Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Method
- Interventions (e.g., intervention, clinical trial, experimental studies)
- Nutrition (e.g., diet, food, beverage)
- Population (e.g., preschool, toddler and parent, family)
- Dairy/Calcium (e.g., yogurt, dairy, milk).
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction and Synthesis
2.5. Intervention Reporting
2.5.1. Intervention Intensity
- (1)
- Duration of the intervention. This category ranked the length of the intervention using the following scale: 1 = ≤6 weeks, 2 = 6 to 11 weeks, 3 = 12 weeks to 5 months, 4 = 6 to 12 months, and 5 = ≥12 months.
- (2)
- Frequency of contact with the intervention. This characteristic assessed the frequency of contact between participants and the intervention. If the intervention employed multiple points of contact, an average contact score was computed. If the frequency of contact was not clearly stated by authors, the points of contact were divided by the overall duration of the intervention to determine an average frequency of contact. The ranking score that was used for frequency of contact with the intervention was 1 = annually, 2 = bimonthly to quarterly, 3 = monthly, 3.5 = twice a month, 4 = weekly, 4.5 = multiple times per week, and 5 = daily.
- (3)
- Level of personalization. This characteristic describes the type and/or level of contact with the intervention. The ranking score used for the level of personalization included: 1 = environmental, 2 = group (parent or child), 2.5 = group (parent and child), 3 = environmental and group (parent or child), 3.5 = environmental and group (parent and child), 4 = group with an individual component (parent or child), 4.5 = group with an individual component (parent and child), and 5 = individual (parent and/or child) or individual, environmental, and group (parent and/or child). If the parent and child experienced different levels of personalization, they were scored independently, and the scores were averaged for a total personalization score out of 5. The more personalized the contact of the intervention, the higher the intensity score.
- (4)
- Reach of the intervention strategies. This characteristic assessed the number of different settings (i.e., home, school) used by the researchers to reach their target audience, and used a scale where 1 = one setting, 3 = two settings, and 5 = three or more settings. The greater number of settings used with the intervention, the higher the intensity of the intervention.
2.5.2. Behavior Change Techniques
2.5.3. WIDER Recommendations
- (1)
- The first recommendation addresses the description of the intervention(s) and the level of detail reported by authors. There are eight supplementary recommendations required for discussion throughout the intervention study, including the characteristics of those delivering the intervention, characteristics of the recipients, setting, mode of intervention delivery, intensity, duration, adherence to delivery protocols, and a detailed description of the intervention content for each study group.
- (2)
- The second recommendation addresses the change process employed in the intervention and the design of the intervention. This recommendation requires a description of how the intervention was developed, the behavior change techniques used in the intervention, and the behavioral processes being targeted by the change techniques.
- (3)
- The third recommendation addresses the extent to which the intervention protocols and/or manuals are accessible, as authors must provide easy access to the protocols/manuals for the interventions as supplementary materials (i.e., online).
- (4)
- The fourth recommendation assesses the control group and the control conditions. Authors must describe the characteristics of the interveners delivering the control, characteristics of the control participants, setting, mode of delivery, intensity, duration, compliance to the delivery protocols, and a detailed description of the control content.
2.6. Quality Criteria
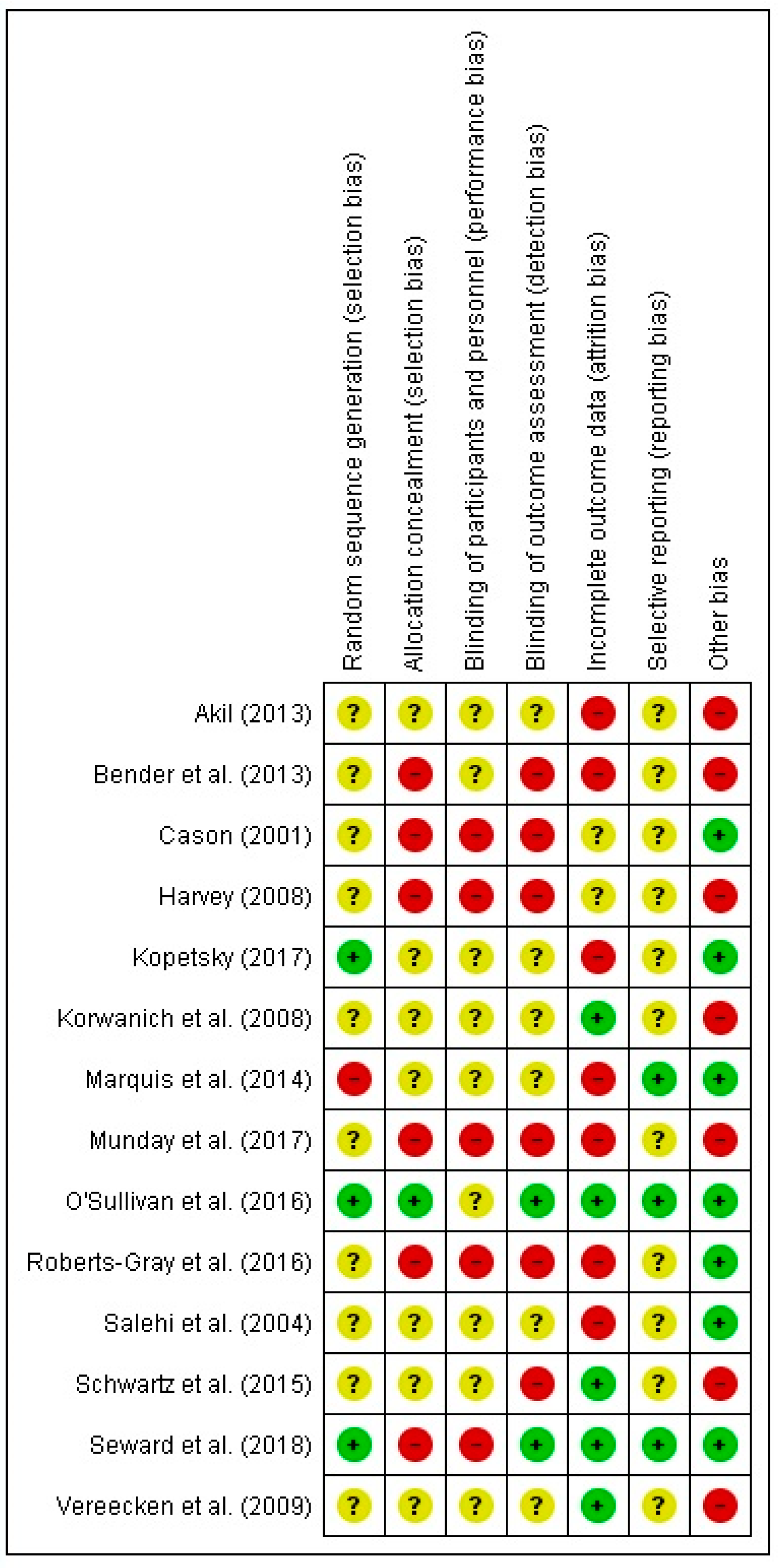
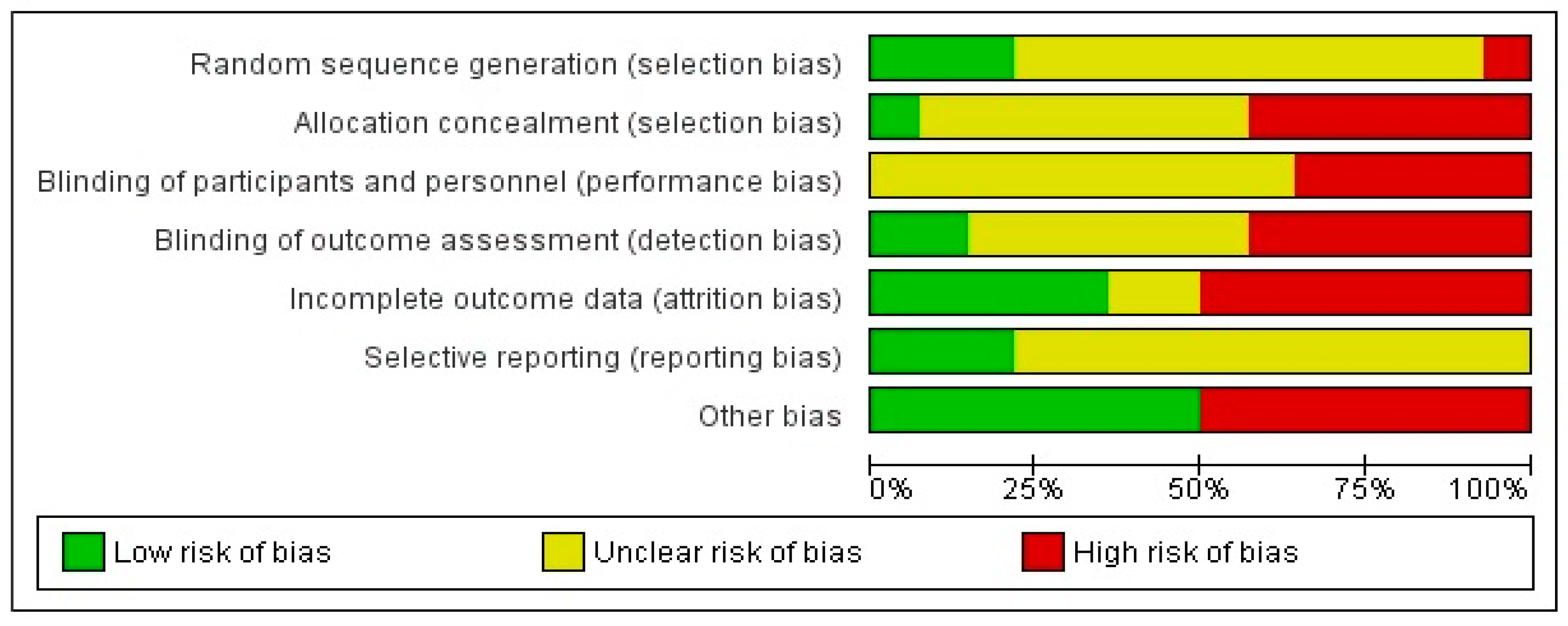
2.6.1. Risk of Bias
- (1)
- Selection bias: assessed two domains: sequence generation and allocation concealment
- (2)
- Performance bias: assessed the blinding procedures implemented in the study
- (3)
- Detection bias: assessed the adequacy of the blinding of outcome assessors
- (4)
- Attrition bias: assessed all the participant withdrawal from the study that lead to incomplete outcome data
- (5)
- Reporting bias: identified the selective reporting of results
- (6)
- Other bias: identified any other sources of bias that may be present in the literature, owing to a variety of circumstances or events.
2.6.2. GRADE
- (1)
- Type of evidence. Scientific evidence derived from randomized control trials begins at a rating of four points; in contrast, evidence from observational studies is assigned a rating of two.
- (2)
- Quality points. A total of three points can be deducted under this category based on inadequacies in follow-up procedures, sparse data, blinding, allocation concealment, and attrition.
- (3)
- Consistency. Heterogeneous studies are evaluated under this category, as long as they all address the same outcomes and interventions. A quality point is deducted under this category for inconsistent results between studies while, in contrast, a quality point is added if a dose-response effect is observed or if adjustment of confounders increased the effect size.
- (4)
- Directness. A maximum of two points can be deducted for issues affecting the generalizability of the results to the population of interest. Examples of issues affecting directness include co-interventions that are being tested alongside the intervention of interest, as well as the use of samples that are either too broad or too restricted.
- (5)
- Effect Size. The GRADE criteria add a quality point for an odds ratio (OR) or relative risk (RR) ≥2 and adds two quality points for an OR or RR ≥5. One quality point is added for effect sizes >2 (or <0.5), while two quality points are added for effect sizes that are >5 (or <0.2) and are all statistically significant. No quality points are added for effect sizes <2 or statistically insignificant results.
3. Results
3.1. Intervention Studies
3.1.1. Study Description
3.1.2. Effectiveness
3.1.3. Sample Size, Control Groups, Effect Size
3.2. Intervention Intensity
3.3. Behavior Change Techniques
3.4. WIDER
3.5. Risk of Bias
3.6. GRADE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canadian Dairy Commission. Available online: http://www.cdc-ccl.gc.ca/CDC/index-eng.php?id=3805 (accessed on 2 November 2018).
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Garriguet, D. Nutrition: Findings from the Canadian Community Health Survey. Overview of Canadians’ Eating Habits. Available online: www.statcan.gc.ca/pub/82-620-m/82-620-m2006002-eng.pdf (accessed on 2 November 2018).
- Nielsen, S.J.; Popkin, B.M. Changes in beverage intake between 1977 and 2001. Am. J. Prev. Med. 2004, 27, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. Dairy product intake in children and adolescents in developed countries: Trends, nutritional contribution, and a review of association with health outcomes. Nutr. Rev. 2014, 72, 68–81. [Google Scholar] [CrossRef]
- Rizzoli, R. Dairy products, yogurts, and bone health. Am. J. Clin. Nutr. 2014, 99, 1256S–1262S. [Google Scholar] [CrossRef]
- Tremblay, A.; Gilbert, J.A. Human obesity: Is insufficient calcium/dairy intake part of the problem? J. Am. Coll. Nutr. 2011, 30, 449S–453S. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Troy, L.M.; Rogers, G.T.; Fox, C.S.; McKeown, N.M.; Meigs, J.B.; Jacques, P.F. Longitudinal association between dairy consumption and changes of body weight and waist circumference: The Framingham Heart Study. Int. J. Obes. 2014, 38, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, T.A.; Qu, H.; Hughes, S.O.; He, M.; Wagner, S.E.; Foushee, H.R.; Shewchuk, R.M. Self-perceived lactose intolerance results in lower intakes of calcium and dairy foods and is associated with hypertension and diabetes in adults. Am. J. Clin. Nutr. 2011, 94, 191–198. [Google Scholar] [CrossRef]
- O’Connor, L.M.; Lentjes, M.A.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Forouhi, N.G. Dietary dairy product intake and incident type 2 diabetes: A prospective study using dietary data from a 7-day food diary. Diabetologia 2014, 57, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Bergkvist, L.; Rutegård, J.; Giovannucci, E.; Wolk, A. Calcium and dairy food intakes are inversely associated with colorectal cancer risk in the cohort of Swedish men. Am. J. Clin. Nutr. 2006, 83, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.; Christoffel, K.K. Obesity in preschool and school-age children: Treatment early and often may be best. Arch. Pediatr. Adolesc. Med. 1994, 148, 1257–1261. [Google Scholar] [CrossRef]
- Skinner, J.D.; Carruth, B.R.; Bounds, W.; Ziegler, P.; Reidy, K. Do food-related experiences in the first 2 years of life predict dietary variety in school-aged children? J. Nutr. Educ. Behav. 2002, 34, 310–315. [Google Scholar] [CrossRef]
- Marshall, T.A.; Eichenberger Gilmore, J.M.; Broffitt, B.; Stumbo, P.J.; Levy, S.M. Diet quality in young children is influenced by beverage consumption. J. Am. Coll. Nutr. 2005, 24, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K. Regular sugar-sweetened beverage consumption between meals increases risk of overweight among preschool-aged children. J. Am. Diet. Assoc. 2007, 107, 924–934. [Google Scholar] [CrossRef]
- Yen, S.T.; Lin, B.H. Beverage consumption among US children and adolescents: Full-information and quasi maximum-likelihood estimation of a censored system. Eur. Rev. Agric. Econ. 2002, 29, 85–103. [Google Scholar] [CrossRef]
- Hendrie, G.A.; Brindal, E.; Baird, D.; Gardner, C. Improving children’s dairy food and calcium intake: Can intervention work? A systematic review of the literature. Public Health Nutr. 2012, 16, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Marquez, O.; Racey, M.; Preyde, M.; Hendrie, G.A.; Newton, G. Interventions to increase dairy consumption in adolescents: A systematic review. Infant Child Adolesc. Nutr. 2015, 7, 242–254. [Google Scholar] [CrossRef]
- Cason, K.L. Evaluation of a preschool nutrition education program based on the theory of multiple intelligences. J. Nutr. Educ. 2001, 33, 161–164. [Google Scholar] [CrossRef]
- Seward, K.; Wolfenden, L.; Finch, M.; Wiggers, J.; Wyse, R.; Jones, J.; Yoong, S.L. Improving the implementation of nutrition guidelines in childcare centres improves child dietary intake: Findings of a randomised trial of an implementation intervention. Public Health Nutr. 2018, 21, 607–617. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Tugwell, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Akil, N. Evaluation of Effectiveness of Classroom-Based Nutrition Intervention on Changes in Eating Behavior in African American Parents/Caregivers and Their Children. Master’s Thesis, Wayne State University, Detroit, MI, USA, 2013. Available online: https://digitalcommons.wayne.edu/oa_theses/224 (accessed on 25 June 2018).
- Bender, M.S.; Nader, P.R.; Kennedy, C.; Gahagan, S. A culturally appropriate intervention to improve health behaviours in Hispanic mother-child dyads. Child. Obes. 2013, 9, 157–163. [Google Scholar] [CrossRef]
- Harvey, S.P. The Results of a Home-Based Physical Activity and Nutrition Program of Preschool Children and Parent Perceptions of Barriers. Ph.D. Thesis, University of Kansas, Lawrence, KS, USA, 2008. [Google Scholar]
- Kopetsky, A. A Healthy Snacking Intervention in Preschool-Aged Children. Master’s Thesis, University of Delaware, Newark, DE, USA, 2017. [Google Scholar]
- Korwanich, K.; Sheiham, A.; Srisuphan, W.; Srisilapanan, P. Promoting healthy eating in nursery schoolchildren: A quasi-experimental intervention study. Health Educ. J. 2008, 67, 16–30. [Google Scholar] [CrossRef]
- Marquis, G.S.; Colecraft, E.K. Community interventions for dietary improvement in Ghana. Food Nutr. Bull. 2014, 35, S193–S197. [Google Scholar] [CrossRef] [PubMed]
- Munday, K.; Wilson, M. Implementing a health and wellbeing programme for children in early childhood: A preliminary study. Nutrients 2017, 9, 1031. [Google Scholar] [CrossRef]
- O’Sullivan, A.; Fitzpatrick, N.; Doyle, O. Effects of early intervention on dietary intake and its mediating role on cognitive functioning: A randomised controlled trial. Public Health Nutr. 2016, 20, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Roberts-Gray, C.; Briley, M.E.; Ranjit, N.; Byrd-Williams, C.E.; Sweitzer, S.J.; Sharma, S.V.; Palafox, M.R.; Hoelscher, D.M. Efficacy of the Lunch is in the Bag intervention to increase parents’ packing of healthy bag lunches for young children: A cluster-randomized trial in early care and education centers. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Kimiagar, S.M.; Shahbazi, M.; Mehrabi, Y.; Kolahi, A.A. Assessing the impact of nutrition education on growth indices of Iranian nomadic children: An application of a modified beliefs, attitudes, subjective-norms and enabling-factors model. Br. J. Nutr. 2004, 91, 779–787. [Google Scholar] [CrossRef]
- Schwartz, M.B.; O’Connell, M.; Henderson, K.E.; Middleton, A.E.; Scarmo, S. Testing variations on family-style feeding to increase whole fruit and vegetable consumption among preschoolers in child care. Child. Obes. 2015, 11, 499–505. [Google Scholar] [CrossRef]
- Vereecken, C.; Huybrechts, I.; van Houte, H.; Martens, V.; Wittebroodt, I.; Maes, L. Results from a dietary intervention study in preschools “Beastly Healthy at School”. Int. J. Public Health 2009, 54, 142–149. [Google Scholar] [CrossRef]
- Racey, M.; O’Brien, C.; Douglas, S.; Marquez, O.; Hendrie, G.; Newton, G. Systematic Review of School-Based Interventions to Modify Dietary Behavior: Does Intervention Intensity Impact Effectiveness? J. Sch. Health 2016, 86, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Abraham, C.; Michie, S. A Taxonomy of Behavior Change Techniques Used in Interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, L.; Archibald, M.; Arseneau, D.; Scott, S.D. Development of a checklist to assess the quality of reporting of knowledge translation interventions using the Workgroup for Intervention Development and Evaluation Research (WIDER) recommendations. Implement. Sci. 2013, 8, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.; Albrecht, L.; O’Leary, K.; Ball, G.; Hartling, L.; Hofmeyer, A.; Dryden, D. Systematic review of knowledge translation strategies in the allied health professions. Implement. Sci. 2012, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://handbook-5-1.cochrane.org/ (accessed on 15 January 2018).
- What Is GRADE? Available online: http://clincialevidence.bmj.com/x/set/static/ebm/learn/665072.html (accessed on 15 January 2018).
- Hawkins, R.P.; Kreuter, M.; Resnicow, K.; Fishbein, M.; Dijkstra, A. Understanding tailoring in communicating about health. Health Educ. Res. 2008, 23, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Grimm, G.C.; Harnack, L.; Story, M. Factors associated with soft drink consumption in school-aged children. J. Am. Diet. Assoc. 2004, 104, 1244–1249. [Google Scholar] [CrossRef]
- Watterworth, J.; Mackay, J.M.; Buchholz, A.C.; Darlington, G.; Randall Simpson, J.; Ma, D.W.L.; Haines, J.; Guelph Family Health Study. Food parenting practices and their associations with child nutrition risk status: Comparing mothers and fathers. Appl. Physiol. Nutr. Metab. 2017, 42, 667–671. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Development of eating behaviours among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef]
- Hanson, N.I.; Neumark-Sztainer, D.; Eisenberg, M.E.; Story, M.; Wall, M. Associations between parental report of the home food environment and adolescent intakes of fruits, vegetables and dairy foods. Public Health Nutr. 2005, 8, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Kratt, P.; Reynolds, K.; Shewchuk, R. The role of availability as a moderator of family fruit and vegetable consumption. Health Educ. Behav. 2000, 27, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Tunis, S.R.; Clarke, M.; Gorst, S.L.; Gargon, E.; Blazeby, J.M.; Altman, D.G.; Williamson, P.R. Improving the relevance and consistency of outcomes in comparative effectiveness research. J. Comp. Eff. Res. 2016, 5, 193–205. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Population | Description of Intervention (I = Intervention, C = Control) | Outcome Measure (s) | Intervention Outcome Measurement (s) | Effect Size (d) | Effective (Y/N) 1 |
|---|---|---|---|---|---|---|
| Akil (2013) [22] | Parents or caregivers of children aged 3 to 5 (n = 140) | I: Parents/caregivers and child followed ordinary HeadStart nutrition curriculum and participated in a nutrition education program (i.e., cooking classes, weekly nutrition newsletters) | Daily number of servings of food groups (i.e., dairy, fruits, and vegetables) | N/A. Study does not report pre/post-intervention consumption. | ND 2 | N |
| C: Parents/caregivers and children followed ordinary HeadStart nutrition curriculum | ||||||
| Bender et al. (2013) [23] | Low income Hispanic mothers (18–35 years old) with children aged 3 to 5 (n = 33) | I: Two-phase intervention program; phase I included four biweekly interactive nutrition group lessons, and phase II included six monthly group community activities to reinforce target health behaviors (i.e., nutrition cooking classes) | Beverage (i.e., fruit juice, milk) serving size(s) and number of servings/day | Children’s baseline milk consumption in ounces per day (mean (SD)): 14.3 (0.96) Post-intervention milk consumption in ounces per day (mean (SD)): 16.8 (2.1) | ND | N |
| Cason (2001) [19] | Children aged 3 to 5 (male = 2990, female = 3112) | I: Children participated in a multiple intelligences theory-based nutrition education curriculum (i.e., nutrition education lessons, food tasting) | Daily number of food group servings (i.e., meat, dairy, fruit) | Reported difference in daily servings of dairy in children as mean (SD). Pre-intervention was 0.99 (1.32) and post-intervention was 2.36 (1.54). | ND | Y |
| Harvey (2008) [24] | Low-income African-American and Hispanic parents (n = 25) | I: Parents participated in a weekly nutrition education intervention; they received weekly nutrition newsletters and tracked child daily dietary servings using a kid calendar | Weekly servings for dietary components (i.e., dairy, fruits, vegetables) | Reported changes in weekly servings of low-fat dairy as mean (SD). Baseline measure was 12.44 (7.10) and week 4 post-intervention was 18.04 (7.55). | ND | Y |
| Children aged 3 to 5 (female = 13, male = 12) | ||||||
| Kopetsky (2017) [25] | Parent/caregiver (female = 7) | I: Parent and child attended five, 45-min nutrition education sessions on behavioral strategies (self-monitoring, parental modeling), attended education sessions on MyPlate food groups, and received weekly recipes in the mail | Dietary quality as measured by the Healthy Eating Index (HEI), 2010 | HEI 2010 scores quality of dairy in the diet out of 10 points. Baseline and week 5 for dairy consumption (mean (SD)): Baseline: 8.2 (2.5) Week 5: 8.9 (2.0) | 0.04 | N |
| Children aged 3 to 5 (male = 3, female = 3) | C: Parent and child received weekly recipes in the mail | |||||
| Korwanich et al. (2008) [26] | Parents (n = 219) | I: Nursery schools had implemented a newly developed healthy eating policy (i.e., advising on snack and beverage consumption at school, children engaged in nutrition education activities) | Frequency of dietary intakes per day (i.e., non-sugar milk, fresh fruit) | Frequency of non-sugar milk consumption within groups (mean (SD)). Baseline in intervention group was 0.94 (0.2) and post-intervention was 0.97 (0.2). | 0.17 | N |
| Children aged 4 to 5 years (male = 111, female = 108) | C: No action provided in control schools | |||||
| Marquis et al. (2014) [27] | Parent/caregiver (n = 201) | I: Parents/caregivers attended weekly meetings for loan payments, entrepreneurship training, and nutrition education on child feeding practices | Frequency of dietary intakes per week (i.e., milk and milk products) | N/A. Study does not report pre/post-intervention consumption. | ND | Y |
| C: Parents/caregivers received health education talks | ||||||
| Munday et al. (2017) [28] | Parents/caregivers (n = 16) | I: Children participated in nutrition education sessions, food tasting sessions, sticker reward charts, kindergarten vegetable plots; parents/caregivers participated in cooking classes | Nutrient intake per day (i.e., calcium) | Reported calcium intakes as mean (SD). Baseline intake was 526 (198.4) and post-intervention was 608 (196.2). | ND | Y |
| Children aged 3 to 5 (male = 13, female = 4) | ||||||
| O’Sullivan et al. (2016) [29] | Mothers of children aged 3 to 5 (n = 149) | I: Mothers received a community-based home visiting program (i.e., provided information and instruction on parenting practice, emotional support, and access to community services), participated in the Triple P Positive Parenting Program, received child developmental materials and book packs, and were encouraged to attend healthy eating workshops | Proportion of participants meeting daily recommendations (i.e., dairy) | Intakes reported as proportion of participants in the intervention group meeting daily dairy recommendations (mean (SD)). Proportions at each of 18, 24, and 36 months were 0.74 (±0.44), 0.64 (±0.48), and 0.66 (±0.48), respectively. | 1.16 to 1.94 | N |
| Children aged 3 to 5 (n = 149) | C: Mothers received child developmental materials and book packs, and were encouraged to attend healthy eating workshops | |||||
| Roberts-Gray et al. (2016) [30] | Parent–child dyads (n = 608) | I: Parents received nutrition newsletters and participated in parent–child activity stations; children participated in parent–child activity stations and teacher–child classroom activities; nutrition workshops implemented at the organizational level | Number of dairy servings per day | Number of dairy servings per day (mean (SD)): pre-intervention 0.73 (0.7) and post-intervention 0.79 (0.07). | 0.86 | N |
| C: No action provided in control schools | ||||||
| Salehi et al. (2004) [31] | Parents or caregivers of children <5 years of age | I: Parents/caregivers were exposed to an educational program (i.e., educated on concepts of “food pyramid”, taught daily requirements for milk and yogurt intakes) | Quantity of milk consumed (grams) | Reported quantity (g) of milk consumption at beginning of program compared to end. Beginning milk quantity (g) reported as mean (SD) was 50 (13.2), and end was 60 (9.5). | ND | N/A |
| Children aged 3 to 5 (n = 811) | C: No action provided in control sub-tribes | |||||
| Schwartz et al. (2015) [32] | Children aged 3 to 5 (male = 40, female = 45) | I: Children were exposed to one of two feeding practices: (1) fruits, vegetables, and milk were served before the main meal (first course), and (2) fruits, vegetables, and milk were served before the main meal, and meats and grains were removed from the table after the first serving (combination) | Number of Child and Adult Care Food Program (CACFP) servings consumed per meal per day (i.e., milk) | N/A. Not reported as overall pre/post-test consumption. | −0.09 to 0.64 | Y |
| Seward et al. (2018) [20] | Long day childcare services (n = 44) | I: Services were provided to staff, including training, receiving a resource pack to support the implementation of nutrition guidelines, having a dietitian complete an audit of the two-week menus, and being allocated an implementation support officer to provide advice and assistance | Number of dietary servings per day (i.e., dairy) | Reported as mean number of daily dairy servings consumed by children as mean (SD). Baseline was 0.55 (0.23) and post-intervention was 1.03 (0.57). | 0.03 | N |
| Children aged 3 to 5 (n = 243) | C: Services posted a hard copy of the Caring for Children resource and received regular care from the local health district health promotion staff | |||||
| Vereecken et al. (2009) [33] | Parents (mother = 189, father = 11) | I: Children participated in guided and self-guided nutrition activities, were given feedback and reinforcement from teachers, and had access to cooking equipment and healthy foods; parents received nutrition newsletters, engaged in nutrition activities with children, and attended school activities with other parents | Average daily consumption of milk products (mL) | Reported changes in milk intakes in mL. Pre-intervention was 176 mL, and post-intervention was 153 mL. No SD reported. | −2.17 | N |
| Children aged 3 to 5 (male = 239, female = 237) | C: No action provided in control schools |
| Effective Interventions | Ineffective Interventions | Total 3 | % Effective 1 | |
|---|---|---|---|---|
| Target of Intervention | ||||
| Mixed | 5 | 8 | 13 | 38.5 |
| Intervention Intensity | ||||
| Low | 2 | 1 | 3 | 66.7 |
| Medium | 3 | 2 | 5 | 60.0 |
| High | 0 | 5 | 5 | 0.0 |
| Duration | ||||
| <6 weeks | 2 | 2 | 4 | 50.0 |
| 6 to 11 weeks | 1 | 0 | 1 | 100.0 |
| 12 weeks to 5 months | - | - | - | - |
| 6 to 12 months | 1 | 5 | 6 | 16.7 |
| >12 months | 1 | 1 | 2 | 50.0 |
| Frequency of Contact 2 | ||||
| Annually | - | - | - | - |
| Bimonthly to quarterly | - | - | - | - |
| Monthly | 0 | 2 | 2 | 0.0 |
| Biweekly | 1 | 2 | 3 | 33.3 |
| Weekly | 2 | 5 | 7 | 28.6 |
| Multiple times per week | 2 | 0 | 2 | 100.0 |
| Daily | - | - | - | - |
| Level of Personalization 2 | ||||
| Environmental | 1 | 1 | 2 | 50.0 |
| Group (Parent or Child) | 3 | 3 | 6 | 50.0 |
| Group (Parent and Child) | - | - | - | - |
| Environmental + Group (Parent or Child) | 1 | 1 | 2 | 50.0 |
| Environmental + Group (Parent and Child) | 0 | 2 | 2 | 0.0 |
| Group + Individual (Parent or Child) | 1 | 1 | 2 | 50.0 |
| Group + Individual (Parent and Child) | 0 | 1 | 1 | 0.0 |
| Individual or Individual + Environmental + Group | 0 | 2 | 2 | 0.0 |
| Reach | ||||
| 1 setting | 5 | 1 | 6 | 83.3 |
| 2 settings | 0 | 5 | 5 | 0.0 |
| 3+ settings | 0 | 2 | 2 | 0.0 |
| Study (n = 14) | Duration 4 | Frequency 4 | Personalization 4 | Reach 4 | Overall Intensity Score | Overall Intensity Rating 2 | Effective 3 | Group Score |
|---|---|---|---|---|---|---|---|---|
| Parent and Child | ||||||||
| Akil (2013) [22] | 4 | 4 | 3 | 5 | 16 | High | N | 13.5 |
| Bender et al. (2013) [23] | 4 | 3.25 | 2.5 | 5 | 14.75 | High | N | |
| Kopetsky (2017) [25] | 1 | 4 | 4.5 | 3 | 12.5 | Medium | N | |
| Korwanich et al. (2008) [26] | 4 | 4 1 | 3.5 | 3 | 14.5 | High | N | |
| Munday et al. (2017) [28] | 2 | 4.5 | 3 | 1 | 10.5 | Medium | Y | |
| Roberts-Gray et al. (2016) [30] | 1 | 4 | 3.5 | 3 | 11.5 | Medium | N | |
| Vereecken et al. (2009) [33] | 4 | 4 1 | 3.5 | 3 | 14.5 | High | N | |
| Parent | ||||||||
| Harvey (2008) [24] | 1 | 4 | 2 | 1 | 8 | Low | Y | 12.2 |
| Marquis et al. (2014) [27] | 5 | 4 | 2 | 1 | 12 | Medium | Y | |
| Salehi et al. (2004) [31] | 4 | N/A | Unclear | 1 | N/A | N/A | N/A | |
| O’Sullivan et al. (2016) [29] | 5 | 3.5 | 5 | 3 | 16.5 | High | N | |
| Child | ||||||||
| Cason (2001) [19] | 4 | 3.5 | 3 | 1 | 11.5 | Medium | Y | 9.5 |
| Schwartz et al. (2015) [32] | 1 | 4.5 | 1 | 1 | 7.5 | Low | Y | |
| Childcare Services | ||||||||
| Seward et al. (2018) [20] | 4 | 3 | 1 | 1 | 9 | Low | N | 9 |
| Behavior Change Technique 1 | Effective (N = 5) | Ineffective (N = 8) | Total (N = 13) 2 | % Effective 3 |
|---|---|---|---|---|
| 1. Provide information on consequences of behavior in general | 3 | 5 | 8 | 37.5 |
| 2. Provide information on consequences of behavior to the individual | 3 | 6 | 9 | 33.3 |
| 4. Provide normative information about others’ behavior | 1 | 0 | 1 | 100.0 |
| 5. Goal setting (behavior) | 4 | 8 | 12 | 33.3 |
| 7. Action planning | 5 | 8 | 13 | 38.5 |
| 8. Problem solving/barrier identification | 2 | 3 | 5 | 40.0 |
| 9. Set graded tasks | 0 | 1 | 1 | 0.0 |
| 10. Review of behavioral goals | 1 | 4 | 5 | 20.0 |
| 13. Rewards contingent on successful behaviors | 2 | 2 | 4 | 50.0 |
| 15. Generalization of target behavior | 4 | 7 | 11 | 36.4 |
| 16. Self-monitoring of behavior | 1 | 3 | 4 | 25.0 |
| 19. Provide feedback on performance | 1 | 6 | 7 | 14.3 |
| 20. Provide information on when and where to perform the behavior | 4 | 8 | 12 | 33.3 |
| 21. Provide instruction on how to perform the behavior | 4 | 8 | 12 | 33.3 |
| 22. Model/demonstrate the behavior | 3 | 7 | 10 | 30.0 |
| 23. Teach to use prompts/cues | 4 | 3 | 7 | 57.1 |
| 24. Environmental restructuring | 5 | 3 | 8 | 62.5 |
| 25. Agree on behavioral contract | 0 | 1 | 1 | 0.0 |
| 26. Prompt practice | 4 | 8 | 12 | 33.3 |
| 27. Use of follow-up prompts | 0 | 2 | 2 | 0.0 |
| 28. Facilitate social comparison | 0 | 2 | 2 | 0.0 |
| 29. Plan social support/social change | 2 | 8 | 10 | 20.0 |
| 30. Identification as a role model | 2 | 7 | 9 | 22.2 |
| 35. Relapse prevention/coping planning | 0 | 1 | 1 | 0.0 |
| 36. Stress management/emotional control training | 0 | 1 | 1 | 0.0 |
| 38. Time management | 0 | 1 | 1 | 0.0 |
| 39. General communication skills training | 1 | 2 | 3 | 33.3 |
| Study (n = 14) | Description of Intervention | Classification of Change Process and Design Principles | Access to Intervention Manuals and/or Protocols | Description of Active Control Conditions |
|---|---|---|---|---|
| Akil (2013) [22] | N | N | N | N |
| Bender et al. (2013) [23] | Y | Y | N | No Control Group |
| Cason (2001) [19] | N | Y | N | No Control Group |
| Harvey (2008) [24] | N | N | N | No Control Group |
| Kopetsky (2017) [25] | Y | Y | N | Y |
| Korwanich et al. (2008) [26] | N | N | N | No Active Control |
| Marquis et al. (2014) [27] | Y | N | Y | No Active Control |
| Munday et al. (2017) [28] | Y | N | N | No Control Group |
| O’Sullivan et al. (2016) [29] | Y | Y | Y | No Active Control |
| Roberts-Gray et al. (2016) [30] | Y | Y | N | No Active Control |
| Salehi et al. (2004) [31] | N | Y | N | No Active Control |
| Schwartz et al. (2015) [32] | N | N | N | No Active Control |
| Seward et al. (2018) [20] | Y | Y | Y | Y |
| Vereecken et al. (2009) [33] | N | Y | N | No Active Control |
| GRADE Criteria | Rating | Support for Judgment | Overall Quality of Evidence |
|---|---|---|---|
| Type of Evidence | +4 | All of the studies included were intervention studies. | High |
| Quality Points | −3 | Multiple studies had <200 participants. The majority of studies had a high or unclear risk of bias for the blinding and allocation process, as well as attrition. | Low |
| Consistency | 0 | Most of the studies reported the ineffectiveness (n = 5) versus effectiveness (n = 2) of dairy intervention. Dairy outcomes assessed are relatively similar, as the majority of studies reported some variation of the number of servings of dairy consumed. | Moderate |
| Directness | −1 | Generalizability of population was a limitation in several studies. | Moderate |
| Effect Size | 0 | n = 3 studies did not provide enough information to allow for the calculation of effect size. All of the other studies (n = 4) allowed for the calculation of effect size; not all of the effect sizes were >2 or <0.5 and significant. | Low |
| Overall Score: 0 | Overall Quality of Evidence: Very Low |
| GRADE Criteria | Rating | Support for Judgment | Overall Quality of Evidence |
|---|---|---|---|
| Type of Evidence | +4 | All of the studies included were intervention studies. | High |
| Quality Points | −1 | All of the studies had a high or unclear risk of bias for blinding and allocation. Three studies had a low risk of attrition bias, with the other three studies having either a high or unclear risk of attrition bias. Generally, sparse data does not appear to be of concern, as the majority of studies had >200 participants. | Moderate |
| Consistency | −1 | Most studies reported ineffectiveness (n = 3) versus effectiveness (n = 2) of dairy intervention, with one study not reporting effectiveness. Variability in reporting of milk outcomes; studies reported volumes of milk consumed, times consumed per day, or quantity of milk consumed in grams. | Low |
| Directness | −1 | Generalizability of population was a limitation in multiple studies. | Moderate |
| Effect Size | 0 | n = 3 studies did not provide enough information to allow for the calculation of effect size. All of the other studies (n = 3) allowed for the calculation of effect size; not all of the effect sizes were >2 or <0.5 and significant. | Low |
| Overall Score: 1 | Overall Quality of Evidence: Very Low |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srbely, V.; Janjua, I.; Buchholz, A.C.; Newton, G. Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review. Nutrients 2019, 11, 714. https://doi.org/10.3390/nu11040714
Srbely V, Janjua I, Buchholz AC, Newton G. Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review. Nutrients. 2019; 11(4):714. https://doi.org/10.3390/nu11040714
Chicago/Turabian StyleSrbely, Victoria, Imtisal Janjua, Andrea C. Buchholz, and Genevieve Newton. 2019. "Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review" Nutrients 11, no. 4: 714. https://doi.org/10.3390/nu11040714
APA StyleSrbely, V., Janjua, I., Buchholz, A. C., & Newton, G. (2019). Interventions Aimed at Increasing Dairy and/or Calcium Consumption of Preschool-Aged Children: A Systematic Literature Review. Nutrients, 11(4), 714. https://doi.org/10.3390/nu11040714