Caffeine Consumption in Switzerland: Results from the First National Nutrition Survey MenuCH



Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Dietary Assessment
2.3. Estimated Caffeine Content (Most Foods)
2.4. Measured Caffeine Content (Coffee and Soft Drinks)
2.5. Anthropometry and Other Parameters
2.6. Statistical Analyses
3. Results
4. Discussion
4.1. Total Daily Caffeine Intake
4.2. Differences Across Population Subgroups
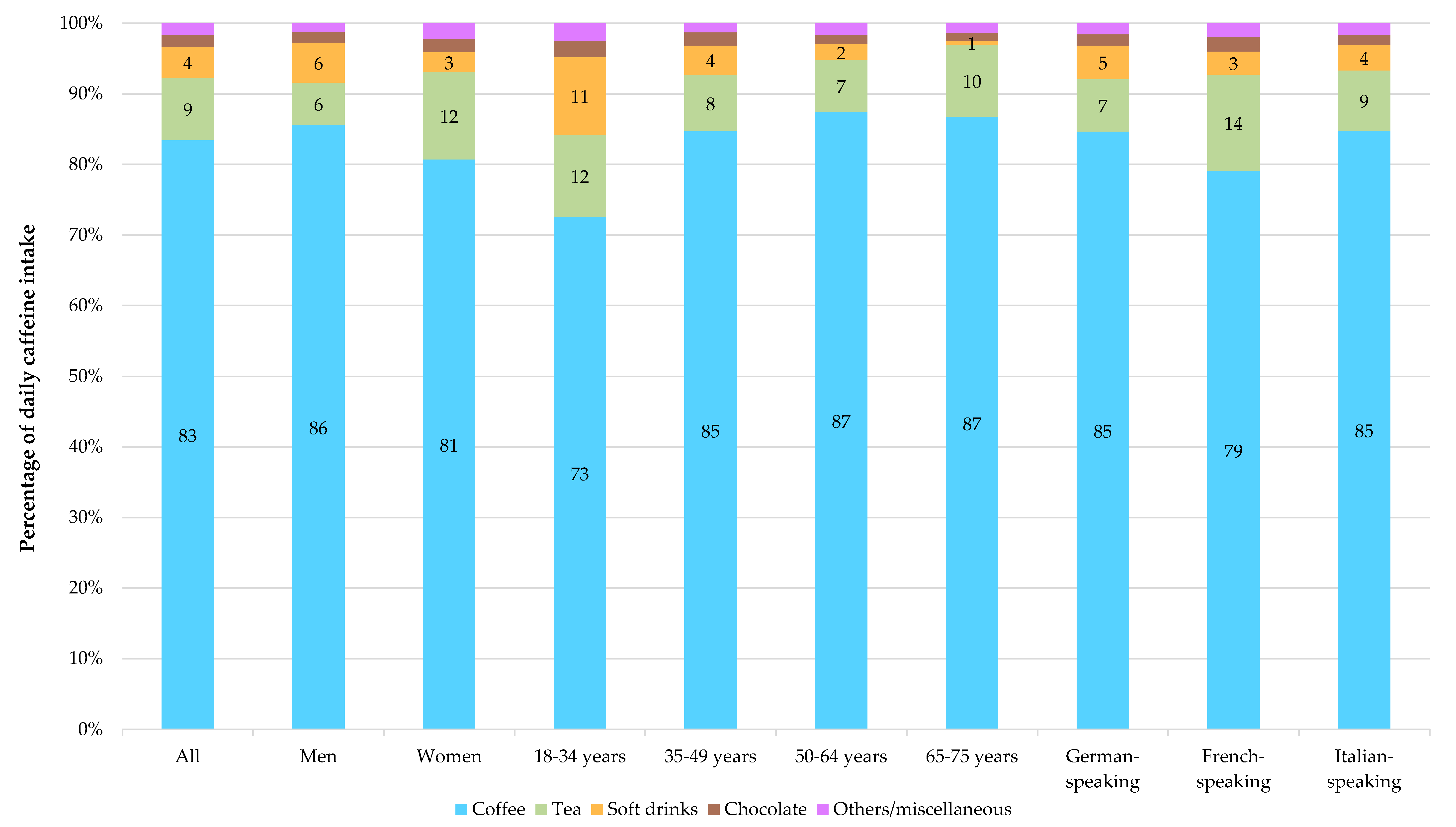
4.3. Main Sources of Caffeine
4.4. Timing of Caffeine Consumption
4.5. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nawrot, P.; Jordan, S.; Eastwood, J.; Rotstein, J.; Hugenholtz, A.; Feeley, M. Effects of caffeine on human health. Food Addit. Contam. 2003, 20, 1–30. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products. Nutrition and Allergies (NDA) Scientific Opinion on the safety of caffeine. EFSA J. 2015, 13, 4120. [Google Scholar]
- Heckman, M.A.; Weil, J.; De Mejia, E.G. Caffeine (1, 3, 7-trimethylxanthine) in Foods: A Comprehensive Review on Consumption, Functionality, Safety, and Regulatory Matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef]
- Higdon, J.V.; Frei, B. Coffee and Health: A Review of Recent Human Research. Crit. Rev. Food Sci. Nutr. 2006, 46, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37, 131–156. [Google Scholar] [CrossRef]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109, 585–648. [Google Scholar] [CrossRef]
- Lieberman, H.R.; Agarwal, S.; Fulgoni, V.L. Daily Patterns of Caffeine Intake and the Association of Intake with Multiple Sociodemographic and Lifestyle Factors in US Adults Based on the NHANES 2007–2012 Surveys. J. Acad. Nutr. Diet. 2019, 119, 106–114. [Google Scholar] [CrossRef]
- O’Callaghan, F.; Muurlink, O.; Reid, N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag. Healthc. Policy 2018, 11, 263–271. [Google Scholar] [CrossRef]
- Noordzij, M.; Uiterwaal, C.S.; Arends, L.R.; Kok, F.J.; Grobbee, D.E.; Geleijnse, J.M. Blood pressure response to chronic intake of coffee and caffeine: A meta-analysis of randomized controlled trials. J. Hypertens. 2005, 23, 921–928. [Google Scholar] [CrossRef]
- Turnbull, D.; Rodricks, J.V.; Mariano, G.F.; Chowdhury, F. Caffeine and cardiovascular health. Regul. Toxicol. Pharmacol. 2017, 89, 165–185. [Google Scholar] [CrossRef]
- Benson, S.M.; Unice, K.M.; Glynn, M.E. Hourly and daily intake patterns among U.S. caffeinated beverage consumers based on the National Health and Nutrition Examination Survey (NHANES, 2013–2016). Food Chem. Toxicol. 2019, 125, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L.; Keast, D.R.; Lieberman, H.R. Trends in intake and sources of caffeine in the diets of US adults: 2001–2010. Am. J. Clin. Nutr. 2015, 101, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Koenig, J. Caffeine intake and its sources: A review of national representative studies. Crit. Rev. Food Sci. Nutr. 2018, 58, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Martyn, D.; Lau, A.; Richardson, P.; Roberts, A. Temporal patterns of caffeine intake in the United States. Food Chem. Toxicol. 2018, 111, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future life expectancy in 35 industrialised countries: Projections with a Bayesian model ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major Differences in Diet across Three Linguistic Regions of Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2017, 9, 1163. [Google Scholar] [CrossRef]
- Petrovic, D.; Estoppey Younes, S.; Pruijm, M.; Ponte, B.; Ackermann, D.; Ehret, G.; Ansermot, N.; Mohaupt, M.; Paccaud, F.; Vogt, B.; et al. Relation of 24-h urinary caffeine and caffeine metabolite excretions with self-reported consumption of coffee and other caffeinated beverages in the general population. Nutr. Metab. 2016, 13, 81. [Google Scholar] [CrossRef]
- Federal Statistical Office. Stichprobenrahmen für Personen- und Haushaltserhebungen (Swiss persons and households registry). Available online: https://www.bfs.admin.ch/bfs/de/home/grundlagen/volkszaehlung/volkszaehlung-teil-gesamtsystem/stichprobenrahmen.html (accessed on 16 October 2019).
- Chatelan, A.; Gaillard, P.; Kruseman, M.; Keller, A. Total, Added, and Free Sugar Consumption and Adherence to Guidelines in Switzerland: Results from the First National Nutrition Survey menuCH. Nutrients 2019, 11, 1117. [Google Scholar] [CrossRef]
- Chatelan, A.; Marques-Vidal, P.; Bucher, S.; Siegenthaler, S.; Metzger, N.; Zuberbühler, C.A.; Camenzind-Frey, E.; Reggli, A.; Bochud, M.; Beer-Borst, S. Lessons Learnt About Conducting a Multilingual Nutrition Survey in Switzerland: Results from menuCH Pilot Survey. Int. J. Vitam. Nutr. Res. 2017, 87, 25–36. [Google Scholar] [CrossRef]
- Camenzind-Frey, E.; Zuberbuehler, C.A. menuCH-Schweizerisches Fotobuch/Livre Photo Suisse/Manuale Fotografico Svizzero (menuCH Picture Book); Federal Office of Public Health & Federal Food Safety and Veterinary Office: Berne, Switzerland, 2014.
- Mitchell, D.C.; Knight, C.A.; Hockenberry, J.; Teplansky, R.; Hartman, T.J. Beverage caffeine intakes in the U.S. Food Chem. Toxicol. 2014, 63, 136–142. [Google Scholar] [CrossRef]
- Federal Food Safety and Veterinary Office. Swiss food composition database. Available online: https://www.naehrwertdaten.ch/en/ (accessed on 6 June 2019).
- Sereshti, H.; Samadi, S. A rapid and simple determination of caffeine in teas, coffees and eight beverages. Food Chem. 2014, 158, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Vin, K.; Beziat, J.; Seper, K.; Wolf, A.; Sidor, A.; Chereches, R.; Luc Volatier, J.; Ménard, C. Nutritional composition of the food supply: A comparison of soft drinks and breakfast cereals between three European countries based on labels. Eur. J. Clin. Nutr. 2019, 1. [Google Scholar] [CrossRef] [PubMed]
- McCusker, R.R.; Fuehrlein, B.; Goldberger, B.A.; Gold, M.S.; Cone, E.J. Caffeine Content of Decaffeinated Coffee. J. Anal. Toxicol. 2006, 30, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Center for the Promotion of Imports, Ministry of Foreign Affairs. Through what channels can you get coffee onto the European market? Available online: https://www.cbi.eu/market-information/coffee/channels-segments (accessed on 6 June 2019).
- World Health Organization MONICA Manual, Part III: Population Survey. Section 1: Population Survey Data Component. 4.6 Height, Weight, Waist and Hip Measurement. Available online: http://www.thl.fi/ publications/monica/manual/part3/iii-1.htm#s4-6 (accessed on 1 July 2017).
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H.; Consortium, E. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, S87–S91. [Google Scholar] [CrossRef]
- Fitt, E.; Pell, D.; Cole, D. Assessing caffeine intake in the United Kingdom diet. Food Chem. 2013, 140, 421–426. [Google Scholar] [CrossRef]
- Drewnowski, A.; Rehm Colin, D. Sources of Caffeine in Diets of US Children and Adults: Trends by Beverage Type and Purchase Location. Nutrients 2016, 8, 154. [Google Scholar] [CrossRef]
- Treur, J.L.; Taylor, A.E.; Ware, J.J.; McMahon, G.; Hottenga, J.-J.; Baselmans, B.M.L.; Willemsen, G.; Boomsma, D.I.; Munafò, M.R.; Vink, J.M. Associations between smoking and caffeine consumption in two European cohorts: Smoking and caffeine consumption. Addiction 2016, 111, 1059–1068. [Google Scholar] [CrossRef]
- Grela, A.; Kulza, M.; Piekoszewsi, W.; Senczuk-Przybylowska, M.; Gomolka, E.; Florek, E. The effects of tobacco smoke exposure on caffeine metabolism. Ital. J. Food Sci. 2013, 25, 76–82. [Google Scholar]
- Treur, J.L.; Taylor, A.E.; Ware, J.J.; Nivard, M.G.; Neale, M.C.; McMahon, G.; Hottenga, J.-J.; Baselmans, B.M.L.; Boomsma, D.I.; Munafò, M.R.; et al. Smoking and caffeine consumption: A genetic analysis of their association: Smoking and caffeine. Addict. Biol. 2017, 22, 1090–1102. [Google Scholar] [CrossRef]
- Hettema, J.M.; Corey, L.A.; Kendler, K.S. A multivariate genetic analysis of the use of tobacco, alcohol, and caffeine in a population based sample of male and female twins. Drug Alcohol Depend. 1999, 57, 69–78. [Google Scholar] [CrossRef]
- Rudolph, E.; Faerbinger, A.; Koenig, J. Caffeine intake from all sources in adolescents and young adults in Austria. Eur. J. Clin. Nutr. 2014, 68, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Vercammen, K.A.; Koma, J.W.; Li, Z. Trends in Beverage Consumption Among Children and Adults, 2003-2014: Trends in Beverage Consumption. Obesity 2018, 26, 432–441. [Google Scholar] [CrossRef]
- Hečimović, I.; Belščak-Cvitanović, A.; Horžić, D.; Komes, D. Comparative study of polyphenols and caffeine in different coffee varieties affected by the degree of roasting. Food Chem. 2011, 129, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- McCusker, R.R.; Goldberger, B.A.; Cone, E.J. Caffeine Content of Specialty Coffees. J. Anal. Toxicol. 2003, 27, 520–522. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Population Characteristics | n | Weighted n | Weighted % | Weighted Mean | SD | Weighted P5 | Weighted P25 | Weighted Median | Weighted P75 | Weighted P95 | >400 mg % | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Entire population | 2057 | 4,627,878 | 100% | 191 | 129 | 29 | 96 | 169 | 260 | 426 | 6.6% |
| Sex | Men | 933 | 2,305,141 | 50% | 210 | 138 | 32 | 108 | 189 | 284 | 445 | 8.8% |
| Women | 1124 | 2,322,737 | 50% | 172 | 117 | 27 | 86 | 155 | 229 | 388 | 4.5% | |
| Age group | 18–34 years | 563 | 1,306,178 | 28% | 140 | 111 | 20 | 58 | 113 | 186 | 359 | 2.4% |
| 35–49 years | 602 | 1,421,756 | 31% | 202 | 134 | 30 | 104 | 175 | 272 | 468 | 8.8% | |
| 50–64 years | 554 | 1,250,918 | 27% | 228 | 135 | 62 | 134 | 207 | 294 | 451 | 9.4% | |
| 65–75 years | 338 | 649,026 | 14% | 202 | 111 | 43 | 125 | 193 | 262 | 406 | 5.2% | |
| Language region | German-speaking | 1341 | 3,183,216 | 69% | 204 | 136 | 30 | 104 | 182 | 277 | 445 | 7.9% |
| French-speaking | 502 | 1,187,738 | 26% | 170 | 112 | 29 | 86 | 148 | 232 | 399 | 4.8% | |
| Italian-speaking | 214 | 256,925 | 6% | 136 | 85 | 22 | 71 | 126 | 193 | 270 | 0.3% | |
| Nationality | Swiss | 1789 | 3,470,404 | 75% | 191 | 128 | 28 | 102 | 172 | 257 | 416 | 6.0% |
| Not Swiss | 265 | 1,145,199 | 25% | 192 | 133 | 31 | 84 | 164 | 266 | 445 | 8.6% | |
| Education | Lower | 286 | 620,712 | 13% | 208 | 156 | 31 | 107 | 175 | 261 | 527 | 8.7% |
| Middle | 771 | 1,589,873 | 34% | 177 | 120 | 28 | 86 | 160 | 243 | 406 | 5.3% | |
| Higher | 997 | 2,405,018 | 52% | 196 | 128 | 29 | 101 | 176 | 267 | 426 | 7.0% | |
| Income | Lower | 486 | 1,128,723 | 24% | 190 | 133 | 27 | 93 | 167 | 249 | 451 | 6.8% |
| Middle | 516 | 1,095,517 | 24% | 188 | 123 | 36 | 100 | 168 | 245 | 401 | 5.1% | |
| Higher | 802 | 1,831,768 | 40% | 195 | 126 | 28 | 101 | 174 | 266 | 415 | 6.2% | |
| No answer | 250 | 559,595 | 12% | 188 | 144 | 15 | 70 | 161 | 262 | 449 | 10.9% | |
| Smoking status | Never smokers | 1072 | 2,307,169 | 50% | 171 | 121 | 22 | 74 | 154 | 240 | 400 | 5.0% |
| Ex-smokers | 530 | 1,271,513 | 27% | 197 | 115 | 38 | 111 | 176 | 268 | 415 | 6.4% | |
| Smokers | 451 | 1,034,578 | 22% | 228 | 152 | 49 | 131 | 199 | 285 | 519 | 10.5% | |
| Weight status | Normal weight | 1166 | 2,625,518 | 57% | 179 | 125 | 25 | 85 | 160 | 243 | 413 | 5.6% |
| Overweight | 629 | 1,422,231 | 31% | 204 | 124 | 43 | 112 | 186 | 269 | 423 | 6.7% | |
| Obesity | 262 | 580,130 | 13% | 217 | 154 | 32 | 101 | 195 | 296 | 506 | 11.2% | |
| Population | n | Weighted n | 12:00–03:00 | 03:00–06:00 | 06:00–09:00 | 09:00–12:00 | 12:00–15:00 | 03:00–06:00 | 06:00–09:00 | 9 p.m.–12 a.m. |
|---|---|---|---|---|---|---|---|---|---|---|
| All | 2057 | 4,627,878 | 0.2 | 2.9 | 29.0 | 26.2 | 15.9 | 13.7 | 8.9 | 3.2 |
| Men | 933 | 2,305,141 | 0.2 | 3.5 | 26.9 | 26.8 | 15.5 | 14.3 | 9.3 | 3.4 |
| Women | 1124 | 2,322,737 | 0.1 | 2.3 | 31.6 | 25.5 | 16.3 | 12.8 | 8.4 | 2.9 |
| 18–34 years | 563 | 1,306,178 | 0.3 | 3.1 | 21.7 | 32.8 | 13.9 | 15.0 | 8.7 | 4.5 |
| 35–49 years | 602 | 1,421,756 | 0.1 | 3.6 | 28.5 | 26.4 | 15.8 | 14.0 | 8.6 | 3.0 |
| 50–64 years | 554 | 1,250,918 | 0.2 | 3.2 | 30.8 | 24.7 | 16.4 | 13.1 | 9.0 | 2.7 |
| 65–75 years | 338 | 649,026 | 0.0 | 0.6 | 37.2 | 19.5 | 17.8 | 12.3 | 9.7 | 2.9 |
| German-speaking | 1341 | 3,183,216 | 0.2 | 3.2 | 27.9 | 27.0 | 15.4 | 14.0 | 9.2 | 3.1 |
| French-speaking | 502 | 1,187,738 | 0.2 | 2.1 | 31.1 | 24.1 | 17.6 | 12.8 | 8.3 | 3.7 |
| Italian-speaking | 214 | 256,925 | 0.0 | 2.8 | 39.8 | 22.0 | 14.5 | 12.2 | 7.2 | 1.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rochat, C.; Eap, C.B.; Bochud, M.; Chatelan, A. Caffeine Consumption in Switzerland: Results from the First National Nutrition Survey MenuCH. Nutrients 2020, 12, 28. https://doi.org/10.3390/nu12010028
Rochat C, Eap CB, Bochud M, Chatelan A. Caffeine Consumption in Switzerland: Results from the First National Nutrition Survey MenuCH. Nutrients. 2020; 12(1):28. https://doi.org/10.3390/nu12010028
Chicago/Turabian StyleRochat, Christèle, Chin B. Eap, Murielle Bochud, and Angeline Chatelan. 2020. "Caffeine Consumption in Switzerland: Results from the First National Nutrition Survey MenuCH" Nutrients 12, no. 1: 28. https://doi.org/10.3390/nu12010028
APA StyleRochat, C., Eap, C. B., Bochud, M., & Chatelan, A. (2020). Caffeine Consumption in Switzerland: Results from the First National Nutrition Survey MenuCH. Nutrients, 12(1), 28. https://doi.org/10.3390/nu12010028