Proinflammatory Dietary Intake is Associated with Increased Risk of Metabolic Syndrome and Its Components: Results from the Population-Based Prospective Study



Abstract
1. Introduction
2. Materials and Methods
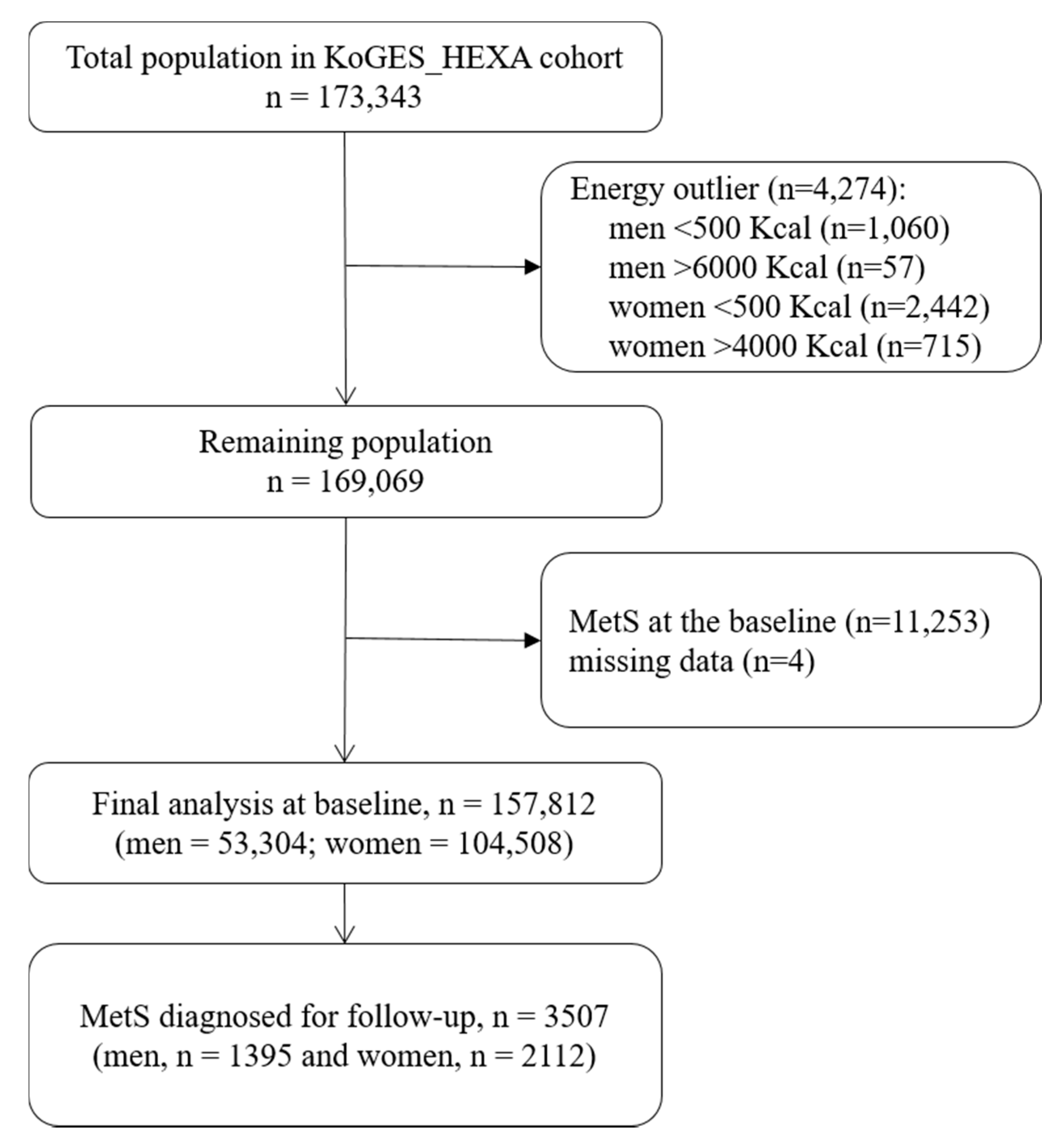
2.1. Cohort Characteristics
2.2. Computation of the Dietary Inflammatory Index (DII®)
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bruce, K.; Byrne, C. The metabolic syndrome: Common origins of a multifactorial disorder. Postgrad. Med. J. 2009, 85, 614–621. [Google Scholar] [CrossRef]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Andreeva, V.; Kesse-Guyot, E.; Hercberg, S. Dietary patterns, inflammation and the metabolic syndrome. Diabetes Metab. Syndr. 2013, 39, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003-2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Kang, D.R.; Jang, J.-Y.; Shin, J.-H.; Kim, J.Y.; Choi, S.; Cho, E.J.; Park, J.-S.; Sohn, I.S.; Jo, S.-H. Metabolic syndrome epidemic among Korean adults: Korean survey of Cardiometabolic Syndrome. Atherosclerosis 2018, 277, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Canela, M.; Bes-Rastrollo, M.; Martínez-González, M.A. The role of dietary inflammatory index in cardiovascular disease, metabolic syndrome and mortality. Int. J. Mol. Sci. 2016, 17, 1265. [Google Scholar] [CrossRef]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jönsson, L.S.; Kolb, H.; Lansink, M. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106, S1–S78. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.J.; Fernandez, M.L. Dietary strategies to reduce metabolic syndrome. Rev. Endocr. Metab. Disord. 2013, 14, 241–254. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Na, W.; Kim, M.; Sohn, C. Dietary inflammatory index and its relationship with high-sensitivity C-reactive protein in Korean: Data from the health examinee cohort. Clin. Biochem. 2018, 62, 83–88. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Zucchetto, A.; Montella, M.; Serraino, D.; La Vecchia, C.; Rossi, M. Dietary inflammatory index and endometrial cancer risk in an Italian case–control study. Br. J. Nutr. 2016, 115, 138–146. [Google Scholar] [CrossRef]
- Ramallal, R.; Toledo, E.; Martínez-González, M.A.; Hernández-Hernández, A.; García-Arellano, A.; Shivappa, N.; Hebert, J.R.; Ruiz-Canela, M. Dietary inflammatory index and incidence of cardiovascular disease in the SUN cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef]
- Phillips, C.M.; Shivappa, N.; Hébert, J.R.; Perry, I.J. Dietary inflammatory index and mental health: A cross-sectional analysis of the relationship with depressive symptoms, anxiety and well-being in adults. Clin. Nutr. 2018, 37, 1485–1491. [Google Scholar] [CrossRef]
- Cervo, M.M.; Shivappa, N.; Hebert, J.R.; Oddy, W.H.; Winzenberg, T.; Balogun, S.; Wu, F.; Ebeling, P.; Aitken, D.; Jones, G. Longitudinal associations between dietary inflammatory index and musculoskeletal health in community-dwelling older adults. Clin. Nutr. 2020, 39, 516–523. [Google Scholar] [CrossRef]
- Phillips, C.M.; Chen, L.-W.; Heude, B.; Bernard, J.Y.; Harvey, N.C.; Duijts, L.; Mensink-Bout, S.M.; Polanska, K.; Mancano, G.; Suderman, M. Dietary inflammatory index and non-communicable disease risk: A narrative review. Nutrients 2019, 11, 1873. [Google Scholar] [CrossRef]
- Wirth, M.; Burch, J.; Shivappa, N.; Violanti, J.M.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Miller, D.B.; Mnatsakanova, A. Association of a dietary inflammatory index with inflammatory indices and the metabolic syndrome among police officers. J. Occup. Environ. Med. 2014, 56, 986–989. [Google Scholar] [CrossRef]
- Sokol, A.; Wirth, M.D.; Manczuk, M.; Shivappa, N.; Zatonska, K.; Hurley, T.G.; Hébert, J.R.J. Association between the dietary inflammatory index, waist-to-hip ratio and metabolic syndrome. Nutr. Res. 2016, 36, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, A.M.; Toledo, E.; Rodriguez-Diez, M.C.; Gea, A.; Lopez-Iracheta, R.; Shivappa, N.; Hébert, J.R.; Martinez-Gonzalez, M.A. Dietary indexes, food patterns and incidence of metabolic syndrome in a Mediterranean cohort: The SUN project. Clin. Nutr. 2015, 34, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Neufcourt, L.; Assmann, K.; Fezeu, L.; Touvier, M.; Graffouillère, L.; Shivappa, N.; Hébert, J.; Wirth, M.; Hercberg, S.; Galan, P. Prospective association between the dietary inflammatory index and metabolic syndrome: Findings from the SU. VI. MAX study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-Y.; Lee, J.; Kim, J. Association between Dietary Inflammatory Index and Metabolic Syndrome in the General Korean Population. Nutrients 2018, 10, 648. [Google Scholar] [CrossRef] [PubMed]
- Nikniaz, L.; Nikniaz, Z.; Shivappa, N.; Hébert, J.R. The association between dietary inflammatory index and metabolic syndrome components in Iranian adults. Prim. Care Diabetes 2018, 12, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.-G. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2016, 46, e20. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, H.S.; Kim, D.J.; Han, J.H.; Kim, S.M.; Cho, G.J.; Kim, D.Y.; Kwon, H.S.; Kim, S.R.; Lee, C.B. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res. Clin. Pract. 2007, 75, 72–80. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Mina, K.; Fritschi, L.; Knuiman, M. A valid semiquantitative food frequency questionnaire to measure fish consumption. Eur. J. Clin. Nutr. 2007, 61, 1023–1031. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; Ahn, Y.-O.; Paik, H.-Y.; Aim, Y.; Tokudome, Y.; Hamajima, N.; Inouc, M.; Tajima, K.; Ahn, Y. Development of a food frequency questionnaire in Koreans. Asia Pac. J. Clin. Nutr. 2003, 12, 243–250. [Google Scholar] [PubMed]
- National Rural Resources Development Institute. Food Composition Table, 9th ed.; Rural Development Administration, National Rural Resources Development Institute: Suwon, Korea. Available online: http://koreanfood.rda.go.kr/eng/fctFoodSrchEng/engMain (accessed on 15 July 2019).
- Hebert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII®): Lessons Learned, Improvements Made and Future Directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Sohn, C.; Kwon, M.; Na, W.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive association between dietary inflammatory index and the risk of osteoporosis: Results from the KoGES_Health Examinee (HEXA) cohort study. Nutrients 2018, 10, 1999. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Shivappa, N.; Crichton, G.; Hébert, J.R. No significant independent relationships with cardiometabolic biomarkers were detected in the Observation of Cardiovascular Risk Factors in Luxembourg study population. Nutr. Res. Pract. 2014, 34, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Shivappa, N.; Nasreddine, L.; Kharroubi, S.; Itani, L.; Hwalla, N.; Mehio Sibai, A.; Hebert, J.R. Role of inflammation in the association between the western dietary pattern and metabolic syndrome among Lebanese adults. Int. J. Food Sci. Nutr. 2017, 68, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Kenđel, G.J.; Pavičić, S.Ž.; Klobučar, S.M.; Mrakovcic-Sutic, I.; Šutić, I. Metabolic syndrome and its association with the Dietary Inflammatory Index (DII®) in a Croatian working population. J. Hum. Nutr. Diet. 2020, 33, 128–137. [Google Scholar] [CrossRef]
- Greenberg, A.; McDaniel, M. Identifying the links between obesity, insulin resistance and β-cell function: Potential role of adipocyte-derived cytokines in the pathogenesis of type 2 diabetes. Eur. J. Clin. Invest. 2002, 32, 24–34. [Google Scholar] [CrossRef]
- Grundy, S.M. Inflammation, metabolic syndrome, and diet responsiveness. Circulation 2003, 108, 126–128. [Google Scholar] [CrossRef]
- Ordovas, J. Diet/genetic interactions and their effects on inflammatory markers. Nutr. Rev. 2007, 65, S203–S207. [Google Scholar] [CrossRef]
- McLaughlin, T.; Abbasi, F.; Lamendola, C.; Liang, L.; Reaven, G.; Schaaf, P.; Reaven, P. Differentiation between obesity and insulin resistance in the association with C-reactive protein. Circulation 2002, 106, 2908–2912. [Google Scholar] [CrossRef]
- Carr, M.C. The emergence of the metabolic syndrome with menopause. J. Clin. Endocrinol. Metab. 2003, 88, 2404–2411. [Google Scholar] [CrossRef] [PubMed]
- Bermudez, V.; Olivar, L.C.; Torres, W.; Navarro, C.; Gonzalez, R.; Espinoza, C.; Morocho, A.; Mindiola, A.; Chacin, M.; Arias, V. Cigarette smoking and metabolic syndrome components: A cross-sectional study from Maracaibo City, Venezuela. F1000Research 2018, 7, 565. [Google Scholar] [CrossRef]
- Chen, C.-C.; Li, T.-C.; Chang, P.-C.; Liu, C.-S.; Lin, W.-Y.; Wu, M.-T.; Li, C.-I.; Lai, M.-M.; Lin, C.-C. Association among cigarette smoking, metabolic syndrome, and its individual components: The metabolic syndrome study in Taiwan. Metabolism 2008, 57, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Thorand, B.; Baumert, J.; Döring, A.; Herder, C.; Kolb, H.; Rathmann, W.; Giani, G.; Koenig, W. Sex differences in the relation of body composition to markers of inflammation. Atherosclerosis 2006, 184, 216–224. [Google Scholar] [CrossRef]
- Kang, Y.; Kim, J. Gender difference on the association between dietary patterns and metabolic syndrome in Korean population. Eur. J. Nutr. 2016, 55, 2321–2330. [Google Scholar] [CrossRef]
- Rossi, I.A.; Bochud, M.; Bovet, P.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Taffé, P. Sex difference and the role of leptin in the association between high-sensitivity C-reactive protein and adiposity in two different populations. Eur. J. Epidemiol. 2012, 27, 379–384. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Quintiles of Dietary Inflammatory Index® a | p for Trend b | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ||
| Total observations (n = 157,812) | 31,542 | 31,565 | 31,593 | 31,555 | 31,557 | |
| Total cases of MS (n = 3507) | 681 | 704 | 732 | 694 | 696 | |
| DII® score range c | −9.12 to −0.97 | −0.97 to 0.41 | 0.41 to 1.29 | 1.29 to 2.19 | 2.19 to 6.93 | |
| Age (years) | 52.1 (7.97) d | 52.2 (8.14) | 52.6 (8.22) | 53.2 (8.45) | 54.5 (8.65) | <0.0001 |
| BMI (Kg/m2) e | 23.9 (2.77) | 23.8 (2.78) | 23.8 (2.76) | 23.7 (2.77) | 23.6 (2.86) | <0.0001 |
| Sex | ||||||
| Male (n = 53,304) | 10,261 (32.6) f | 10,678 (33.9) | 10,777 (34.2) | 10,545 (33.5) | 11,043 (35.0) | <0.0001 |
| Female (n = 104,508) | 21,281 (67.4) | 20,887 (66.1) | 20,816 (65.8) | 21,010 (66.5) | 20,514 (65.0) | |
| Education level | ||||||
| Elementary school | 3583 (11.5) | 4066 (13.1) | 4886 (15.7) | 5895 (19.0) | 7992 (25.7) | <0.0001 |
| Middle ~ high school | 18,511 (59.5) | 18,259 (58.6) | 18,117 (58.1) | 17,971 (57.8) | 17,360 (55.9) | |
| College~ | 9014 (29.0) | 8812 (28.3) | 8205 (26.2) | 7243 (23.2) | 5712 (18.4) | |
| Alcohol consumption | ||||||
| Never | 15,609 (49.7) | 15,511 (49.3) | 15,811 (50.1) | 16,196 (51.4) | 16,646 (53.0) | <0.0001 |
| Past | 1258 (4.0) | 1148 (3.7) | 1117 (3.6) | 1273 (4.1) | 1294 (4.1) | |
| Current | 14,525 (46.3) | 14,780 (47.0) | 14,573 (46.3) | 13,986 (44.5) | 13,495 (42.9) | |
| Physical activity g | ||||||
| Irregular | 12,234 (38.9) | 13,719 (43.6) | 14,607 (46.4) | 15,688 (49.9) | 17,944 (57.1) | <0.0001 |
| Regular | 19,212 (61.1) | 17,758 (56.4) | 16,911 (53.6) | 15,759 (50.1) | 13,494 (42.9) | |
| Income (million (s) Korean won) | ||||||
| Less than 1 | 2017 (7.8) | 2206 (8.3) | 2691 (10.1) | 3467 (13.0) | 4669 (17.3) | |
| 1~less than 2 | 4636 (18.0) | 4924 (18.5) | 5290 (19.9) | 5707 (21.5) | 6552 (24.2) | <0.0001 |
| 2~less than 3 | 5929 (23.0) | 6343 (23.9) | 6079 (22.9) | 5901 (22.2) | 5794 (21.4) | |
| More than 3 | 13,243 (51.2) | 13,088 (49.3) | 12,545 (47.1) | 11,522 (43.3) | 10,056 (37.1) | |
| Marital status | ||||||
| Married | 28,269 (90.3) | 28,224 (90.0) | 27,972 (89.1) | 27,270 (87.0) | 26,543 (84.8) | <0.0001 |
| Unmarried/divorced | 3055 (9.7) | 3142 (10.0) | 3453 (10.9) | 4101 (13.0) | 4788 (15.2) | |
| Smoking | ||||||
| Never | 23,450 (74.8) | 23,161 (73.7) | 23,178 (73.6) | 23,255 (74.0) | 22,278 (70.9) | <0.0001 |
| Past | 4312 (13.7) | 4668 (14.9) | 4674 (14.9) | 4508 (14.3) | 4562 (14.5) | |
| Current | 3610 (11.5) | 3605 (11.4) | 3632 (11.5) | 3680 (11.7) | 4592 (14.6) | |
| Menopause status | ||||||
| Post-menopause | 10,986 (55.9) | 11,053 (55.9) | 11,360 (57.4) | 12,050 (60.3) | 12,994 (65.2) | <0.0001 |
| Pre-/peri-menopause | 8644 (44.1) | 8731 (44.1) | 8427 (42.6) | 7943 (39.7) | 6931 (34.8) | |
| Family history of diabetes | ||||||
| Negative | 25,796 (81.8) | 25,901 (82.1) | 25,834 (81.8) | 26,010 (82.5) | 26,451 (83.9) | <0.0001 |
| Positive | 5746 (18.2) | 5664 (17.9) | 5759 (18.2) | 5545 (17.5) | 5106 (16.1) | |
| Family history of hypertension | ||||||
| Negative | 22,605 (71.7) | 22,188 (70.3) | 22,293 (70.6) | 22,587 (71.6) | 22,986 (72.9) | <0.0001 |
| Positive | 8937 (28.3) | 9377 (29.7) | 9300 (29.4) | 8968 (28.4) | 8571 (27.1) | |
| Waist circumference (cm) | 80.5 (8.4) | 80.4 (8.4) | 80.4 (8.3) | 80.2 (8.3) | 80.4 (8.4) | 0.05 |
| Triglycerides (mg/dL) | 117.2 (78.3) | 118.6 (78) | 118.6 (79.2) | 119 (80) | 121.2 (82.5) | <0.0001 |
| HDL-C (mg/dL) | 55.3 (12.8) | 55 (12.7) | 54.8 (12.7) | 54.7 (12.7) | 54.3 (13) | <0.0001 |
| Glucose concentration (mg/dL) | 93.5 (20) | 93.4 (18.4) | 93.8 (19.5) | 93.8 (19.8) | 94 (20.2) | <0.0001 |
| Blood pressure (mmHg) | ||||||
| Systolic | 121.5 (15) | 121.4 (14.9) | 121.7 (15) | 121.8 (15.1) | 122.2 (15.3) | <0.0001 |
| Diastolic | 74.3 (9.9) | 74.3 (9.7) | 74.4 (9.8) | 74.4 (9.7) | 74.6 (9.8) | 0.05 |
| Quintiles of DII® Score a,b,c | P for Trend d | DII® Continuous | ||||||
|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | ||||
| Cases/Persons-years | 618/245,414 | 704/236,148 | 732/231,182 | 694/231,190 | 696/220,584 | |||
| DII®, median (IQR) | ||||||||
| All | −2.05 (1.46) | −0.20 (0.68) | 0.91 (0.43) | 1.64 (0.40) | 2.86 (0.96) | |||
| Men | −2.05 (1.47) | −0.20 (0.69) | 0.91 (0.43) | 1.64 (0.39) | 2.95 (1.06) | |||
| Women | −2.05 (1.45) | −0.20 (0.68) | 0.90 (0.43) | 1.65 (0.40) | 2.82 (0.89) | |||
| Metabolic syndrome | ||||||||
| All | 1.00 (ref.) | 1.16 (1.03−1.29) c | 1.25 (1.12−1.41) | 1.26 (1.11−1.43) | 1.31 (1.15−1.49) | 0.002 | 1.02 (1.01−1.04) | |
| Men | 1.00 (ref.) | 1.04 (0.88−1.24) | 1.09 (0.91−1.31) | 1.23 (1.01−1.48) | 1.14 (0.93−1.39) | 0.39 | 0.98 (0.96−1.01) | |
| Women | 1.00 (ref.) | 1.23 (1.06−1.42) | 1.36 (1.17−1.58) | 1.28 (1.08−1.50) | 1.43 (1.21−1.69) | <0.0001 | 1.04 (1.02−1.07) | |
| Elevated waist circumference | ||||||||
| All | 1.00 (ref.) | 1.13 (1.03−1.22) | 1.18 (1.08−1.29) | 1.23 (1.11−1.35) | 1.37 (1.24−1.51) | <0.0001 | 1.06 (1.04−1.07) | |
| Men (≥90cm) | 1.00 (ref.) | 1.15 (0.99−1.33) | 1.25 (1.07−1.47) | 1.20 (1.02−1.42) | 1.28 (1.08−1.52) | 0.01 | 1.06 (1.03−1.09) | |
| Women (or ≥85cm) | 1.00 (ref.) | 1.12 (1.01−1.24) | 1.14 (1.02−1.27) | 1.25 (1.11−1.40) | 1.42 (1.26−1.61) | <0.0001 | 1.06 (1.03−1.08) | |
| High triacylglycerol (≥150 mg/dL), | ||||||||
| All | 1.00 (ref.) | 1.15 (1.07−1.23) | 1.18 (1.11−1.27) | 1.20 (1.11−1.30) | 1.24 (1.14−1.35) | <0.0001 | 1.03 (1.01−1.04) | |
| Men | 1.00 (ref.) | 1.10 (0.97−1.24) | 1.11 (0.96−1.25) | 1.11 (0.96−1.27) | 1.11 (0.96−1.28) | 0.23 | 1.01 (0.98−1.03) | |
| Women | 1.00 (ref.) | 1.16 (1.07−1.26) | 1.22 (1.11−1.33) | 1.25 (1.13−1.37) | 1.30 (1.18−1.44) | <0.0001 | 1.03 (1.02−1.05) | |
| Low HDL-C | ||||||||
| All | 1.00 (ref.) | 1.20 (1.08−1.33) | 1.22 (1.09−1.37) | 1.37 (1.21−1.54) | 1.63 (1.44−1.84) | <0.0001 | 1.08 (1.06−1.11) | |
| Men (<40 mg/dL) | 1.00 (ref.) | 1.26 (1.03−1.53) | 1.15 (0.93−1.42) | 1.34 (1.08−1.67) | 1.59 (1.27−1.99) | 0.0001 | 1.06 (1.02−1.11) | |
| Women (<50 mg/dL) | 1.00 (ref.) | 1.17 (1.03−1.33) | 1.25 (1.09−1.43) | 1.37 (1.19−1.58) | 1.64 (1.41−1.90) | <0.0001 | 1.09 (1.06−1.12) | |
| High glucose (≥100 mg/dL) | ||||||||
| All | 1.00 (ref.) | 1.09 (1.03−1.16) | 1.14 (1.07−1.21) | 1.16 (1.08−1.24) | 1.18 (1.09−1.26) | <0.0001 | 1.02 (1.01−1.03) | |
| Men | 1.00 (ref.) | 1.08 (0.98−1.18) | 1.08 (0.98−1.20) | 1.08 (0.97−1.20) | 1.01 (0.90−1.13) | 0.94 | 0.99 (0.97−1.01) | |
| Women | 1.00 (ref.) | 1.10 (1.02−1.19) | 1.17 (1.07−1.27) | 1.21 (1.11−1.32) | 1.30 (1.18−1.43) | <0.0001 | 1.04 (1.02−1.05) | |
| High blood pressure | ||||||||
| All | 1.00 (ref.) | 1.11 (1.04−1.18) | 1.14 (1.06−1.22) | 1.14 (1.06−1.23) | 1.24 (1.15−1.34) | <0.0001 | 1.03 (1.02−1.04) | |
| Men | 1.00 (ref.) | 1.16 (1.04−1.30) | 1.13 (1.01−1.27) | 1.16 (1.03−1.31) | 1.17 (1.03−1.32) | 0.05 | 1.02 (1.00−1.04) | |
| Women | 1.00 (ref.) | 1.07 (0.99−1.16) | 1.14 (1.05−1.24) | 1.12 (1.02−1.23) | 1.29 (1.17−1.41) | <0.0001 | 1.04 (1.02−1.05) | |
| MS with Components | Quintiles of Dietary Inflammatory Index® (DII®) a,b,c | |||||||
|---|---|---|---|---|---|---|---|---|
| Menopausal Status | Q1 | Q2 | Q3 | Q4 | Q5 | P for trend d | DII® Continuous | |
| Metabolic syndrome | Pre-/peri- | 1.00 (ref.) | 1.02 (0.77−1.36) | 1.02 (0.75−1.39) | 1.19 (0.87−1.63) | 1.26 (0.90−1.77) | 0.11 | 1.03 (0.97−1.10) |
| Post- | 1.00 (ref.) | 1.27 (1.07−1.51) | 1.47 (1.23−1.76) | 1.28 (1.05−1.56) | 1.50 (1.23−1.83) | 0.0008 | 1.05 (1.02−1.09) | |
| Elevated waist circumference | Pre-/peri- | 1.00 (ref.) | 1.12 (0.95−1.34) | 0.93 (0.76−1.13) | 1.19 (0.97−1.46) | 1.42 (1.14−1.76) | 0.003 | 1.06 (1.02−1.10) |
| Post- | 1.00 (ref.) | 1.12 (0.99−1.28) | 1.22 (1.07−1.40) | 1.27 (1.10−1.46) | 1.40 (1.21−1.63) | <0.0001 | 1.05 (1.02−1.08) | |
| High triacylglycerol | Pre-/peri- | 1.00 (ref.) | 1.12 (0.97−1.29) | 1.11 (0.95−1.29) | 1.15 (0.98−1.36) | 1.25 (1.04−1.48) | 0.02 | 1.03 (1.00−1.06) |
| Post- | 1.00 (ref.) | 1.19 (1.07−1.33) | 1.29 (1.15−1.44) | 1.32 (1.18−1.49) | 1.37 (1.21−1.55) | <0.0001 | 1.04 (1.02−1.06) | |
| Low HDL-C | Pre-/peri- | 1.00 (ref.) | 1.15 (0.93−1.43) | 1.27 (1.01−1.58) | 1.46 (1.15−1.85) | 1.81 (1.41−2.33) | <0.0001 | 1.10 (1.05−1.16) |
| Post- | 1.00 (ref.) | 1.11 (0.94−1.31) | 1.15 (0.97−1.37) | 1.26 (1.05−1.51) | 1.45 (1.20−1.74) | <0.0001 | 1.07 (1.03−1.10) | |
| High glucose | Pre-/peri- | 1.00 (ref.) | 1.06 (0.92−1.21) | 1.13 (0.97−1.30) | 1.13 (0.97−1.32) | 1.27 (1.07−1.49) | 0.004 | 1.04 (1.01−1.07) |
| Post- | 1.00 (ref.) | 1.13 (1.02−1.25) | 1.20 (1.07−1.33) | 1.27 (1.14−1.43) | 1.33 (1.19−1.50) | <0.0001 | 1.04 (1.02−1.06) | |
| High blood pressure | Pre-/peri- | 1.00 (ref.) | 1.08 (0.94−1.25) | 1.15 (0.99−1.33) | 1.12 (0.95−1.32) | 1.42 (1.20−1.68) | 0.0001 | 1.06 (1.03−1.09) |
| Post- | 1.00 (ref.) | 1.09 (0.98−1.21) | 1.15 (1.04−1.29) | 1.14 (1.01−1.28) | 1.25 (1.11−1.41) | 0.0005 | 1.03 (1.01−1.05) | |
| Sex | Smoking e Status | Quintiles of Dietary Inflammatory Index® (DII®) a,b,c | ||||||
|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | P for Trend d | DII® Continuous | ||
| Elevated waist circumference | ||||||||
| Men | No | 1.00 (ref.) | 1.04 (0.79−1.38) | 1.07 (0.79−1.44) | 1.01 (0.74−1.39) | 1.18 (0.85−1.64) | 0.39 | 1.03 (0.97−1.09) |
| Yes | 1.00 (ref.) | 1.17 (0.98−1.40) | 1.31 (1.08−1.57) | 1.24 (1.02−1.51) | 1.25 (1.02−1.53) | 0.05 | 1.06 (1.02−1.10) | |
| Women | No | 1.00 (ref.) | 1.10 (0.99−1.22) | 1.11 (0.99−1.24) | 1.23 (1.09−1.38) | 1.41 (1.25−1.59) | <0.0001 | 1.05 (1.03−1.08) |
| Yes | 1.00 (ref.) | 2.20 (1.13−4.28) | 3.01 (1.49−6.05) | 2.31 (1.05−5.06) | 2.30 (1.04−5.06) | 0.14 | 1.10 (0.97−1.24) | |
| High triacylglycerol | ||||||||
| Men | No | 1.00 (ref.) | 1.30 (1.01−1.67) | 1.29 (0.99−1.69) | 1.23 (0.92−1.63) | 1.25 (0.92−1.69) | 0.33 | 1.02 (0.97−1.07) |
| Yes | 1.00 (ref.) | 1.04 (0.90−1.19) | 1.04 (0.89−1.21) | 1.07 (0.91−1.26) | 1.07 (0.90−1.26) | 0.40 | 1.00 (0.98−1.03) | |
| Women | No | 1.00 (ref.) | 1.18 (1.08−1.28) | 1.22 (1.11−1.33) | 1.25 (1.14−1.38) | 1.31 (1.18−1.45) | <0.0001 | 1.03 (1.02−1.05) |
| Yes | 1.00 (ref.) | 0.69 (0.41−1.16) | 1.11 (0.69−1.80) | 1.06 (0.63−1.78) | 1.16 (0.68−1.98) | 0.23 | 1.05 (0.96−1.15) | |
| Low HDL-C | ||||||||
| Men | No | 1.00 (ref.) | 1.13 (0.78−1.63) | 0.79 (0.52−1.19) | 1.03 (0.67−1.58) | 1.08 (0.69−1.70) | 0.90 | 0.99 (0.92−1.07) |
| Yes | 1.00 (ref.) | 1.30 (1.03−1.65) | 1.30 (1.02−1.67) | 1.48 (1.14−1.91) | 1.83 (1.41−2.38) | <0.0001 | 1.09 (1.05−1.14) | |
| Women | No | 1.00 (ref.) | 1.18 (1.04−1.34) | 1.27 (1.11−1.46) | 1.37 (1.18−1.58) | 1.62 (1.39−1.88) | <0.0001 | 1.09 (1.06−1.12) |
| Yes | 1.00 (ref.) | 0.86 (0.42−1.79) | 0.84 (0.37−1.89) | 1.47 (0.67−3.22) | 2.66 (1.20−5.90) | 0.005 | 1.20 (1.05−1.36) | |
| High glucose | ||||||||
| Men | No | 1.00 (ref.) | 1.20 (1.00−1.44) | 1.18 (0.97−1.42) | 1.17 (0.95−1.44) | 1.20 (0.96−1.49) | 0.21 | 1.01 (0.97−1.05) |
| Yes | 1.00 (ref.) | 1.03 (0.92−1.15) | 1.05 (0.93−1.19) | 1.04 (0.92−1.18) | 0.94 (0.83−1.08) | 0.43 | 0.99 (0.96−1.01) | |
| Women | No | 1.00 (ref.) | 1.11 (1.03−1.21) | 1.19 (1.09−1.29) | 1.22 (1.11−1.34) | 1.29 (1.18−1.42) | <0.0001 | 1.04 (1.02−1.06) |
| Yes | 1.00 (ref.) | 0.81 (0.51−1.28) | 0.68 (0.41−1.14) | 0.98 (0.60−1.62) | 1.28 (0.79−2.08) | 0.10 | 1.03 (0.95−1.12) | |
| High blood pressure | ||||||||
| Men | No | 1.00 (ref.) | 1.30 (1.06−1.59) | 1.19 (0.96−1.48) | 1.18 (0.94−1.49) | 1.27 (0.99−1.61) | 0.23 | 1.03 (0.98−1.07) |
| Yes | 1.00 (ref.) | 1.11 (0.98−1.27) | 1.11 (0.97−1.27) | 1.15 (1.00−1.33) | 1.12 (0.96−1.29) | 0.17 | 1.01 (0.99−1.04) | |
| Women | No | 1.00 (ref.) | 1.07 (0.99−1.17) | 1.13 (1.04−1.23) | 1.11 (1.01−1.22) | 1.26 (1.15−1.39) | <0.0001 | 1.03 (1.01−1.05) |
| Yes | 1.00 (ref.) | 0.91 (0.45−1.83) | 1.82 (0.97−3.40) | 1.96 (1.01−3.82) | 2.71 (1.41−5.18) | 0.0002 | 1.18 (1.06−1.30) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, I.; Kwon, M.; Shivappa, N.; R. Hébert, J.; Kim, M.K. Proinflammatory Dietary Intake is Associated with Increased Risk of Metabolic Syndrome and Its Components: Results from the Population-Based Prospective Study. Nutrients 2020, 12, 1196. https://doi.org/10.3390/nu12041196
Khan I, Kwon M, Shivappa N, R. Hébert J, Kim MK. Proinflammatory Dietary Intake is Associated with Increased Risk of Metabolic Syndrome and Its Components: Results from the Population-Based Prospective Study. Nutrients. 2020; 12(4):1196. https://doi.org/10.3390/nu12041196
Chicago/Turabian StyleKhan, Imran, Minji Kwon, Nitin Shivappa, James R. Hébert, and Mi Kyung Kim. 2020. "Proinflammatory Dietary Intake is Associated with Increased Risk of Metabolic Syndrome and Its Components: Results from the Population-Based Prospective Study" Nutrients 12, no. 4: 1196. https://doi.org/10.3390/nu12041196
APA StyleKhan, I., Kwon, M., Shivappa, N., R. Hébert, J., & Kim, M. K. (2020). Proinflammatory Dietary Intake is Associated with Increased Risk of Metabolic Syndrome and Its Components: Results from the Population-Based Prospective Study. Nutrients, 12(4), 1196. https://doi.org/10.3390/nu12041196