
Can 3 mg·kg−1 of Caffeine Be Used as An Effective Nutritional Supplement to Enhance the Effects of Resistance Training in Rugby Union Players?


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
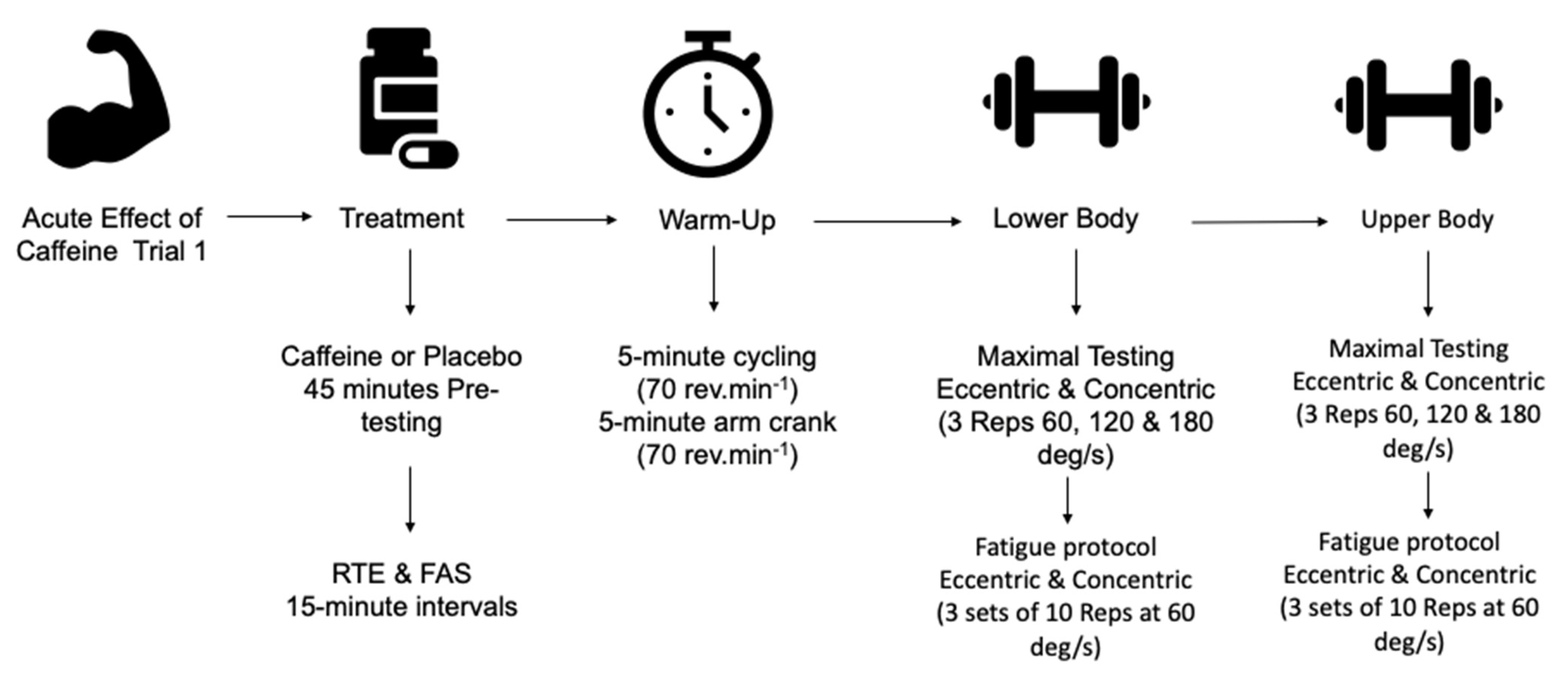
2.3. Acute Effect of Caffeine on Upper and Lower Body Strength
2.4. Familiarisation
2.5. Warm-Up
2.6. Isokinetic Strength Assessment
2.7. Experimental Trials
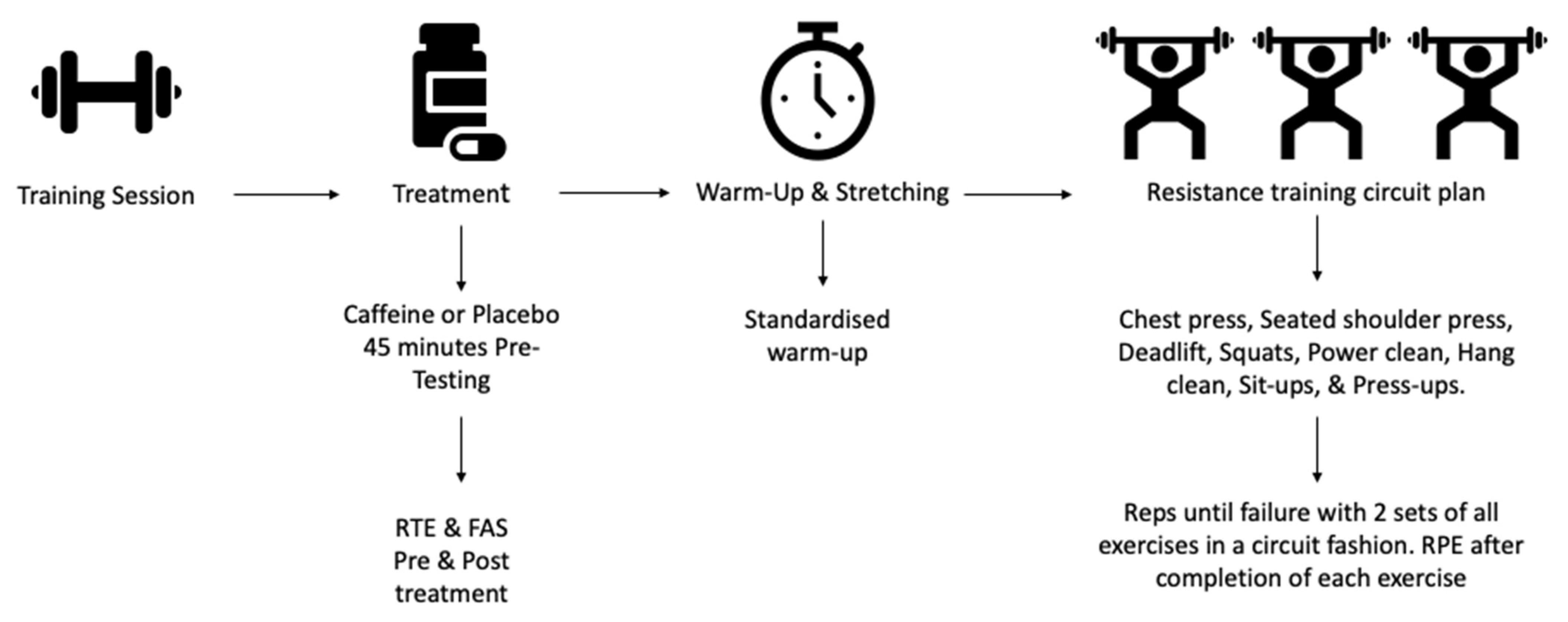
2.8. Chronic Effects of Caffeine Ingestion during a 7-Week Resistance Training Program
2.9. Assessment of 1 Repetition Maximum
2.10. Resistance Training Intervention (7-Weeks)
2.11. Statistical Analysis
3. Results
3.1. Participation Characteristics
3.2. Peak Torque
3.2.1. Elbow Extension Peak Torque
3.2.2. Elbow Flexion Peak Torque
3.2.3. Knee Extension Peak Torque
3.2.4. Knee Flexion Peak Torque
3.3. Total Work
3.3.1. Elbow Extension Total Work
3.3.2. Elbow Flexion Total Work
3.3.3. Knee Extension Total Work
3.3.4. Knee Flexion Total Work
3.4. Rate of Perceived Exertion
3.4.1. Elbow Extension Rate of Perceived Exertion
3.4.2. Elbow Flexion Rate of Perceived Exertion
3.4.3. Knee Extension Rate of Perceived Exertion
3.4.4. Knee Flexion Rate of Perceived Exertion
3.5. Readiness to Invest Effort and Felt Arousal Scale
3.6. 1RM
3.7. Intervention Repetitions until Failure
3.8. Intervention RPE
4. Discussion
4.1. Acute Effects of Caffeine on Muscular Strength
4.2. Habituation to Chronic Caffeine Consumption
4.3. Effects of Chronic Caffeine Consumption on Resistance Training
5. Limitations and Future Direction
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. Wake up and smell the coffee: Caffeine supplementation and exercise performance—An umbrella review of 21 published meta-analyses. Br. J. Sports Med. 2020, 54, 681–688. [Google Scholar] [CrossRef]
- Astorino, T.A.; Roberson, D.W. Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: A systematic review. J. Strength Cond. Res. 2010, 24, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Trexler, E.T.; Lazinica, B.; Pedisic, Z. Effects of caffeine intake on muscle strength and power: A systematic review and meta-analysis. J. Int. Soc. Sports Nutr. 2018, 15, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polito, M.D.; Souza, D.B.; Casonatto, J.; Farinatti, P. Acute effect of caffeine consumption on isotonic muscular strength and endurance: A systematic review and meta-analysis. Sci. Sports 2016, 31, 119–128. [Google Scholar] [CrossRef]
- Grgic, J.; Pickering, C. The effects of caffeine ingestion on isokinetic muscular strength: A meta-analysis. J. Sci. Med. Sport 2019, 22, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Salinero, J.J.; Lara, B.; Del Coso, J. Effects of acute ingestion of caffeine on team sports performance: A systematic review and meta-analysis. Res. Sports Med. 2019, 27, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Park, N.D.; Maresca, R.D.; McKibans, K.I.; Millard-Stafford, M.L. Effect of caffeine ingestion on muscular strength and endurance: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef]
- Grgic, J.; Mikulic, P.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. The influence of caffeine supplementation on resistance exercise: A review. Sports Med. 2019, 49, 17–30. [Google Scholar] [CrossRef]
- Kemp, J.; Eaton, T.; Jarvis, S.; Meehan, D.; Whyte, D.G. Caffeine improves strength gains in response to 6 weeks of resistance training. J. Aust. Strength Cond. 2012, 20, 48–51. [Google Scholar]
- Del Coso, J.; Lara, B.; Ruiz-Moreno, C.; Salinero, J.J. Challenging the myth of non-response to the ergogenic effects of caffeine ingestion on exercise performance. Nutrients 2019, 11, 732. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, L.d.S.; Painelli, V.d.S.; Yamaguchi, G.; Oliveira, L.F.d.; Saunders, B.; da Silva, R.P.; Maciel, E.; Artioli, G.G.; Roschel, H.; Gualano, B. Dispelling the myth that habitual caffeine consumption influences the performance response to acute caffeine supplementation. J. Appl. Physiol. 2017, 123, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Lara, B.; Ruiz-Moreno, C.; Salinero, J.J.; Del Coso, J. Time course of tolerance to the performance benefits of caffeine. PLoS ONE 2019, 14, e0210275. [Google Scholar] [CrossRef] [Green Version]
- Beaumont, R.; Cordery, P.; Funnell, M.; Mears, S.; James, L.; Watson, P. Chronic ingestion of a low dose of caffeine induces tolerance to the performance benefits of caffeine. J. Sports Sci. 2017, 35, 1920–1927. [Google Scholar] [CrossRef]
- Wilk, M.; Filip, A.; Krzysztofik, M.; Maszczyk, A.; Zajac, A. The acute effect of various doses of caffeine on power output and velocity during the bench press exercise among athletes habitually using caffeine. Nutrients 2019, 11, 1465. [Google Scholar] [CrossRef] [Green Version]
- Filip, A.; Wilk, M.; Krzysztofik, M.; Del Coso, J. Inconsistency in the ergogenic effect of caffeine in athletes who regularly consume caffeine: Is it due to the disparity in the criteria that defines habitual caffeine intake? Nutrients 2020, 12, 1087. [Google Scholar] [CrossRef] [Green Version]
- Giráldez-Costas, V.; Ruiz Moreno, C.; González-García, J.; Lara, B.; Del Coso, J.; Salinero, J.J. Pre-exercise caffeine intake enhances bench press strength training adaptations. Front. Nutr. 2021, 8, 3. [Google Scholar] [CrossRef]
- Tallis, J.; Yavuz, H.C. The effects of low and moderate doses of caffeine supplementation on upper and lower body maximal voluntary concentric and eccentric muscle force. Appl. Physiol. Nutr. Metab. 2018, 43, 274–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tallis, J.; Muhammad, B.; Islam, M.; Duncan, M.J. Placebo effects of caffeine on maximal voluntary concentric force of the knee flexors and extensors. Muscle Nerve 2016, 54, 479–486. [Google Scholar] [CrossRef]
- Timmins, T.D.; Saunders, D.H. Effect of caffeine ingestion on maximal voluntary contraction strength in upper-and lower-body muscle groups. J. Strength Cond. Res. 2014, 28, 3239–3244. [Google Scholar] [CrossRef] [PubMed]
- Tallis, J.; James, R.S.; Cox, V.M.; Duncan, M.J. Is the ergogenicity of caffeine affected by increasing age? The direct effect of a physiological concentration of caffeine on the power output of maximally stimulated EDL and diaphragm muscle isolated from the mouse. J. Nutr. Health Aging 2017, 21, 440–448. [Google Scholar] [CrossRef] [PubMed]
- General Assembly of the World Medical Association World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18.
- Tallis, J.; Duncan, M.J.; James, R.S. What can isolated skeletal muscle experiments tell us about the effects of caffeine on exercise performance? Br. J. Pharmacol. 2015, 172, 3703–3713. [Google Scholar] [CrossRef] [Green Version]
- Graham, T.E. Caffeine and exercise. Sports Med. 2001, 31, 785–807. [Google Scholar] [CrossRef] [PubMed]
- Shohet, K.L.; Landrum, R.E. Caffeine consumption questionnaire: A standardized measure for caffeine consumption in undergraduate students. Psychol Rep 2001, 89, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Huntley, E.D.; Juliano, L.M. Caffeine Expectancy Questionnaire (CaffEQ): Construction, psychometric properties, and associations with caffeine use, caffeine dependence, and other related variables. Psychol. Assess. 2012, 24, 592. [Google Scholar] [CrossRef] [PubMed]
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PMR 2011, 3, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Habets, B.; Staal, J.B.; Tijssen, M.; van Cingel, R. Intrarater reliability of the Humac NORM isokinetic dynamometer for strength measurements of the knee and shoulder muscles. BMC Res. Notes 2018, 11, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seven, B.; Cobanoglu, G.; Oskay, D.; Atalay-Guzel, N. Test–Retest Reliability of Isokinetic Wrist Strength and Proprioception Measurements. J. Sport Rehabil. 2019, 28. [Google Scholar] [CrossRef] [Green Version]
- Eustace, S.J.; Page, R.M.; Greig, M. Angle-specific isokinetic metrics highlight strength training needs of elite youth soccer players. J. Strength Cond. Res. 2020, 34, 3258–3265. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Duncan, M.J.; Smith, M.; Cook, K.; James, R.S. The acute effect of a caffeine-containing energy drink on mood state, readiness to invest effort, and resistance exercise to failure. J. Strength Cond. Res. 2012, 26, 2858–2865. [Google Scholar] [CrossRef] [Green Version]
- Raedeke, T.D.; Focht, B.C.; Scales, D. Mediators of affective responses to acute exercise among women with high social physique anxiety. Psychol. Sport Exerc. 2009, 10, 573–578. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Beckham, G.K.; Wright, G.A. The impact of load on lower body performance variables during the hang power clean. Sports Biomech. 2014, 13, 87–95. [Google Scholar] [CrossRef]
- Kawamori, N.; Crum, A.J.; Blumert, P.A.; Kulik, J.R. Influence of different relative intensities on power output during the hang power clean: Identification of the optimal load. J. Strength Cond. Res. 2005, 19, 698. [Google Scholar] [CrossRef]
- MacKenzie, S.J.; Lavers, R.J.; Wallace, B.B. A biomechanical comparison of the vertical jump, power clean, and jump squat. J. Sports Sci. 2014, 32, 1576–1585. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Fry, A.C.; Ratamess, N.; French, D. Strength testing: Development and evaluation of methodology. Physiol. Assess. Hum. Fit. 1995, 2, 119–150. [Google Scholar]
- Aragón-Vela, J.; Casuso, R.A.; Casals, C.; Plaza-Díaz, J.; Fontana, L.; Huertas, J.R. Differential IL 10 serum production between an arm-based and a leg-based maximal resistance test. Cytokine 2020, 126, 154915. [Google Scholar] [CrossRef] [PubMed]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Duncan, M.J.; Oxford, S.W. Acute caffeine ingestion enhances performance and dampens muscle pain following resistance exercise to failure. J. Sports Med. Phys. Fit. 2012, 52, 280–285. [Google Scholar]
- Duncan, M.J.; Oxford, S.W. The effect of caffeine ingestion on mood state and bench press performance to failure. J. Strength Cond. Res. 2011, 25, 178–185. [Google Scholar] [CrossRef]
- Martorelli, S.; Cadore, E.L.; Izquierdo, M.; Celes, R.; Martorelli, A.; Cleto, V.A.; Alvarenga, J.G.; Bottaro, M. Strength training with repetitions to failure does not provide additional strength and muscle hypertrophy gains in young women. Eur. J. Transl. Myol. 2017, 27, 6339. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.D.; Cribb, P.J.; Cooke, M.B.; Hayes, A. The effect of ephedra and caffeine on maximal strength and power in resistance-trained athletes. J. Strength Cond. Res. 2008, 22, 464–470. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise; Columbia University: Columbia, SC, USA, 2011. [Google Scholar] [CrossRef]
- Willardson, J.M. The application of training to failure in periodized multiple-set resistance exercise programs. J. Strength Cond. Res. 2007, 21, 628. [Google Scholar]
- Rooney, K.J.; Herbert, R.D.; Balnave, R.J. Fatigue contributes to the strength training stimulus. Med. Sci. Sports Exerc. 1994, 26, 1160–1164. [Google Scholar] [PubMed]
- Drinkwater, E.J.; Lawton, T.W.; Lindsell, R.P.; Pyne, D.B.; Hunt, P.H.; McKenna, M.J. Training leading to repetition failure enhances bench press strength gains in elite junior athletes. J. Strength Cond. Res. 2005, 19, 382–388. [Google Scholar] [PubMed] [Green Version]
- Davies, T.; Orr, R.; Halaki, M.; Hackett, D. Effect of training leading to repetition failure on muscular strength: A systematic review and meta-analysis. Sports Med. 2016, 46, 487–502. [Google Scholar] [CrossRef]
- van Ginkel, J.R. SPSS Syntax for Applying Rules for Combining Multivariate Estimates in Multiple Imputation; Leiden University: Leiden, The Netherlands, 2014. [Google Scholar]
- van Ginkel, J.R.; Kroonenberg, P.M. Analysis of variance of multiply imputed data. Multivar. Behav. Res. 2014, 49, 78–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanca, M.J.; Alarcón, R.; Arnau, J.; Bono, R.; Bendayan, R. Non-normal data: Is ANOVA still a valid option? Psicothema 2017, 29, 552–557. [Google Scholar] [PubMed]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Okada, M.; Kiryu, K.; Kawata, Y.; Mizuno, K.; Wada, K.; Tasaki, H.; Kaneko, S. Determination of the effects of caffeine and carbamazepine on striatal dopamine release by in vivo microdialysis. Eur. J. Pharmacol. 1997, 321, 181–188. [Google Scholar] [CrossRef]
- Fredholm, B.B. Adenosine, adenosine receptors and the actions of caffeine. Pharmacol. Toxicol. 1995, 76, 93–101. [Google Scholar] [CrossRef]
- Fredholm, B.B. On the mechanism of action of theophylline and caffeine. Acta Med. Scand. 1985, 217, 149–153. [Google Scholar] [CrossRef]
- Rall, T. Evolution of the mechanism of action of methylxanthines: From calcium mobilizers to antagonists of adenosine receptors. Pharmacologist 1982, 24, 277–287. [Google Scholar]
- Davis, J.K.; Green, J.M. Caffeine and anaerobic performance. Sports Med. 2009, 39, 813–832. [Google Scholar] [CrossRef]
- Dunford, M.; Doyle, J.A. Nutrition for Sport and Exercise; Cengage Learning: Boston, MA, USA, 2008. [Google Scholar]
- Hodgson, A.B.; Randell, R.K.; Jeukendrup, A.E. The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS ONE 2013, 8, e59561. [Google Scholar] [CrossRef] [Green Version]
- Damiani, E.; Larsson, L.; Margreth, A. Age-related abnormalities in regulation of the ryanodine receptor in rat fast-twitch muscle. Cell Calcium 1996, 19, 15–27. [Google Scholar] [CrossRef]
- Bhat, M.B.; Zhao, J.; Zang, W.; Balke, C.W.; Takeshima, H.; Wier, W.G.; Ma, J. Caffeine-induced release of intracellular Ca2 from Chinese hamster ovary cells expressing skeletal muscle ryanodine receptor: Effects on full-length and carboxyl-terminal portion of Ca2 release channels. J. Gen. Physiol. 1997, 110, 749–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredholm, B.B.; Bättig, K.; Holmén, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 1999, 51, 83–133. [Google Scholar] [PubMed]
- Rossi, R.; Bottinelli, R.; Sorrentino, V.; Reggiani, C. Response to caffeine and ryanodine receptor isoforms in mouse skeletal muscles. Am. J. Physiol.-Cell Physiol. 2001, 281, C585–C594. [Google Scholar] [CrossRef]
- Allen, D.G.; Lee, J.A.; Westerblad, H. Intracellular calcium and tension during fatigue in isolated single muscle fibres from Xenopus laevis. J. Physiol. 1989, 415, 433–458. [Google Scholar] [CrossRef]
- Westerblad, H.; Allen, D.G. Changes of myoplasmic calcium concentration during fatigue in single mouse muscle fibers. J. Gen. Physiol. 1991, 98, 615–635. [Google Scholar] [CrossRef] [Green Version]
- Allen, D.G.; Westerblad, H. The effects of caffeine on intracellular calcium, force and the rate of relaxation of mouse skeletal muscle. J. Physiol. 1995, 487, 331–342. [Google Scholar] [CrossRef]
- Astorino, T.A.; Terzi, M.N.; Roberson, D.W.; Burnett, T.R. Effect of two doses of caffeine on muscular function during isokinetic exercise. Med. Sci. Sports Exerc. 2010, 42, 2205–2210. [Google Scholar] [CrossRef]
- Da Silva, V.L.; Messias, F.R.; Zanchi, N.E.; Gerlinger-Romero, F.; Duncan, M.J.; Guimarães-Ferreira, L. Effects of acute caffeine ingestion on resistance training performance and perceptual responses during repeated sets to failure. J. Sports Med. Phys. Fit. 2015, 55, 383–389. [Google Scholar]
- Duncan, M.J.; Stanley, M.; Parkhouse, N.; Cook, K.; Smith, M. Acute caffeine ingestion enhances strength performance and reduces perceived exertion and muscle pain perception during resistance exercise. Eur. J. Sport Sci. 2013, 13, 392–399. [Google Scholar] [CrossRef]
- Arazi, H.; Sotoudeh, K.; Sadeghi, M.M.; Mohammadi, S.M.; Saeedi, T. Influence of Upper-Body Exercise Order on Repetition Performance and Ratings of Perceived Exertion during a Super-Set Resistance Training Session. J. Sport Sci. 2015, 8, 24–27. [Google Scholar]
- Grgic, J.; Mikulic, P. Caffeine ingestion acutely enhances muscular strength and power but not muscular endurance in resistance-trained men. Eur. J. Sport Sci. 2017, 17, 1029–1036. [Google Scholar] [CrossRef]
- de Azevedo, A.P.; Guerra, M.A.; Caldas, L.C.; Guimarães-Ferreira, L. Acute caffeine ingestion did not enhance punch performance in professional mixed-martial arts athletes. Nutrients 2019, 11, 1422. [Google Scholar] [CrossRef] [Green Version]
- Bell, D.G.; McLellan, T.M. Exercise endurance 1, 3, and 6 h after caffeine ingestion in caffeine users and nonusers. J. Appl. Physiol. 2002, 93, 1227–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilk, M.; Filip, A.; Krzysztofik, M.; Gepfert, M.; Zajac, A.; Del Coso, J. Acute caffeine intake enhances mean power output and bar velocity during the bench press throw in athletes habituated to caffeine. Nutrients 2020, 12, 406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grgic, J.; Mikulic, P. Acute effects of caffeine supplementation on resistance exercise, jumping, and Wingate performance: No influence of habitual caffeine intake. Eur. J. Sport Sci. 2020, 1–11. [Google Scholar] [CrossRef]
- Wilk, M.; Krzysztofik, M.; Filip, A.; Zajac, A.; Del Coso, J. Correction: Wilk et al. “The Effects of High Doses of Caffeine on Maximal Strength and Muscular Endurance in Athletes Habituated to Caffeine” Nutrients 2019, 11(8), 1912. Nutrients 2019, 11, 2660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, T.D.; Tolusso, D.V.; Fedewa, M.V.; Esco, M.R. Comparison of periodized and non-periodized resistance training on maximal strength: A meta-analysis. Sports Med. 2017, 47, 2083–2100. [Google Scholar] [CrossRef]
- Pakulak, A.; Candow, D.G.; Totosy de Zepetnek, J.; Forbes, S.C.; Basta, D. Effects of Creatine and Caffeine Supplementation During Resistance Training on Body Composition, Strength, Endurance, Rating of Perceived Exertion and Fatigue in Trained Young Adults. J. Diet. Suppl. 2021, 1–16. [Google Scholar] [CrossRef]
- Astorino, T.A.; Cottrell, T.; Lozano, A.T.; Aburto-Pratt, K.; Duhon, J. Effect of caffeine on RPE and perceptions of pain, arousal, and pleasure/displeasure during a cycling time trial in endurance trained and active men. Physiol Behav 2012, 106, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.H.; Wyld, K.; Chrismas, B.C. Acute Effects of Caffeine on Strength Performance in Trained and Untrained Individuals. J. Athl. Enhanc. 2015, 5, 31–33. [Google Scholar] [CrossRef]
- Mizuno, M.; Kimura, Y.; Tokizawa, K.; Ishii, K.; Oda, K.; Sasaki, T.; Nakamura, Y.; Muraoka, I.; Ishiwata, K. Greater adenosine A2A receptor densities in cardiac and skeletal muscle in endurance-trained men: A [11C] TMSX PET study. Nucl. Med. Biol. 2005, 32, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Pickering, C.; Kiely, J. What should we do about habitual caffeine use in athletes? Sports Med. 2019, 49, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porterfield, S.; Linderman, J.; Laubach, L.L.; Daprano, C.M. Comparison of the effect of caffeine ingestion on time to exhaustion between endurance trained and untrained men. J. Exerc. Physiol.-Online 2013, 16, 90–99. [Google Scholar]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of resistance training frequency on gains in muscular strength: A systematic review and meta-analysis. Sports Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef]
- Fulton, J.L.; Dinas, P.C.; Carrillo, A.E.; Edsall, J.R.; Ryan, E.J.; Ryan, E.J. Impact of genetic variability on physiological responses to caffeine in humans: A systematic review. Nutrients 2018, 10, 1373. [Google Scholar] [CrossRef] [Green Version]
- Southward, K.; Rutherfurd-Markwick, K.; Badenhorst, C.; Ali, A. The role of genetics in moderating the inter-individual differences in the ergogenicity of caffeine. Nutrients 2018, 10, 1352. [Google Scholar] [CrossRef] [Green Version]
- Tennent, R.; Ali, A.; Wham, C.; Rutherfurd-Markwick, K. Narrative Review: Impact of Genetic Variability of CYP1A2, ADORA2A, and AHR on Caffeine Consumption and Response. J. Caffeine Adenosine Res. 2020, 10, 125–134. [Google Scholar] [CrossRef]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on exercise testing: A meta-analysis. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 626–646. [Google Scholar] [CrossRef]
- Ganio, M.S.; Klau, J.F.; Casa, D.J.; Armstrong, L.E.; Maresh, C.M. Effect of caffeine on sport-specific endurance performance: A systematic review. J. Strength Cond. Res. 2009, 23, 315–324. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. Are low doses of caffeine as ergogenic as higher doses? A critical review highlighting the need for comparison with current best practice in caffeine research. Nutrition 2019, 67, 110535. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Ayuso, J.; Marques-Jiménez, D.; Refoyo, I.; Del Coso, J.; León-Guereño, P.; Calleja-González, J. Effect of caffeine supplementation on sports performance based on differences between sexes: A systematic review. Nutrients 2019, 11, 2313. [Google Scholar] [CrossRef] [Green Version]
- Grgic, J. Effects of Caffeine on Resistance Exercise: A Review of Recent Research. Sports Med. 2021, 1–18. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Caffeine Intervention Group | Placebo Intervention Group | |
|---|---|---|
| Caffeine Intake | 133 ± 123 mg/day | 121 ± 95 mg/day |
| Withdrawal/ Dependence (n = 12) | 2 ± 1 | 2 ± 1 |
| Energy/ Work Enhancement (n = 8) | 4 ± 1 | 5 ± 1 |
| Appetite Suppression (n = 5) | 2 ± 1 | 3 ± 1 |
| Social mood Enhancement (n = 6) | 3 ± 1 | 3 ± 1 |
| Physical Performance Enhancement (n = 3) | 3 ± 1 | 4 ± 1 |
| Anxiety/ Negative Physical Effect (n = 9) | 2 ± 1 | 2 ± 1 |
| Sleep Disturbance (n = 4) | 3 ± 1 | 4 ± 1 |
| Total Questions (n = 47) |
| Caffeine Intervention Group | Placebo Intervention Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Angular Velocity (Deg/s) | Acute Placebo | Acute Caffeine | Acute Placebo | Acute Caffeine | |||||
| Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | ||
| Elbow Extension | |||||||||
| Con | 60 | 38 ± 8 | 42 ± 8 | 41 ± 12 | 40 ± 7 | 36 ± 10 | 41 ± 11 | 42 ± 14 | 42 ± 10 |
| 120 | 32 ± 8 | 38 ± 9 | 38 ± 14 | 35 ± 6 | 30 ± 9 | 35 ± 11 | 36 ± 14 | 38 ± 8 | |
| 180 | 30 ± 6 | 32 ± 7 | 33 ± 15 | 32 ± 6 | 30 ± 9 | 32 ± 8 | 32 ± 8 | 36 ± 8 | |
| Ecc | 60 | 44 ± 11 | 48 ± 9 | 50 ± 16 | 46 ± 10 | 46 ± 18 | 48 ± 15 | 51 ± 17 | 49 ± 17 |
| 120 | 40 ± 10 * | 46 ± 8 ^ | 56 ± 19 * | 48 ± 8 ^ | 41 ± 22 * | 49 ± 13 ^ | 52 ± 13 * | 54 ± 25 ^ | |
| 180 | 40 ± 10 * | 49 ± 10 ^ | 59 ± 20 * | 50 ± 11 ^ | 44 ± 28 * | 51 ± 14 ^ | 55 ± 16 * | 62 ± 27 ^ | |
| Elbow Flexion | |||||||||
| Con | 60 | 51 ± 7 *# | 56 ± 10 ^# | 58 ± 16 *# | 56 ± 9 ^# | 51 ± 10 | 56 ± 15 | 60 ± 16 # | 61 ± 18 # |
| 120 | 50 ± 10 *# | 51 ± 9 ^# | 52 ± 15 *# | 53 ± 10 ^# | 45 ± 11 | 54 ± 16 | 55 ± 15 # | 58 ± 11 # | |
| 180 | 45 ± 8 # | 48 ± 7 ^# | 48 ± 15 # | 49 ± 9 # | 50 ± 12 | 49 ± 14 | 41 ± 11 # | 50 ± 10 # | |
| Ecc | 60 | 54 ± 15 | 59 ± 12 | 61 ± 15 | 63 ± 21 | 62 ± 17 | 68 ± 22 | 64 ± 16 | 67 ± 21 |
| 120 | 61 ± 17 | 59 ± 12 | 61 ± 15 | 63 ± 16 | 59 ± 13 | 68 ± 20 | 68 ± 19 | 70 ± 19 | |
| 180 | 61 ± 14 | 63 ± 10 | 61 ± 14 | 66 ± 14 | 65 ± 11 | 70 ± 17 | 62 ± 20 | 72 ± 19 | |
| Knee Extension | |||||||||
| Con | 60 | 147 ± 47 # | 181 ± 67 # | 167 ± 61 | 188 ± 69 | 179 ± 59 | 187 ± 49 | 190 ± 41 | 175 ± 41 |
| 120 | 139 ± 49 # | 160 ± 56 # | 150 ± 50 | 177 ± 62 | 153 ± 70 | 159 ± 65 | 166 ± 51 | 149 ± 41 | |
| 180 | 121 ± 46 # | 142 ± 52 # | 126 ± 58 | 141 ± 49 | 140 ± 54 | 122 ± 37 | 146 ± 63 | 126 ± 48 | |
| Ecc | 60 | 156 ± 56 | 187 ± 66 | 187 ± 76 | 203 ± 73 | 192 ± 74 | 211 ± 72 | 212 ± 74 | 205 ± 52 |
| 120 | 167 ± 54 | 174 ± 50 | 192 ± 75 | 221 ± 69 | 207 ± 76 | 208 ± 64 | 227 ± 88 | 189 ± 49 | |
| 180 | 161 ± 72 | 183 ± 46 | 202 ± 61 | 206 ± 60 | 225 ± 82 | 200 ± 61 | 230 ± 89 | 200 ± 52 | |
| Knee Flexion | |||||||||
| Con | 60 | 92 ± 33 # | 112 ± 37 # | 103 ± 31 | 124 ± 38 | 111 ± 44 # | 115 ± 45 # | 119 ± 42 | 120 ± 45 |
| 120 | 90 ± 32 # | 106 ± 33 # | 100 ± 37 | 119 ± 21 | 100 ± 40 # | 107 ± 42 # | 100 ± 35 | 100 ± 36 | |
| 180 | 80 ± 27 # | 96 ± 26 # | 89 ± 34 | 105 ± 25 | 87 ± 36 # | 97 ± 32 # | 97 ± 34 | 97 ± 32 | |
| Ecc | 60 | 99 ± 37 | 125 ± 40 | 115 ± 36 | 135 ± 52 | 125 ± 47 | 140 ± 56 | 132 ± 45 | 142 ± 46 |
| 120 | 98 ± 40 | 126 ± 46 | 121 ± 40 | 145 ± 37 | 125 ± 42 | 130 ± 50 | 119 ± 44 | 137 ± 50 | |
| 180 | 92 ± 27 | 119 ± 39 | 113 ± 30 | 142 ± 37 | 120 ± 43 | 128 ± 40 | 122 ± 40 | 138 ± 54 | |
| Caffeine Intervention Group | Placebo Intervention Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Set | Acute Placebo | Acute Caffeine | Acute Placebo | Acute Caffeine | |||||
| Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | ||
| Elbow Extension | |||||||||
| Con | Set 1 | 393 ± 168 | 370 ± 66 | 348 ± 75 | 411 ± 228 | 344 ± 87 | 349 ± 105 | 369 ± 137 | 356 ± 66 |
| Set 2 | 298 ± 140 | 281 ± 63 | 266 ± 60 | 328 ± 230 | 277 ± 86 | 278 ± 63 | 311 ± 124 | 314 ± 85 | |
| Set 3 | 232 ± 138 | 216 ± 53 | 216 ± 74 | 268 ± 213 | 213 ± 78 | 220 ± 61 | 246 ± 112 | 262 ± 98 | |
| Ecc | Set 1 | 428 ± 309 | 381 ± 91 | 410 ± 118 | 421 ± 193 | 366 ± 202 | 398 ± 132 | 444 ± 167 | 425 ± 141 |
| Set 2 | 334 ± 253 | 313 ± 72 | 334 ± 94 | 339 ± 225 | 303 ± 161 | 336 ± 108 | 478 ± 533 | 346 ± 131 | |
| Set 3 | 279 ± 266 | 248 ± 52 | 265 ± 67 | 295 ± 208 | 237 ± 127 | 278 ± 104 | 303 ± 130 | 280 ± 95 | |
| Elbow Flexion | |||||||||
| Con | Set 1 | 486 ± 116 | 458 ± 91 | 490 ± 102 | 463 ± 71 | 500 ± 119 | 463 ± 107 | 523 ± 129 | 478 ± 92 |
| Set 2 | 377 ± 84 | 361 ± 70 | 369 ± 90 | 360 ± 82 | 395 ± 77 | 383 ± 104 | 412 ± 68 | 403 ± 76 | |
| Set 3 | 312 ± 69 | 319 ± 78 | 321 ± 87 | 315 ± 71 | 341 ± 67 | 325 ± 68 | 362 ± 83 | 354 ± 80 | |
| Ecc | Set 1 | 538 ± 166 * | 463 ± 87 ^ | 551 ± 134 * | 505 ± 131 ^ | 493 ± 187 * | 521 ± 205 ^ | 587 ± 194 * | 537 ± 156 ^ |
| Set 2 | 416 ± 149 * | 376 ± 80 ^ | 431 ± 118 * | 402 ± 126 ^ | 408 ± 136 * | 453 ± 149 ^ | 472 ± 133 * | 448 ± 97 ^ | |
| Set 3 | 345 ± 116 * | 352 ± 89 ^ | 373 ± 85 * | 345 ± 95 ^ | 372 ± 114 * | 389 ± 104 ^ | 425 ± 135 * | 409 ± 122 ^ | |
| Knee Extension | |||||||||
| Con | Set 1 | 612 ± 359 *# | 1010 ± 361 # | 1080 ± 375 * | 1045 ± 374 | 648 ± 402 *# | 1036 ± 250 # | 981 ± 304 * | 1120 ± 279 |
| Set 2 | 553 ± 342 *# | 980 ± 351 # | 989 ± 278 * | 971 ± 296 | 603 ± 403 *# | 1006 ± 237 # | 1013 ± 164 * | 1003 ± 189 | |
| Set 3 | 495 ± 325 *# | 856 ± 250 # | 911 ± 265 * | 893 ± 252 | 598 ± 454 *# | 903 ± 169 # | 967 ± 206 * | 915 ± 124 | |
| Ecc | Set 1 | 586 ± 267 | 1036 ± 383 | 1179 ± 417 | 1144 ± 466 | 738 ± 407 | 1251 ± 423 | 1223 ± 401 | 1246 ± 275 |
| Set 2 | 503 ± 261 | 1011 ± 353 | 1084 ± 351 | 1061 ± 453 | 552 ± 345 | 1238 ± 411 | 1213 ± 320 | 1176 ± 253 | |
| Set 3 | 435 ± 216 | 918 ± 301 | 990 ± 314 | 940 ± 368 | 572 ± 334 | 1171 ± 375 | 1110 ± 370 | 1146 ± 304 | |
| Knee Flexion | |||||||||
| Con | Set 1 | 524 ± 99 | 574 ± 179 | 569 ± 179 | 644 ± 169 | 547 ± 152 | 542 ± 127 | 563 ± 144 | 542 ± 144 |
| Set 2 | 442 ± 114 | 521 ± 173 | 485 ± 137 | 568 ± 104 | 448 ± 115 | 449 ± 96 | 477 ± 132 | 492 ± 150 | |
| Set 3 | 404 ± 116 | 467 ± 140 | 476 ± 125 | 503 ± 97 | 379 ± 109 | 421 ± 110 | 450 ± 120 | 441 ± 108 | |
| Ecc | Set 1 | 505 ± 178 * | 630 ± 241 ^ | 601 ± 235 * | 699 ± 261 ^ | 610 ± 214 * | 657 ± 210 ^ | 668 ± 235 * | 630 ± 166 ^ |
| Set 2 | 496 ± 268 | 537 ± 200 | 528 ± 172 | 610 ± 220 | 514 ± 168 * | 542 ± 165 ^ | 589 ± 213 * | 578 ± 173 ^ | |
| Set 3 | 422 ± 214 | 516 ± 193 | 482 ± 163 | 561 ± 203 | 430 ± 112 * | 536 ± 182 ^ | 551 ± 199 * | 545 ± 126 ^ | |
| Caffeine Intervention Group | Placebo Intervention Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Acute Placebo | Acute Caffeine | Acute Placebo | Acute Caffeine | ||||||
| Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | Pre-Int | Post-Int | ||
| Elbow Extension | Set1 | 14 ± 3 | 16 ± 2 | 13 ± 2 | 16 ± 2 | 14 ± 2 | 14 ± 3 | 14 ± 2 | 15 ± 2 |
| Set2 | 15 ± 2 | 17 ± 2 | 15 ± 2 | 17 ± 2 | 15 ± 2 | 15 ± 3 ^ | 15 ± 2 | 17 ± 1 ^ | |
| Set3 | 17 ± 2 | 19 ± 2 | 16 ± 2 | 19 ± 1 | 17 ± 1 | 16 ± 3 ^ | 17 ± 2 | 18 ± 2 ^ | |
| Elbow Flexion | Set1 | 14 ± 3 | 16 ± 2 | 14 ± 2 | 16 ± 2 | 14 ± 2 | 17 ± 2 | 14 ± 2 | 16 ± 2 |
| Set2 | 15 ± 2 | 18 ± 2 | 16 ± 2 | 17 ± 2 | 16 ± 2 | 18 ± 1 | 15 ± 2 | 18 ± 1 | |
| Set3 | 17 ± 2 | 19 ± 2 | 17 ± 2 | 18 ± 2 | 17 ± 1 | 19 ± 1 | 17 ± 2 | 19 ± 1 | |
| Knee Extension | Set1 | 13 ± 3 | 17 ± 2 | 14 ± 2 | 16 ± 3 | 13 ± 3 | 16 ± 2 | 14 ± 2 | 16 ± 2 |
| Set2 | 14 ± 3 | 18 ± 2 | 15 ± 2 | 17 ± 3 | 13 ± 3 | 18 ± 1 | 16 ± 2 | 18 ± 1 | |
| Set3 | 15 ± 2 | 19 ± 2 | 17 ± 2 | 18 ± 3 | 14 ± 3 | 19 ± 1 | 17 ± 2 | 19 ± 1 | |
| Knee Flexion | Set1 | 14 ± 2 | 16 ± 1 | 14 ± 2 | 16 ± 2 | 14 ± 3 | 16 ± 2 | 14 ± 2 | 16 ± 3 |
| Set2 | 15 ± 2 | 17 ± 2 | 15 ± 2 | 17 ± 2 | 15 ± 2 | 17 ± 1 | 16 ± 2 | 17 ± 2 | |
| Set3 | 17 ± 2 | 19 ± 2 | 17 ± 2 | 18 ± 2 | 17 ± 2 | 19 ± 1 | 17 ± 2 | 19 ± 1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamilio, R.A.; Clarke, N.D.; Duncan, M.J.; Morris, R.; Grgic, J.; Tallis, J. Can 3 mg·kg−1 of Caffeine Be Used as An Effective Nutritional Supplement to Enhance the Effects of Resistance Training in Rugby Union Players? Nutrients 2021, 13, 3367. https://doi.org/10.3390/nu13103367
Tamilio RA, Clarke ND, Duncan MJ, Morris R, Grgic J, Tallis J. Can 3 mg·kg−1 of Caffeine Be Used as An Effective Nutritional Supplement to Enhance the Effects of Resistance Training in Rugby Union Players? Nutrients. 2021; 13(10):3367. https://doi.org/10.3390/nu13103367
Chicago/Turabian StyleTamilio, Ryan A., Neil D. Clarke, Michael J. Duncan, Rhys Morris, Jozo Grgic, and Jason Tallis. 2021. "Can 3 mg·kg−1 of Caffeine Be Used as An Effective Nutritional Supplement to Enhance the Effects of Resistance Training in Rugby Union Players?" Nutrients 13, no. 10: 3367. https://doi.org/10.3390/nu13103367
APA StyleTamilio, R. A., Clarke, N. D., Duncan, M. J., Morris, R., Grgic, J., & Tallis, J. (2021). Can 3 mg·kg−1 of Caffeine Be Used as An Effective Nutritional Supplement to Enhance the Effects of Resistance Training in Rugby Union Players? Nutrients, 13(10), 3367. https://doi.org/10.3390/nu13103367