Consumption Patterns of Grain-Based Foods among Adults in Canada: Evidence from Canadian Community Health Survey—Nutrition 2015

 ,
, 
Abstract
:1. Background
2. Subject and Method
2.1. Data
2.2. Dietary Intake Data
2.3. Socioeconomic Status
2.4. Method
3. Results
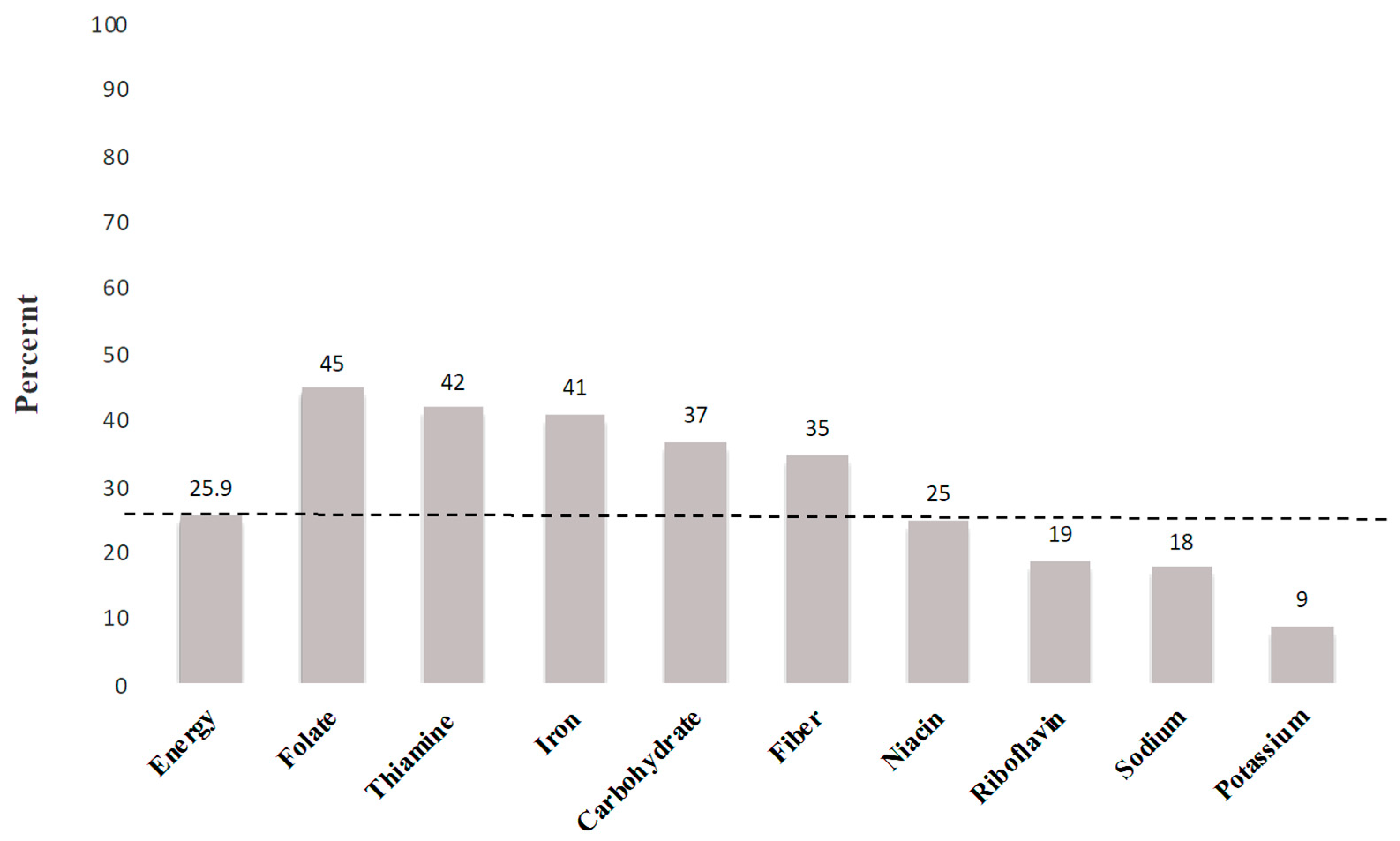
3.1. Nutrient and Energy Intake
3.2. SES and GBFs Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ye, E.Q.; Chacko, S.A.; Chou, E.L.; Kugizaki, M.; Liu, S. Greater Whole-Grain Intake Is Associated with Lower Risk of Type 2 Diabetes, Cardiovascular Disease, and Weight Gain. J. Nutr. 2012, 142, 1304–1313. [Google Scholar] [CrossRef]
- Pauline, K.-B.; Rimm, E.B. Whole grain consumption and weight gain: a review of the epidemiological evidence, potential mechanisms and opportunities for future research. Proc. Nutr. Soc. 2003, 62, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Overview of Canadians’ Eating Habits. Health Rep. 2004, 2, 1–43. [Google Scholar]
- Harland, J.I.; Garton, L.E. Whole-grain intake as a marker of healthy body weight and adiposity. Public Health Nutr. 2008, 11, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Expert Advisory Group on National Nutrition Pregnancy Guidelines. Prenatal Nutrition Guidelines for Health Professionals—Folate Contributes to a Healthy Pregnancy. Government of Canada, 2009. Available online: http://www.hc-sc.gc.ca/fn-an/alt_formats/hpfb-dgpsa/pdf/pubs/iron-fer-eng.pdf (accessed on 12 March 2019).
- Williams, P.G. Evaluation of the evidence between consumption of refined grains and health outcomes. Nutr. Rev. 2012, 70, 80–99. [Google Scholar] [CrossRef] [PubMed]
- Mobley, A.R.; Slavin, J.L.; Hornick, B.A. The Future of Recommendations on Grain Foods in Dietary Guidance. J. Nutr. 2013, 143, 1527S–1532S. [Google Scholar] [CrossRef]
- Aune, D.; Chan, D.S.M.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343, 1082. [Google Scholar] [CrossRef]
- Aune, D.; Keum, N.N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, i2716. [Google Scholar] [CrossRef]
- Threapleton, D.E.; Greenwood, D.C.; Evans, C.E.L.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Cade, J.E.; Gale, C.P.; Burley, V.J. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2013, 347, f6879. [Google Scholar] [CrossRef] [PubMed]
- De Munter, J.S.L.; Hu, F.B.; Spiegelman, D.; Franz, M.; Van Dam, R.M. Whole grain, bran, and germ intake and risk of type 2 diabetes: A prospective cohort study and systematic review. PLoS Med. 2007, 4, e261. [Google Scholar] [CrossRef] [PubMed]
- Channell, P.J. Exact Vlasov equilibria for field-reversing rings. Phys. Fluids 1980, 23, 1263–1267. [Google Scholar] [CrossRef]
- Zong, G.; Gao, A.; Hu, F.B.; Sun, Q. Whole grain intake and mortality from all causes, cardiovascular disease, and cancer. Circulation 2016, 133, 2370–2380. [Google Scholar] [CrossRef] [PubMed]
- Radhika, G.; Van Dam, R.M.; Sudha, V.; Ganesan, A.; Mohan, V. Refined grain consumption and the metabolic syndrome in urban Asian Indians (Chennai Urban Rural Epidemiology Study 57). Metabolism 2009, 58, 675–681. [Google Scholar] [CrossRef] [PubMed]
- AlEssa, H.B.; Bhupathiraju, S.N.; Malik, V.S.; Wedick, N.M.; Campos, H.; Rosner, B.; Willett, W.C.; Hu, F.B. Carbohydrate quality and quantity and risk of type 2 diabetes in US women. Am. J. Clin. Nutr. 2015, 102, 1543–1553. [Google Scholar] [CrossRef] [PubMed]
- Canadian Food Inspection Agency Fortification—Labelling and Composition Requirements for Grain and Bakery Products—Food—Canadian Food Inspection Agency. Available online: http://www.inspection.gc.ca/food/labelling/food-labelling-for-industry/grain-and-bakery-products/eng/1392135900214/1392135960867 (accessed on 10 December 2018).
- Papanikolaou, Y.; Fulgoni, V.L., III. Certain Grain Food Patterns Are Associated with Improved 2015 Dietary Guidelines Shortfall Nutrient Intakes, Diet Quality, and Lower Body Weight in US Adults: Results from the National Health and Nutrition Examination Survey, 2005-2010. Food Nutr. Sci. 2016, 7, 772–781. [Google Scholar] [CrossRef]
- Papanikolaou, Y.; Fulgoni, V.L. Grain foods are contributors of nutrient density for American adults and help close nutrient recommendation gaps: Data from the national health and nutrition examination survey, 2009–2012. Nutrients 2017, 9, 873. [Google Scholar] [CrossRef]
- Bautista-Castaño, I.; Sánchez-Villegas, A.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Covas, M.I.; Schroder, H.; Alvarez-Pérez, J.; Quilez, J.; et al. Changes in bread consumption and 4-year changes in adiposity in Spanish subjects at high cardiovascular risk. Br. J. Nutr. 2013, 110, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Pol, K.; Christensen, R.; Bartels, E.M.; Raben, A.; Tetens, I.; Kristensen, M. Whole grain and body weight changes in apparently healthy adults: A systematic review and meta-analysis of randomized controlled studies. Am. J. Clin. Nutr. 2013, 98, 872–884. [Google Scholar] [CrossRef]
- Vatanparast, H.; Whiting, S.; Hossain, A.; Mirhosseini, N.; Merchant, A.T.; Szafron, M. National pattern of grain products consumption among Canadians in association with body weight status. BMC Nutr. 2017, 3, 59. [Google Scholar] [CrossRef]
- Statistics Canada Canadian Community Health Survey (CCHS): Nutrition—2015 (First Interview). Available online: http://www23.statcan.gc.ca/imdb/p3Instr.pl?Function=assembleInstr&lang=en&Item_Id=202664#qb210826 (accessed on 12 March 2019).
- Health Canada. Bureau of Nutritional Sciences (BNS) Food Group Codes and Descriptions—Canadian Community Health Survey (CCHS) 2.2. Government of Canada, 2014. Available online: http://www23.statcan.gc.ca/imdb-bmdi/pub/document/5049_D23_T9_V1-eng.pdf (accessed on 12 March 2019).
- Health Canada. The Development and Use of a Surveillance Tool: The Classification of Foods in the Canadian Nutrient File According to Eating Well with Canada’s Food GuideHealth Canada (2014). The Development and Use of a Surveillance Tool: The Classification of Foods. 2014. Available online: http://publications.gc.ca/collections/collection_2014/sc-hc/H164-158-2-2014-eng.pdf (accessed on 12 March 2019).
- Jain, A.K. Data clustering: 50 years beyond K-means. Pattern Recognit. Lett. 2010, 31, 651–666. [Google Scholar] [CrossRef]
- Kanungo, T.; Mount, D.M.; Netanyahu, N.S.; Piatko, C.D.; Silverman, R.; Wu, A.Y. An efficient k-means clustering algorithms: Analysis and implementation. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 881–892. [Google Scholar] [CrossRef]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Wirfält, A.K.E.; Jeffery, R.W. Using cluster analysis to examine dietary patterns: Nutrient intakes, gender, and weight status differ across food pattern clusters. J. Am. Diet. Assoc. 1997, 97, 272–279. [Google Scholar] [CrossRef]
- Makles, A. Stata tip 110: How to get the optimal k-means cluster solution. Stata J. 2012, 12, 347–351. [Google Scholar] [CrossRef]
- StataCorp cluster stop—Cluster-analysis stopping rules. Stata 13 Base Ref. Man. 2013, 1–8.
- Caliñski, T.; Harabasz, J. A Dendrite Method Foe Cluster Analysis. Commun. Stat. 1974, 3, 1–27. [Google Scholar]
- Majumder, S.; Fisk, H.A. VDAC3 and Mps1 negatively regulate ciliogenesis. Cell Cycle 2013, 12, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Schenker, N.; Gentleman, J.F. On judging the significance of differences by examining the overlap between confidence intervals. Am. Stat. 2001, 55, 182–186. [Google Scholar] [CrossRef]
- Health Canada. Health Canada’s Proposed Changes to the Core Nutrients Declared in the Canadian Nutrition Facts Table. Government of Canada, 2014. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/public-involvement-partnerships/technical-consultation-proposed-changes-core-nutrientsdeclared-canadian-nutrition-facts-table/consultation.html (accessed on 10 December 2018).
- Sacco, J. Food fortification policy in Canada. In Handbook of Food Fortification and Health. Nutrition and Health; Preedy, V., Srirajaskanthan, R., Patel, V., Eds.; Humana Press: New York, NY, USA, 2013; Volume 1, pp. 59–71. ISBN 978-1-4614-7076-2. [Google Scholar]
- Health Canada Canada’s Food Guide. Government of Canada. Available online: https://food-guide.canada.ca/en/ (accessed on 5 February 2019).
- Pingali, P. Westernization of Asian diets and the transformation of food systems: Implications for research and policy. Food Policy 2007, 32, 281–298. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef]
- Drewnowski, A. Obesity and the food environment: Dietary energy density and diet costs. Am. J. Prev. Med. 2004, 27, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.K. Wheat in national diets. Wheat Stud. Food Res. Inst. 1941, 18, 37–76. [Google Scholar]
- Timmer, C.P. Farmers and Markets: The Political Economy of New Paradigms. Am. J. Agric. Econ. 1997, 79, 621. [Google Scholar] [CrossRef]
- Macdiarmid, J.; Blundell, J. Assessing dietary intake: who, what and why of under-reporting. Nutr. Res. Rev. 1998, 11, 231–253. [Google Scholar] [CrossRef]
- Papanikolaou, Y.; Jones, J.M.; Fulgoni, V.L. Several grain dietary patterns are associated with better diet quality and improved shortfall nutrient intakes in US children and adolescents: A study focusing on the 2015–2020 Dietary Guidelines for Americans. Nutr. J. 2017, 16, 13. [Google Scholar] [CrossRef]

{kind=link}
| GBFs Pattern | The Contribution of GBFs to Total Energy Intake (%) | The Contribution of GBFs Within Cluster (%) | Canadian Adults in the Cluster (%) | Population (n) |
|---|---|---|---|---|
| Mixed | 40.7 | 11,000,000 | ||
| Whole Grain Cereals | 3.2 | 14.2 | ||
| Other Bread | 2.5 | 10.9 | ||
| Salty Snacks | 2.4 | 10.5 | ||
| Muffin | 2.2 | 9.7 | ||
| White Bread | 1.6 | 6.9 | ||
| Cakes & Cookies | 1.5 | 6.4 | ||
| Whole Bread | 1.4 | 6.2 | ||
| Rice | 1.2 | 5.1 | ||
| Whole Grain Bread | 1.0 | 4.2 | ||
| Whole Grain and Whole Wheat Bread | 0.9 | 3.9 | ||
| White Bread | 20.5 | 62.3 | 12.2 | 3,300,000 |
| Cakes & Cookies | 1.9 | 5.6 | ||
| Other Bread | 1.5 | 4.6 | ||
| Whole Grain Cereals | 1.5 | 4.5 | ||
| Pasta | 1.2 | 3.6 | ||
| Salty Snacks | 1.1 | 3.4 | ||
| Rice | 1.0 | 3.2 | ||
| Danish and Doughnuts | 0.8 | 2.4 | ||
| Muffin | 0.8 | 2.3 | ||
| Other Cereals | 0.6 | 1.9 | ||
| Other Bread | 23.5 | 63.4 | 10.4 | 2,800,000 |
| Rice | 1.7 | 4.6 | ||
| Whole Grain Cereals | 1.7 | 4.5 | ||
| White Bread | 1.5 | 4.0 | ||
| Cakes & Cookies | 1.4 | 3.9 | ||
| Whole Grain and Whole Wheat Bread | 1.2 | 3.2 | ||
| Salty Snacks | 1.1 | 3.0 | ||
| Pasta | 0.9 | 2.5 | ||
| Muffin | 0.9 | 2.5 | ||
| Danish and Doughnuts | 0.7 | 2.0 | ||
| Pasta | 20.9 | 52.6 | 8.6 | 2,300,000 |
| White Bread | 2.9 | 7.4 | ||
| Other Bread | 2.2 | 5.5 | ||
| Whole Grain Cereals | 2.1 | 5.3 | ||
| Cakes & Cookies | 1.7 | 4.4 | ||
| Salty Snacks | 1.5 | 3.9 | ||
| Whole Grain and Whole Wheat Bread | 1.5 | 3.8 | ||
| Muffin | 1.4 | 3.4 | ||
| Rice | 1.2 | 3.0 | ||
| Whole Bread | 0.7 | 1.8 | ||
| Rice | 21.9 | 58.0 | 8 | 2,200,000 |
| Other Bread | 2.3 | 6.0 | ||
| White Bread | 2.2 | 5.8 | ||
| Whole Grain and Whole Wheat Bread | 1.9 | 4.9 | ||
| Whole Grain Cereals | 1.7 | 4.6 | ||
| Cakes & Cookies | 1.6 | 4.2 | ||
| Salty Snacks | 1.1 | 2.8 | ||
| Muffin | 1.0 | 2.8 | ||
| Pasta | 1.0 | 2.5 | ||
| Danish and Doughnuts | 0.6 | 1.6 | ||
| Whole Grain and Whole Wheat Bread | 0.9 | 3.9 | ||
| Whole Grain and Whole Wheat Bread | 17.9 | 56.7 | 8 | 2,200,000 |
| Whole Grain Cereals | 2.4 | 7.5 | ||
| Cakes & Cookies | 2.0 | 6.3 | ||
| Other Bread | 1.5 | 4.7 | ||
| Rice | 1.5 | 4.6 | ||
| Salty Snacks | 1.2 | 3.8 | ||
| Pasta | 0.9 | 2.8 | ||
| Muffin | 0.8 | 2.6 | ||
| White Bread | 0.6 | 1.8 | ||
| Other Cereals | 0.5 | 1.6 | ||
| Cakes & Cookies | 23.5 | 55.8 | 5.9 | 1,600,000 |
| White Bread | 3.5 | 8.3 | ||
| Other Bread | 2.8 | 6.7 | ||
| Whole Grain Cereals | 2.1 | 4.9 | ||
| Whole Grain and Whole Wheat Bread | 1.7 | 3.9 | ||
| Pasta | 1.5 | 3.5 | ||
| Rice | 1.4 | 3.3 | ||
| Salty Snacks | 1.3 | 3.1 | ||
| Muffin | 0.9 | 2.2 | ||
| Whole Bread | 0.7 | 1.6 |
| No Grain Consumers | Other Bread | Cakes & Cookies | Pasta | Rice | Mixed | White Bread | Whole Wheat & Whole-Grain Bread | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Energy (Kcal) | 1457 (76.8) | 1738.6 (39.5) | 2040.3 (54.2) | 1866.6 (47.02) | 1609.8 (44.1) | 2102.3 (21.8) | 1805.8 (41) | 1561.6 (35.7) | 0.99 |
| Calcium (mg) | 584.1 (31.7) | 738.4 (24.6) | 768.4 (25) | 779.3 (27) | 568.4† (21) | 914.3 *† (15) | 709.02 (20.6) | 690.81 (23.3) | 0 < 0.0001 |
| Iron (mg) | 8.3 *† (0.4) | 12.4 (0.3) | 13.5 (0.4) | 12.9 (0.4) | 9.8 (0.29) | 13.5 (0.17) | 12.7 (0.3) | 10.4 (0.3) | 0 < 0.0001 |
| Potassium (mg) | 2547.8 (83.8) | 2438.7 (52.22) | 2637.4 (66.5) | 2587.1 (65.4) | 2337.7 (61.3) | 3029.7 *† (34) | 2362 (55.4) | 2469.5 (56.17) | 0 < 0.0001 |
| Folate DFE. (mcg) | 263.2 *† (14.6) | 461.6 (13.3) | 480.7 (19.55) | 609.4 *† (17.08) | 329.6 (10.8) | 455.1 (6.75) | 492.5 (12.85) | 309.7 (9.36) | 0 < 0.0001 |
| Folic Acid (mcg) | 23.79 *† (3.49) | 122.17 (4.06) | 135.61 (8.07) | 221.7 *† (7.6) | 60.22 (3.51) | 103.23 (2.31) | 160.2 *† (4.69) | 53.83 (2.74) | 0 < 0.0001 |
| Riboflavin (mg) | 1.62 (0.09) | 1.88 (0.05) | 1.92 (0.05) | 1.92 (0.06) | 1.47† (0.04) | 2.1 *† (0.03) | 1.96 (0.05) | 1.61 (0.05) | 0 < 0.0001 |
| Thiamin (mg) | 0.95 *† (0.04) | 1.67 (0.05) | 1.69 (0.07) | 1.88 (0.06) | 1.23 (0.04) | 1.69 (0.02) | 1.66 (0.04) | 1.25 (0.03) | 0 < 0.0001 |
| Niacin (mg) | 34.55 (2.32) | 37.58 (1.05) | 37.36 (1.3) | 41.48 (1.29) | 35.06 (1.18) | 43.1 (0.57) | 37.02 (0.91) | 33.96 (1.01) | 0 < 0.0001 |
| Dietary fibres (g) | 12.45 *† (0.61) | 17.68 (0.57) | 17.17 (0.62) | 17.89 (0.61) | 15.21 (0.63) | 18.54 (0.25) | 14.59 (0.38) | 18.52 (0.48) | 0 < 0.0001 |
| Sodium (mg) | 1853.5 *† (119.78) | 2637.31 (79.46) | 2686.9 (91.51) | 2674.3 (83.7) | 2292 *† (79.3) | 2977.33 (41.09) | 2941 (76.2) | 2607.5 (84.87) | 0 < 0.0001 |
| Sugars (g) | 73.83 (3.78) | 72.32 (1.96) | 116.7 *† (3.25) | 79.42 (2.59) | 65.36 (2.87) | 98.3 *† (1.58) | 85.52 (2.44) | 69.94 (2.21) | 0 < 0.0001 |
| Vitamin B6 (mg) | 1.74 (0.1) | 1.55 (0.04) | 1.6 (0.08) | 1.55 (0.05) | 1.68 (0.05) | 1.9 † (0.03) | 1.36 *† (0.04) | 1.5 (0.05) | 0 < 0.0001 |
| Total Carbohydrates (g) | 141.9 *† (6.1) | 216.5 (4.5) | 257.9 *† (7.1) | 236.3 (5.7) | 212.5 (6.3) | 237.5 (2.7) | 223.4 (5.1) | 189.1 *† (4.5) | 0 < 0.0001 |
| Cholesterol (mg) | 292.6 (22.8) | 238.9 (22.5) | 265.4 (10) | 237.8 (9.9) | 240.8 (10.7) | 305.2† (7.1) | 254.6 (13.2) | 243.9 (12.1) | 0 < 0.0001 |
| % Energy from Carbohydrates | 40.2 *† (0.89) | 50.1 (0.55) | 50.4 (0.59) | 51.1 (0.55) | 53.3 *† (0.6) | 45.1 *† (0.27) | 49.7 (0.48) | 48.7 (0.78) | 0 < 0.0001 |
| Saturated Fatty Acid (g) | 18.0 (1.2) | 20.8 (0.7) | 25 (1.0) | 21.1 (0.7) | 15.0† (0.6) | 26.6 (0.4) | 22.2 (0.7) | 18.1† (0.8) | 0 < 0.0001 |
| Fat (g) | 57.88 (3.66) | 61.59 (1.92) | 77.29 (2.67) | 64.07 (2.19) | 50.2 *† (1.78) | 82.05 (1.1) | 66.06 (2.05) | 56.74 (1.81) | 0 < 0.0001 |
| Magnesium (mg) | 264.9 (10.84) | 283.66 (5.85) | 299.92 (8.22) | 305.7 (10.11) | 281.56 (9.15) | 340.2 *† (4) | 270.91 (7.28) | 308.18 (7.28) | 0 < 0.0001 |
| Proteins (g) | 74.07 (4.97) | 75.59 (2.18) | 76.25 (2.3) | 78.69 (2.36) | 72.24 (2.13) | 88.03 *† (1.09) | 72.66 (1.74) | 69.29 (1.89) | 0 < 0.0001 |
| Vitamin A (mcg) | 635.37 (49.52) | 536.02 (27.29) | 661.73 (31.3) | 612.16 (27.15) | 600.81 (50.47) | 745.41 (20.85) | 523.96 (18.33) | 638.92 (33.41) | 0 < 0.0001 |
| Zinc (mg) | 8.86 (0.48) | 10 (0.3) | 10.53 (0.46) | 9.92 (0.34) | 9.28 (0.28) | 11.96 (0.21) | 9.43 (0.27) | 9.19 (0.29) | 0 < 0.0001 |
| No Grain Consumers | Other Bread | Cakes & Cookies | Pasta | Rice | Mixed | White Bread | Whole Wheat & Whole-Grain Bread | |
|---|---|---|---|---|---|---|---|---|
| Total Fruits & Vegetables | 5.1 (0.29) | 3.8 (0.13) | 4.4 (0.21) | 4.6 (0.18) | 4.3 (0.19) | 5 (0.1) | 3.8 (0.17) | 4.2 (0.16) |
| Fruits (excluding fruit juice) | 1.4 (0.11) | 1 (0.06) | 1 (0.09) | 1.1 (0.08) | 1.4 (0.11) | 1.5 (0.05) | 1.1 (0.08) | 1.3 (0.11) |
| Dark Green Vegetables | 0.7 (0.08) | 0.4 (0.04) | 0.5 (0.06) | 0.6 (0.08) | 0.8 (0.08) | 0.6 (0.03) | 0.3 † (0.03) | 0.6 (0.06) |
| Orange Vegetables | 0.3 (0.05) | 0.2 (0.04) | 0.2 (0.04) | 0.2 (0.02) | 0.2 (0.03) | 0.2 (0.02) | 0.1 (0.02) | 0.2 (0.03) |
| Potato | 0.8 (0.09) | 0.5 (0.05) | 0.7 (0.1) | 0.3 (0.04) | 0.2 (0.03) | 0.8 (0.04) | 0.7 (0.08) | 0.5 (0.05) |
| Other Vegetables | 1.6 (0.21) | 1.1 (0.06) | 1.1 (0.1) | 1.8† (0.08) | 1.2 (0.08) | 1.4 (0.04) | 1.1 (0.06) | 1 (0.07) |
| Total Milk & Alternatives | 1 (0.08) | 1.3 (0.07) | 1.3 (0.08) | 1.4 (0.07) | 0.8 *† (0.07) | 1.7 *† (0.05) | 1.3 (0.06) | 1.2 (0.07) |
| Fluid Milk or Soy Milk | 0.5 (0.05) | 0.5 (0.03) | 0.6 (0.05) | 0.7 (0.06) | 0.4† (0.04) | 0.7 (0.03) | 0.5 (0.04) | 0.5 (0.03) |
| Other Product Made of Milk | 0.6 (0.05) | 0.8 (0.05) | 0.7 (0.06) | 0.8 (0.06) | 0.4† * (0.05) | 1†* (0.03) | 0.8 (0.05) | 0.7 (0.06) |
| Total Meat & Alternatives | 2.4 (0.28) | 1.9 (0.1) | 1.9 (0.1) | 1.7 (0.09) | 2 (0.08) | 2.4† (0.05) | 1.9 (0.08) | 1.9 (0.08) |
| Poultry | 1.1 (0.27) | 0.7 (0.09) | 0.5 (0.09) | 0.5 (0.07) | 0.7 (0.07) | 0.7 (0.03) | 0.4 (0.04) | 0.5 (0.04) |
| Beef | 0.4 (0.05) | 0.4 (0.04) | 0.5 (0.09) | 0.4 (0.04) | 0.3 (0.03) | 0.5 (0.03) | 0.4 (0.04) | 0.3 (0.03) |
| Legumes | 0.2 (0.04) | 0.2 (0.02) | 0.2 (0.04) | 0.3 (0.04) | 0.3 (0.04) | 0.4 (0.02) | 0.3 (0.03) | 0.3 (0.04) |
| Egg | 0.3 (0.03) | 0.2 (0.05) | 0.2 (0.02) | 0.2 (0.02) | 0.2 (0.03) | 0.2 (0.01) | 0.3 (0.03) | 0.3 (0.03) |
| Processed Meat | 0.1 (0.02) | 0.3 (0.03) | 0.2 (0.03) | 0.2 (0.02) | 0.1 (0.02) | 0.3 (0.02) | 0.4 (0.03) | 0.3 (0.03) |
| SES | No Grain Consumers | Other Bread | Cakes and Cookies | Pasta | Rice | Mixed | White Bread | Whole Wheat & Whole Grain Bread |
|---|---|---|---|---|---|---|---|---|
| Mean age (SEM) | 47.9 (1) | 46.5 (0.7) | 51 (1.5) | 44.9 (1) | 46.3 (0.8) | 49.5 (0.4) | 51.9 (0.7) | 55.8 *† (0.9) |
| BMI (SEM) | 27.6 (0.6) | 27.1 (0.4) | 26.8 (0.4) | 26.7 (0.3) | 26.5 (0.4) | 27.5 (0.2) | 27.9 (0.3) | 28.1 (0.4) |
| % male | 40 *† | 47 | 55 | 50 | 53 | 51 | 51 | 47 |
| % Caucasian | 76 | 70 | 74 | 73 | 31 *† | 83 | 82 | 78 |
| Smoker | 26 | 16 | 14 | 20 | 15 | 18 | 28† | 12 |
| Education (% university grad) 1 | 38 | 42 | 33 | 41 | 47 | 40 | 29 | 32 |
| Married (%) | 58 | 66 | 65 | 63 | 73 *† | 64 | 62 | 63 |
| Food secure (%) | 87 | 89 | 87 | 92 | 88 | 90 | 83 *† | 90 |
| Urban (%) | 80 | 84 | 84 | 85 | 93 *† | 81 | 81 | 78 |
| Immigrant (%) | 26 | 35 | 32 | 26 | 67 *† | 20 | 21 | 28 |
| Overweight/obese (%) | 61 | 57 | 60 | 58 | 53 | 64 | 67 | 69 |
| Physical Act (%) | 68 | 73 | 69 | 73 | 72 | 76 | 66 | 73 |
| Mean age (SEM) | 55.8 *† (0.9) |
| The Lowest | Low | Middle | High | The Highest | |
|---|---|---|---|---|---|
| No Grain Consumers | 19.4 | 14.1 * | 20.6 | 20.2 | 25.7 |
| Other Bread | 21.2 | 18.1 | 20.3 | 19.1 | 21.3 |
| Cakes and Cookies | 21.0 | 21.6 | 18.9 | 21.3 | 17.2 |
| Pasta | 16.5 | 23.3 | 20.3 | 18.3 | 21.6 |
| Rice | 28.6 | 24.7 | 17.9 | 17.2 | 11.6 * |
| Mixed | 16.4 | 18.0 | 19.4 | 21.2 | 25.0 * |
| White Bread | 25.8 | 23.3 | 16.4 | 16.1 | 18.3 |
| Whole Wheat & Whole-Grain Bread | 22.2 | 20.2 | 20.8 | 19.3 | 17.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini, S.H.; Papanikolaou, Y.; Islam, N.; Rashmi, P.; Shamloo, A.; Vatanparast, H. Consumption Patterns of Grain-Based Foods among Adults in Canada: Evidence from Canadian Community Health Survey—Nutrition 2015. Nutrients 2019, 11, 784. https://doi.org/10.3390/nu11040784
Hosseini SH, Papanikolaou Y, Islam N, Rashmi P, Shamloo A, Vatanparast H. Consumption Patterns of Grain-Based Foods among Adults in Canada: Evidence from Canadian Community Health Survey—Nutrition 2015. Nutrients. 2019; 11(4):784. https://doi.org/10.3390/nu11040784
Chicago/Turabian StyleHosseini, Seyed H., Yanni Papanikolaou, Naorin Islam, Patil Rashmi, Arash Shamloo, and Hassan Vatanparast. 2019. "Consumption Patterns of Grain-Based Foods among Adults in Canada: Evidence from Canadian Community Health Survey—Nutrition 2015" Nutrients 11, no. 4: 784. https://doi.org/10.3390/nu11040784
APA StyleHosseini, S. H., Papanikolaou, Y., Islam, N., Rashmi, P., Shamloo, A., & Vatanparast, H. (2019). Consumption Patterns of Grain-Based Foods among Adults in Canada: Evidence from Canadian Community Health Survey—Nutrition 2015. Nutrients, 11(4), 784. https://doi.org/10.3390/nu11040784