Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
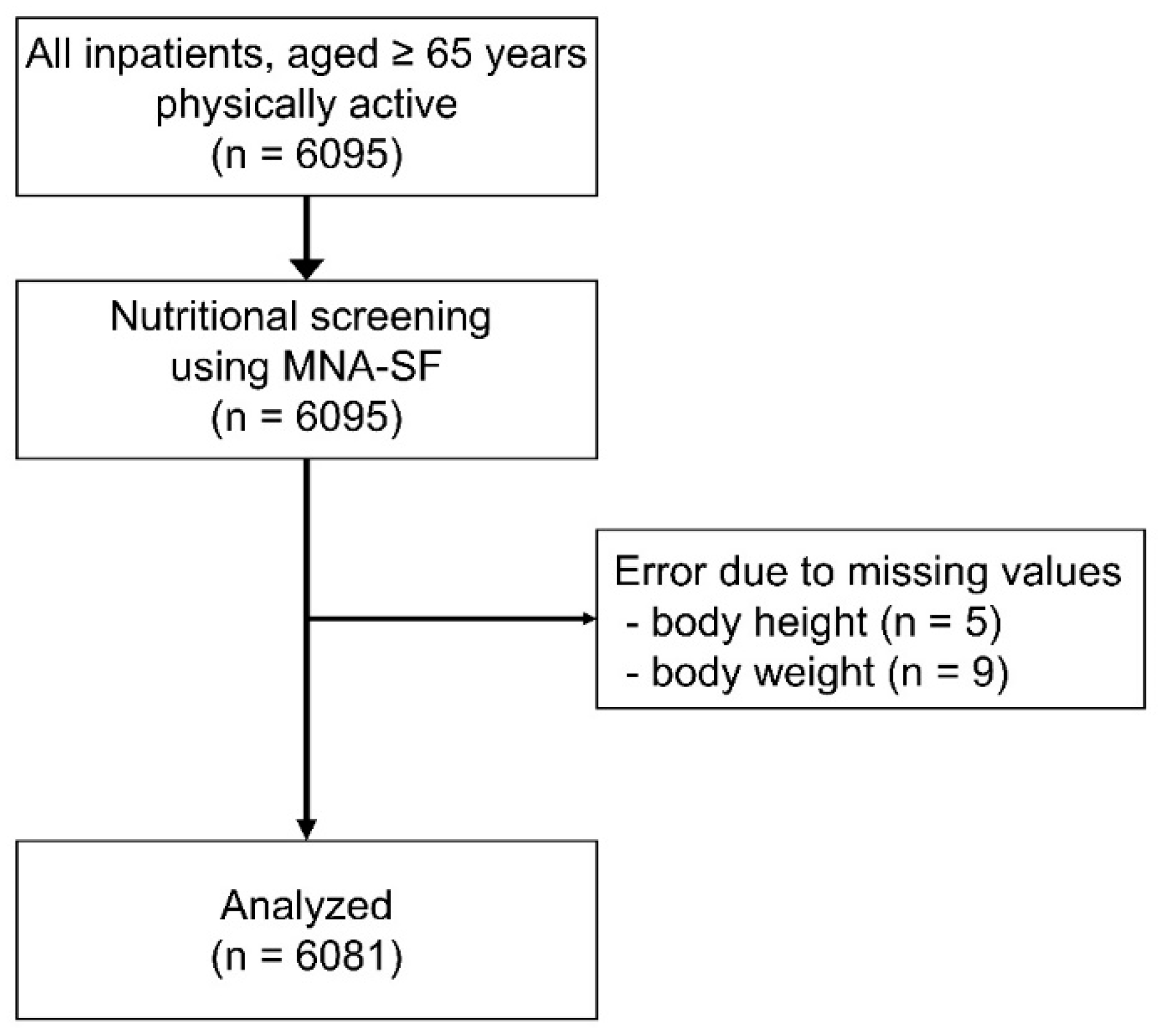
2.1. Study Design and Participants
2.2. Fall Detection
2.3. Baseline Parameters
2.4. Diagnosis of Malnutrition
2.5. Sample Size Calculation
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef] [PubMed]
- Pfortmueller, C.A.; Lindner, G.; Exadaktylos, A.K. Reducing fall risk in the elderly: Risk factors and fall prevention, a systematic review. Minerva Med. 2014, 105, 275–281. [Google Scholar] [PubMed]
- Hendrich, A.; Nyhuis, A.; Kippenbrock, T.; Soja, M.E. Hospital falls: Development of a predictive model for clinical practice. Appl. Nurs. Res. 1995, 8, 129–139. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Josephson, K.R. The epidemiology of falls and syncope. Clin. Geriatr Med. 2002, 18, 141–158. [Google Scholar] [CrossRef]
- Tanaka, S.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Maekawa, E.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; Masuda, T.; et al. Utility of SARC-F for Assessing Physical Function in Elderly Patients With Cardiovascular Disease. J. Am. Med. Dir. Assoc. 2017, 18, 176–181. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, in press. [Google Scholar] [CrossRef]
- Brown, C.J.; Redden, D.T.; Flood, K.L.; Allman, R.M. The underrecognized epidemic of low mobility during hospitalization of older adults. J. Am. Geriatr Soc. 2009, 57, 1660–1665. [Google Scholar] [CrossRef]
- Frenkel, W.J.; Jongerius, E.J.; Mandjes-van Uitert, M.J.; van Munster, B.C.; de Rooij, S.E. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: A prospective cohort study. J. Am. Geriatr Soc. 2014, 62, 342–346. [Google Scholar] [CrossRef]
- Lim, S.L.; Ong, K.C.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef]
- Maeda, K.; Koga, T.; Akagi, J. Nutritional variables predict chances of returning home and activities of daily living in post-acute geriatric care. Clin. Interv. Aging 2018, 13, 151–157. [Google Scholar] [CrossRef]
- Maeda, K.; Ishida, Y.; Nonogaki, T.; Mori, N. Reference body mass index values and the prevalence of malnutrition according to the Global Leadership Initiative on Malnutrition criteria. Clin. Nutr. 2020, 39, 180–184. [Google Scholar] [CrossRef]
- Jensen, G.L.; Wheeler, D. A new approach to defining and diagnosing malnutrition in adult critical illness. Curr. Opin. Crit. Care 2012, 18, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.H.; Sun, S.; Walls, R.C. Protein-energy undernutrition among elderly hospitalized patients: A prospective study. JAMA 1999, 281, 2013–2019. [Google Scholar] [CrossRef]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Reijnierse, E.M.; Verlaan, S.; Pham, V.K.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Lower Skeletal Muscle Mass at Admission Independently Predicts Falls and Mortality 3 Months Post-discharge in Hospitalized Older Patients. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, C.; Crippa, A.; Ek, S.; Welmer, A.K.; Sergi, G.; Maggi, S.; Manzato, E.; Bea, J.W.; Cauley, J.A.; Decullier, E.; et al. Nutritional Status, Body Mass Index, and the Risk of Falls in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 569–582. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salva, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Ix, J.H.; Wassel, C.L.; Stevens, L.A.; Beck, G.J.; Froissart, M.; Navis, G.; Rodby, R.; Torres, V.E.; Zhang, Y.L.; Greene, T.; et al. Equations to estimate creatinine excretion rate: The CKD epidemiology collaboration. Clin. J. Am. Soc. Nephrol. 2011, 6, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Jassal, S.K.; Wassel, C.L.; Laughlin, G.A.; Barrett-Connor, E.; Rifkin, D.E.; Ix, J.H. Urine creatinine-based estimates of fat-free mass in community-dwelling older persons: The Rancho Bernardo study. J. Ren. Nutr. 2015, 25, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Maeda, K.; Nonogaki, T.; Shimizu, A.; Yamanaka, Y.; Matsuyama, R.; Kato, R.; Mori, N. Impact of edema on length of calf circumference in older adults. Geriatr. Gerontol. Int. 2019, 19, 993–998. [Google Scholar] [CrossRef]
- Koh, S.S.; Manias, E.; Hutchinson, A.M.; Johnston, L. Fall incidence and fall prevention practices at acute care hospitals in Singapore: A retrospective audit. J. Eval. Clin. Pract. 2007, 13, 722–727. [Google Scholar] [CrossRef]
- Tsai, A.C.; Lai, M.Y. Mini Nutritional Assessment and short-form Mini Nutritional Assessment can predict the future risk of falling in older adults - results of a national cohort study. Clin. Nutr. 2014, 33, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Lackoff, A.S.; Hickling, D.; Collins, P.F.; Stevenson, K.J.; Nowicki, T.A.; Bell, J.J. The association of malnutrition with falls and harm from falls in hospital inpatients: Findings from a 5-year observational study. J. Clin. Nurs. 2020, 29, 429–436. [Google Scholar] [CrossRef]
- Eglseer, D.; Hoedl, M.; Schoberer, D. Malnutrition risk and hospital-acquired falls in older adults: A cross-sectional, multicenter study. Geriatr. Gerontol. Int. 2020, in press. [Google Scholar] [CrossRef]
- Sillner, A.Y.; Holle, C.L.; Rudolph, J.L. The Overlap Between Falls and Delirium in Hospitalized Older Adults: A Systematic Review. Clin. Geriatr. Med. 2019, 35, 221–236. [Google Scholar] [CrossRef]
- Inouye, S.K.; Schlesinger, M.J.; Lydon, T.J. Delirium: A symptom of how hospital care is failing older persons and a window to improve quality of hospital care. Am. J. Med. 1999, 106, 565–573. [Google Scholar] [CrossRef]
- Krumholz, H.M. Post-hospital syndrome—An acquired, transient condition of generalized risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef]
- Coker, R.H.; Wolfe, R.R. Bedrest and sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, D.; Marco, E.; Ronquillo-Moreno, N.; Miralles, R.; Vazquez-Ibar, O.; Escalada, F.; Muniesa, J.M. Prevalence of malnutrition and sarcopenia in a post-acute care geriatric unit: Applying the new ESPEN definition and EWGSOP criteria. Clin. Nutr. 2017, 36, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Hartley, P.; Costello, P.; Fenner, R.; Gibbins, N.; Quinn, E.; Kuhn, I.; Keevil, V.L.; Romero-Ortuno, R. Change in skeletal muscle associated with unplanned hospital admissions in adult patients: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210186. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Plati, C.; Lanara, V.; Mantas, J. Risk factors responsible for patients’ falls. Scand. J. Caring Sci. 1992, 6, 113–118. [Google Scholar] [CrossRef]
- Church, S.; Robinson, T.N.; Angles, E.M.; Tran, Z.V.; Wallace, J.I. Postoperative falls in the acute hospital setting: Characteristics, risk factors, and outcomes in males. Am. J. Surg. 2011, 201, 197–202. [Google Scholar] [CrossRef]
- Zhao, Y.L.; Alderden, J.; Lind, B.; Stibrany, J. Risk factors for falls in homebound community-dwelling older adults. Public Health Nurs. 2019, 36, 772–778. [Google Scholar] [CrossRef]
- Peng, K.; Tian, M.; Andersen, M.; Zhang, J.; Liu, Y.; Wang, Q.; Lindley, R.; Ivers, R. Incidence, risk factors and economic burden of fall-related injuries in older Chinese people: A systematic review. Inj. Prev. 2019, 25, 4–12. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Ciol, M.A.; Hoffman, J.; Dudgeon, B.J.; Yorkston, K.; Chan, L. Falls in the Medicare population: Incidence, associated factors, and impact on health care. Phys. Ther. 2009, 89, 324–332. [Google Scholar] [CrossRef]
- Seppala, L.J.; van de Glind, E.M.M.; Daams, J.G.; Ploegmakers, K.J.; de Vries, M.; Wermelink, A.; van der Velde, N.; Task, E.; Finish Group on Fall-Risk-Increasing, D. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-analysis: III. Others. J. Am. Med. Dir. Assoc. 2018, 19, 372.e1–372.e8. [Google Scholar] [CrossRef]
- Kropelin, T.F.; Neyens, J.C.; Halfens, R.J.; Kempen, G.I.; Hamers, J.P. Fall determinants in older long-term care residents with dementia: A systematic review. Int. Psychogeriatr. 2013, 25, 549–563. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 6081) | Malnutrition (n = 668) | Non-Malnutrition (n = 5413) | p-Value | |
|---|---|---|---|---|
| Age, year | 74.4 ± 6.1 | 75.3 ± 6.4 | 74.3 ± 6.0 | <0.001 a |
| Sex, n (%) | ||||
| Male | 3535 (58.1) | 296 (44.3) | 3239 (59.8) | <0.001 b |
| Female | 2546 (41.9) | 372 (55.7) | 2174 (40.2) | |
| Height (cm) | ||||
| Male | 165.1 ± 6.0 | 164.7 ± 6.1 | 165.2 ± 6.0 | 0.165 a |
| Female | 151.8 ± 5.7 | 152.5 ± 6.0 | 151.7 ± 5.7 | 0.008 a |
| Weight (kg) | ||||
| Male | 62.5 ± 10.0 | 47.9 ± 5.8 | 63.8 ± 9.2 | <0.001 a |
| Female | 51.8 ± 9.2 | 40.8 ± 4.7 | 53.6 ± 8.4 | <0.001 a |
| Body mass index (kg/m2) | ||||
| Male | 22.9 ± 3.2 | 17.7 ± 1.7 | 23.4 ± 2.8 | <0.001 a |
| Female | 22.5 ± 3.6 | 17.5 ± 1.6 | 23.3 ± 3.2 | <0.001 a |
| FFMI (kg/m2) | ||||
| Male | 18.0 ± 1.4 | 16.0 ± 1.0 | 18.2 ± 1.3 | <0.001 a |
| Female | 14.6 ± 1.5 | 12.7 ± 0.8 | 14.9 ± 1.4 | <0.001 a |
| Charlson Comorbidity Index, score | 2.3 ± 2.8 | 3.0 ± 3.2 | 2.2 ± 2.7 | <0.001 a |
| MNA-SF, score | 13 (11–14) | 11 (9–11) | 13 (12–14) | <0.001 c |
| 12–14, n (%) | 4,531 (74.5) | 0 (0.0) | 4,531 (83.7) | <0.001 b |
| 8–11, n (%) | 1,483 (24.4) | 620 (92.8) | 863 (15.9) | |
| 0–7, n (%) | 67 (1.1) | 48 (7.2) | 19 (0.4) | |
| Any recent weight loss, n (%) | 808 (13.3) | 223 (33.4) | 585 (10.8) | <0.001 b |
| Weight loss > 5%, n (%) | 205 (3.4) | 145 (21.7) | 60 (1.1) | <0.001 b |
| Overall (n = 6208) | Malnutrition (n = 682) | Non-Malnutrition (n = 5526) | p-Value | |
|---|---|---|---|---|
| Incidence of a fall | ||||
| Yes (%) | 55 (0.9) | 16 (2.4) | 39 (0.7) | <0.001 |
| No (%) | 6026 (99.1) | 652 (97.6) | 5374 (99.3) |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.05 | 1.01–1.09 | 0.013 | 1.05 | 1.01–1.09 | 0.022 |
| Sex (male) | 2.53 | 1.33–4.80 | <0.001 | 2.50 | 1.31–4.79 | 0.006 |
| Charlson Comorbidity Index * | 1.11 | 1.03–1.20 | 0.005 | 1.14 | 1.04–1.25 | 0.004 |
| Disease | ||||||
| Neoplasms | 0.33 | 0.10–1.12 | 0.075 | 0.61 | 0.34–1.10 | 0.101 |
| Diseases of the eye and adnexa | 0.16 | 0.02–1.64 | 0.124 | |||
| Diseases of the digestive system | 0.38 | 0.09–1.64 | 0.194 | |||
| Diseases of the circulatory system | 0.49 | 0.14–1.74 | 0.270 | |||
| Diseases of the genitourinary system | 0.44 | 0.07–2.71 | 0.379 | |||
| Diseases of the nervous system | 0.00 | 0.00–Inf. | 0.980 | |||
| Diseases of the respiratory system | 0.56 | 0.13–2.53 | 0.453 | |||
| Diseases of the musculoskeletal system and connective tissue | 0.10 | 0.01–0.94 | 0.044 | 0.40 | 0.05–2.97 | 0.371 |
| Injury, poisoning, and certain other consequences of external causes | 0.00 | 0.00–Inf. | 0.968 | |||
| Endocrine, nutritional, and metabolic diseases | 0.30 | 0.05–1.83 | 0.192 | |||
| Diseases of the ear and mastoid process | 0.60 | 0.06–5.86 | 0.659 | |||
| Certain infectious and parasitic diseases | 1.00 | reference | 0.758 | |||
| Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism | 0.44 | 0.05–4.22 | 0.475 | |||
| Diseases of the skin and subcutaneous tissue | 1.31 | 0.14–12.70 | 0.814 | |||
| Mental and behavioral disorders | 1.07 | 0.22–5.32 | 0.934 | |||
| Others | 0.00 | 0.00–Inf. | 0.990 | |||
| Malnutrition | 2.67 | 1.49–4.77 | <0.001 | 2.78 | 1.51–5.00 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishida, Y.; Maeda, K.; Nonogaki, T.; Shimizu, A.; Yamanaka, Y.; Matsuyama, R.; Kato, R.; Mori, N. Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults. Nutrients 2020, 12, 541. https://doi.org/10.3390/nu12020541
Ishida Y, Maeda K, Nonogaki T, Shimizu A, Yamanaka Y, Matsuyama R, Kato R, Mori N. Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults. Nutrients. 2020; 12(2):541. https://doi.org/10.3390/nu12020541
Chicago/Turabian StyleIshida, Yuria, Keisuke Maeda, Tomoyuki Nonogaki, Akio Shimizu, Yosuke Yamanaka, Remi Matsuyama, Ryoko Kato, and Naoharu Mori. 2020. "Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults" Nutrients 12, no. 2: 541. https://doi.org/10.3390/nu12020541
APA StyleIshida, Y., Maeda, K., Nonogaki, T., Shimizu, A., Yamanaka, Y., Matsuyama, R., Kato, R., & Mori, N. (2020). Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults. Nutrients, 12(2), 541. https://doi.org/10.3390/nu12020541