 |
| Expected Savings Potential with Productivity Costs (M€) with 95% CIs; [Savings in %] | |||||||||
| Scenario # | 10-Year Time Horizon | 20-Year Horizon | 30-Year Horizon | ||||||
| Women | Men | Total | Women | Men | Total | Women | Men | Total | |
| Scenario I | 113.0 (41.8 to 236.7) | 172.5 (74.1 to 316.0) | 285.5 [3.3%] (115.9 to 552.7) | 341.9 (132.7 to 663.2) | 486.1 (224.3 to 842.0) | 828.0 [3.0%] (357.0 to 1505.2) | 565.0 (279.9 to 930.7) | 656.9 (345.3 to 1015.7) | 1221.9 [2.6%] (625.2 to 1946.4) |
| Scenario II | 248.0 (79.0 to 517.0) | 367.6 (138.0 to 745.5) | 615.6 [7.2%] (217.0 to 1262.5) | 707.8 (269.2 to 1368.8) | 1043.1 (430.8 to 1925.5) | 1750.9 [6.6%] (699.9 to 3294.3) | 1200.3 (479.9 to 2156.3) | 1402.3 (661.0 to 2316.9) | 2602.6 [5.7%] (1140.9 to 4473.2) |
| Scenario III | 402.1 (153.0 to 781.5) | 587.0 (235.7 to 1111.9) | 989.2 [12.2%] (388.7 to 1893.4) | 1145.4 (441.5 to 2281.8) | 1669.6 (770.2 to 2929.4) | 2815.0 [11.2%] (1211.7 to 5211.2) | 1871.7 (848.7 to 3164.0) | 2365.7 (1235.1 to 3694.5) | 4237.3 [9.6%] (2083.8 to 6858.5) |
| Expected Savings Potential without Productivity Costs (M€) with 95% CIs; [Savings in %] | |||||||||
| 10-Year Time Horizon | 20-Year Horizon | 30-Year Horizon | |||||||
| Scenario # | Women | Men | Total | Women | Men | Total | Women | Men | Total |
| Scenario I | 44.1 (15.2 to 91.8) | 66.0 (26.2 to 125.5) | 110.0 [3.4%] (41.4 to 217.2) | 263.7 (102.5 to 516.7) | 347.4 (174.9 to 599.3) | 611.1 [3.0%] (277.4 to 1116.0) | 488.5 (223.8 to 838.6) | 531.2 (281.0 to 869.0) | 1019.7 [2.5%] (504.8 to 1707.6) |
| Scenario II | 91.9 (28.5 to 195.2) | 136.9 (49.0 to 266.3) | 228.8 [7.2%] (77.4 to 461.5) | 565.7 (203.0 to 1074.8) | 735.5 (310.0 to 1298.8) | 1301.2 [6.4%] (512.9 to 2373.6) | 1027.9 (439.0 to 1830.8) | 1132.1 (533.1 to 1931.1) | 2160.0 [5.4%] (972.1 to 3761.8) |
| Scenario III | 146.1 (51.9 to 298.3) | 222.1 (90.4 to 433.8) | 368.2 [12.3%] (142.3 to 732.0) | 909.7 (384.5 to 1665.7) | 1219.2 (565.8 to 2091.2) | 2128.9 [11.0%] (950.3 to 3756.9) | 1678.1 (801.4 to 2871.1) | 1824.0 (959.6 to 2805.2) | 3502.2 [9.3%] (1760.9 to 5676.3) |
| 10-Year Horizon | 20-Year Horizon | 30-Year Horizon | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Scenario # | Women | Men | Total | Women | Men | Total | Women | Men | Total |
| Scenario I | 501 (170 to 1041) | 822 (310 to 1587) | 1323 (480 to 2628) | 5300 (2021 to 9990) | 8314 (3224 to 15,691) | 13,614 (5245 to 25,681) | 20,310 (8407 to 36,205) | 23,927 (9925 to 41,424) | 44,237 (18,332 to 77,629) |
| Scenario II | 1091 (331 to 2325) | 1749 (570 to 3440) | 2840 (901 to 5765) | 11,012 (3673 to 21,294) | 17,590 (6626 to 34,373) | 28,602 (10,299 to 55,667) | 41,850 (16,002 to 78,749) | 50,842 (19,830 to 93,074) | 92,692 (35,832 to 171,823) |
| Scenario III | 1748 (593 to 3806) | 2845 (1033 to 5603) | 4593 (1626 to 9409) | 17,620 (6882 to 34,991) | 27,494 (10,632 to 52,799) | 45,114 (17,514 to 87,790) | 70,426 (31,723 to 124,935) | 83,668 (36,171 to 148,325) | 154,094 (67,894 to 273,260) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martikainen, J.; Jalkanen, K.; Heiskanen, J.; Lavikainen, P.; Peltonen, M.; Laatikainen, T.; Lindström, J. Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland. Nutrients 2021, 13, 3583. https://doi.org/10.3390/nu13103583
Martikainen J, Jalkanen K, Heiskanen J, Lavikainen P, Peltonen M, Laatikainen T, Lindström J. Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland. Nutrients. 2021; 13(10):3583. https://doi.org/10.3390/nu13103583
Chicago/Turabian StyleMartikainen, Janne, Kari Jalkanen, Jari Heiskanen, Piia Lavikainen, Markku Peltonen, Tiina Laatikainen, and Jaana Lindström. 2021. "Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland" Nutrients 13, no. 10: 3583. https://doi.org/10.3390/nu13103583
APA StyleMartikainen, J., Jalkanen, K., Heiskanen, J., Lavikainen, P., Peltonen, M., Laatikainen, T., & Lindström, J. (2021). Type 2 Diabetes-Related Health Economic Impact Associated with Increased Whole Grains Consumption among Adults in Finland. Nutrients, 13(10), 3583. https://doi.org/10.3390/nu13103583