Importance of Self-Efficacy in Eating Behavior and Physical Activity Change of Overweight and Non-Overweight Adolescent Girls Participating in Healthy Me: A Lifestyle Intervention with Mobile Technology




Abstract
1. Introduction
2. Materials and Methods
2.1. Study and Intervention Design
2.2. Evaluation Surveys
- Study 1—at the beginning of the program implementation (November 2017).
- Study 2—after the intervention completion (June 2018).
- Study 3—three months after the intervention completion (September 2018).
2.3. Sample Characteristics
2.4. Measures
2.4.1. Health Behavior Indicators
- 1.
- Eating behaviors
- Frequency of eating fruits, vegetables, sweets, drinking soft drinks with added sugar. Girls answered how often they eat or drink the products by choosing one answer from seven categories, from “never” to “daily, more than once”.
- Breakfast consumption. Girls were asked to answer the questions on the frequency of eating breakfast on schooldays, choosing from six answer categories, from “never” to “five days a week”, and during the weekends, choosing from three options, from “never” to “both days”.
- 2.
- Physical activity
- Moderate-to-vigorous physical activity. Girls answered the question: “Over the past seven days, on how many days were you physically active for a total of at least 60 min per day? Please add up all the time you spent in physical activity each day”. The questions had eight response categories: from “zero days” to “seven days”.
2.4.2. HBI
- Fruit and vegetables: 0 points—never or less than once a week; 1 point—“once a week”; 2 points—“two to six days a week”; 3 points—“daily, at least once or daily more than once”.
- Sweets and soft drinks consumption: 0 points—“daily, at least once or daily more than once”; 1 point—“two to six days a week”; 2 points—“once a week”; 3 points—“never or less than once a week”.
- Breakfast consumption on schooldays: 0 points—“never”; 1 point—“one to two days”; 2 points—“three to four days”; 3 points—“daily”.
- Breakfast consumption on weekends: 0 points—“never”; 1 point—“one day”; 3 points—“both days”.
- Moderate-to-vigorous physical activity: 0 points—“zero days”; 1 point—“one to three days”; 2 points—“four to six days”; 3 points—“seven days”.
2.4.3. Self-Efficacy—Personal Competence Scale
2.4.4. Body Weight Status
2.5. Statistical Analysis
3. Results
3.1. HBI
3.2. Self-Efficacy—Personal Competence
3.3. School Effect
3.4. Independent Predictors of the Change in HBI
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dick, B.; Ferguson, B.J. Health for the World’s Adolescents: A Second Chance in the Second Decade. J. Adolesc. Health 2015, 56, 3–6. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sixty-Fourth World Health Assembly. Resolution WHA 64.28: Youth and Health Risks; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Sawyer, S.M.; A Afifi, R.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Salam, R.A.; Das, J.K.; Ahmed, W.; Irfan, O.; Sheikh, S.S.; Bhutta, Z.A. Effects of Preventive Nutrition Interventions among Adolescents on Health and Nutritional Status in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Nutrients 2019, 12, 49. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Már Arnarsson, Á. (Eds.) Spotlight on Adolescent Health and Well-Being. - Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Mazur, J.; Małkowska-Szkutnik, A. (Eds.) Zdrowie Uczniów w 2018 Roku na Tle Nowego Modelu Badań HBSC; Instytut Matki i Dziecka: Warsaw, Poland, 2018. [Google Scholar]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 7, CD001871. [Google Scholar] [CrossRef]
- Blüher, S.; Kromeyer-Hauschild, K.; Graf, C.; Widhalm, K.; Korsten-Reck, U.; Jödicke, B.; Markert, J.; Müller, M.J.; Moss, A.; Wabitsch, M.; et al. Current Guidelines for Obesity Prevention in Childhood and Adolescence. Obes. Facts 2018, 11, 263–276. [Google Scholar] [CrossRef]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, CD001871. [Google Scholar] [CrossRef]
- Mazur, J.; Kowalewska, A.; Baska, T.; Sigmund, E.; Nałęcz, H.; Nemeth, A.; Zawadzka, D. Patterns of physical activity and multiple risk behaviour in adolescents from Visegrad countries. Zdr. Publiczne Zarządz. 2014, 12, 56–67. [Google Scholar] [CrossRef]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef]
- Brown, T.; Summerbell, C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: An update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes. Rev. 2009, 10, 110–141. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenberghe, E.; Maes, L.; Spittaels, H.; Van Lenthe, F.J.; Brug, J.; Oppert, J.-M.; De Bourdeaudhuij, I. Effectiveness of school-based interventions in Europe to promote healthy nutrition in children and adolescents: Systematic review of published and ‘grey’ literature. Br. J. Nutr. 2010, 103, 781–797. [Google Scholar] [CrossRef] [PubMed]
- Safron, M.; Cislak, A.; Sacchi, M.G.D.M.D.; Luszczynska, A. Effects of School-based Interventions Targeting Obesity-Related Behaviors and Body Weight Change: A Systematic Umbrella Review. Behav. Med. 2011, 37, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Hynynen, S.-T.; Van Stralen, M.M.; Sniehotta, F.F.; Araujo-Soares, V.; Hardeman, W.; Chinapaw, M.J.; Vasankari, T.; Hankonen, N. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int. Rev. Sport Exerc. Psychol. 2015, 9, 22–44. [Google Scholar] [CrossRef] [PubMed]
- Hendrie, G.A.; Brindal, E.; Corsini, N.; Gardner, C.; Baird, D.L.; Golley, R.K. Combined Home and School Obesity Prevention Interventions for Children. Health Edu. Behav. 2011, 39, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.; Curry, W.; Kerner, C.; Newson, L.; Fairclough, S.J. The effectiveness of school-based physical activity interventions for adolescent girls: A systematic review and meta-analysis. Prev. Med. 2017, 105, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Avery, L.; Flynn, D.; Van Wersch, A.; Sniehotta, F.F.; Trenell, M.I. Changing Physical Activity Behavior in Type 2 Diabetes: A systematic review and meta-analysis of behavioral interventions. Diabetes Care 2012, 35, 2681–2689. [Google Scholar] [CrossRef]
- Martyn-Nemeth, P.; Penckofer, S.; Gulanick, M.; Velsor-Friedrich, B.; Bryant, F.B. The relationships among self-esteem, stress, coping, eating behavior, and depressive mood in adolescents. Res. Nurs. Health 2009, 32, 96–109. [Google Scholar] [CrossRef]
- Rose, T.; Barker, M.; Jacob, C.M.; Morrison, L.; Lawrence, W.; Strömmer, S.; Vogel, C.; Woods-Townsend, K.; Farrell, D.; Inskip, H.; et al. A Systematic Review of Digital Interventions for Improving the Diet and Physical Activity Behaviors of Adolescents. J. Adolesc. Health 2017, 61, 669–677. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Marques, M.M. Health Behavior Change for Obesity Management. Obes. Facts 2017, 10, 666–673. [Google Scholar] [CrossRef]
- Bandura, A.; Freeman, W.H.; Lightsey, R. Self-Efficacy: The Exercise of Control. J. Cogn. Psychother. 1999, 13, 158–166. [Google Scholar] [CrossRef]
- Mokhtari, S.; Grace, B.; Pak, Y.; Reina, A.; Durand, Q.; Yee, J.K. Motivation and perceived competence for healthy eating and exercise among overweight/obese adolescents in comparison to normal weight adolescents. BMC Obes. 2017, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Mazur, J.; Dzielska, A.; Kleszczewska, D.; Oblacińska, A.; Fijałkowska, A. Changes in physical activity of adolescent girls in the context of their perception of the Healthy Me programme. Eur. J. Public Health 2020, 30, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Moores, C.; Bell, L.K.; Miller, J.; A Damarell, R.; Matwiejczyk, L.; Miller, M.D. A systematic review of community-based interventions for the treatment of adolescents with overweight and obesity. Obes. Rev. 2018, 19, 698–715. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Jeon, S.; Grey, M. An Internet Obesity Prevention Program for Adolescents. J. Adolesc. Health 2013, 52, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- De Onis, M.; Lobstein, T. Defining obesity risk status in the general childhood population: Which cut-offs should we use? Pediatr. Obes. 2010, 5, 458–460. [Google Scholar] [CrossRef]
- Jarosz, M.; Respondek, W.; Wolnicka, K.; Sajór, I.; Wierzejska, R. Zalecenia dotyczące żywienia i aktywności fizycznej. In Normy Dla Populacji Polskiej—Nowelizacja; Jarosz, M., Ed.; Instytut żywności i Żywienia: Warsaw, Poland, 2012; pp. 158–163. [Google Scholar]
- Global Recommendations on Physical Activity for Health. World Health Organization 2010. Available online: https://www.who.int/activities/developing-new-guidelines-on-physical-activity-and-sedentary-behaviour-for-youth-adults-and-sub-populations (accessed on 16 June 2020).
- Peterson, R. A Meta-Analysis of Cronbach’s Coefficient Alpha. J. Consum. Res. 1994, 21, 381–391. [Google Scholar] [CrossRef]
- Juczynski, Z. Narzędzia Pomiaru w Promocji i Psychologii Zdrowia, 2nd ed.; Pracownia Testów Psychologicznych PTP: Warsaw, Poland, 2012. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy Scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, S., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Goodman, N.; Coopersmith, S. The Antecedents of Self-Esteem. Am. Sociol. Rev. 1969, 34, 116. [Google Scholar] [CrossRef]
- Coopersmith, S. Revised Coopersmith Self-Esteem Inventory Manual; Mind Garden: Redwood City, CA, USA, 2002. [Google Scholar]
- Jodkowska, M.; Oblacińska, A.M.; Tabak, I.; Radiukiewicz, K. Differences in dietary patterns between overweight and normal-weight adolescents. Med. Wieku Rozw. 2011, 15, 266–273. [Google Scholar]
- Monzani, A.; Ricotti, R.; Caputo, M.; Caputo, M.; Archero, F.; Bellone, S.; Prodam, F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef]
- Zalewska, M.; Maciorkowska, E. Selected nutritional habits of teenagers associated with overweight and obesity. PeerJ 2017, 5, 3681. [Google Scholar] [CrossRef]
- Olds, T.S.; Ferrar, K.; Schranz, N.; Maher, C. Obese Adolescents Are Less Active Than Their Normal-Weight Peers, but Wherein Lies the Difference? J. Adolesc. Health 2011, 48, 189–195. [Google Scholar] [CrossRef]
- Bullen, B.A.; Reed, R.B.; Mayer, J. Physical Activity of Obese and Nonobese Adolescent Girls Appraised by Motion Picture Sampling. Am. J. Clin. Nutr. 1964, 14, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.; Marti, C.N. A meta-analytic review of obesity prevention programs for children and adolescents: The skinny on interventions that work. Psychol. Bull. 2006, 132, 667–691. [Google Scholar] [CrossRef]
- Issel, L.M. Health Program Planning and Evaluation. A Practical, Systematic Approach for Community Health; Jones & Bartlett Learning: Burlington, MA, USA, 2018. [Google Scholar]
- Inchley, J.; Currie, D.; Jewell, J.; Breda, J.; Barnekov, V. (Eds.) Adolescent Obesity and Related Behaviours: Trends and Inequalities in the WHO European Region, 2002–2014; Observations from the Health Behaviour in School-Aged Children (HBSC) WHO Collaborative cross-National Study; WHO: Copenhagen, Denmark, 2017. [Google Scholar]
- Nixon, C.A.; Moore, H.J.; Douthwaite, W.; Gibson, E.L.; Vögele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Summerbell, C. ToyBox-study group Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: A systematic review. Obes. Rev. 2012, 13, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.; Mazurek Melnyk, B. Psychosocial Correlates of Healthy Beliefs, Choices, and Behaviors in Overweight and Obese School-Age Children: A Primary Care Healthy Choices Intervention Pilot Study. J. Pediatr. Nurs. 2011, 26, 456–464. [Google Scholar] [CrossRef]
- Morano, M.; Rutigliano, I.; Rago, A.; Pettoello-Mantovani, M.; Campanozzi, A. A multicomponent, school-initiated obesity intervention to promote healthy lifestyles in children. Nutrients 2016, 32, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Kołoło, H.; Guszkowska, M.; Mazur, J.; Dzielska, A. Self-efficacy, self-esteem and body image as psychological determinants of 15-year-old adolescents’ physical activity levels. Hum. Mov. 2012, 13, 264–270. [Google Scholar] [CrossRef]
- Goffman, E. Stigma. Notes on the Management of Spoiled Identity; Penguin: London, UK, 1963. [Google Scholar]
- Nolan, L.; Eshleman, A. Paved with good intentions: Paradoxical eating responses to weight stigma. Appetite 2016, 102, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.; Cunningham, S.A. Social Competence and Obesity in Elementary School. Am. J. Public Health 2015, 105, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Jacobson, D.; Kelly, S.A.; O’Haver, J.; Small, L.; Mays, M.Z. Improving the Mental Health, Healthy Lifestyle Choices, and Physical Health of Hispanic Adolescents: A Randomized Controlled Pilot Study. J. Sch. Health 2009, 79, 575–584. [Google Scholar] [CrossRef]
- Vila, G. Mental Disorders in Obese Children and Adolescents. Psychosom. Med. 2004, 66, 387–394. [Google Scholar] [CrossRef]
- Racey, M.; O’Brien, C.; Douglas, S.; Marquez, O.; A Hendrie, G.; Newton, G. Systematic Review of School-Based Interventions to Modify Dietary Behavior: Does Intervention Intensity Impact Effectiveness? J. Sch. Health 2016, 86, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Stewart, D.E. The implementation and effectiveness of school-based nutrition promotion programmes using a health-promoting schools approach: A systematic review. Public Health Nutr. 2012, 16, 1082–1100. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Xu, H.-M.; Wen, L.-M.; Peng, Y.-Z.; Lin, L.-Z.; Zhou, S.; Li, W.-H.; Wang, H. A systematic review and meta-analysis of the overall effects of school-based obesity prevention interventions and effect differences by intervention components. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 95. [Google Scholar] [CrossRef]
- Cassar, S.; Salmon, J.; Timperio, A.; Naylor, P.-J.; Van Nassau, F.; Ayala, A.M.C.; Koorts, H. Adoption, implementation and sustainability of school-based physical activity and sedentary behaviour interventions in real-world settings: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.M. Optimization of Behavioral, Biobehavioral, and Biomedical Interventions. In Statistics for Social and Behavioral Sciences; Springer Science and Business Media LLC: Berlin, Germany, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
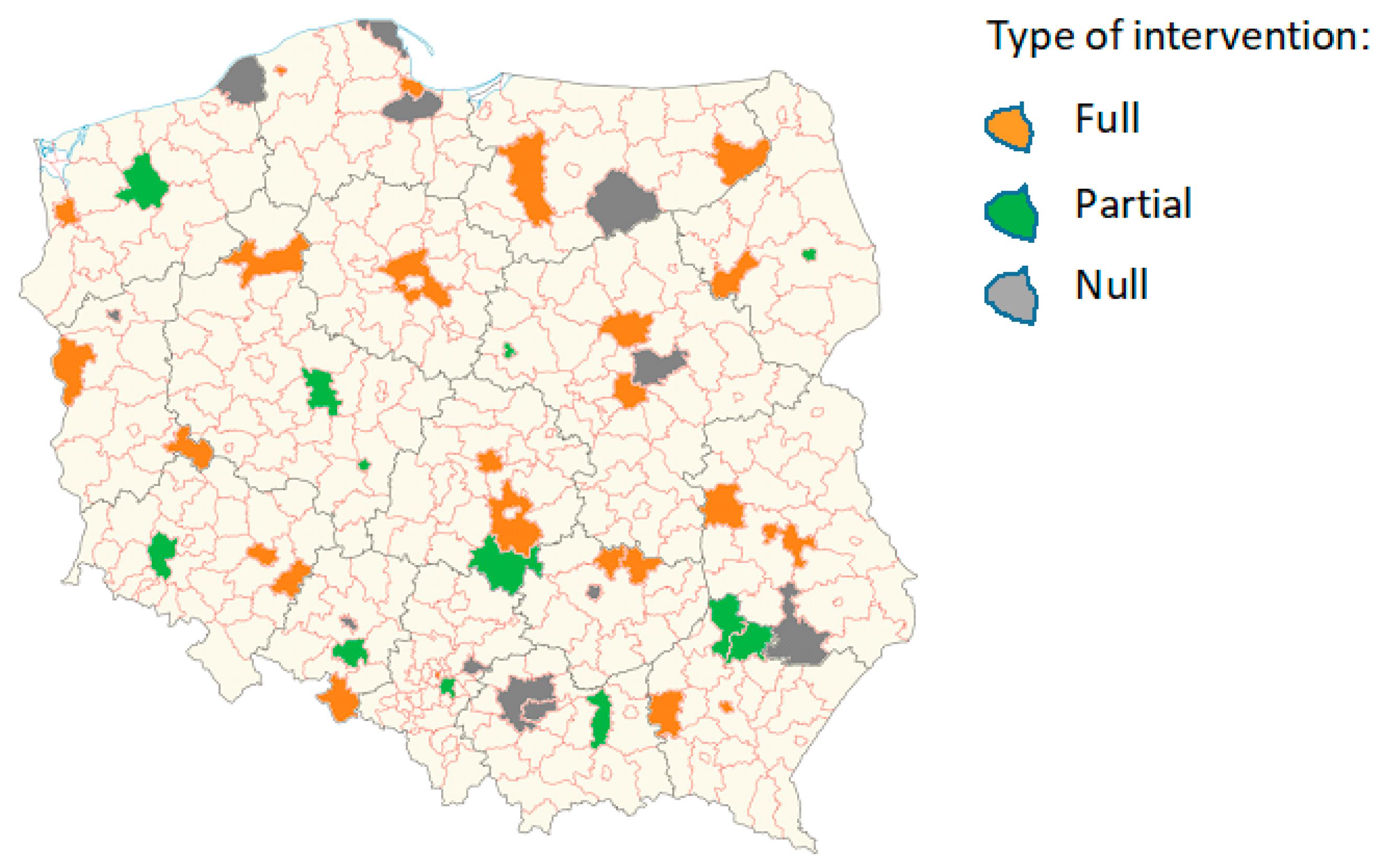
| Intervention Type | |||
|---|---|---|---|
| COMPONENTS | Full | Partial | Null |
| FITNESS BAND | |||
| Objective measurement (steps, heart rate, sleep quality) | X | X | X |
| MOBILE APP | |||
| Feedback from physical activity telemonitoring (steps, heart rate, distance, sleep quality) | X | X | X |
| Short messages (facts about a healthy lifestyle) | X | X | |
| Articles about a healthy lifestyle | X | ||
| Gamification (challenges related to physical activity, nutrition, personal and social competences—individual and group, to be performed alone or in cooperation with family and friends) | X | ||
| OTHER | |||
| Workshops at school run by the project coordinator (health education) | X | ||
| Promotion of the intervention theme (physical activity, eating behavior, risk behaviors, personal and social competences) at school and in the local environment—involvement of young people (e.g., preparation by girls of a poster promoting the program and the theme of intervention) | X | X | X |
| Promotional campaign via Facebook (closed group, competition) | X | X | X |
| Total | Non-Overweight | Overweight | |
|---|---|---|---|
| N 1 | n (%) | n (%) | |
| Total | 1111 | 843(76.5) | 259(23.5) |
| Type of intervention | n (%) | n (%) | n (%) |
| Full | 597(53.7) | 451(76.1) | 142(23.9) |
| Partial | 252(22.7) | 190(76.3) | 59(23.7) |
| Null | 262(23.6) | 202(77.7) | 58(22.3) |
| M ± SD | M ± SD | M ± SD | |
| HBI 2 | 13.69 ± 3.23 | 13.65 ± 3.19 | 13.81 ± 3.35 |
| GSE 3 | 34.69 ± 5.33 | 34.78 ± 5.40 | 34.37 ± 5.10 |
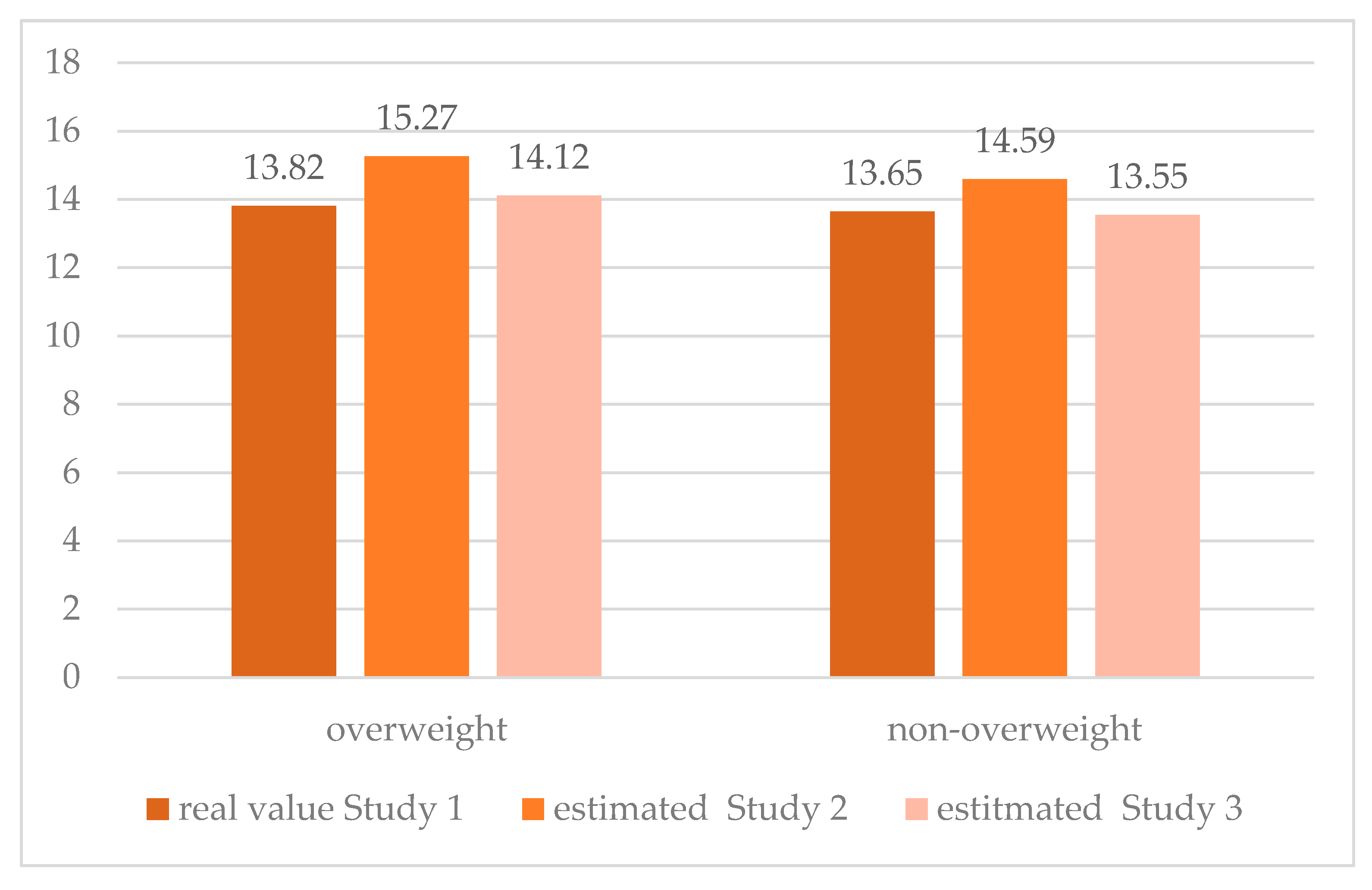
| Total | Overweight | Non-Overweight | p 2 | |
|---|---|---|---|---|
| M ± S | M ± SD | M ± SD | ||
| Study 1 | 13.71 ± 3.30 | 13.81 ± 3.35 | 13.65 ± 3.19 | 0.405 |
| Study 2 | 14.73 ± 4.11 | 15.12 ± 4.23 | 14.61 ± 4.07 | 0.052 |
| Study 3 | 13.69 ± 3.23 | 14.16 ± 3.27 | 13.56 ± 3.29 | 0.008 |
| p 1 | <0.001 | <0.001 | <0.001 |
| Self-Efficacy | Total | Overweight | Non-Overweight | p 3 |
|---|---|---|---|---|
| General self-efficacy (GSE) 1 | ||||
| Study 1 | 34.68 ± 5.33 | 34.36 ± 5.10 | 34.78 ± 5.40 | 0.206 |
| Study 3 | 34.33 ± 5.13 | 33.99 ± 5.04 | 34.43 ± 5.16 | 0.228 |
| p 2 | 0.027 | 0.677 | 0.030 | |
| Domain of strength | ||||
| Study 1 | 17.38 ± 3.17 | 17.30 ± 3.07 | 17.42 ± 3.21 | 0.451 |
| Study 3 | 17.16 ± 3.20 | 17.05 ± 3.30 | 17.19 ± 3.18 | 0.696 |
| p 2 | 0.023 | 0.328 | 0.043 | |
| Domain of perseverance | ||||
| Study 1 | 17.28 ± 3.33 | 17.06 ± 3.32 | 17.34 ± 3.33 | 0.227 |
| Study 3 | 17.16 ± 3.13 | 17.02 ± 3.05 | 17.20 ± 3.15 | 0.608 |
| p 2 | 0.191 | 0.831 | 0.165 |
| Predictors | Dependent Variable | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HBI Change Study 1–Study 2 | HBI Change Study 2–Study 3 | HBI Change Study 1–Study 3 | |||||||
| Beta | SE | p | Beta | SE | p | Beta | SE | P | |
| Constant | 3.394 | 0.653 | 0.000 | −1.332 | 0.908 | 0.142 | 4.738 | 0.899 | 0.000 |
| Main effect: | |||||||||
| Body weight status | |||||||||
| Overweight | 0.412 | 0.193 | 0.033 | −0.113 | 0.269 | 0.674 | 0.539 | 0.266 | 0.043 |
| Non-overweight | Reference category | ||||||||
| Type of intervention | |||||||||
| Full | −0.007 | 0.203 | 0.971 | 0.335 | 0.282 | 0.235 | −0.357 | 0.280 | 0.201 |
| Partial | −0.425 | 0.241 | 0.078 | 0.393 | 0.336 | 0.242 | −0.833 | 0.332 | 0.012 |
| Null (control) | Reference category | ||||||||
| Initial HBI 1 | −0.397 | 0.027 | 0.000 | −0.018 | 0.037 | 0.618 | −0.380 | 0.037 | 0.000 |
| Initial GSE 2 | 0.062 | 0.019 | 0.001 | 0.009 | 0.026 | 0.725 | 0.054 | 0.026 | 0.040 |
| Interaction: | |||||||||
| Overweight with GSE | 0.134 | 0.034 | 0.000 | 0.000 | 0.048 | 0.992 | 0.132 | 0.048 | 0.006 |
| Non-overweight with GSE | 0.096 | 0.021 | 0.000 | 0.060 | 0.029 | 0.038 | 0.037 | 0.029 | 0.198 |
| Scale | 6.393 | 0.291 | 12.352 | 0.562 | 12.106 | 0.551 | |||
| Omnibus test—p | 0.000 | 0.455 | 0.000 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dzielska, A.; Mazur, J.; Nałęcz, H.; Oblacińska, A.; Fijałkowska, A. Importance of Self-Efficacy in Eating Behavior and Physical Activity Change of Overweight and Non-Overweight Adolescent Girls Participating in Healthy Me: A Lifestyle Intervention with Mobile Technology. Nutrients 2020, 12, 2128. https://doi.org/10.3390/nu12072128
Dzielska A, Mazur J, Nałęcz H, Oblacińska A, Fijałkowska A. Importance of Self-Efficacy in Eating Behavior and Physical Activity Change of Overweight and Non-Overweight Adolescent Girls Participating in Healthy Me: A Lifestyle Intervention with Mobile Technology. Nutrients. 2020; 12(7):2128. https://doi.org/10.3390/nu12072128
Chicago/Turabian StyleDzielska, Anna, Joanna Mazur, Hanna Nałęcz, Anna Oblacińska, and Anna Fijałkowska. 2020. "Importance of Self-Efficacy in Eating Behavior and Physical Activity Change of Overweight and Non-Overweight Adolescent Girls Participating in Healthy Me: A Lifestyle Intervention with Mobile Technology" Nutrients 12, no. 7: 2128. https://doi.org/10.3390/nu12072128
APA StyleDzielska, A., Mazur, J., Nałęcz, H., Oblacińska, A., & Fijałkowska, A. (2020). Importance of Self-Efficacy in Eating Behavior and Physical Activity Change of Overweight and Non-Overweight Adolescent Girls Participating in Healthy Me: A Lifestyle Intervention with Mobile Technology. Nutrients, 12(7), 2128. https://doi.org/10.3390/nu12072128