Effects of Intermittent Fasting on Specific Exercise Performance Outcomes: A Systematic Review Including Meta-Analysis


 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Screening and Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
2.6. Data Analysis
3. Results
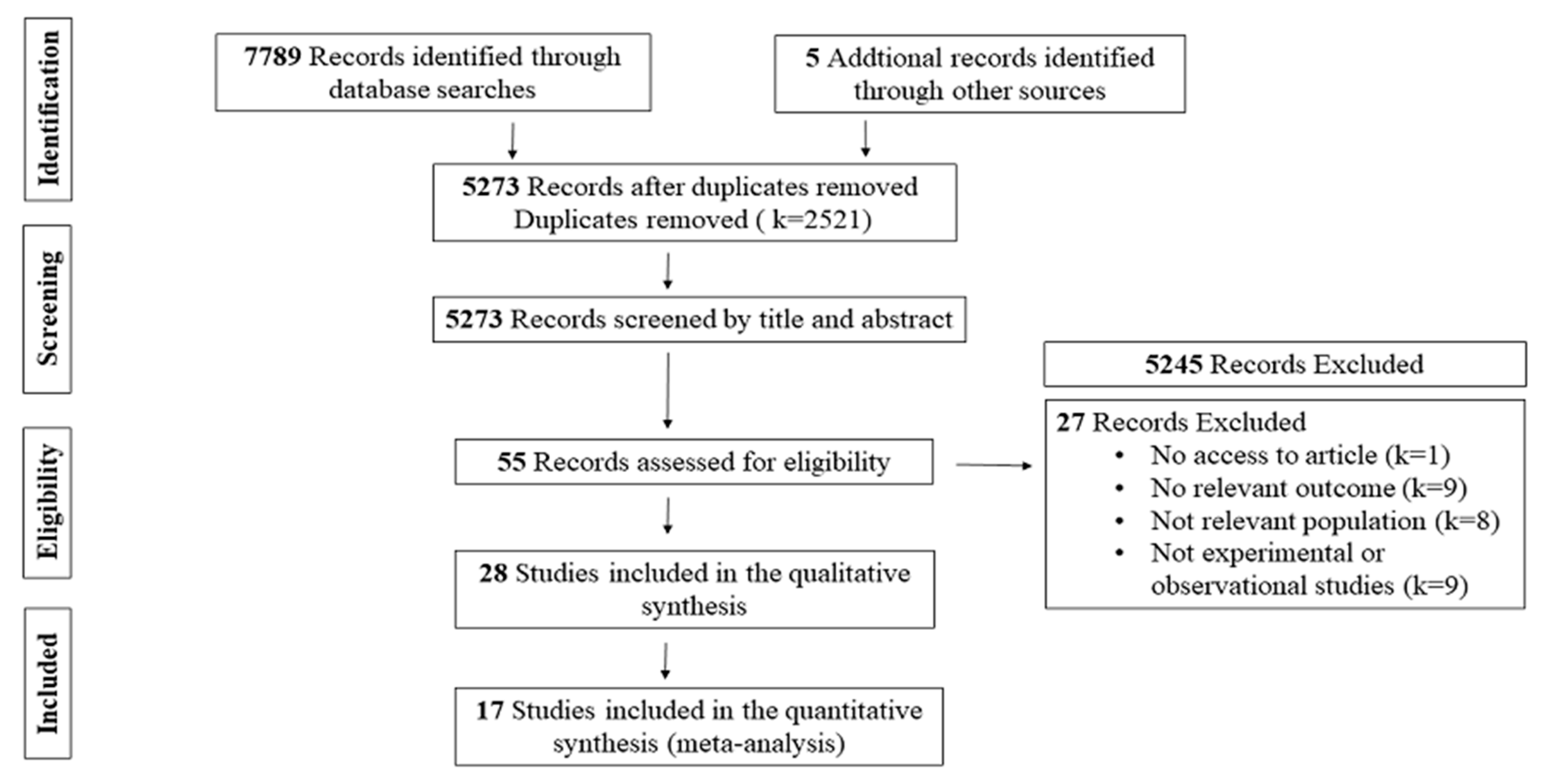
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Effects of Intermittent Fasting on Specific Outcomes
3.4.1. Primary Outcomes
Changes in Muscle Strength
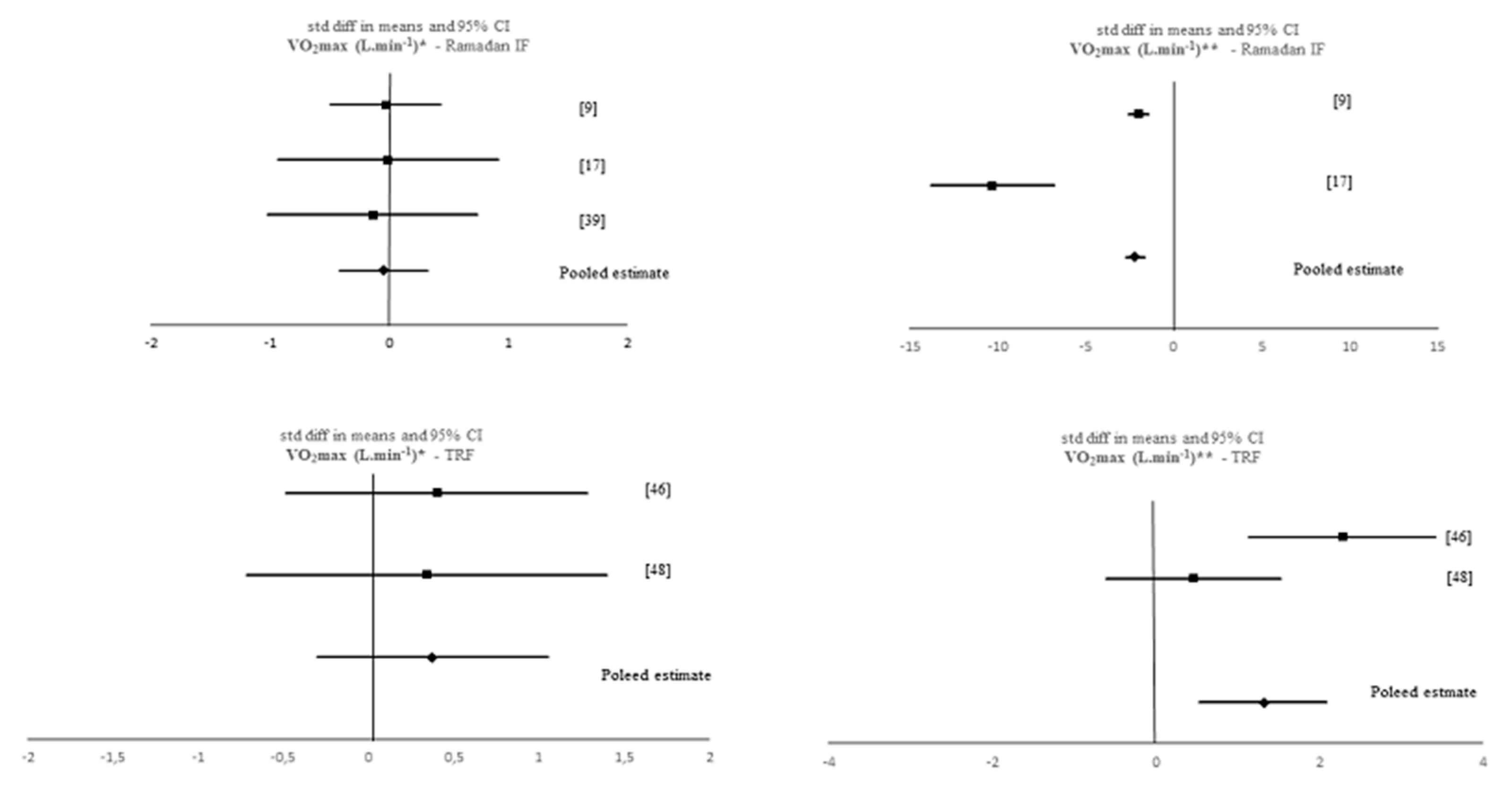
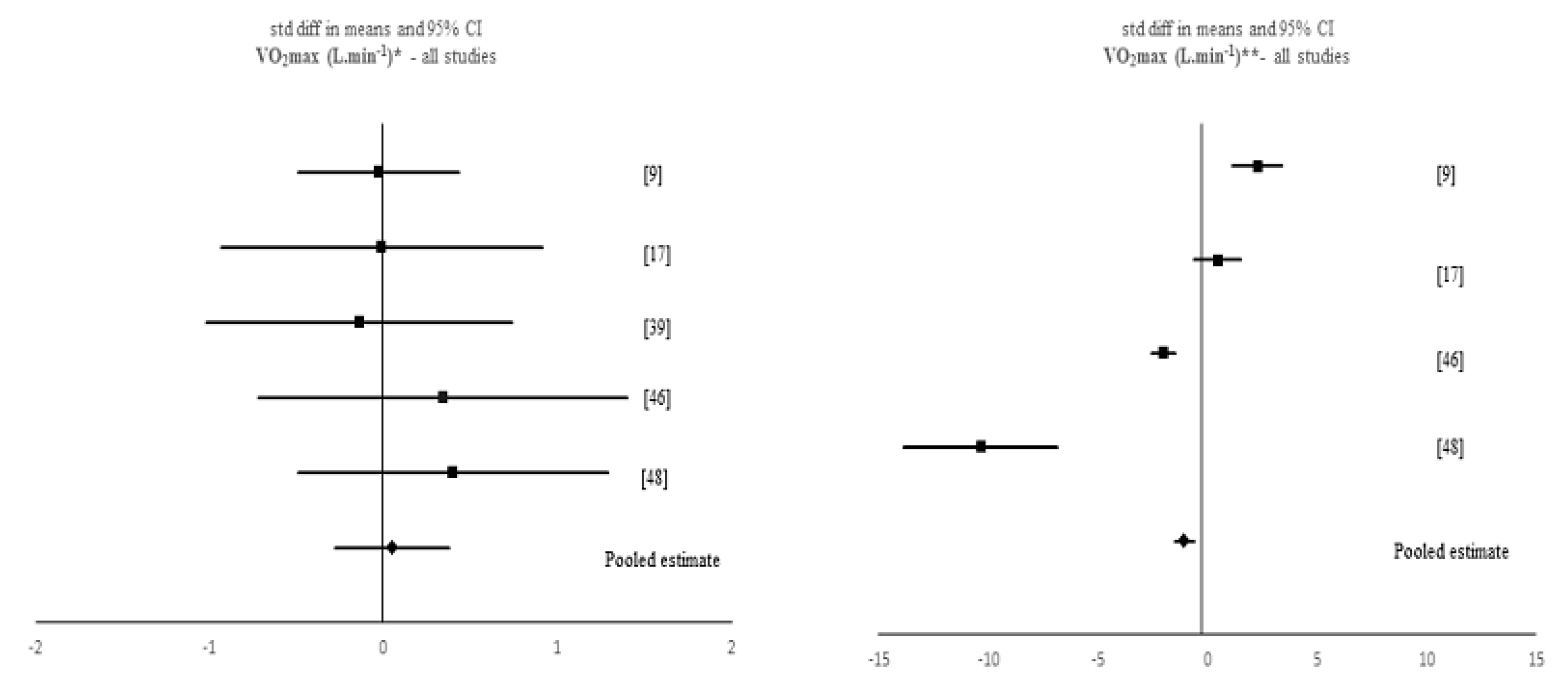
Changes in Aerobic Capacity
Changes in Anaerobic Capacity
3.4.2. Secondary Outcome
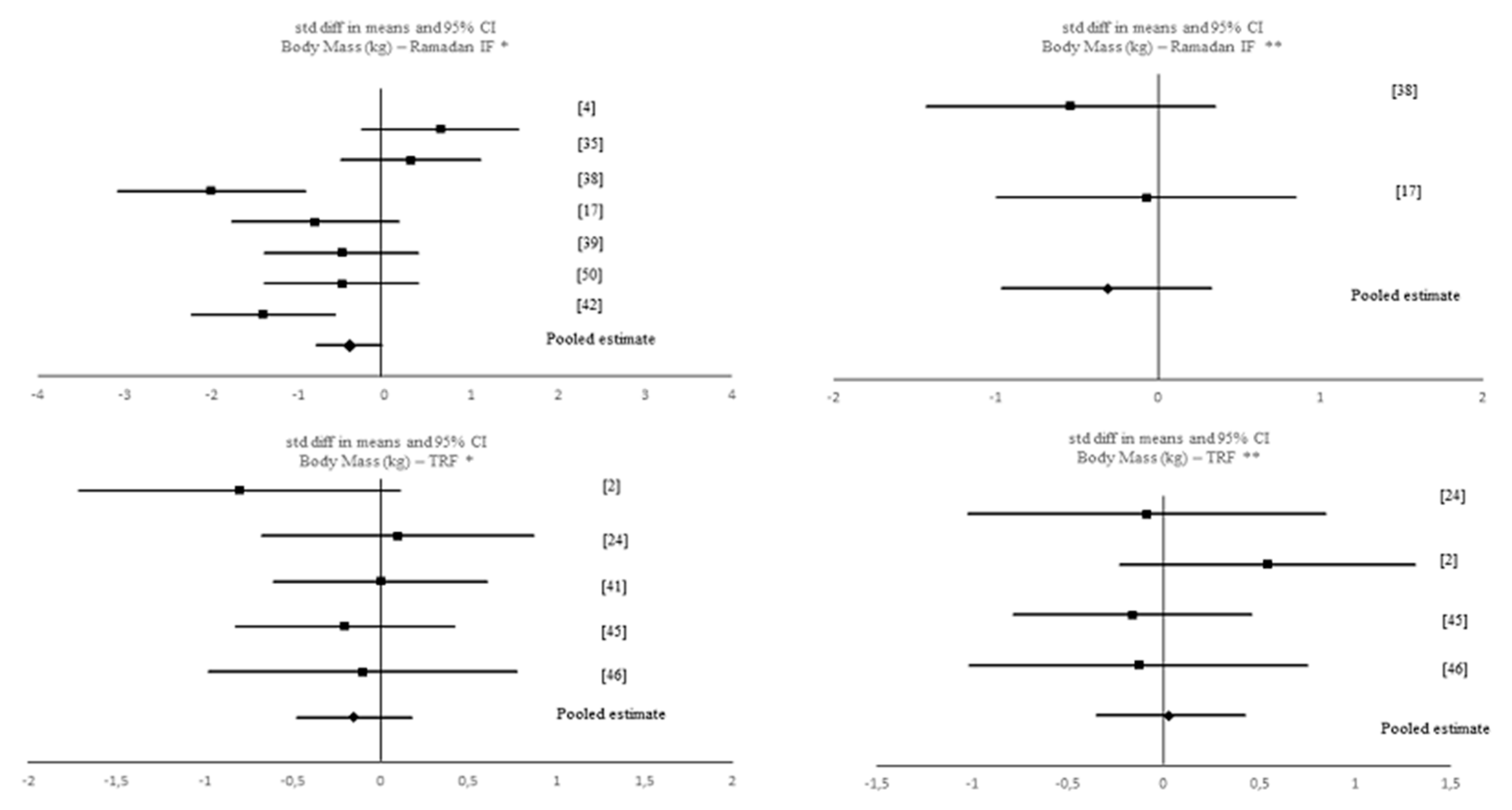
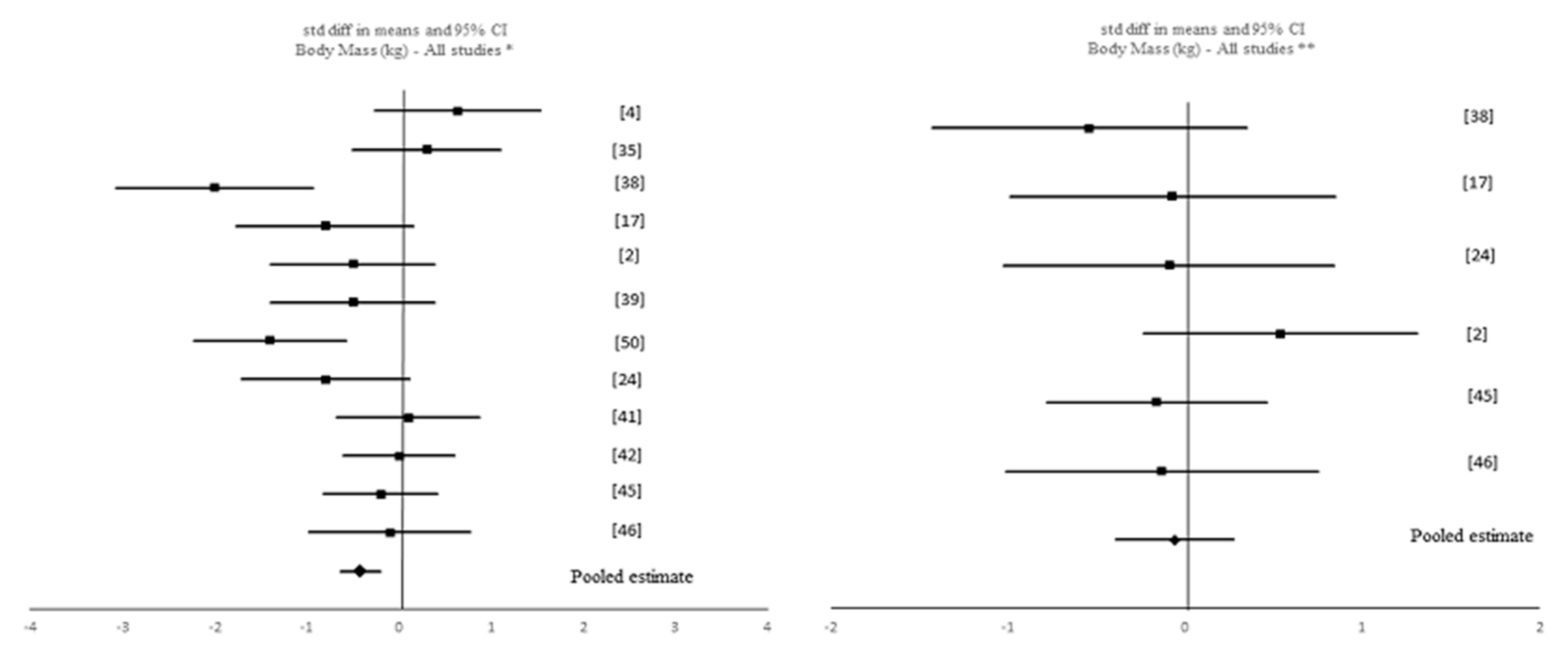
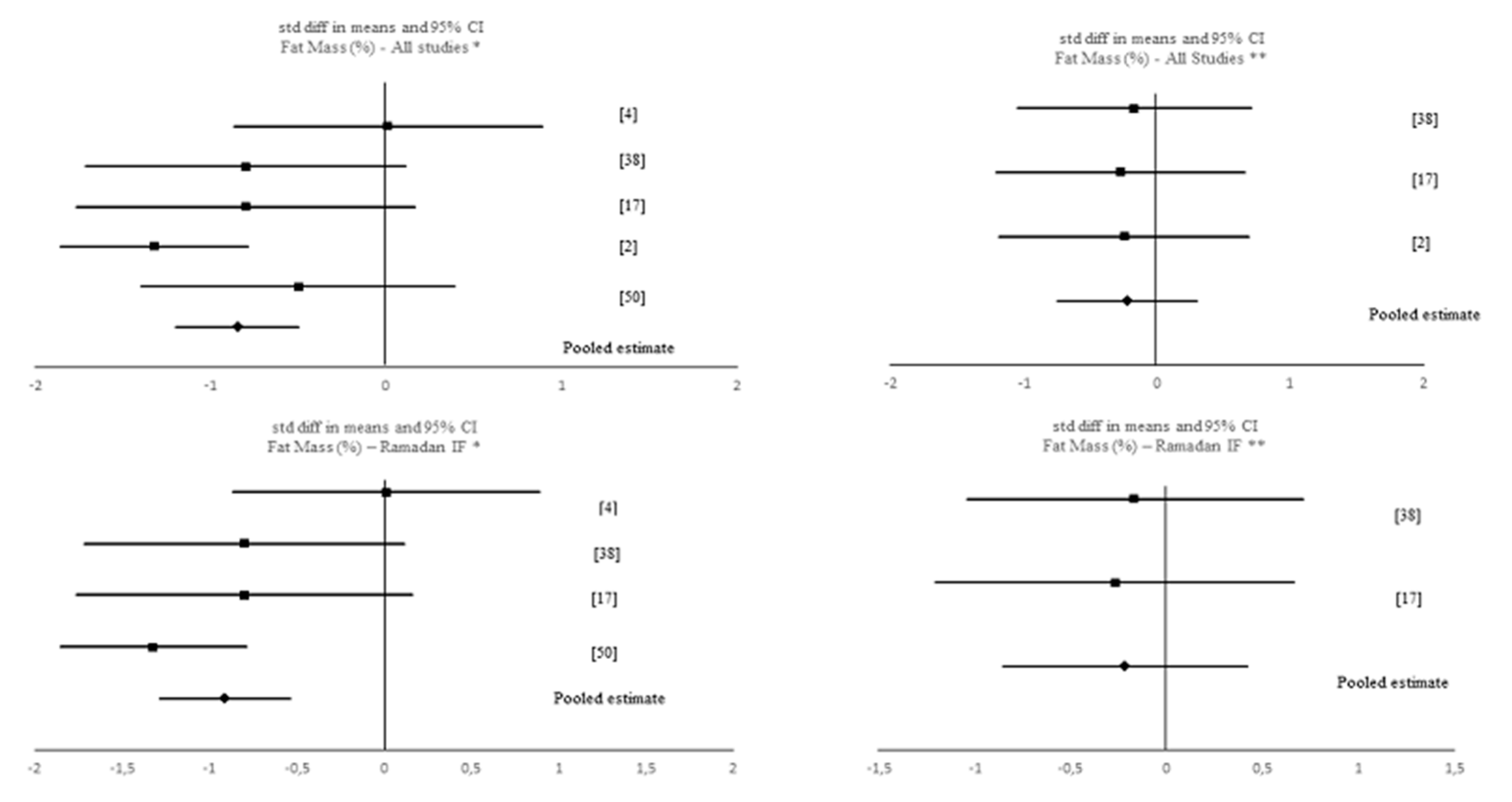
Changes in Body Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IF | Intermittent fasting |
| Ramadan IF | Ramadan intermittent fasting |
| TRF | Time-restricted feeding |
| SMD | Standardized mean difference |
| VO2max | Maximum oxygen uptake |
| CR | Caloric restriction |
| PRISMA | Preferred reporting items for systematic reviews and meta-analysis |
| EPHPP | Effective public health practice project |
| CMA | Comprehensive meta-analysis |
| CI | Confidence interval |
References
- Horne, B.D.; Muhlestein, J.B.; Anderson, J.L. Health effects of intermittent fasting: Hormesis or harm? A systematic review. Am. J. Clin. Nutr. 2015, 102, 464–470. [Google Scholar] [CrossRef]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G., 3rd; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity (Silver Spring) 2018, 26, 254–268. [Google Scholar] [CrossRef]
- Karli, U.; Guvenc, A.; Aslan, A.; Hazir, T.; Acikada, C. Influence of Ramadan Fasting on Anaerobic Performance and Recovery Following Short time High Intensity Exercise. J. Sports Sci. Med. 2007, 6, 490–497. [Google Scholar]
- Chaouachi, A.; Coutts, A.J.; Chamari, K.; Wong, D.P.; Chaouachi, M.; Chtara, M.; Roky, R.; Amri, M. Effect of Ramadan intermittent fasting on aerobic and anaerobic performance and perception of fatigue in male elite judo athletes. J. Strength Cond. Res. 2009, 23, 2702–2709. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q.F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J. Transl. Med. 2016, 14, 290. [Google Scholar] [CrossRef]
- Tinsley, G.M.; Gann, J.G.; La Bounty, P.M. Intermittent Fasting Programs and Their Effects on Body Composition: Implications for Weight-Restricted Sports. Strength Cond. J. 2015, 37, 60–71. [Google Scholar] [CrossRef]
- Anis, C.; Leiper, J.B.; Nizar, S.; Coutts, A.J.; Karim, C. Effects of Ramadan intermittent fasting on sports performance and training: A review. Int. J. Sports Physiol. Perform. 2009, 4, 419–434. [Google Scholar] [CrossRef]
- Roy, A.S.; Bandyopadhyay, A. Effect of Ramadan intermittent fasting on selective fitness profile parameters in young untrained Muslim men. BMJ Open Sport Exerc. Med. 2015, 1, e000020. [Google Scholar] [CrossRef]
- Aziz, A.R.; Wahid, M.F.; Png, W.; Jesuvadian, C.V. Effects of Ramadan fasting on 60 min of endurance running performance in moderately trained men. Br. J. Sports Med. 2010, 44, 516–521. [Google Scholar] [CrossRef]
- Gueldich, H.; Zghal, F.; Borji, R.; Chtourou, H.; Sahli, S.; Rebai, H. The effects of Ramadan intermittent fasting on the underlying mechanisms of force production capacity during maximal isometric voluntary contraction. Chronobiol. Int. 2019, 36, 698–708. [Google Scholar] [CrossRef]
- Ferguson, L.M.; Rossi, K.A.; Ward, E.; Jadwin, E.; Miller, T.A.; Miller, W.C. Effects of caloric restriction and overnight fasting on cycling endurance performance. J. Strength Cond. Res. 2009, 23, 560–570. [Google Scholar] [CrossRef]
- Ramadan, J. Does fasting during Ramadan alter body composition, blood constituents and physical performance? Med Princ. Pract. 2002, 11 (Suppl. 2), 41–46. [Google Scholar] [CrossRef]
- Chaouachi, A.; Leiper, J.B.; Chtourou, H.; Aziz, A.R.; Chamari, K. The effects of Ramadan intermittent fasting on athletic performance: Recommendations for the maintenance of physical fitness. J. Sports Sci. 2012, 30 (Suppl. 1), S53–S73. [Google Scholar] [CrossRef]
- McMurray, R.G.; Ben-Ezra, V.; Forsythe, W.A.; Smith, A.T. Responses of endurance-trained subjects to caloric deficits induced by diet or exercise. Med. Sci. Sports Exerc. 1985, 17, 574–579. [Google Scholar] [CrossRef]
- Shephard, R.J. The Impact of Ramadan Observance upon Athletic Performance. Nutrients 2012, 4, 491–505. [Google Scholar] [CrossRef]
- Brisswalter, J.; Bouhlel, E.; Falola, J.M.; Abbiss, C.R.; Vallier, J.M.; Hausswirth, C. Effects of Ramadan intermittent fasting on middle-distance running performance in well-trained runners. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2011, 21, 422–427. [Google Scholar] [CrossRef]
- Sweileh, N.; Schnitzler, A.; Hunter, G.R.; Davis, B. Body composition and energy metabolism in resting and exercising muslims during Ramadan fast. J. Sports Med. Phys. Fit. 1992, 32, 156–163. [Google Scholar]
- Ramadan, J.M.; Barac-Nieto, M. Cardio-respiratory responses to moderately heavy aerobic exercise during the Ramadan fasts. Saudi Med. J. 2000, 21, 238–244. [Google Scholar]
- Gueye, L.; Samb, A.; Seck, D.; Cissé, F.; Camara, K.; Martineaud, J. Influence of a 12 hours-fast on maximal exercise. Scr. Med. 2004, 77, 5–8. [Google Scholar]
- Racinais, S.; Periard, J.D.; Li, C.K.; Grantham, J. Activity patterns, body composition and muscle function during Ramadan in a Middle-East Muslim country. Int. J. Sports Med. 2012, 33, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Templeman, I.; Thompson, D.; Gonzalez, J.; Walhin, J.P.; Reeves, S.; Rogers, P.J.; Brunstrom, J.M.; Karagounis, L.G.; Tsintzas, K.; Betts, J.A. Intermittent fasting, energy balance and associated health outcomes in adults: Study protocol for a randomised controlled trial. Trials 2018, 19, 86. [Google Scholar] [CrossRef]
- Schoenfeld, B. Does cardio after an overnight fast maximize fat loss? Strength Cond. J. 2011, 33, 23–25. [Google Scholar] [CrossRef]
- Tinsley, G.M.; Moore, M.L.; Graybeal, A.J.; Paoli, A.; Kim, Y.; Gonzales, J.U.; Harry, J.R.; VanDusseldorp, T.A.; Kennedy, D.N.; Cruz, M.R. Time-restricted feeding plus resistance training in active females: A randomized trial. Am. J. Clin. Nutr. 2019, 110, 628–640. [Google Scholar] [CrossRef] [PubMed]
- Halberg, N.; Henriksen, M.; Soderhamn, N.; Stallknecht, B.; Ploug, T.; Schjerling, P.; Dela, F. Effect of intermittent fasting and refeeding on insulin action in healthy men. J. Appl. Physiol. 2005, 99, 2128–2136. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis, version 3; Biostat: Englewood, NJ, USA, 2013. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Meta-Analysis Methods Based on Direction and P-Values. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009. [Google Scholar]
- Sedgwick, P.; Marston, L. Meta-analyses: Standardised mean differences. BMJ 2013, 347, f7257. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Cochran, W.G. The Combination of Estimates from Different Experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, J.; Telahoun, G.; Al-Zaid, N.S.; Barac-Nieto, M. Responses to exercise, fluid, and energy balances during Ramadan in sedentary and active males. Nutrition 1999, 15, 735–739. [Google Scholar] [CrossRef]
- Souissi, N.; Souissi, H.; Sahli, S.; Tabka, Z.; Dogui, M.; Ati, J.; Davenne, D. Effect of Ramadan on the diurnal variation in short-term high power output. Chronobiol. Int. 2007, 24, 991–1007. [Google Scholar] [CrossRef] [PubMed]
- Kirkendall, D.T.; Leiper, J.B.; Bartagi, Z.; Dvorak, J.; Zerguini, Y. The influence of Ramadan on physical performance measures in young Muslim footballers. J. Sports Sci. 2008, 26 (Suppl. 3), S15–S27. [Google Scholar] [CrossRef]
- Dannecker, E.A.; Liu, Y.; Rector, R.S.; Thomas, T.R.; Sayers, S.P.; Leeuwenburgh, C.; Ray, B.K. The effect of fasting on indicators of muscle damage. Exp. Gerontol. 2013, 48, 1101–1106. [Google Scholar] [CrossRef]
- Bouhlel, H.; Shepard, R.; Gmada, N.; Aouichaoui, C.; Peres, G.; Tabka, Z.; Bouhlel, E. Effect of Ramadan observance on maximal muscular performance of trained men. Clin. J. Sport Med. 2013, 23, 222–227. [Google Scholar] [CrossRef]
- Bouhlel, H.; Latiri, I.; Zarrouk, N.; Bigard, X.; Shepard, R.; Tabka, Z.; Bouhlel, E. Effet du jeûne du Ramadan et de l’exercice maximal sur le temps de réaction simple et de choix chez des sujets entraînés. Sci. Sports 2014, 29, 131–137. [Google Scholar] [CrossRef]
- Charlot, K.; Pichon, A.; Chapelot, D. Effets de l’entraînement à jeun sur la V˙ O2max, l’oxydation des lipides et la performance aérobie chez des jeunes hommes modérément entraînés. Sci. Sports 2016, 31, 166–171. [Google Scholar] [CrossRef]
- Cherif, A.; Meeusen, R.; Farooq, A.; Ryu, J.; Fenneni, M.A.; Nikolovski, Z.; Elshafie, S.; Chamari, K.; Roelands, B. Three Days of Intermittent Fasting: Repeated-Sprint Performance Decreased by Vertical-Stiffness Impairment. Int. J. Sports Physiol. Perform. 2017, 12, 287–294. [Google Scholar] [CrossRef]
- Aziz, A.R.; Che Muhamad, A.M.; Roslan, S.R.; Ghulam Mohamed, N.; Singh, R.; Chia, M.Y.H. Poorer Intermittent Sprints Performance in Ramadan-Fasted Muslim Footballers despite Controlling for Pre-Exercise Dietary Intake, Sleep and Training Load. Sports (Basel) 2017, 5. [Google Scholar] [CrossRef]
- Naharudin, M.N.B.; Yusof, A. The effect of 10 days of intermittent fasting on Wingate anaerobic power and prolonged high-intensity time-to-exhaustion cycling performance. Eur. J. Sport Sci. 2018, 18, 667–676. [Google Scholar] [CrossRef]
- Terada, T.; Toghi Eshghi, S.R.; Liubaoerjijin, Y.; Kennedy, M.; Myette-Cote, E.; Fletcher, K.; Boule, N.G. Overnight fasting compromises exercise intensity and volume during sprint interval training but improves high-intensity aerobic endurance. J. Sports Med. Phys. Fit. 2019, 59, 357–365. [Google Scholar] [CrossRef]
- Van Proeyen, K.; Szlufcik, K.; Nielens, H.; Ramaekers, M.; Hespel, P. Beneficial metabolic adaptations due to endurance exercise training in the fasted state. J. Appl. Physiol. 2010, 110, 236–245. [Google Scholar] [CrossRef]
- De Bock, K.; Derave, W.; Eijnde, B.O.; Hesselink, M.K.; Koninckx, E.; Rose, A.J.; Schrauwen, P.; Bonen, A.; Richter, E.A.; Hespel, P. Effect of training in the fasted state on metabolic responses during exercise with carbohydrate intake. J. Appl. Physiol. 2008, 104, 1045–1055. [Google Scholar] [CrossRef]
- Stocks, B.; Dent, J.R.; Ogden, H.B.; Zemp, M.; Philp, A. Postexercise skeletal muscle signaling responses to moderate- to high-intensity steady-state exercise in the fed or fasted state. Am. J. Physiol. Endocrinol. Metab. 2019, 316, E230–E238. [Google Scholar] [CrossRef]
- Stannard, S.R.; Buckley, A.J.; Edge, J.A.; Thompson, M.W. Adaptations to skeletal muscle with endurance exercise training in the acutely fed versus overnight-fasted state. J. Sci. Med. Sport 2010, 13, 465–469. [Google Scholar] [CrossRef]
- Cherif, A.; Meeusen, R.; Farooq, A.; Briki, W.; Fenneni, M.A.; Chamari, K.; Roelands, B. Repeated Sprints in Fasted State Impair Reaction Time Performance. J. Am. Coll. Nutr. 2017, 36, 210–217. [Google Scholar] [CrossRef]
- Kocaaga, T.; Tamer, K.; Karli, U.; Yarar, H. Effects of Ramadan Fasting on Physical Activity Level and Body Composition in Young Males. Int. J. Appl. Exerc. Phy. 2019, 8, 2322–3537. [Google Scholar]
- Aloui, A.; Driss, T.; Baklouti, H.; Jaafar, H.; Hammouda, O.; Chamari, K.; Souissi, N. Repeated-sprint training in the fasted state during Ramadan: Morning or evening training? J. Sports Med. Phys. Fit. 2018, 58, 990–997. [Google Scholar] [CrossRef]
- Png, W.; Bhaskaran, K.; Sinclair, A.J.; Aziz, A.R. Effects of ingesting low glycemic index carbohydrate food for the sahur meal on subjective, metabolic and physiological responses, and endurance performance in Ramadan fasted men. Int. J. Food Sci. Nutr. 2014, 65, 629–636. [Google Scholar] [CrossRef]
- Stote, K.S.; Baer, D.J.; Spears, K.; Paul, D.R.; Harris, G.K.; Rumpler, W.V.; Strycula, P.; Najjar, S.S.; Ferrucci, L.; Ingram, D.K. A controlled trial of reduced meal frequency without caloric restriction in healthy, normal-weight, middle-aged adults. Am. J. Clin. Nutr. 2007, 85, 981–988. [Google Scholar] [CrossRef]
- Zouhal, H.; Saeidi, A.; Salhi, A.; Li, H.; Essop, M.F.; Laher, I.; Rhibi, F.; Amani-Shalamzari, S.; Ben Abderrahman, A. Exercise Training and Fasting: Current Insights. Open Access J. Sports Med. 2020, 11, 1–28. [Google Scholar] [CrossRef]
- Güvenç, A. Effects of Ramadan fasting on body composition, aerobic performance and lactate, heart rate and perceptual responses in young soccer players. J. Hum. Kinet. 2011, 29, 79–91. [Google Scholar] [CrossRef]
- Bouhlel, E.; Denguezli, M.; Zaouali, M.; Tabka, Z.; Shephard, R.J. Ramadan fasting’s effect on plasma leptin, adiponectin concentrations, and body composition in trained young men. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 617–627. [Google Scholar] [CrossRef]
- Maughan, R.J.; Bartagi, Z.; Dvorak, J.; Zerguini, Y. Dietary intake and body composition of football players during the holy month of Ramadan. J. Sports Sci. 2008, 26 (Suppl. 3), S29–S38. [Google Scholar] [CrossRef]
- Ganesan, K.; Habboush, Y.; Sultan, S. Intermittent fasting: The choice for a healthier lifestyle. Cureus 2018, 10, e2947. [Google Scholar] [CrossRef]
- Harris, L.; Hamilton, S.; Azevedo, L.B.; Olajide, J.; De Brún, C.; Waller, G.; Whittaker, V.; Sharp, T.; Lean, M.; Hankey, C. Intermittent fasting interventions for treatment of overweight and obesity in adults: A systematic review and meta-analysis. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 507–547. [Google Scholar] [CrossRef]
- Mohsenzadeh, A.; Baghbani, M.M.; Ranjbar, R. The effect of endurance training accompanied by Ramadan fasting on lipid profiles and body composition in men. Jentashapir J. Health Res. 2013, 4, 287–295. [Google Scholar]
- Teo, W.; Newton, M.J.; McGuigan, M.R. Circadian rhythms in exercise performance: Implications for hormonal and muscular adaptation. J. Sports Sci. Med. 2011, 10, 600–606. [Google Scholar]
- Aziz, A.R.; Slater, G.J.; Chia, M.Y.H.; Teh, K.C. Effects of Ramadan fasting on training induced adaptations to a seven-week high-intensity interval exercise programme. Sci. Sports 2012, 27, 31–38. [Google Scholar] [CrossRef]
- Meckel, Y.; Ismaeel, A.; Eliakim, A. The effect of the Ramadan fast on physical performance and dietary habits in adolescent soccer players. Eur. J. Appl. Physiol. 2008, 102, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Rittig, N.; Bach, E.; Thomsen, H.H.; Møller, A.B.; Hansen, J.; Johannsen, M.; Jensen, E.; Serena, A.; Jørgensen, J.O.; Richelsen, B. Anabolic effects of leucine-rich whey protein, carbohydrate, and soy protein with and without β-hydroxy-β-methylbutyrate (HMB) during fasting-induced catabolism: A human randomized crossover trial. Clin. Nutr. 2017, 36, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Leiper, J.B.; Molla, A.M.; Molla, A.M. Effects on health of fluid restriction during fasting in Ramadan. Eur. J. Clin. Nutr. 2003, 57, S30–S38. [Google Scholar] [CrossRef] [PubMed]
- Zarrouk, N.; Hammouda, O.; Latiri, I.; Adala, H.; Bouhlel, E.; Rebai, H.; Dogui, M. Ramadan fasting does not adversely affect neuromuscular performances and reaction times in trained karate athletes. J. Int. Soc. Sports Nutr. 2016, 13, 18. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Parameters | Participants | Age | Trial Length & Intervention | Aerobic Changes | Anaerobic Changes | Strength Changes | Body Composition Changes (Secondary Outcome) |
|---|---|---|---|---|---|---|---|---|
| [34] | BC; VO2max; VE; VCO2; R; HR; Blood sample. | 6 physically active men (A). 7 sedentary men (S). | Group A, 35.5 ± 1.6 years Group S, 37.6 ± 2.3 years | 1 week before RF. 2 weeks after the start of RF. 4th week of RF. | ↓ HR (submax exercise) in S group during Ramadan. Significant ↓ of HR (submax exercise) in A group during Ramadan. | - | - | Total BM and FM ↓ non-significantly in both groups. |
| [4] | Anaerobic power; Anaerobic capacity; HR; BC; Blood lactate. | 10 male elite power athletes | 22.3 ± 1.3 years | 3 days before Ramadan (pre-RF). The last 3 days of Ramadan (end-RF). The last 3 d of the 4th week after the end of Ramadan (post-RF). | - | No adverse effects on anaerobic power and capacity. | - | No significant differences in body weight, BM index, FFM, % of body fat (↑ 0.2%). |
| [35] | Pmax; Pmean; Ppeak; BC. | 12 healthy males | 22.6 ± 1.3 years | 1 week before Ramadan. 2nd week of Ramadan. 4th week of Ramadan. 2 weeks after Ramadan. | - | Negative effect of Ramadan on anaerobic performance during the afternoon and evening. No effect on anaerobic performance in the morning. | - | No significant changes for body mass. |
| [36] | Speed; Power; Agility; Endurance; Passing and dribbling skills | 85 junior soccer players | 18.0 years | 3 weeks before Ramadan. 2nd week of Ramadan. 4th week of Ramadan. 3 weeks after Ramadan. | No change in fasted 10 or 30 m run during the afternoon, but ↑ fatigue index during Ramadan. | - | ↑ in vertical jump height from pre-Ramadan to the 2nd and 4th week of Ramadan, especially in the afternoon. Significant ↑ in vertical jump performance from pre-to post-Ramadan, especially in the afternoon. | - |
| [10] | Mean speed; Mean HR; Distance covered in 30 min TT run; Physiological variables taken before and after the 60 min exercise runs. | 10 moderately trained male runners | 27.3 ± 7.2 years | 1 week before Ramadan. During Ramadan. 1 week after Ramadan. | Shorter distance covered during the 30 min TT run during Ramadan. | - | - | - |
| [17] | VO2max; Submaximal VO2 kinetics; Anthropometric parameters; MVC; Running efficiency; Running Performance | 18 well-trained Muslim runners (EG, n = 9; CG, n = 9) | 23.6 ± 2.9 years | 1 week before Ramadan. Last week of the fasting period. After Ramadan. | Significant ↓ in running speed at VO2max in the EG. No changes in VO2max or running efficiency. Significant improvement of VO2 kinetics in EG. Significant ↓ in 5000 m running in EG. | - | No significant difference was observed in MVC between groups. Significant ↓ in MVC was observed, after Ramadan, only in the EG. | No significant differences on BM and FM between groups before and after (EG ↓ 0.8% FM; CG ↓ 1.3% FM). |
| [21] | PA; BC; Muscle force; EMG activity. | 11 moderately active Muslim males | 31.0 ± 3.0 years | 1 month and 1 week before Ramadan. During Ramadan. 1 month after Ramadan. | - | - | Maximal force was maintained during Ramadan. Maximal isometric torque measurements were not significantly different between sessions for both the knee extensors and flexors. | Little influence of Ramadan on BM and BC. |
| [37] | Upper arm girth; Isometric strength; Blood sample; RPE; BMI. | 29 participants (19 men, 12 women). Post-prandial group (n = 5 men, n = 5 women). Fasting group (n = 12 men, n = 7 women) | 22.0 ± 3.3 years | Pre-fasting. Post-fasting - session #1, 2, 3, 4 and 5. (8 h water-only fast) | - | - | Upper arm girth ↑ significantly within each group. Elbow extension and isometric strength ↓ significantly over time within each group. Less induction of muscle damage (EG). | BMI was similar between groups and sessions. |
| [38] | Wmax-A; Wmax-L; VJH; HGF; Anthropometric data; Hemoglobin and hematocrit | 20 trained men (RF, n = 10). (CG, n = 10) | RF, 21.8 ± 1.9 years; CG, 20.5 ± 1.0 years | Before Ramadan. End of the 1st week of Ramadan (R1). During the 4th week of Ramadan (R4). | - | - | Significant ↓ in the Wmax-A and Wmax-L during Ramadan. No significant change in VJH and HGF during Ramadan. | BM and BM index was ↓ at R1 and R4. FM was lower at R4 (↓0.3%).e |
| [39] | VO2max; MAP; Reaction time; Anthropometric variables. | 10 adolescents karate athletes | 18.5 ± 0.5 years | 3 weeks before Ramadan. At the end of the first week of Ramadan. During the 4th week of Ramadan. 3 weeks after Ramadan. | No significant changes at VO2max, MAP and HRmax during Ramadan. No effect on reaction time. | - | - | No significant changes in BM and FM during Ramadan. |
| [9] | VO2max; HIE; Flexibility; Agility; Vertical jump; Handgrip strength. | 77 untrained Muslim men (EG, n = 37; CG, n = 40) | EG, 22.6 ± 1.8 years. CG, 23.0 ±1.5 years | 1 week pre-Remadan. During Ramadan. 2 weeks post-Ramadan. | Significant ↓ in VO2max. | Significant ↓ in HIE | Vertical jump did not show any alteration. Non-significant variation in handgrip strength. | ↓ BM, but not significant. |
| [40] | Ventilatory variables; Metabolic variables. | 16 healthy and active men (FAST, n = 8) (FED, n = 8) | FAST, 20.9 ± 2.0 years; FED, 21.3 ± 2.5 years | 3 d/week for 6 weeks in the fasted state (Night fast) | Significant ↑ of VO2max for both groups. ↓of time to run 3000 m (EG and CG). | - | - | Fat oxidation was not modified by training. |
| [6] | TRF; ND; BC; Strength; Blood sample. | 34 resistance-trained males (TRF, n = 17; ND, n = 17) | TRF, 29.2 ± 3.8 years; ND, 28.5 ± 3.5 years | Tested 8 weeks pre-RT. 8 weeks of TRF. Tested 8 weeks post-RT. (Intermittent fast 8/16 h) | - | - | Maintained in TRF and ND. | Significant ↓ FM TRF (−16.4%); FFM was maintained in TRF and ND. |
| [41] | Maximal speed; Mean speed; Maximal power; Mean power; Vertical stiffness; Vertical COM; FI; Blood sample; HR; Body mass; RPE; | 21 active males | 29.8 ± 5.9 years | Fed/control session (pre-3 d of IF). 3 d of IF. | - | Significant effect of fasting on maximal and mean speed, maximal and mean power, vertical stiffness and vertical COM displacement. Sprint speed and mean power significantly ↓ from the CG. 3 d of IF impaired speed and power through a ↓ in vertical stiffness. | - | No significant changes on BM loss. |
| [2] | RT-TRF; BC; Muscle strength. | 18 active men (RT-TRF, n= 10; RT-ND, n = 8) | RT-ND, 22.0 ± 2.4 years. RT-TRF, 22.9 ± 4.1 years | 8 weeks of RT-ND. 8 weeks of RT-TRF. TRF for 4 d/week. Analysis 4 and 8 weeks post study. (No fasting on training days; intermittent fasting on non-training days 4/20 h) | - | - | ↑in upper and lower body muscle strength in ND and TRF groups, but ↑ were better in RT-TRF group. No changes after 4 weeks. | TRF-RT group lost up to 5.5% and 22% of initial BM and FM, respectively. |
| [42] | VO2max; HRmax; MVIC; BC; Sleep; Tre; Tsk; RPE; Blood markers; Training load. | 14 male trained Muslim football players | 21.8 ± 2.4 years | Before Ramadan. During Ramadan. After Ramadan. | mLIST were significantly faster in both CG (before and after Ramadan) as compared to Ramadan fasting group. An adverse effect on prolonged performance during Ramadan fasting. | - | Minimal ↓ in fatigue within the working muscles and in the neuromuscular activation. No changes were verifying in MVIC of the upper limb. No significant differences on knee extension MVIC over trials in each group. | BM at pre- and post-exercise was not significantly different before, during and after Ramadan. |
| [43] | VO2peak; Anaerobic power; BC; Blood sample; Urine sample. | 20 healthy male | EG, 21.0 ± 1.0 years; CG, 20.0 ± 1.0 years | 7 d of DS and EF. Baseline data (day 0). Day #2, 4, 6, 8, 10 (exercise test). (Intermittent fasting with lunch deprivation) | - | ↓ WnT power in EG during Day 2, Performance returned to baseline results from Day 4. HIT TTE in EG ↓throughout the 10-day period, but seems to recovered at the end of the experiment. | - | ↓ BM in the EG (−1.55%). |
| [11] | MVIC; Voluntary activation level; Neuromuscular efficiency Body mass. | 10 healthy male | 22.1 ± 2.0 years | Before Ramadan. During Ramadan. After Ramadan. | - | - | MVIC↓during Ramadan. Voluntary activation level↓during Ramadan. Neuromuscular efficiency remained unaffected by Ramadan. | BM remained unaffected by Ramadan. |
| [44] | VO2 peak, PO, PPO, Mean PO, FI, Blood samples, VT1, VT2 | 20 male cyclists (SIT FAST, n = 11; SIT CHO, n = 9). | SIT FAST, 33.3 ± 7.2 years SIT CHO 34.0 ± 8.2 years | SIT in overnight fasted state or with carbohydrate supplementation. Groups performed 3 times per week for 4 weeks. | PPO was significantly ↑ in SIT CHO compared to SIT FAST. No differences in post-training VO2 VT1 nor VT2 between groups. | - | - | - |
| [45] | VO2max; VCO2; HR; BM; Time to exhaustion; RER; Fat and CHO oxidation rate; Muscle and blood samples. | 20 young male. (Fasted state, n = 10; Fed state CHO, n = 10) | d.s | 6 weeks endurance training program, 4 days per week, in fasted or ingested CHO before and during training sessions. | VO2 max and time to exhaustion, between fasted and fed groups, were similar in the pre-test and ↑ 9% after training, but not significantly. | - | - | ↑ fat mass oxidation in fast group (+ 21%), but not significant. Body weight ↓ in both groups (not significantly). |
| [46] | VO2 peak; VO2; VCO2; RER; BM; Muscle and blood samples. | 20 moderately active males. (Fast, n = 10; CHO, n = 10) | 21.2 ± 0.4 years | Endurance training program, 6 weeks of 3 days per week, in fasted or CHO fed state. | VO2 peak ↑ within group but was not different between groups. | - | - | No significant changes on body mass loss. |
| [47] | VO2 peak; VO2; VCO2; RER; HR; Muscle and blood samples. | 8 males | 25 ± 2 years | Cycling in fasted state or 2 h following ingestion of CHO. | VCO2 ↓ significantly during fast exercise. VO2; HR and RER were not different during exercise between trials. | - | - | - |
| [48] | VO2 max; VO2 peak; biochemical analyses. | 8 females untrained 6 males untrained | 26.6 ± 5.8 years | 4 weeks of 5 days per week endurance cycle ergometer in overnight-fasted or acutely fed state. | Fast group showed ↑ in VO2 max than Fed group. Peak power ↑ more in fasted group compared to CG. | - | - | - |
| [49] | HR; Blood samples; Reaction time; cognitive performance. | 21 physically active, healthy Muslims males. | 29.8 ± 5.9 years | 3 days of IF | - | Simple and complex reaction times ↑ during the 3d-IF after 2 bouts of intensive RS. | - | - |
| [24] | Skeletal muscle hypertrophy; muscular performance; BM; FFM; Commonly physiological and metabolic variables. | 40 resistance trained females. (CG, n = 14; TRF, n = 13; TRFHMB, n13). | CG, 22.0 ±2.4 TRF, 22.1 ± 2.1 TRFHMB, 22.3 3.4 | 8 weeks of supervised RT in TRF state with or without HMB. | - | - | TRF did not attenuate FFM, muscle hypertrophy, or developments in muscle performance. | FFM ↑ in three groups without differences between all. Significant ↓ in FM in TRF group. |
| [50] | PA level; Anthropometric status; Body composition; Dietary information. | 33 healthy young males | 21.85 ± 1.87 years | Before Ramadan; 1st week of Ramadan; Last week of Ramadan. | Statistically significant ↓ in high intensity PA in 1st w of RF. Statistically significant ↓ in moderate PA in 1st w of RF compared with before RF. | - | - | Significant ↓ in BM and %FM at last week of RF compared to before RF. |
| [51] | CMJ; RS test; YYIRT1 | 30 amateur soccer players. (MTG, n = 10; ETG, n = 10; CG, n = 10) | 22.9 ± 1.3 years | Before Ramadan. After Ramadan. | - | After RF YYIRT1 ↑in the morning and in the evening. ↑in RS training (fasted state) in the morning or in the evening. But significant difference compared to before and after Ramadan in the morning. | No differences were observed in CMJ before and after RF for any group. | - |
| [52] | Blood samples; VO2 max; HR; BM; Endurance exercise performance; metabolic measurements; Mood state and daytime sleepiness. | 12 Muslims men runners. | 27.9 ± 7.2 years. | Endurance running performance during Ramadan, after ingesting LGI or normal mixed CHO food as sahur meal. | TT distance ran was statistically significant ↓ in LGI vs. CG. | - | - | No significant changes in BM. |
| Reference | Selection Bias | Study Design | Confounders | Data Collection Method | Withdrawals | Global |
|---|---|---|---|---|---|---|
| [34] | 1 | 1 | 3 | 3 | 3 | Weak |
| [4] | 1 | 1 | 3 | 3 | 3 | Weak |
| [35] | 1 | 1 | 3 | 3 | 3 | Weak |
| [36] | 2 | 1 | 3 | 3 | 3 | Moderate |
| [46] | 1 | 2 | 3 | 3 | 3 | Moderate |
| [10] | 1 | 1 | 3 | 3 | 3 | Weak |
| [48] | 1 | 2 | 3 | 3 | 3 | Moderate |
| [45] | 1 | 2 | 3 | 3 | 3 | Moderate |
| [17] | 1 | 1 | 3 | 3 | 3 | Weak |
| [21] | 1 | 1 | 3 | 3 | 3 | Weak |
| [37] | 1 | 1 | 3 | 3 | 3 | Weak |
| [38] | 1 | 1 | 3 | 3 | 3 | Weak |
| [52] | 3 | 2 | 3 | 3 | 3 | Strong |
| [39] | 1 | 1 | 3 | 3 | 3 | Weak |
| [9] | 2 | 1 | 3 | 3 | 3 | Moderate |
| [40] | 1 | 3 | 3 | 3 | 3 | Moderate |
| [41] | 1 | 2 | 3 | 3 | 3 | Moderate |
| [6] | 1 | 3 | 3 | 3 | 3 | Moderate |
| [2] | 1 | 3 | 3 | 3 | 3 | Moderate |
| [49] | 3 | 2 | 3 | 3 | 3 | Strong |
| [42] | 1 | 3 | 3 | 3 | 3 | Moderate |
| [51] | 2 | 2 | 3 | 3 | 3 | Strong |
| [43] | 1 | 3 | 3 | 3 | 3 | Moderate |
| [44] | 2 | 2 | 3 | 3 | 3 | Moderate |
| [11] | 1 | 1 | 3 | 3 | 3 | Weak |
| [50] | 1 | 1 | 3 | 3 | 3 | Weak |
| [24] | 2 | 3 | 3 | 3 | 3 | Strong |
| [47] | 1 | 2 | 3 | 3 | 3 | Moderate |
| Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|
| Primary Outcomes | Point Estimate | CI Lower | CI Upper | p-Value | Q-Value | p-Value | I-Squared |
| Muscle strength | |||||||
| Vertical Jump (cm) * | |||||||
| All studies | |||||||
| Only Ramadan IF studies | 0.012 | −0.324 | 0.348 | 0.945 | 43.598 | <0.001 | 95.413 |
| Only TRF studies | |||||||
| Vertical Jump (cm) ** | |||||||
| All studies | |||||||
| Only Ramadan IF studies | 0.021 | −0.316 | 0.358 | 0.902 | 1.23 | 0.541 | <0.001 |
| Only TRF studies | |||||||
| Aerobic capacity | |||||||
| VO2max (L·min−1) * | |||||||
| All studies | 0.051 | −0.275 | 0.376 | 0.761 | 1.205 | 0.877 | <0.001 |
| Only Ramadan IF studies | −0.046 | −0.417 | 0.324 | 0.806 | 0.055 | 0.973 | <0.001 |
| Only TRF studies | 0.375 | −0.303 | 1.053 | 0.278 | 0.007 | 0.932 | <0.001 |
| VO2max (L·min−1) ** | |||||||
| All studies | −1.045 | −1.488 | −0.602 | <0.001 | 80.05 | <0.001 | 96.252 |
| Only Ramadan IF studies | −2.204 | −2.745 | −1.663 | <0.001 | 21.229 | <0.001 | 95.289 |
| Only TRF studies | 1.315 | 0.543 | 2.087 | 0.001 | 5.323 | 0.021 | 81.212 |
| 30 min distance (m) ** | |||||||
| All studies | |||||||
| Only Ramadan IF studies *** | 0.187 | −0.405 | 0.78 | 0.536 | 0.044 | 0.835 | <0.001 |
| Only TRF studies | |||||||
| Anaerobic capacity | |||||||
| Mean power (w) * | |||||||
| All studies | 0.04 | −0.753 | 0.834 | 0.921 | 123.219 | <0.001 | 98.377 |
| Only Ramadan IF studies | 0.355 | −0.442 | 1.151 | 0.383 | 38.813 | <0.001 | 97.424 |
| Only TRF studies | |||||||
| Peak Power (w) * | |||||||
| All studies | 0.758 | −0.019 | 1.535 | 0.056 | 113.389 | <0.001 | 98.236 |
| Only Ramadan IF studies | −0.11 | −0.912 | 0.691 | 0.788 | 40.109 | <0.001 | 97.507 |
| Only TRF studies | |||||||
| Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|
| Secondary Outcomes | Point Estimate | CI Lower | CI Upper | p-Value | Q-Value | p-Value | I-Squared |
| Body Mass (Kg) * | |||||||
| All studies | −0.435 | −0.811 | −0.059 | 0.023 | 30.718 | 0.001 | 64.19 |
| Only Ramadan IF studies | −0.638 | −1.248 | −0.029 | 0.04 | 23.256 | 0.001 | 74.2 |
| Only TRF studies | −0.152 | −0.476 | 0.173 | 0.359 | 2.635 | 0.621 | <0.001 |
| Body Mass (Kg) ** | |||||||
| All studies | −0.058 | −0.388 | 0.272 | 0.732 | 3.58 | 0.611 | <0.001 |
| Only Ramadan IF studies | −0.313 | −0.955 | 0.329 | 0.339 | 0.508 | 0.476 | <0.001 |
| Only TRF studies | 0.034 | −0.351 | 0.419 | 0.862 | 2.246 | 0.523 | <0.001 |
| Fat Mass (%) * | |||||||
| All studies | −0.848 | −1.193 | −0.502 | <0.001 | 7.307 | 0.121 | 45.256 |
| Only Ramadan IF studies | −0.910 | −1.284 | −0.535 | <0.001 | 6.616 | 0.085 | 54.655 |
| Only TRF studies | |||||||
| Fat Mass (%) ** | |||||||
| All studies | −0.224 | −0.751 | 0.302 | 0.404 | 0.029 | 0.986 | <0.001 |
| Only Ramadan IF studies | −0.215 | −0.853 | 0.423 | 0.508 | 0.026 | 0.872 | <0.001 |
| Only TRF studies | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
M. Correia, J.; Santos, I.; Pezarat-Correia, P.; Minderico, C.; V. Mendonca, G. Effects of Intermittent Fasting on Specific Exercise Performance Outcomes: A Systematic Review Including Meta-Analysis. Nutrients 2020, 12, 1390. https://doi.org/10.3390/nu12051390
M. Correia J, Santos I, Pezarat-Correia P, Minderico C, V. Mendonca G. Effects of Intermittent Fasting on Specific Exercise Performance Outcomes: A Systematic Review Including Meta-Analysis. Nutrients. 2020; 12(5):1390. https://doi.org/10.3390/nu12051390
Chicago/Turabian StyleM. Correia, Joana, Inês Santos, Pedro Pezarat-Correia, Cláudia Minderico, and Goncalo V. Mendonca. 2020. "Effects of Intermittent Fasting on Specific Exercise Performance Outcomes: A Systematic Review Including Meta-Analysis" Nutrients 12, no. 5: 1390. https://doi.org/10.3390/nu12051390
APA StyleM. Correia, J., Santos, I., Pezarat-Correia, P., Minderico, C., & V. Mendonca, G. (2020). Effects of Intermittent Fasting on Specific Exercise Performance Outcomes: A Systematic Review Including Meta-Analysis. Nutrients, 12(5), 1390. https://doi.org/10.3390/nu12051390