Snack Consumption Patterns among Canadians

 ,
, 

Abstract
1. Background
2. Subject and Method
2.1. Data Source, Study Design, and Dietary Data Collection
2.2. Analytical Sample
2.3. Snack Consumption
2.4. Daily Nutrients and Food Groups Intake
2.5. Other Variables of Interest
2.6. Statistical Analyses
3. Results
3.1. Prevalence of Snack Consumption
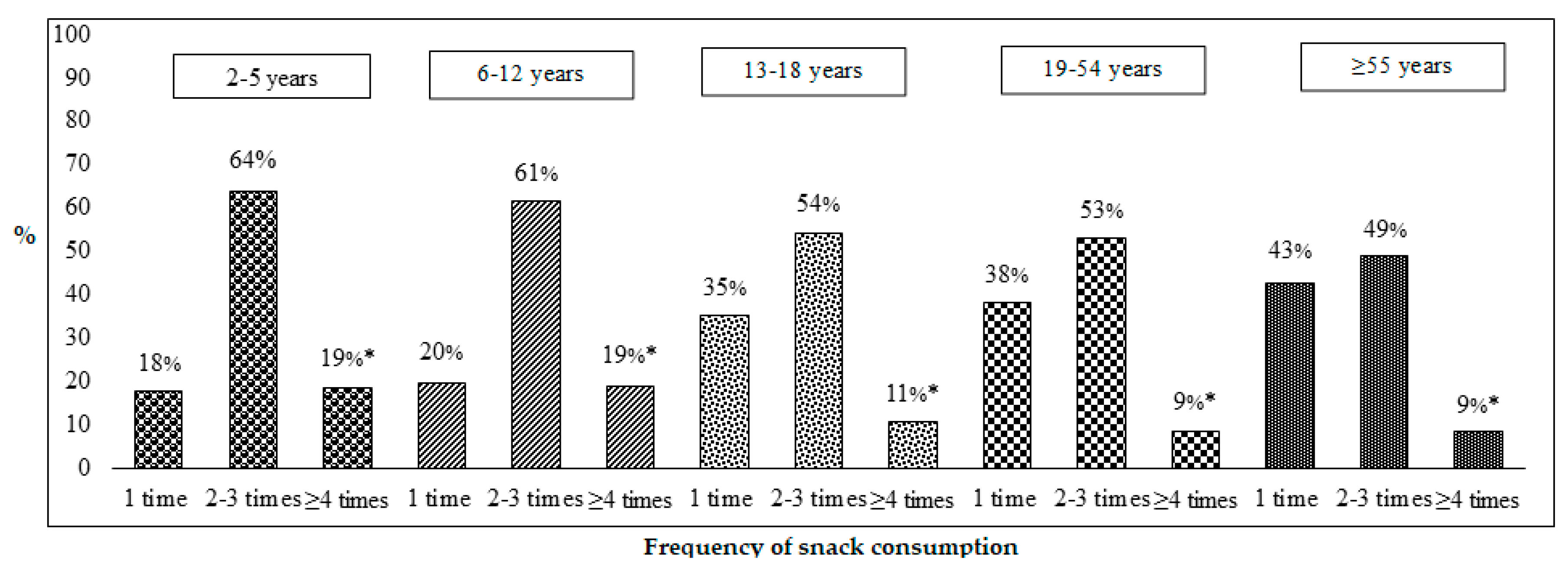
3.2. The Frequency of Snack Consumption among Canadians
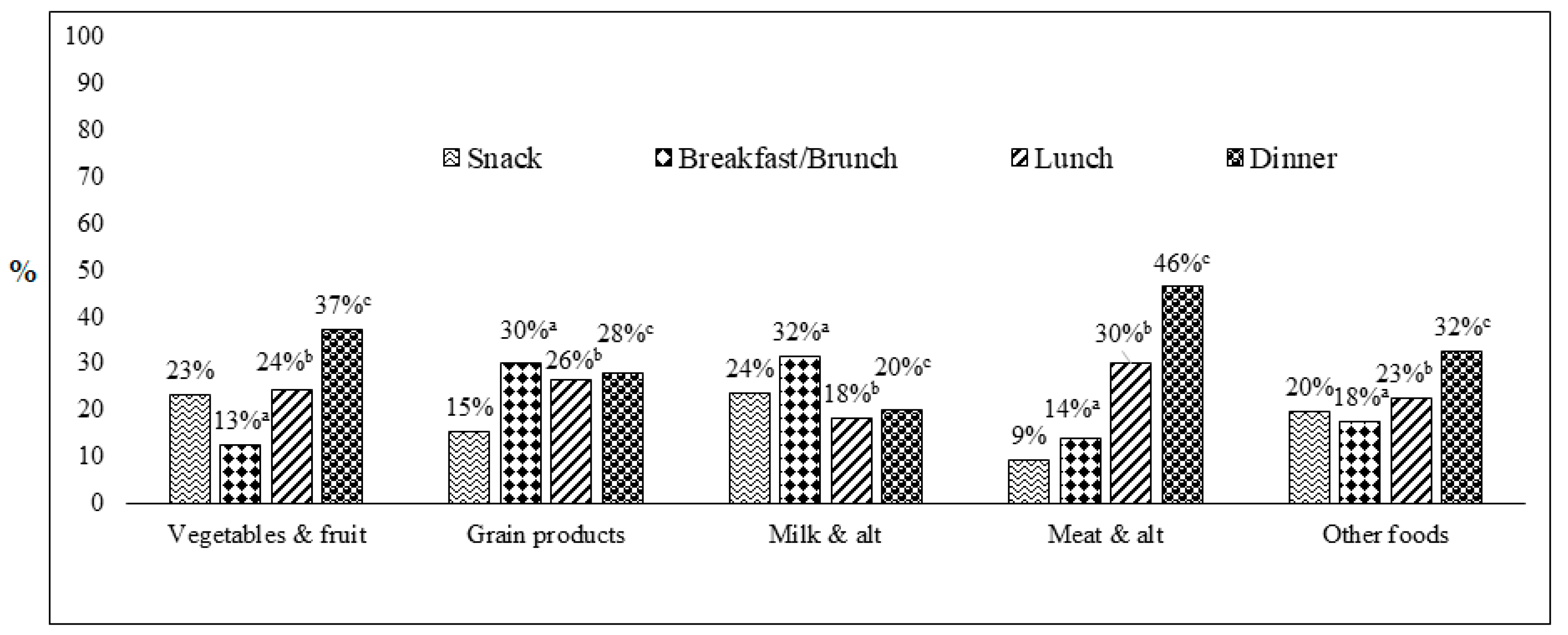
3.3. Distributions of Food Group Consumption across Meal Occasions (Snack, Breakfast/Brunch, Lunch and Dinner)
3.4. Nutrient Contribution (%) of Snack, Breakfast/Brunch, Lunch, and Dinner to Daily Intake
3.5. Energy and Nutrient Contribution of Snack among Five Age Groups
3.6. The Contribution of Grain Subgroups to Total Grain Product Consumed as Snack
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bellisle, F. Meals and snacking, diet quality and energy balance. Physiol. Behav. 2014, 134, 38–43. [Google Scholar] [CrossRef]
- Johnson, G.H.; Anderson, G.H. Snacking definitions: Impact on interpretation of the literature and dietary recommendations. Crit. Rev. Food Sci. Nutr. 2010, 50, 848–871. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B. Associations between meal and snack frequency and diet quality and adiposity measures in British adults: Findings from the National Diet and Nutrition Survey. Public Health Nutr. 2016, 19, 1624–1634. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B. Associations between meal and snack frequency and overweight and abdominal obesity in US children and adolescents from National Health and Nutrition Examination Survey (NHANES) 2003–2012. Br. J. Nutr. 2016, 115, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Na, L.; Han, T.; Zhang, W.; Wu, X.; Na, G.; Du, S.; Sun, C. A Snack Dietary Pattern Increases the Risk of Hypercholesterolemia in Northern Chinese Adults: A Prospective Cohort Study. PLoS ONE 2015, 10, e0134294. [Google Scholar] [CrossRef] [PubMed]
- Barnes, T.L.; French, S.A.; Harnack, L.J.; Mitchell, N.R.; Wolfson, J. Snacking behaviors, diet quality, and body mass index in a community sample of working adults. J. Acad. Nutr. Diet. 2015, 115, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, C.; Siegrist, M.; van der Horst, K. Snack frequency: Associations with healthy and unhealthy food choices. Public Health Nutr. 2013, 16, 1487–1496. [Google Scholar] [CrossRef]
- Maugeri, A.; Kunzova, S.; Medina-Inojosa, J.R.; Agodi, A.; Barchitta, M.; Homolka, M.; Kiacova, N.; Bauerova, H.; Sochor, O.; Lopez-Jimenez, F.; et al. Association between eating time interval and frequency with ideal cardiovascular health: Results from a random sample Czech urban population. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. 40-year trends in meal and snack eating behaviors of American adults. J. Acad. Nutr. Diet. 2015, 115, 50–63. [Google Scholar] [CrossRef]
- Nielsen, S.J.; Siega-Riz, A.M.; Popkin, B.M. Trends in energy intake in U.S. between 1977 and 1996: Similar shifts seen across age groups. Obes. Res. 2002, 10, 370–378. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; Peters, V.; McConnell, A.; Petocz, P.; Eldridge, A.L. Weekday snacking prevalence, frequency, and energy contribution have increased while foods consumed during snacking have shifted among Australian children and adolescents: 1995, 2007 and 2011–12 National Nutrition Surveys. Nutr. J. 2017, 16, 65. [Google Scholar] [CrossRef]
- Kerr, M.A.; Rennie, K.L.; McCaffrey, T.A.; Wallace, J.M.; Hannon-Fletcher, M.P.; Livingstone, M.B. Snacking patterns among adolescents: A comparison of type, frequency and portion size between Britain in 1997 and Northern Ireland in 2005. Br. J. Nutr. 2009, 101, 122–131. [Google Scholar] [CrossRef]
- Piernas, C.; Popkin, B.M. Snacking increased among U.S. adults between 1977 and 2006. J. Nutr. 2010, 140, 325–332. [Google Scholar] [CrossRef]
- Gilbert, J.A.; Miller, D.; Olson, S.; St-Pierre, S. After-school snack intake among Canadian children and adolescents. Can. J. Public Health 2012, 103, e448–e452. [Google Scholar]
- Canadian Community Health Survey (CCHS): Nutrition-2015 (First Interview) (2017). Available online: http://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=assembleInstr&lang=en&Item_Id=202664 (accessed on 5 April 2019).
- Canadian Community Health Survey-Nutrition (CCHS). 2017. Available online: http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5049#a1 (accessed on 5 April 2019).
- Canada Food Guide. Eating Well with Canada Food Guide. 2007. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/hpfb-dgpsa/pdf/food-guide-aliment/print_eatwell_bienmang-eng.pdf (accessed on 5 April 2019).
- Canada’s Food Guide. Government of Canada. 2019. Available online: https://food-guide.canada.ca/en/ (accessed on 5 April 2019).
- World Health Organization. WHO Anthro (Version 3.2.2, January 2011) and Macros. 2011. Available online: https://www.who.int/childgrowth/software/en/) (accessed on 5 April 2019).
- Statistics Canada. The Research Data Centres Information and Technical Bulletin—Weighted Estimation and Bootstrap Variance Estimation for Analyzing Survey Data: How to Implement in Selected Software. 2014. Available online: http://www5.statcan.gc.ca/olc-cel/olc?ObjId=12-002-X201400111901&ObjType=47&lang=en (accessed on 5 April 2019).
- Duffey, K.J.; Pereira, R.A.; Popkin, B.M. Prevalence and energy intake from snacking in Brazil: Analysis of the first nationwide individual survey. Eur. J. Clin. Nutr. 2013, 67, 868–874. [Google Scholar] [CrossRef]
- Dunford, E.K.; Popkin, B.M. 37 year snacking trends for US children 1977–2014. Pediatr. Obes. 2018, 13, 247–255. [Google Scholar] [CrossRef]
- Wang, Z.; Zhai, F.; Zhang, B.; Popkin, B.M. Trends in Chinese snacking behaviors and patterns and the social-demographic role between 1991 and 2009. Asia Pac. J. Clin. Nutr. 2012, 21, 253–262. [Google Scholar]
- Wang, D.; van der Horst, K.; Jacquier, E.; Eldridge, A.L. Snacking Among US Children: Patterns Differ by Time of Day. J. Nutr. Educ. Behav. 2016, 48, 369–375.e361. [Google Scholar] [CrossRef]
- Berteus Forslund, H.; Torgerson, J.S.; Sjostrom, L.; Lindroos, A.K. Snacking frequency in relation to energy intake and food choices in obese men and women compared to a reference population. Int. J. Obes. (Lond.) 2005, 29, 711–719. [Google Scholar] [CrossRef]
- Hampl, J.S.; Heaton, C.L.; Taylor, C.A. Snacking patterns influence energy and nutrient intakes but not body mass index. J. Hum. Nutr. Diet. 2003, 16, 3–11. [Google Scholar] [CrossRef]
- Keast, D.R.; Nicklas, T.A.; O’Neil, C.E. Snacking is associated with reduced risk of overweight and reduced abdominal obesity in adolescents: National Health and Nutrition Examination Survey (NHANES) 1999–2004. Am. J. Clin. Nutr. 2010, 92, 428–435. [Google Scholar] [CrossRef]
- Zizza, C.A.; Duffy, P.A.; Gerrior, S.A. Food insecurity is not associated with lower energy intakes. Obesity (Silver Spring) 2008, 16, 1908–1913. [Google Scholar] [CrossRef] [PubMed]
- Elena, F.; Maria, B. Snack patterns of Greek adults 20–50 years of age. J. Foodserv. 2006, 17, 197–204. [Google Scholar] [CrossRef]
- Robinson, E.; Harris, E.; Thomas, J.; Aveyard, P.; Higgs, S. Reducing high calorie snack food in young adults: A role for social norms and health based messages. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 73. [Google Scholar] [CrossRef]
- Chamontin, A.; Pretzer, G.; Booth, D.A. Ambiguity of ‘snack’ in British usage. Appetite 2003, 41, 21–29. [Google Scholar] [CrossRef]
- Champagne, C.M.; Baker, N.B.; DeLany, J.P.; Harsha, D.W.; Bray, G.A. Assessment of energy intake underreporting by doubly labeled water and observations on reported nutrient intakes in children. J. Am. Diet. Assoc. 1998, 98, 426–433. [Google Scholar] [CrossRef]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 hour recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Children/Teens (2–18 years) n = 6,430,741 | Adults (≥19 years) n = 27,008,078 | ||
|---|---|---|---|---|
| Snack (Mean or %, SE) n = 5,817,816 | No Snack (Mean or %, SE) n = 612,925 | Snack (Mean or %, SE) n = 21,078,984 | No Snack (Mean or %, SE) n = 5,929,094 | |
| Mean age +/− SD (y) | 9.6 ± 0.1 | 12.2 ± 0.3 * | 48.9 ± 0.2 | 50.5 ± 0.6 * |
| Sex (% male) | 50.3 (0.8) | 48.2 (3.4) | 49.5 (0.4) | 51.0 (1.6) |
| Smoker (% yes) 2 | 3.3 (0.5) | 4.2 (1.2) | 18.6 (0.8) | 19.5 (1.4) |
| Ethnicity (% Caucasian) | 68.6 (1.4) | 56.9 (3.9)* | 75.9 (1.02) | 71.8 (1.9) * |
| Education (% university grad) 3 | 45.0 (1.2) | 39.4 (3.5) | 39.5 (1.03) | 34.6 (1.9) * |
| Marital status (% married or co-habiting) | N/A | N/A | 64.8 (0.9) | 61.1 (1.8) |
| Food secure (% yes) | 83.8 (0.9) | 85.7 (2.3) | 88.1 (0.6) | 90.2 (1.01) |
| BMI (kg/m2) | N/A | N/A | 27.3 (0.1) | 27.7 (0.2) |
| BMI z-score 4 | 0.46 (0.04) | 0.44 (0.1) | N/A | N/A |
| Overweight/obese (% yes) | 26.1 (1.1) | 27.5 (3.7) | 62.2 (1.2) | 60.5 (2.3) |
| Urban residence (% yes) | 81.7 (1.1) | 86.8 (2.2) | 82.3 (0.9) | 83.3 (1.3) |
| Immigrant to Canada (% yes) 5 | 8.5 (0.6) | 14.4 (2.4) | 27.8 (1.1) | 26.1 (1.7) |
| Nutrient | Snack | Breakfast/Brunch | Lunch | Dinner |
|---|---|---|---|---|
| % ± SE | % ± SE | % ± SE | % ± SE | |
| Energy (%) | 22.7 ± 0.3 | 19.2 ± 0.2 a | 22.8 ± 0.2 | 31.3 ± 0.2 c |
| Carbohydrates (%) | 25.8 ± 0.3 | 21.9 ± 0.2 a | 21.1 ± 0.2 b | 26.7 ± 0.3 c |
| Dietary fibers (%) | 25.8 ± 0.3 | 22.1 ± 0.3 a | 22.4 ± 0.3 b | 28.4 ± 0.3 c |
| Total sugars (%) | 33.0 ± 0.4 | 23.5 ± 0.3 a | 16.9 ± 0.3 b | 19.4 ± 0.3 c |
| Total Fat (%) | 23.4 ± 0.3 | 17.9 ± 0.3 a | 24.2 ± 0.3 b | 32.5 ± 0.3 c |
| SFA (%) | 22.9 ± 0.3 | 19.2 ± 0.3 a | 23.6 ± 0.3 | 31.6 ± 0.3 c |
| MUFA (%) | 23.4 ± 0.3 | 17.2 ± 0.3 a | 24.1 ± 0.3 b | 33.5 ± 0.3 c |
| PUFA (%) | 23.0 ± 0.4 | 17.5 ± 0.3 a | 25.5 ± 0.3 b | 32.9 ± 0.3 c |
| Cholesterol (%) | 12.4 ± 0.3 | 20.1 ± 0.4 a | 25.8 ± 0.4 b | 39.5 ± 0.4 c |
| Protein (%) | 14.7 ± 0.2 | 18.0 ± 0.2 a | 26.1 ± 0.2 b | 38.8 ± 0.3 c |
| Vitamin A RAE (%) | 16.8 ± 0.3 | 23.6 ± 0.4 a | 23.0 ± 0.4 b | 32.7 ± 0.4 c |
| Vitamin D (%) | 14.4 ± 0.4 | 35.3 ± 0.5 a | 19.1 ± 0.5 b | 25.9 ± 0.4 c |
| Vitamin C (%) | 23.4 ± 0.5 | 16.3 ± 0.4 a | 23.0 ± 0.4 b | 32.5 ± 0.5 c |
| Thiamin (%) | 16.7 ± 0.3 | 24.5 ± 0.3 a | 23.8 ± 0.3 b | 32.0 ± 0.3 c |
| Riboflavin (%) | 18.4 ± 0.3 | 26.9 ± 0.3 a | 20.5 ± 0.3 b | 27.3 ± 0.3 c |
| Niacin NEA (%) | 14.7 ± 0.2 | 17.9 ± 0.2 a | 25.7 ± 0.2 b | 38.9 ± 0.3 c |
| Vitamin B6 (%) | 17.6 ± 0.3 | 18.1 ± 0.3 | 23.2 ± 0.3 b | 37.8 ± 0.3 c |
| Vitamin B12 (%) | 13.4 ± 0.3 | 23.7 ± 0.4 a | 23.3 ± 0.4 b | 35.1 ± 0.4 c |
| Folic acid (%) | 17.4 ± 0.4 | 27.9 ± 0.5 a | 25.3 ± 0.5 b | 28.6 ± 0.5 c |
| Folate DFE (%) | 18.0 ± 0.3 | 22.2 ± 0.3 a | 24.6 ± 0.3 b | 32.2 ± 0.3 c |
| Calcium (%) | 21.1 ± 0.3 | 25.9 ± 0.3 a | 20.8 ± 0.3 | 25.0 ± 0.3 c |
| Magnesium (%) | 21.2 ± 0.3 | 22.5 ± 0.3 a | 20.9 ± 0.3 | 28.5 ± 0.3 c |
| Iron (%) | 18.2 ± 0.3 | 24.1 ± 0.3 a | 23.4 ± 0.3 b | 32.1 ± 0.3 c |
| Zinc (%) | 16.4 ± 0.3 | 19.5 ± 0.3 a | 24.7 ± 0.3 b | 36.7 ± 0.3 c |
| Sodium (%) | 14.8 ± 0.3 | 17.6 ± 0.3 a | 28.9 ± 0.3 b | 36.3 ± 0.3 c |
| Potassium (%) | 20.7 ± 0.3 | 20.0 ± 0.2 a | 21.6 ± 0.2 | 31.8 ± 0.3 c |
| Nutrients | 2–5 years % ± SE | 6–12 years % ± SE | 13–18 years % ± SE | 19–54 years % ± SE | ≥55 years % ± SE |
|---|---|---|---|---|---|
| Energy (%) | 27.0 ± 0.6 | 26.5 ± 0.5 | 24.9 ± 0.6 | 22.3 ± 0.5 | 20.8 ± 0.4 * |
| Carbohydrates (%) | 29.9 ± 0.7 | 29.8 ± 0.6 | 28.1 ± 0.5 | 25.3 ± 0.5 | 24.2 ± 0.5 * |
| Dietary fibers (%) | 30.4 ± 0.9 | 29.6 ± 0.7 | 29.3 ± 0.6 | 25.9 ± 0.6 | 22.9 ± 0.5 * |
| Total sugars (%) | 37.0 ± 0.9 | 35.8 ± 0.7 | 34.0 ± 0.7 | 32.8 ± 0.7 | 31.7 ± 0.6 * |
| Total Fat (%) | 27.2 ± 1.0 | 26.4 ± 0.7 | 25.1 ± 0.7 | 23.5 ± 0.6 | 21.4 ± 0.5 * |
| SFA (%) | 26.8 ± 1.1 | 25.9 ± 0.7 | 24.7 ± 0.8 | 22.9 ± 0.6 | 21.2 ± 0.5 * |
| MUFA (%) | 26.6 ± 1.1 | 25.8 ± 0.7 | 24.9 ± 0.8 | 23.6 ± 0.6 | 21.4 ± 0.5 * |
| PUFA (%) | 27.8 ± 1.0 | 26.7 ± 0.8 | 24.6 ± 0.8 | 23.3 ± 0.7 | 20.2 ± 0.5 * |
| Cholesterol (%) | 17.4 ± 0.9 | 14.8 ± 0.6 | 14.2 ± 0.6 | 11.8 ± 0.5 | 11.5 ± 0.4 * |
| Protein (%) | 19.6 ± 0.7 | 17.0 ± 0.5 | 16.5 ± 0.5 | 14.6 ± 0.4 | 13.1 ± 0.3 * |
| Vitamin A RAE (%) | 20.0 ± 0.9 | 20.0 ± 0.7 | 19.7 ± 0.8 | 16.6 ± 0.6 | 15.0 ± 0.5 * |
| Vitamin D (%) | 17.7 ± 0.6 | 16.9 ± 0.5 | 15.6 ± 0.6 | 14.8 ± 0.5 | 12.4 ± 0.4 * |
| Vitamin C (%) | 30.2 ± 1.7 | 29.7 ± 1.0 | 25.8 ± 0.9 | 22.9 ± 0.8 | 20.5 ± 0.7 * |
| Thiamin (%) | 20.4 ± 0.7 | 19.2 ± 0.6 | 18.8 ± 0.6 | 16.8 ± 0.4 | 14.8 ± 0.4 * |
| Riboflavin (%) | 24.3 ± 0.9 | 21.2 ± 0.5 | 20.1 ± 0.6 | 18.1 ± 0.5 | 16.8 ± 0.3 * |
| Niacin NEA (%) | 18.7 ± 0.6 | 16.8 ± 0.5 | 16.6 ± 0.5 | 14.6 ± 0.4 | 13.1 ± 0.3 |
| Vitamin B6 (%) | 22.6 ± 0.8 | 20.8 ± 0.6 | 20.3 ± 0.6 | 17.6 ± 0.5 | 15.3 ± 0.4 * |
| Vitamin B12 (%) | 18.4 ± 0.9 | 16.1 ± 0.6 | 15.9 ± 0.7 | 13.1 ± 0.5 | 11.7 ± 0.4 * |
| Folic acid (%) | 20.3 ± 1.2 | 19.2 ± 0.8 | 18.3 ± 0.8 | 16.7 ± 0.6 | 17.1 ± 0.7 * |
| Folate DFE (%) | 21.4 ± 0.9 | 20.7 ± 0.6 | 19.4 ± 0.6 | 17.6 ± 0.5 | 16.9 ± 0.4 * |
| Calcium (%) | 26.3 ± 1.1 | 23.3 ± 0.6 | 22.0 ± 0.7 | 20.9 ± 0.6 | 19.7 ± 0.5 * |
| Magnesium (%) | 24.9 ± 0.7 | 23.9 ± 0.5 | 23.9 ± 0.6 | 21.3 ± 0.5 | 19.1 ± 0.4 * |
| Iron (%) | 21.9 ± 0.8 | 21.3 ± 0.5 | 21.5 ± 0.6 | 18.2 ± 0.5 | 15.9 ± 0.4 * |
| Zinc (%) | 20.5 ± 0.7 | 18.4 ± 0.5 | 18.6 ± 0.6 | 16.5 ± 0.5 | 14.3 ± 0.3 * |
| Sodium (%) | 18.6 ± 0.7 | 18.1 ± 0.5 | 17.6 ± 0.6 | 14.8 ± 0.5 | 12.7 ± 0.4 * |
| Potassium (%) | 25.7 ± 0.7 | 24.5 ± 0.5 | 23.7 ± 0.6 | 20.7 ± 0.5 | 18.2 ± 0.4 * |
| Whole Grain | Non-Whole Grain, Enriched | Non-Whole Grain, Not Enriched | |
|---|---|---|---|
| Age groups | %± SE | % ± SE | % ± SE |
| All ages (≥2 years) n = 26,896,800 | 15.2 ± 0.8 | 66.6 ± 1.0 | 18.2 ± 0.8 * |
| 2–5 years n = 1,181,823 | 15.6 ± 2.2 | 69.2 ± 2.8 | 15.2 ± 2.0 * |
| 6–12 years n = 2,407,637 | 15.8 ± 1.4 | 62.6 ± 2.0 | 21.5 ± 1.9 * |
| 13–18 years n = 2,228,356 | 15.0 ± 1.8 | 61.4 ± 2.1 | 23.6 ± 1.8 * |
| 19–54 years n = 12,768,195 | 14.6 ± 1.3 | 65.8 ± 1.8 | 19.7 ± 1.4 * |
| ≥55 years n = 8,310,789 | 15.9 ± 1.5 | 70.9 ± 1.8 | 13.2 ± 1.4 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vatanparast, H.; Islam, N.; Patil, R.P.; Shafiee, M.; Smith, J.; Whiting, S. Snack Consumption Patterns among Canadians. Nutrients 2019, 11, 1152. https://doi.org/10.3390/nu11051152
Vatanparast H, Islam N, Patil RP, Shafiee M, Smith J, Whiting S. Snack Consumption Patterns among Canadians. Nutrients. 2019; 11(5):1152. https://doi.org/10.3390/nu11051152
Chicago/Turabian StyleVatanparast, Hassan, Naorin Islam, Rashmi Prakash Patil, Mojtaba Shafiee, Jessica Smith, and Susan Whiting. 2019. "Snack Consumption Patterns among Canadians" Nutrients 11, no. 5: 1152. https://doi.org/10.3390/nu11051152
APA StyleVatanparast, H., Islam, N., Patil, R. P., Shafiee, M., Smith, J., & Whiting, S. (2019). Snack Consumption Patterns among Canadians. Nutrients, 11(5), 1152. https://doi.org/10.3390/nu11051152