
Associations of Food and Nutrient Intake with Serum Hepcidin and the Risk of Gestational Iron-Deficiency Anemia among Pregnant Women: A Population-Based Study

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. 24-h Dietary Recall and FFQ
2.4. Laboratory Examination
2.5. Definitions
2.6. Statistical Analysis
3. Results
3.1. Maternal Baseline Characteristics Stratified by Quartiles (Qs) of Serum Hepcidin Levels
3.2. Associations between Maternal Nutrient/Food Intake and Serum Hepcidin Levels
3.3. Potential Foods and Nutrients That Affect Serum Hepcidin Levels
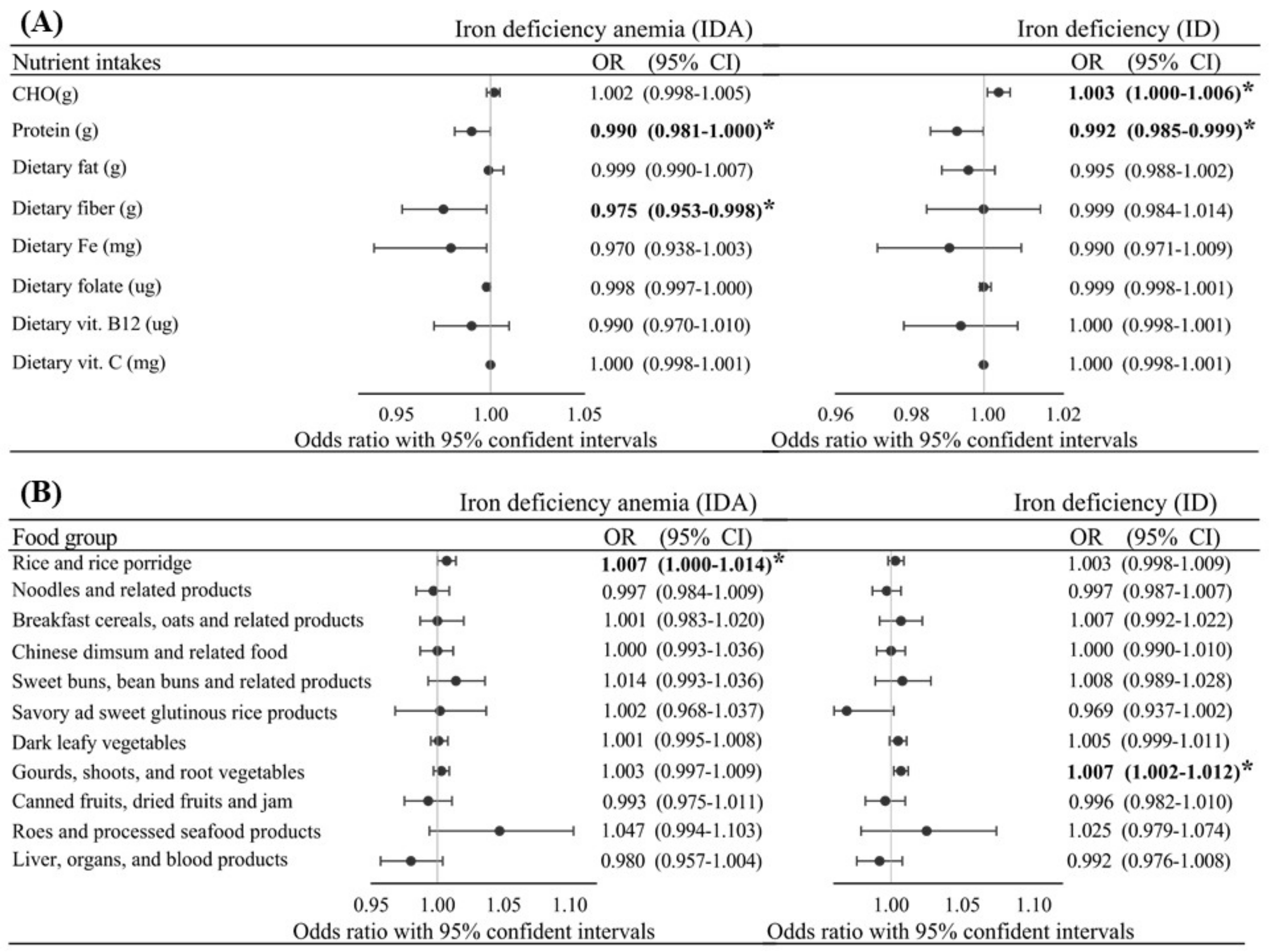
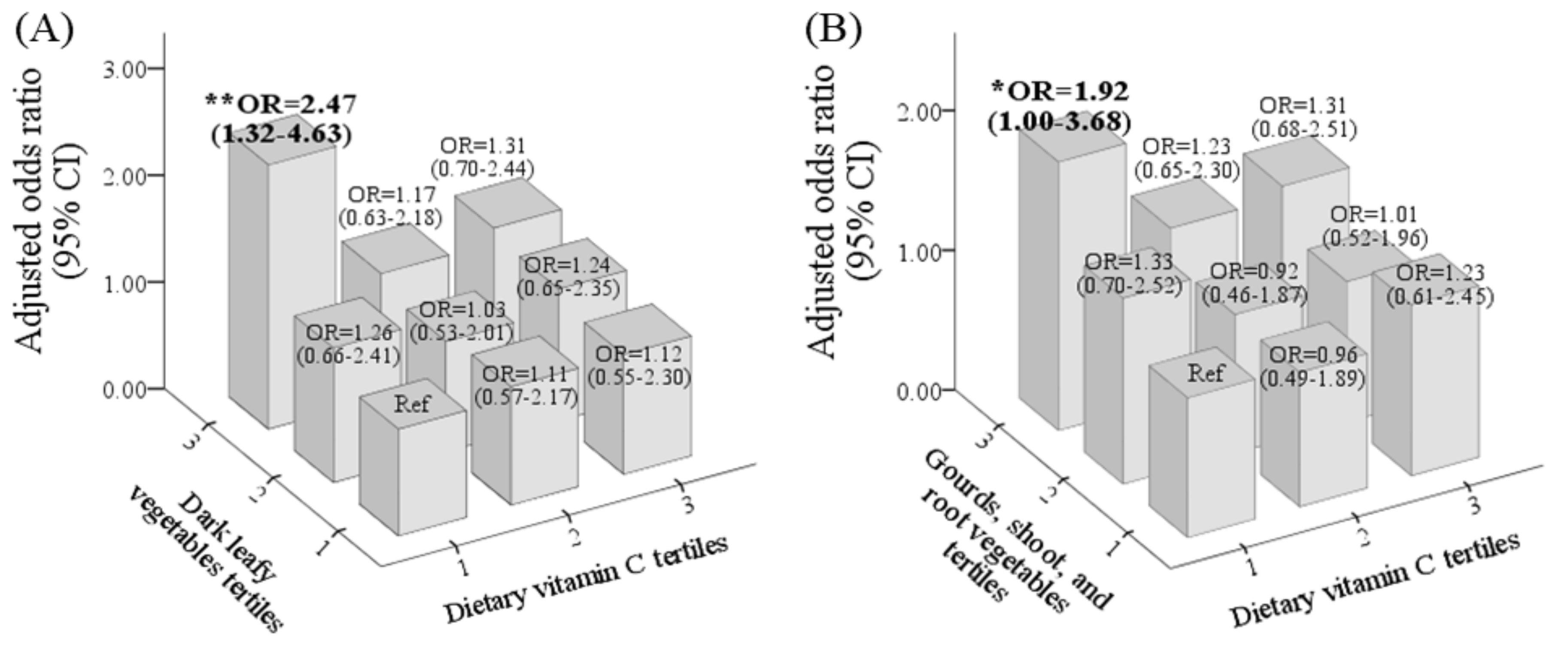
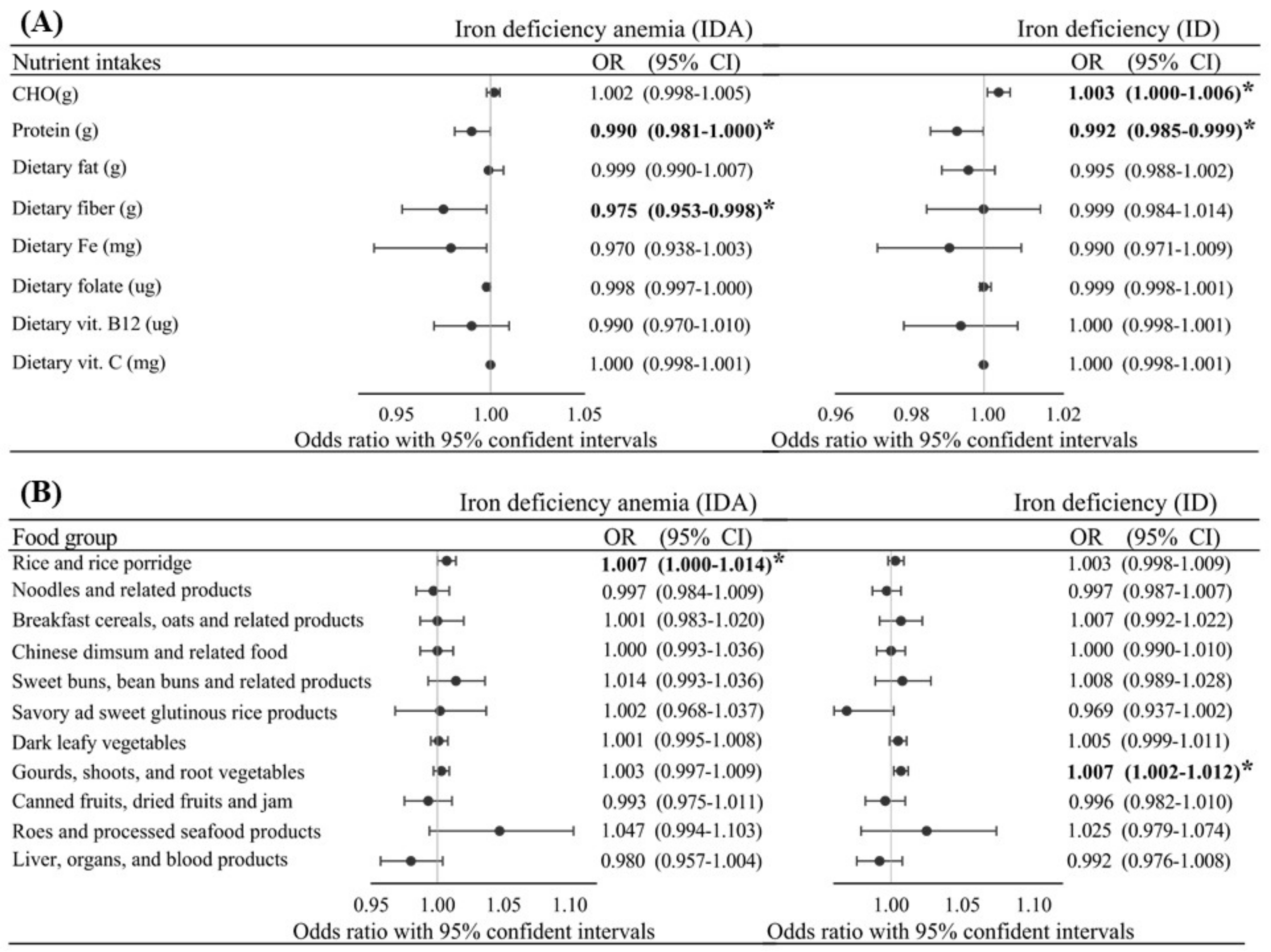
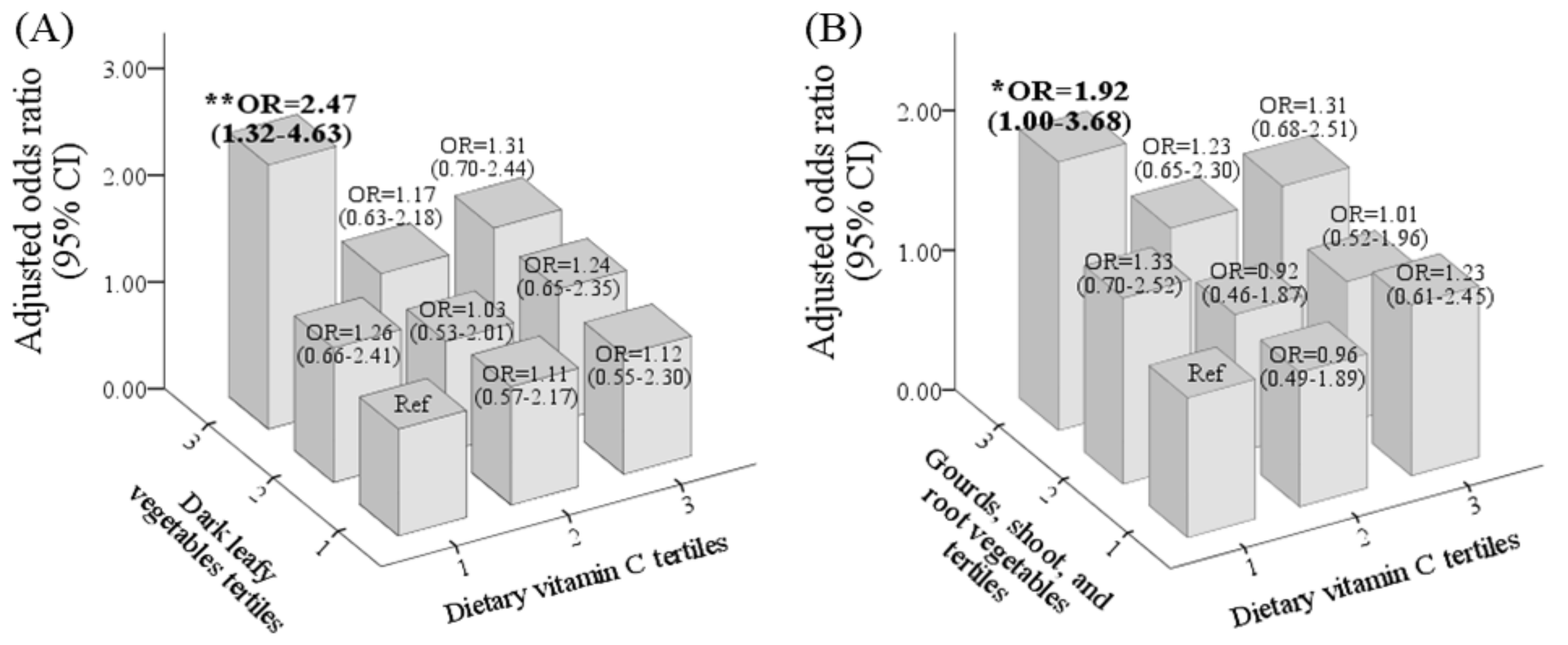
3.4. Predictive Effects of Nutrients and Food Groups on Gestational ID and IDA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). The Global Prevalence of Anaemia in 2011; WHO Document Production Services: Genewa, Switzerland, 2015. [Google Scholar]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study Group. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. J. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.O.; Ru, Y. Iron status of North American pregnant women: An update on longitudinal data and gaps in knowledge from the United States and Canada. Am. J. Clin. Nutr. 2017, 106, 1647S–1654S. [Google Scholar] [CrossRef] [Green Version]
- Teichman, J.; Nisenbaum, R.; Lausman, A.; Sholzberg, M. Suboptimal iron deficiency screening in pregnancy and the impact of socioeconomic status in a high-resource setting. Blood Adv. 2021. [Google Scholar] [CrossRef] [PubMed]
- Breymann, C.; Auerbach, M. Iron deficiency in gynecology and obstetrics: Clinical implications and management. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaskheli, M.-N.; Baloch, S.; Sheeba, A.; Baloch, S.; Khaskheli, F.K. Iron deficiency anaemia is still a major killer of pregnant women. Pak. J. Med. Sci. 2016, 32, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.L.; Nemeth, E. Iron homeostasis during pregnancy. Am. J. Clin. Nutr. 2017, 106, 1567s–1574s. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Hepcidin and iron homeostasis. Biochim. Biophys. Acta 2012, 1823, 1434–1443. [Google Scholar] [CrossRef] [Green Version]
- Sangkhae, V.; Ganz, T.; Nemeth, E. Maternal Hepcidin Suppression Is Essential for Healthy Pregnancy. Blood 2020, 136, 43–44. [Google Scholar] [CrossRef]
- Bah, A.; Pasricha, S.-R.; Jallow, M.W.; Sise, E.A.; Wegmuller, R.; Armitage, A.E.; Drakesmith, H.; Moore, S.E.; Prentice, A.M. Serum Hepcidin Concentrations Decline during Pregnancy and May Identify Iron Deficiency: Analysis of a Longitudinal Pregnancy Cohort in The Gambia. J. Nutr. 2017, 147, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Santen, S.v.; Kroot, J.J.C.; Zijderveld, G.; Wiegerinck, E.T.; Spaanderman, M.E.A.; Swinkels, D.W. The iron regulatory hormone hepcidin is decreased in pregnancy: A prospective longitudinal study. Clin. Chem. Lab. Med. 2013, 51, 1395–1401. [Google Scholar] [CrossRef]
- Sangkhae, V.; Fisher, A.L.; Chua, K.J.; Ruchala, P.; Ganz, T.; Nemeth, E. Maternal hepcidin determines embryo iron homeostasis in mice. Blood 2020, 136, 2206–2216. [Google Scholar] [CrossRef]
- Koenig, M.D.; Tussing-Humphreys, L.; Day, J.; Cadwell, B.; Nemeth, E. Hepcidin and iron homeostasis during pregnancy. Nutrients 2014, 6, 3062–3083. [Google Scholar] [CrossRef] [PubMed]
- Hamlin, F.; Latunde-Dada, G.O. Iron bioavailability from a tropical leafy vegetable in anaemic mice. Nutr. Metab. 2011, 8, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zehra, A.; Saleh Abdullah, S.M.; Saboor, M. Moinuddin. Effect of Intravenous Iron Supplementation on Hepcidin Levels in Iron Deficient Pregnant Females in Second and Third Trimester. Indian J. Hematol. Blood Transfus. 2017, 33, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Ghatpande, N.S.; Apte, P.P.; Naik, S.S.; Kulkarni, P.P. Fruit and Vegetable Consumption and Their Association With the Indicators of Iron and Inflammation Status Among Adolescent Girls. J. Am. Coll. Nutr. 2019, 38, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Saini, R.K.; Manoj, P.; Shetty, N.P.; Srinivasan, K.; Giridhar, P. Dietary iron supplements and Moringa oleifera leaves influence the liver hepcidin messenger RNA expression and biochemical indices of iron status in rats. Nutr. Res. 2014, 34, 630–638. [Google Scholar] [CrossRef]
- Sim, M.; Dawson, B.; Landers, G.; Wiegerinck, E.T.; Swinkels, D.W.; Townsend, M.-A.; Trinder, D.; Peeling, P. The effects of carbohydrate ingestion during endurance running on post-exercise inflammation and hepcidin levels. Eur. J. Appl. Physiol. 2012, 112, 1889–1898. [Google Scholar] [CrossRef] [PubMed]
- Cercamondi, C.I.; Icard-Vernière, C.; Egli, I.M.; Vernay, M.; Hama, F.; Brouwer, I.D.; Zeder, C.; Berger, J.; Hurrell, R.F.; Mouquet-Rivier, C. A Higher Proportion of Iron-Rich Leafy Vegetables in a Typical Burkinabe Maize Meal Does Not Increase the Amount of Iron Absorbed in Young Women. J. Nutr. 2014, 144, 1394–1400. [Google Scholar] [CrossRef]
- Karanja, P.N.; Kenji, G.M.; Njoroge, S.M.; Sila, D.N.; Onyango, C.A.; Koaze, H.; Baba, N. Compositional Characteristics of Young Shoots of Selected Bamboo Species Growing in Kenya and Their Potential as Food Source. J. Food Nutr. Res. 2015, 3, 607–612. [Google Scholar] [CrossRef]
- Tang, Y.; Li, Y.; Yu, H.; Gao, C.; Liu, L.; Chen, S.; Xing, M.; Liu, L.; Yao, P. Quercetin prevents ethanol-induced iron overload by regulating hepcidin through the BMP6/SMAD4 signaling pathway. J. Nutr. Biochem. 2014, 25, 675–682. [Google Scholar] [CrossRef]
- Mu, M.; An, P.; Wu, Q.; Shen, X.; Shao, D.; Wang, H.; Zhang, Y.; Zhang, S.; Yao, H.; Min, J.; et al. The dietary flavonoid myricetin regulates iron homeostasis by suppressing hepcidin expression. J. Nutr. Biochem. 2016, 30, 53–61. [Google Scholar] [CrossRef]
- Lesjak, M.; Balesaria, S.; Skinner, V.; Debnam, E.S.; Srai, S.K.S. Quercetin inhibits intestinal non-haem iron absorption by regulating iron metabolism genes in the tissues. Eur. J. Nutr. 2019, 58, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Pabón de Rozo, M.; VanCampen, D.; Miller, D.D. Effects of some carbohydrates on iron absorption. Arch. Latinoam. Nutr. 1986, 36, 688–700. [Google Scholar] [PubMed]
- Trinidad, T.P.; Mallillin, A.C.; Sagum, R.S.; Briones, D.P.; Encabo, R.R.; Juliano, B.O. Iron absorption from brown rice/brown rice-based meal and milled rice/milled rice-based meal. Int. J. Food Sci. Nutr. 2009, 60, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Milman, N.T. A Review of Nutrients and Compounds, Which Promote or Inhibit Intestinal Iron Absorption: Making a Platform for Dietary Measures That Can Reduce Iron Uptake in Patients with Genetic Haemochromatosis. J. Nutr. Metab. 2020, 2020, 7373498. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-S.; Pan, W.-H.; Liu, K.-L.; Yu, M.-S.J.A.P.j.o.c.n. Reproducibility and validity of a Chinese food frequency questionnaire used in Taiwan. Asia Pac. J. Clin. Nutr. 2006, 15, 127–286. [Google Scholar]
- Zhang, H.; Qiu, X.; Zhong, C.; Zhang, K.; Xiao, M.; Yi, N.; Xiong, G.; Wang, J.; Yao, J.; Hao, L.J.N.j. Reproducibility and relative validity of a semi-quantitative food frequency questionnaire for Chinese pregnant women. Nutr. J. 2015, 14, 56. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Iron Deficiency Anaemia: Assessment, Prevention and Control: A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Breymann, C. Iron Deficiency Anemia in Pregnancy. Semin. Hematol. 2015, 52, 339–347. [Google Scholar] [CrossRef]
- Centers for Disease Contol and Prevention. (CDC) criteria for anemia in children and childbearing-aged women. MMWR Morb. Mortal. Wkly. Rep. 1989, 38, 400–404. [Google Scholar]
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. The importance of the normality assumption in large public health data sets. J. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Willett, W.C.; Howe, G.R.; Kushi, L.H.J.T.A.j.o.c.n. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef]
- Zhen, A.W.; Nguyen, N.H.; Gibert, Y.; Motola, S.; Buckett, P.; Wessling-Resnick, M.; Fraenkel, E.; Fraenkel, P.G. The small molecule, genistein, increases hepcidin expression in human hepatocytes. Hepatology 2013, 58, 1315–1325. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-J.; Kim, K.-S.; Lim, D.; Yang, D.J.; Park, J.-I.; Kim, K.W.; Jeong, J.-H.; Choi, H.-S.; Kim, D.-K. Epigallocatechin-3-Gallate (EGCG)-Inducible SMILE Inhibits STAT3-Mediated Hepcidin Gene Expression. Antioxidants 2020, 9, 514. [Google Scholar] [CrossRef]
- Lesjak, M.; K S Srai, S. Role of Dietary Flavonoids in Iron Homeostasis. Pharmaceuticals 2019, 12, 119. [Google Scholar] [CrossRef] [Green Version]
- Chiu, P.F.; Ko, S.Y.; Chang, C.C. Vitamin C affects the expression of hepcidin and erythropoietin receptor in HepG2 cells. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2012, 22, 373–376. [Google Scholar] [CrossRef]
- Foster-Powell, K.; Holt, S.H.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.-H.A.; Wu, M.-C.; Lu, S.; Lin, J. Glycemic index, glycemic load and insulinemic index of Chinese starchy foods. World J. Gastroenterol. 2010, 16, 4973–4979. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, S.; Hancock, D.P.; Petocz, P.; Ceriello, A.; Brand-Miller, J. High-glycemic index carbohydrate increases nuclear factor-kappaB activation in mononuclear cells of young, lean healthy subjects. Am. J. Clin. Nutr. 2008, 87, 1188–1193. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-S.; Chen, Y.-C.; Owaga, E.; Palupi, K.C.; Pan, W.-H.; Bai, C.-H. Interactive Effects of Dietary Fat/Carbohydrate Ratio and Body Mass Index on Iron Deficiency Anemia among Taiwanese Women. Nutrients 2014, 6, 3929–3941. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Wang, X.; Song, G.; Xing, H.; Yang, L.; Han, K.; Chang, Y.Z.J.J.o.F.B. A high-fructose diet in rats induces systemic iron deficiency and hepatic iron overload by an inflammation mechanism. J. Food Biochem. 2021, 45, e13578. [Google Scholar] [PubMed]
- Moran, L.J.; McNaughton, S.A.; Sui, Z.; Cramp, C.; Deussen, A.R.; Grivell, R.M.; Dodd, J.M. The characterisation of overweight and obese women who are under reporting energy intake during pregnancy. BMC Pregnancy Childbirth 2018, 18, 204. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Godfrey, K.; Osmond, C.; Cox, V.; Barker, D. Evaluation of a food frequency questionnaire used to assess nutrient intakes in pregnant women. Eur. J. Clin. Nutr. 1996, 50, 302–308. [Google Scholar] [PubMed]
- Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Robinson, S.M. Dietary patterns in pregnant women: A comparison of food-frequency questionnaires and 4 d prospective diaries. Br. J. Nutr. 2008, 99, 869–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variable | Serum Hepcidin Level, Quartiles | p for Trend a | |||
|---|---|---|---|---|---|
| Q1 (n = 355) | Q2 (n = 360) | Q3 (n = 358) | Q4 (n = 357) | ||
| Basic characteristic | |||||
| Age (years) | 31.7 ± 5.0 | 32.9 ± 4.6 | 32.8 ± 4.6 | 32.9 ± 4.6 | 0.002 |
| Pre-pregnancy body-mass index (kg/m2) | 22.1 ± 3.9 | 22.8 ± 4.0 | 22.7 ± 4.1 | 23.0 ± 4.1 | 0.006 |
| Region | <0.001 | ||||
| Northern (n, %) | 95 (26.8) | 115 (31.9) | 132 (36.9) | 136 (38.1) | |
| Central (n, %) | 79 (22.3) | 95 (26.4) | 88 (24.6) | 67 (18.8) | |
| Southern (n, %) | 67 (18.9) | 65 (18.1) | 80 (22.3) | 74 (20.7) | |
| Eastern (n, %) | 114 (32.1) | 85 (23.6) | 58 (16.2) | 80 (22.4) | |
| Trimester | <0.001 | ||||
| First trimester (n, %) | 43 (12.1) | 36 (10.0) | 97 (27.1) | 178 (49.9) | |
| Second trimester (n, %) | 112 (31.5) | 84 (23.3) | 145 (40.5) | 122 (34.2) | |
| Third trimester (n, %) | 200 (56.3) | 240 (66.7) | 116 (32.4) | 57 (16.0) | |
| Parity | <0.001 | ||||
| Primiparous (n, %) | 158 (44.6) | 191 (53.2) | 215 (60.2) | 212 (59.7) | |
| Reported use of prenatal dietary supplements | |||||
| Total supplement use (n, %) | 259 (73.4) | 291 (82.7) | 320 (90.4) | 321 (90.9) | <0.001 |
| Multivitamin-mineral (n, %) | 199 (56.5) | 220 (63.2) | 246 (69.5) | 216 (61.4) | 0.071 |
| Vitamin B (n, %) | 47 (13.5) | 61 (17.4) | 74 (21.1) | 73 (20.9) | 0.005 |
| Folate (n, %) | 138 (39.2) | 145 (41.4) | 165 (47.3) | 195 (55.7) | <0.001 |
| Iron (n, %) | 33 (9.5) | 44 (12.6) | 33 (9.3) | 37 (10.6) | 0.988 |
| Blood biochemistry | |||||
| Serum hepcidin (ng/mL) | 0.3 ± 0.3 | 2.4 ± 1.4 | 19.8 ± 10.6 | 73.2 ± 24.6 | <0.001 |
| TS (%) | 10.1 ± 7.5 | 12.8 ± 7.9 | 20.8 ± 9.3 | 22.2 ± 9.1 | <0.001 |
| Hb (g/dL) | 11.2 ± 1.8 | 11.5 ± 1.7 | 12.2 ± 2.0 | 12.1 ± 2.0 | <0.001 |
| Serum ferritin (ng/mL) | 8.0 ± 6.0 | 10.3 ± 4.4 | 23.8 ± 14.6 | 50.0 ± 33.7 | <0.001 |
| Iron abnormality | |||||
| Anemia (n, %) | 142 (40.0) | 104 (28.9) | 51 (14.2) | 57 (16.0) | <0.001 |
| Non-IDA anemia (n, %) | 10 (2.8) | 12 (3.3) | 39 (10.9) | 57 (16.0) | <0.001 |
| IDA (n, %) | 132 (37.2) | 92 (25.6) | 12 (3.4) | 0 (0.0) | <0.001 |
| Iron deficiency (n, %) | 293 (82.5) | 263 (73.1) | 49 (13.7) | 1 (0.3) | <0.001 |
| Variable | Hepcidin-Level, Quartiles | p for Trend a | |||
|---|---|---|---|---|---|
| Quartile 1 (n = 355) | Quartile 2 (n = 360) | Quartile 3 (n = 358) | Quartile 4 (n = 357) | ||
| Nutrient intake b | |||||
| Carbohydrates (g) | 14.3 ± 48.7 | 13.6 ± 45.3 | 11.3 ± 43.3 | 9.7 ± 45.0 | 0.141 |
| Protein (g) | 5.0 ± 17.7 | 6.5 ± 18.2 | 7.8 ± 16.9 | 6.8 ± 16.0 | 0.099 |
| Fat (g) | −8.0 ± 19.8 | −7.9 ± 17.4 | −7.6 ± 18.1 | −6.4 ± 18.9 | 0.255 |
| Dietary fiber (g) | 1.5 ± 8.6 | 2.2 ± 8.2 | 2.0 ± 7.3 | 3.0 ± 9.4 | 0.04 |
| Dietary Fe (mg) | 2.0 ± 4.9 | 2.8 ± 6.8 | 2.2 ± 4.7 | 3.0 ± 8.6 | 0.108 |
| Dietary B9 (µg) | 74.2 ± 83.0 | 76.8 ± 83.1 | 76.2 ± 84.0 | 78.2 ± 108.3 | 0.594 |
| Dietary B12 (µg) | 2.9 ± 10.3 | 2.5 ± 7.3 | 2.2 ± 5.9 | 2.9 ± 9.6 | 0.941 |
| Dietary vitamin C (mg) | 67.7 ± 100.3 | 66.8 ± 108.0 | 80.8 ± 119.0 | 86.0 ± 145.2 | 0.014 |
| Food group b (frequency: times/month) | |||||
| Rice and rice porridge | 38.6 ± 23.2 | 36.4 ± 21.7 | 36.0 ± 23.0 | 35.8 ± 21.6 | 0.096 |
| Noodles and related products | 15.5 ± 13.4 | 15.0 ± 12.0 | 16.0 ± 12.2 | 16.1 ± 12.9 | 0.303 |
| Breakfast cereals, oats, and related products | 2.9 ± 9.3 | 1.7 ± 7.0 | 2.0 ± 8.3 | 1.4 ± 8.5 | 0.029 |
| Chinese dim sum and related foods | 9.0 ± 11.6 | 9.6 ± 11.8 | 10.0 ± 12.3 | 10.5 ± 13.4 | 0.144 |
| Sweet buns, bean buns, and related products | 3.2 ± 6.2 | 2.8 ± 8.0 | 1.6 ± 4.6 | 2.1 ± 5.1 | 0.002 |
| Savory and sweet glutinous rice products | 0.9 ± 3.3 | 0.9 ± 3.1 | 0.67 ± 2.8 | 1.3 ± 6.8 | 0.512 |
| Light-colored vegetables | 23.4 ± 21.3 | 24.1 ± 22.0 | 21.3 ± 18.0 | 21.2 ± 19.2 | 0.05 |
| Dark leafy vegetables | 26.4 ± 20.8 | 29.8 ± 23.4 | 26.6 ± 21.0 | 24.9 ± 18.7 | 0.121 |
| Gourds, shoots, and root vegetables | 29.3 ± 26.2 | 30.1 ± 27.5 | 26.0 ± 22.9 | 25.4 ± 22.8 | 0.007 |
| Legumes | 4.0 ± 7.9 | 3.6 ± 7.5 | 3.1 ± 5.5 | 2.7 ± 4.8 | 0.007 |
| Total vegetables | 47.2 ± 27.6 | 48.9 ± 29.8 | 44.8 ± 28.0 | 45.2 ± 27.6 | 0.135 |
| Fresh fruits | 32.6 ± 20.9 | 32.2 ± 21.3 | 29.4 ± 18.5 | 30.1 ± 20.0 | 0.029 |
| 100% pure fruit juice or fruit/vegetable juice | 5.4 ± 8.6 | 5.4 ± 9.5 | 4.8 ± 6.6 | 7.3 ± 12.9 | 0.033 |
| Canned fruits, dried fruits, and jam | 2.3 ± 9.6 | 2.1 ± 7.8 | 1.8 ± 7.9 | 4.4 ± 14.5 | 0.016 |
| Fish, shellfish, and seafood | 20.9 ± 20.1 | 21.5 ± 19.6 | 17.7 ± 16.4 | 19.1 ± 18.0 | 0.043 |
| Roe and processed seafood products | 0.6 ± 2.3 | 0.5 ± 2.76 | 0.4 ± 2.0 | 0.7 ± 2.7 | 0.845 |
| Poultry meat | 17.1 ± 15.4 | 17.4 ± 15.6 | 16.7 ± 14.4 | 15.6 ± 13.1 | 0.14 |
| Liver, organs, and blood products | 2.8 ± 8.5 | 3.0 ± 7.2 | 2.6 ± 5.9 | 3.9 ± 9.6 | 0.123 |
| All Pregnant Women (N = 1430) | Non-Iron Deficiency/Iron-Deficiency Anemia (Non-ID/IDA) Pregnant Women (N = 824) | Iron Deficiency (ID) Pregnant Women (N = 606) | Iron Deficiency Anemia (IDA) Pregnant Women (N = 236) | |||||
|---|---|---|---|---|---|---|---|---|
| ß (95% CI) | p Value a | ß (95% CI) | p Value a | ß (95% CI) | p Value a | ß (95% CI) | p Value a | |
| Nutrient intake b | ||||||||
| Carbohydrates (g) | −0.027 (−0.061–0.007) | 0.122 | −0.016 (−0.068–0.036) | 0.554 | 0.000 (−0.006–0.005) | 0.891 | −0.001 (−0.004–0.002) | 0.531 |
| Protein (g) | 0.023 (−0.067–0.113) | 0.617 | −0.051 (−0.188–0.086) | 0.465 | −0.004 (−0.019–0.011) | 0.574 | −0.004 (−0.014–0.005) | 0.382 |
| Fat (g) | 0.071 (−0.014–0.155) | 0.100 | 0.069 (−0.059–0.196) | 0.291 | 0.003 (−0.011–0.018) | 0.652 | −0.002 (−0.010–0.007) | 0.711 |
| Dietary fiber (g) | 0.121 (−0.063–0.306) | 0.198 | 0.184 (−0.093–0.460) | 0.192 | −0.010 (−0.042–0.021) | 0.525 | 0.001 (−0.038–0.040) | 0.969 |
| Dietary Fe (mg) | 0.203 (−0.032–0.439) | 0.091 | 0.209 (−0.104–0.522) | 0.191 | −0.029 (−0.080–0.021) | 0.255 | −0.026 (−0.080–0.027) | 0.333 |
| Dietary folate (µg) | 0.008 (−0.009–0.025) | 0.338 | 0.006 (−0.018–0.031) | 0.602 | −0.002 (−0.005–−0.001) | 0.243 | −0.002 (−0.005–0.001) | 0.201 |
| Dietary vitamin B12 (µg) | 0.117 (−0.002–0.355) | 0.052 | 0.268 (−0.014–0.550) | 0.062 | −0.011 (−0.039–0.018) | 0.451 | −0.017 (−0.047–0.012) | 0.254 |
| Dietary vitamin C (mg) | 0.014 (0.001–0.026) | 0.041 | 0.014 (−0.004–0.031) | 0.136 | −0.000 (−0.003–0.002) | 0.942 | 0.001 (−0.002–0.004) | 0.560 |
| Food group b (frequency: times/month) | ||||||||
| Rice and rice porridge | −0.035 (−0.103–0.034) | 0.318 | −0.023 (−0.126–0.080) | 0.658 | −0.009 (−0.021–0.002) | 0.123 | −0.006 (−0.016–0.004) | 0.233 |
| Noodles and related products | 0.071 (−0.051–0.192) | 0.255 | 0.070 (−0.113–−0.253) | 0.453 | −0.008 (−0.029–0.012) | 0.421 | −0.022 (−0.043–−0.001) | 0.038 |
| Breakfast cereals, oats, and related products | −0.187 (−0.370–−0.003) | 0.046 | −0.295 (−0.567–−0.023) | 0.034 | 0.027 (−0.005–0.058) | 0.097 | 0.005 (−0.026–0.037) | 0.737 |
| Chinese dim sum and related foods | 0.033 (−0.090–0.156) | 0.603 | 0.063 (−0.123–0.249) | 0.505 | 0.007 (−0.014–0.028) | 0.506 | 0.037 (0.015–0.058) | 0.001 |
| Sweet buns, bean buns, and related products | 0.097 (−0.347–0.152) | 0.445 | −0.160 (−0.614–0.294) | 0.489 | −0.019 (−0.055–0.016) | 0.286 | −0.001 (−0.027–0.026) | 0.969 |
| Savory and sweet glutinous rice products | 0.677 (0.330–1.024) | <0.001 | 0.662 (0.218–1.107) | 0.004 | −0.007 (−0.091–0.076) | 0.862 | 0.017 (−0.064–0.097) | 0.683 |
| Light–colored vegetables | −0.075 (−0.150–0.001) | 0.052 | −0.079 (−0.201–0.042) | 0.201 | 0.003 (−0.009–0.015) | 0.602 | 0.003 (−0.011–0.017) | 0.693 |
| Dark leafy vegetables | −0.061 (−0.133–0.012) | 0.101 | −0.079 (−0.195–0.037) | 0.181 | 0.012 (0.000–0.023) | 0.006 | 0.013 (0.001–0.025) | 0.04 |
| Gourds, shoots, and root vegetables | −0.071 (−0.133–−0.010) | 0.022 | −0.066 (−0.165–0.033) | 0.190 | 0.004 (−0.006–0.014) | 0.403 | −0.009 (−0.018–0.001) | 0.076 |
| Legumes | −0.129 (−0.362–0.104) | 0.276 | −0.045 (−0.456–0.366) | 0.831 | −0.015 (−0.049–0.019) | 0.375 | −0.009 (−0.052–0.033) | 0.666 |
| Total vegetables | −0.024 −0.079–0.030) | 0.376 | −0.022 (−0.105–0.060) | 0.595 | 0.007 (−0.002–0.016) | 0.105 | 0.003 (−0.006–0.012) | 0.541 |
| Fresh fruits | −0.046 (−0.122–0.030) | 0.237 | −0.022 (−0.142–0.098) | 0.716 | 0.008 (0.005–0.020) | 0.220 | 0.003 (−0.009–0.015) | 0.637 |
| 100% pure fruit juice or fruit/vegetable juice | 0.140 (−0.017–0.298) | 0.08 | 0.173 (−0.057–0.404) | 0.140 | 0.018 (−0.010–0.046) | 0.198 | −0.010 (−0.035–0.014) | 0.392 |
| Canned fruits, dried fruits, and jam | 0.157 (0.009–0.304) | 0.037 | 0.176 (−0.018–0.370) | 0.076 | −0.014 (−0.046–0.019) | 0.415 | −0.005 (−0.042–0.032) | 0.8 |
| Fish, shellfish, and seafood | −0.014 (−0.097–0.068) | 0.733 | −0.001 (−0.132–0.130) | 0.991 | −0.014 (−0.046–0.019) | 0.415 | −0.002 (−0.015–0.011) | 0.764 |
| Roe and processed seafood products | 0.434 (−0.153–1.022) | 0.147 | 1.223 (0.321–2.124) | 0.008 | −0.021 (−0.118–0.077) | 0.678 | −0.015 (−0.099–0.070) | 0.731 |
| Poultry meat | −0.076 (−0.180–0.028) | 0.151 | −0.083 (−0.249–0.082) | 0.323 | −0.010 (−0.027–0.006) | 0.226 | −0.007 (−0.022–0.008) | 0.378 |
| Liver, organs, and blood products | 0.332 (0.139–0.526) | 0.001 | 0.489 (0.189–0.790) | 0.001 | 0.001 (−0.033–0.030) | 0.927 | 0.012 (−0.029–0.053) | 0.558 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayasari, N.R.; Bai, C.-H.; Hu, T.-Y.; Chao, J.C.-J.; Chen, Y.C.; Huang, Y.L.; Wang, F.-F.; Tinkov, A.A.; Skalny, A.V.; Chang, J.-S. Associations of Food and Nutrient Intake with Serum Hepcidin and the Risk of Gestational Iron-Deficiency Anemia among Pregnant Women: A Population-Based Study. Nutrients 2021, 13, 3501. https://doi.org/10.3390/nu13103501
Mayasari NR, Bai C-H, Hu T-Y, Chao JC-J, Chen YC, Huang YL, Wang F-F, Tinkov AA, Skalny AV, Chang J-S. Associations of Food and Nutrient Intake with Serum Hepcidin and the Risk of Gestational Iron-Deficiency Anemia among Pregnant Women: A Population-Based Study. Nutrients. 2021; 13(10):3501. https://doi.org/10.3390/nu13103501
Chicago/Turabian StyleMayasari, Noor Rohmah, Chyi-Huey Bai, Tzu-Yu Hu, Jane C.-J. Chao, Yi Chun Chen, Ya Li Huang, Fan-Fen Wang, Alexey A. Tinkov, Anatoly V. Skalny, and Jung-Su Chang. 2021. "Associations of Food and Nutrient Intake with Serum Hepcidin and the Risk of Gestational Iron-Deficiency Anemia among Pregnant Women: A Population-Based Study" Nutrients 13, no. 10: 3501. https://doi.org/10.3390/nu13103501
APA StyleMayasari, N. R., Bai, C.-H., Hu, T.-Y., Chao, J. C.-J., Chen, Y. C., Huang, Y. L., Wang, F.-F., Tinkov, A. A., Skalny, A. V., & Chang, J.-S. (2021). Associations of Food and Nutrient Intake with Serum Hepcidin and the Risk of Gestational Iron-Deficiency Anemia among Pregnant Women: A Population-Based Study. Nutrients, 13(10), 3501. https://doi.org/10.3390/nu13103501