Long-Term Whole Grain Wheat and Rye Intake Reflected by Adipose Tissue Alkylresorcinols and Breast Cancer: A Case-Cohort Study

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
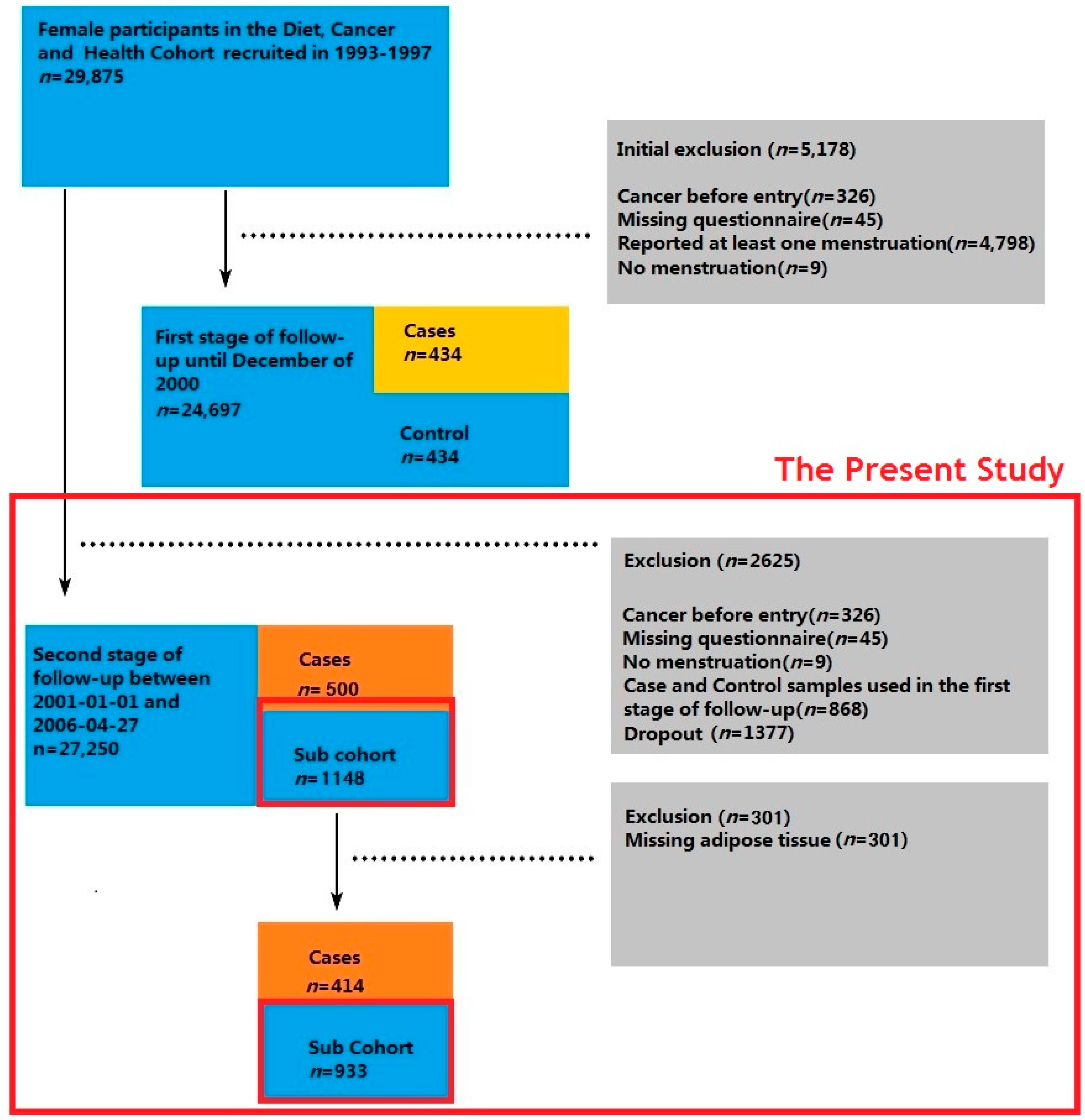
2.1. Study Population and Breast Cancer Incidence
2.2. Case Ascertainment and Study Design
2.3. Dietary Assessment
2.4. Analysis of Alkylresorcinol in Adipose Tissue
2.5. Statistical Analysis.
- (1)
- Crude FFQ models: WGRWGW + WGR% + Total energy intake.
- (2)
- Multivariate-adjusted FFQ models: Energy-adjusted WGRWGW (the residual method) + WGR% + Total energy intake + Other breast cancer risk factors.
- (3)
- Crude biomarker models: Total alkylresorcinol concentration in adipose tissue + Alkylresorcinol C17:0/C21:0 ratio in adipose tissue.
- (4)
- Multivariate-adjusted biomarker models: Total alkylresorcinol concentration in adipose tissue + Alkylresorcinol C17:0/C21:0 ratio in adipose tissue + Other breast cancer risk factors.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- McPherson, K.; Steel, C.M.; Dixon, J.M. Breast cancer—Epidemiology, risk factors, and genetics. Br. Med. J. 2000, 321, 624–628. [Google Scholar] [CrossRef]
- Althuis, M.D.; Fergenbaum, J.H.; Garcia-Closas, M.; Brinton, L.A.; Madigan, M.P.; Sherman, M.E. Etiology of Hormone Receptor–Defined Breast Cancer: A Systematic Review of the Literature. Cancer Epidemiol. Biomark. Prev. 2004, 13, 1558–1568. [Google Scholar]
- Jacobs, D.R.; Slavin, J.; Marquart, L. Whole grain intake and cancer: A review of the literature. Nutr. Cancer 1995, 24, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L. Mechanisms for the Impact of Whole Grain Foods on Cancer Risk. J. Am. Coll. Nutr. 2000, 19, 300S–307S. [Google Scholar] [CrossRef] [PubMed]
- Adlercreutz, H. Can rye intake decrease risk of human breast cancer? Food Nutr. Res. 2010, 54, 5231. [Google Scholar] [CrossRef] [PubMed]
- Arts, C.J.; Govers, C.A.; Van den Berg, H.; Blankenstein, M.A.; Thijssen, J.H. Effect of wheat bran on excretion of radioactively labeled estradiol-17 beta and estrone-glucuronide injected intravenously in male rats. J. Steroid Biochem. Mol. Biol. 1992, 42, 103–111. [Google Scholar] [CrossRef]
- Arts, C.J.; de Bie, A.T.; van den Berg, H.; van’t Veer, P.; Bunnik, G.S.; Thijssen, J.H. Influence of wheat bran on NMU-induced mammary tumor development, plasma estrogen levels and estrogen excretion in female rats. J. Steroid Biochem. Mol. Biol. 1991, 39, 193–202. [Google Scholar] [CrossRef]
- Braaten, J.T.; Wood, P.J.; Scott, F.W.; Wolynetz, M.S.; Lowe, M.K.; Bradley-White, P.; Collins, M.W. Oat beta-glucan reduces blood cholesterol concentration in hypercholesterolemic subjects. Eur. J. Clin. Nutr. 1994, 48, 465–474. [Google Scholar] [PubMed]
- Adlercreutz, H.; Mousavi, Y.; Clark, J.; Höckerstedt, K.; Hämäläinen, E.; Wähälä, K.; Mäkelä, T.; Hase, T. Dietary phytoestrogens and cancer: In vitro and in vivo studies. J. Steroid Biochem. Mol. Biol. 1992, 41, 331–337. [Google Scholar] [CrossRef]
- Adlercreutz, H.; Bannwart, C.; Wahala, K.; Makela, T.; Brunow, G.; Hase, T.; Arosemena, P.J.; Kellis, J.T., Jr.; Vickery, L.E. Inhibition of human aromatase by mammalian lignans and isoflavonoid phytoestrogens. J. Steroid Biochem. Mol. Biol. 1993, 44, 147–153. [Google Scholar] [CrossRef]
- Adlercreutz, H. Lignans and human health. Crit. Rev. Clin. Lab. Sci. 2007, 44, 483–525. [Google Scholar] [CrossRef] [PubMed]
- Andersson, A.A.M.; Andersson, R.; Piironen, V.; Lampi, A.-M.; Nyström, L.; Boros, D.; Fraś, A.; Gebruers, K.; Courtin, C.M.; Delcour, J.A.; et al. Contents of dietary fibre components and their relation to associated bioactive components in whole grain wheat samples from the HEALTHGRAIN diversity screen. Food Chem. 2013, 136, 1243–1248. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Åman, P.; Härkönen, H.; Hallmans, G.; Knudsen, K.E.B.; Mazur, W.; Adlercreutz, H. Content of nutrients and lignans in roller milled fractions of rye. J. Sci. Food Agric. 1997, 73, 143–148. [Google Scholar] [CrossRef]
- Pietinen, P.; Stumpf, K.; Männistö, S.; Kataja, V.; Uusitupa, M.; Adlercreutz, H. Serum Enterolactone and Risk of Breast Cancer: A Case-Control Study in Eastern Finland. Cancer Epidemiol. Biomark. Prev. 2001, 10, 339–344. [Google Scholar]
- Boccardo, F.; Lunardi, G.; Guglielmini, P.; Parodi, M.; Murialdo, R.; Schettini, G.; Rubagotti, A. Serum enterolactone levels and the risk of breast cancer in women with palpable cysts. Eur. J. Cancer 2004, 40, 84–89. [Google Scholar] [CrossRef]
- Olsen, A.; Knudsen, K.E.B.; Thomsen, B.L.; Loft, S.; Stripp, C.; Overvad, K.; Møller, S.; Tjønneland, A. Plasma Enterolactone and Breast Cancer Incidence by Estrogen Receptor Status. Cancer Epidemiol. Biomark. Prev. 2004, 13, 2084–2089. [Google Scholar]
- Buck, K.; Zaineddin, A.K.; Vrieling, A.; Linseisen, J.; Chang-Claude, J. Meta-analyses of lignans and enterolignans in relation to breast cancer risk. Am. J. Clin. Nutr. 2010, 92, 141–153. [Google Scholar] [CrossRef]
- Mourouti, N.; Kontogianni, M.D.; Papavagelis, C.; Psaltopoulou, T.; Kapetanstrataki, M.G.; Plytzanopoulou, P.; Vassilakou, T.; Malamos, N.; Linos, A.; Panagiotakos, D.B. Whole Grain Consumption and Breast Cancer: A Case-Control Study in Women. J. Am. Coll. Nutr. 2016, 35, 143–149. [Google Scholar] [CrossRef]
- Farvid, M.S.; Cho, E.; Eliassen, A.H.; Chen, W.Y.; Willett, W.C. Lifetime grain consumption and breast cancer risk. Breast Cancer Res. Treat. 2016, 159, 335–345. [Google Scholar] [CrossRef]
- Terry, P.; Jain, M.; Miller, A.B.; Howe, G.R.; Rohan, T.E. No association among total dietary fiber, fiber fractions, and risk of breast cancer. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1507–1508. [Google Scholar]
- Cho, E.; Spiegelman, D.; Hunter, D.J.; Chen, W.Y.; Colditz, G.A.; Willett, W.C. Premenopausal Dietary Carbohydrate, Glycemic Index, Glycemic Load, and Fiber in Relation to Risk of Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2003, 12, 1153–1158. [Google Scholar]
- Park, Y.; Brinton, L.A.; Subar, A.F.; Hollenbeck, A.; Schatzkin, A. Dietary fiber intake and risk of breast cancer in postmenopausal women: The National Institutes of Health–AARP Diet and Health Study. Am. J. Clin. Nutr. 2009, 90, 664–671. [Google Scholar] [CrossRef]
- Nicodemus, K.K.; Jacobs, D.R.; Folsom, A.R. Whole and refined grain intake and risk of incident postmenopausal breast cancer (United States). Cancer Causes Control 2001, 12, 917–925. [Google Scholar] [CrossRef]
- Deschasaux, M.; Zelek, L.; Pouchieu, C.; His, M.; Hercberg, S.; Galan, P.; Latino-Martel, P.; Touvier, M. Prospective Association between Dietary Fiber Intake and Breast Cancer Risk. PLoS ONE 2013, 8, e79718. [Google Scholar] [CrossRef]
- Cade, J.E.; Burley, V.J.; Greenwood, D.C. Dietary fibre and risk of breast cancer in the UK Women’s Cohort Study. Int. J. Epidemiol. 2007, 36, 431–438. [Google Scholar] [CrossRef]
- Egeberg, R.; Olsen, A.; Loft, S.; Christensen, J.; Johnsen, N.F.; Overvad, K.; Tjonneland, A. Intake of whole grain products and risk of breast cancer by hormone receptor status and histology among postmenopausal women. Int. J. Cancer 2009, 124, 745–750. [Google Scholar] [CrossRef]
- Ferrari, P.; Rinaldi, S.; Jenab, M.; Lukanova, A.; Olsen, A.; Tjønneland, A.; Overvad, K.; Clavel-Chapelon, F.; Fagherazzi, G.; Touillaud, M.; et al. Dietary fiber intake and risk of hormonal receptor–defined breast cancer in the European Prospective Investigation into Cancer and Nutrition study. Am. J. Clin. Nutr. 2013, 97, 344–353. [Google Scholar] [CrossRef]
- Van der Kamp, J.W.; Poutanen, K.; Seal, C.J.; Richardson, D.P. The HEALTHGRAIN definition of ‘whole grain’. Food Nutr. Res. 2014, 58. [Google Scholar] [CrossRef]
- Jonnalagadda, S.S.; Harnack, L.; Hai Liu, R.; McKeown, N.; Seal, C.; Liu, S.; Fahey, G.C. Putting the Whole Grain Puzzle Together: Health Benefits Associated with Whole Grains—Summary of American Society for Nutrition 2010 Satellite Symposium. J. Nutr. 2011, 141, 1011S–1022S. [Google Scholar] [CrossRef]
- Bellisle, F.; Hébel, P.; Colin, J.; Reyé, B.; Hopkins, S. Consumption of whole grains in French children, adolescents and adults. Br. J. Nutr. 2014, 112, 1674–1684. [Google Scholar] [CrossRef]
- Wang, J.-B.; Fan, J.-H.; Dawsey, S.M.; Sinha, R.; Freedman, N.D.; Taylor, P.R.; Qiao, Y.-L.; Abnet, C.C. Dietary components and risk of total, cancer and cardiovascular disease mortality in the Linxian Nutrition Intervention Trials cohort in China. Sci. Rep. 2016, 6, 22619. [Google Scholar] [CrossRef]
- Kyrø, C.; Skeie, G.; Dragsted, L.O.; Christensen, J.; Overvad, K.; Hallmans, G.; Johansson, I.; Lund, E.; Slimani, N.; Johnsen, N.F.; et al. Intake of whole grain in Scandinavia: Intake, sources and compliance with new national recommendations. Scand. J. Public Health 2012, 40, 76–84. [Google Scholar] [CrossRef]
- Nyman, M.; Siljestrom, M.; Pedersen, B.; Bach Knudsen, K.; Asp, N. Dietary fiber content and composition in six cereals at different extraction rates [Wheat, rye, barley, sorghum, rice, and corn]. Cereal Chem. 1984, 61, 14–19. [Google Scholar]
- Nurmi, T.; Nyström, L.; Edelmann, M.; Lampi, A.-M.; Piironen, V. Phytosterols in Wheat Genotypes in the HEALTHGRAIN Diversity Screen. J. Agric. Food Chem. 2008, 56, 9710–9715. [Google Scholar] [CrossRef]
- Baranowski, T. 24-Hour recall and diet record methods. In Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012; pp. 49–69. [Google Scholar]
- Rodrigo, C.P.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food frequency questionnaires. Nutr. Hosp. 2015, 31, 49–56. [Google Scholar]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Landberg, R.; Marklund, M.; Kamal-Eldin, A.; Åman, P. An update on alkylresorcinols—Occurrence, bioavailability, bioactivity and utility as biomarkers. J. Funct. Foods 2014, 7, 77–89. [Google Scholar] [CrossRef]
- Ross, A.B.; Shepherd, M.J.; Schupphaus, M.; Sinclair, V.; Alfaro, B.; Kamal-Eldin, A.; Aman, P. Alkylresorcinols in cereals and cereal products. J. Agric. Food Chem. 2003, 51, 4111–4118. [Google Scholar] [CrossRef]
- Kulawinek, M.; Jaromin, A.; Kozubek, A.; Zarnowski, R. Alkylresorcinols in Selected Polish Rye and Wheat Cereals and Whole-Grain Cereal Products. J. Agric. Food Chem. 2008, 56, 7236–7242. [Google Scholar] [CrossRef]
- Ross, A.B.; Kamal-Eldin, A.; Lundin, E.A.; Zhang, J.X.; Hallmans, G.; Aman, P. Cereal alkylresorcinols are absorbed by humans. J. Nutr. 2003, 133, 2222–2224. [Google Scholar] [CrossRef]
- Landberg, R.; Linko, A.-M.; Kamal-Eldin, A.; Vessby, B.; Adlercreutz, H.; Åman, P. Human Plasma Kinetics and Relative Bioavailability of Alkylresorcinols after Intake of Rye Bran. J. Nutr. 2006, 136, 2760–2765. [Google Scholar] [CrossRef] [PubMed]
- Marklund, M.; Stromberg, E.A.; Laerke, H.N.; Knudsen, K.E.; Kamal-Eldin, A.; Hooker, A.C.; Landberg, R. Simultaneous pharmacokinetic modeling of alkylresorcinols and their main metabolites indicates dual absorption mechanisms and enterohepatic elimination in humans. J. Nutr. 2014, 144, 1674–1680. [Google Scholar] [CrossRef] [PubMed]
- Landberg, R.; Åman, P.; Friberg, L.E.; Vessby, B.; Adlercreutz, H.; Kamal-Eldin, A. Dose response of whole-grain biomarkers: Alkylresorcinols in human plasma and their metabolites in urine in relation to intake. Am. J. Clin. Nutr. 2009, 89, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Jansson, E.; Landberg, R.; Kamal-Eldin, A.; Wolk, A.; Vessby, B.; Aman, P. Presence of alkylresorcinols, potential whole grain biomarkers, in human adipose tissue. Br. J. Nutr. 2010, 104, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Åman, P.; Kamal-Eldin, A. Identification of cereal alkylresorcinol metabolites in human urine—Potential biomarkers of wholegrain wheat and rye intake. J. Chromatogr. B 2004, 809, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Kamal-Eldin, A.; Åman, P. Dietary Alkylresorcinols: Absorption, bioactivities, and possible use as biomarkers of whole-grain wheat—And rye–rich foods. Nutr. Rev. 2004, 62, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Åman, P.; Andersson, R.; Kamal-Eldin, A. Chromatographic analysis of alkylresorcinols and their metabolites. J. Chromatogr. 2004, 1054, 157–164. [Google Scholar] [CrossRef]
- Kristensen, M.; Toubro, S.; Jensen, M.G.; Ross, A.B.; Riboldi, G.; Petronio, M.; Bügel, S.; Tetens, I.; Astrup, A. Whole Grain Compared with Refined Wheat Decreases the Percentage of Body Fat Following a 12-Week, Energy-Restricted Dietary Intervention in Postmenopausal Women. J. Nutr. 2012, 142, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Bruce, S.J.; Blondel-Lubrano, A.; Oguey-Araymon, S.; Beaumont, M.; Bourgeois, A.; Nielsen-Moennoz, C.; Vigo, M.; Fay, L.B.; Kochhar, S.; et al. A whole-grain cereal-rich diet increases plasma betaine, and tends to decrease total and LDL-cholesterol compared with a refined-grain diet in healthy subjects. Br. J. Nutr. 2011, 105, 1492–1502. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Kolehmainen, M.; Mykkänen, H.; Poutanen, K.; Uusitupa, M.; Schwab, U.; Wolk, A.; Landberg, R. Alkylresorcinols in adipose tissue biopsies as biomarkers of whole-grain intake: An exploratory study of responsiveness to advised intake over 12 weeks. Eur. J. Clin. Nutr. 2015, 69, 1244. [Google Scholar] [CrossRef]
- Wu, H.; Mhd Omar, N.A.; Håkansson, N.; Wolk, A.; Michaëlsson, K.; Landberg, R. Evaluation of alkylresorcinols in adipose tissue biopsies as a long-term biomarker of whole-grain wheat and rye intake in free-living Swedish men and women. Public Health Nutr. 2018, 21, 1933–1942. [Google Scholar] [CrossRef]
- Marklund, M.; Landberg, R.; Andersson, A.; Åman, P.; Kamal-Eldin, A. Alkylresorcinol metabolites in urine correlate with the intake of whole grains and cereal fibre in free-living Swedish adults. Br. J. Nutr. 2012, 109, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Guyman, L.A.; Adlercreutz, H.; Koskela, A.; Li, L.; Beresford, S.A.A.; Lampe, J.W. Urinary 3-(3,5-Dihydroxyphenyl)-1-Propanoic Acid, an Alkylresorcinol Metabolite, Is a Potential Biomarker of Whole-Grain Intake in a U.S. Population. J. Nutr. 2008, 138, 1957–1962. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ross, A.B.; Aman, P.; Kamal-Eldin, A. Alkylresorcinols as markers of whole grain wheat and rye in cereal products. J. Agric. Food Chem. 2004, 52, 8242–8246. [Google Scholar] [CrossRef] [PubMed]
- Menzel, C.; Kamal-Eldin, A.; Marklund, M.; Andersson, A.; Åman, P.; Landberg, R. Alkylresorcinols in Swedish cereal food products. J. Food Compost. Anal. 2012, 28, 119–125. [Google Scholar] [CrossRef]
- Linko-Parvinen, A.-M.; Landberg, R.; Tikkanen, M.J.; Adlercreutz, H.; Peñalvo, J.L. Alkylresorcinols from Whole-Grain Wheat and Rye Are Transported in Human Plasma Lipoproteins. J. Nutr. 2007, 137, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Landberg, R.; Kamal-Eldin, A.; Andersson, S.-O.; Johansson, J.-E.; Zhang, J.-X.; Hallmans, G.; Åman, P. Reproducibility of plasma alkylresorcinols during a 6-week rye intervention study in men with prostate cancer. J. Nutr. 2009, 139, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Soderholm, P.P.; Lundin, J.E.; Koskela, A.H.; Tikkanen, M.J.; Adlercreutz, H.C. Pharmacokinetics of alkylresorcinol metabolites in human urine. Br. J. Nutr. 2011, 106, 1040–1044. [Google Scholar] [CrossRef]
- Landberg, R.; Aman, P.; Hallmans, G.; Johansson, I. Long-term reproducibility of plasma alkylresorcinols as biomarkers of whole-grain wheat and rye intake within Northern Sweden Health and Disease Study Cohort. Eur. J. Clin. Nutr. 2013, 67, 259–263. [Google Scholar] [CrossRef]
- Tjønneland, A.; Olsen, A.; Boll, K.; Stripp, C.; Christensen, J.; Engholm, G.; Overvad, K. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: A population-based prospective cohort study of 57,053 men and women in Denmark. Scand. J. Soc. Med. 2007, 35, 432–441. [Google Scholar] [CrossRef]
- Gjerstorff, M.L. The Danish cancer registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, B.; Larsen, O.B. The Danish pathology register. Scand. J. Public Health 2011, 39, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Witt, P.M.; Christensen, J.H.; Schmidt, E.B.; Dethlefsen, C.; Tjønneland, A.; Overvad, K.; Ewertz, M. Marine n-3 polyunsaturated fatty acids in adipose tissue and breast cancer risk: A case–cohort study from Denmark. Cancer Causes Control 2009, 20, 1715. [Google Scholar] [CrossRef] [PubMed]
- Raaschou-Nielsen, O.; Pavuk, M.; Leblanc, A.; Dumas, P.; Philippe Weber, J.; Olsen, A.; Tjonneland, A.; Overvad, K.; Olsen, J.H. Adipose organochlorine concentrations and risk of breast cancer among postmenopausal Danish women. Cancer Epidemiol. Biomark. Prev. 2005, 14, 67–74. [Google Scholar]
- Joensen, A.M.; Overvad, K.; Dethlefsen, C.; Johnsen, S.P.; Tjønneland, A.; Rasmussen, L.H.; Schmidt, E.B. Marine n-3 polyunsaturated fatty acids in adipose tissue and the risk of acute coronary syndrome. Circulation 2011, 124, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Tjonneland, A.; Overvad, K.; Haraldsdottir, J.; Bang, S.; Ewertz, M.; Jensen, O.M. Validation of a semiquantitative food frequency questionnaire developed in Denmark. Int. J. Epidemiol. 1991, 20, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Tjonneland, A.; Haraldsdottir, J.; Overvad, K.; Stripp, C.; Ewertz, M.; Jensen, O.M. Influence of individually estimated portion size data on the validity of a semiquantitative food frequency questionnaire. Int. J. Epidemiol. 1992, 21, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Haraldsdottir, J.; Tjonneland, A.; Overvad, K. Validity of individual portion size estimates in a food frequency questionnaire. Int. J. Epidemiol. 1994, 23, 786–796. [Google Scholar] [CrossRef] [PubMed]
- Helnæs, A.; Kyrø, C.; Andersen, I.; Lacoppidan, S.; Overvad, K.; Christensen, J.; Tjønneland, A.; Olsen, A. Intake of whole grains is associated with lower risk of myocardial infarction: The Danish Diet, Cancer and Health Cohort. Am. J. Clin. Nutr. 2016, 103, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Kyro, C.; Skeie, G.; Dragsted, L.O.; Christensen, J.; Overvad, K.; Hallmans, G.; Johansson, I.; Lund, E.; Slimani, N.; Johnsen, N.F.; et al. Intake of whole grains in Scandinavia is associated with healthy lifestyle, socio-economic and dietary factors. Public Health Nutr. 2011, 14, 1787–1795. [Google Scholar] [CrossRef]
- Slimani, N.; Kaaks, R.; Ferrari, P.; Casagrande, C.; Clavel-Chapelon, F.; Lotze, G.; Kroke, A.; Trichopoulos, D.; Trichopoulou, A.; Lauria, C.; et al. European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study: Rationale, design and population characteristics. Public Health Nutr. 2002, 5, 1125–1145. [Google Scholar] [CrossRef] [PubMed]
- Slimani, N.; Ferrari, P.; Ocke, M.; Welch, A.; Boeing, H.; Liere, M.; Pala, V.; Amiano, P.; Lagiou, A.; Mattisson, I.; et al. Standardization of the 24-h diet recall calibration method used in the European prospective investigation into cancer and nutrition (EPIC): General concepts and preliminary results. Eur. J. Clin. Nutr. 2000, 54, 900–917. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, R.; Wu, H.; Franek, M.; Kamal-Eldin, A.; Landberg, R. Determination of alkylresorcinols and their metabolites in biological samples by gas chromatography–mass spectrometry. J. Chromatogr. B 2015, 1000, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Prentice, R.L. A case-cohort design for epidemiologic cohort studies and disease prevention trials. Biometrika 1986, 73, 1–11. [Google Scholar] [CrossRef]
- Kalbfleisch, J.D.; Lawless, J.F. Likelihood analysis of multi-state models for disease incidence and mortality. Stat. Med. 1988, 7, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, A.; Ohlsson Andersson, Å. Suppressed Sex Hormone Biosynthesis by Alkylresorcinols: A Possible Link to Chemoprevention. Nutr. Cancer 2016, 68, 978–987. [Google Scholar] [CrossRef] [PubMed]
- Kyro, C.; Olsen, A.; Bueno-de-Mesquita, H.B.; Skeie, G.; Loft, S.; Aman, P.; Leenders, M.; Dik, V.K.; Siersema, P.D.; Pischon, T.; et al. Plasma alkylresorcinol concentrations, biomarkers of whole-grain wheat and rye intake, in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Br. J. Nutr. 2014, 111, 1881–1890. [Google Scholar] [CrossRef]
- Nurmi, T.; Mursu, J.; Peñalvo, J.L.; Poulsen, H.E.; Voutilainen, S. Dietary intake and urinary excretion of lignans in Finnish men. Br. J. Nutr. 2009, 103, 677–685. [Google Scholar] [CrossRef]
- Hollænder, P.L.; Ross, A.B.; Kristensen, M. Whole-grain and blood lipid changes in apparently healthy adults: A systematic review and meta-analysis of randomized controlled studies. Am. J. Clin. Nutr. 2015, 102, 556–572. [Google Scholar] [CrossRef]
- Ross, A.B.; Pineau, N.; Kochhar, S.; Bourgeois, A.; Beaumont, M.; Decarli, B. Validation of a FFQ for estimating whole-grain cereal food intake. Br. J. Nutr. 2009, 102, 1547–1551. [Google Scholar] [CrossRef]
- Landberg, R. Alkylresorcinols as Biomarkers of Whole Grain Wheat and Rye Intake; Acta Universitatis Agriculturae Sueciae: Uppsala, Sweden, 2009. [Google Scholar]
- Benz, C.C. Impact of aging on the biology of breast cancer. Crit. Rev. Oncol./Hematol. 2008, 66, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Haraldsdottir, A.; Torfadottir, J.E.; Valdimarsdottir, U.A.; Adami, H.-O.; Aspelund, T.; Tryggvadottir, L.; Thordardottir, M.; Birgisdottir, B.E.; Harris, T.B.; Launer, L.J.; et al. Dietary habits in adolescence and midlife and risk of breast cancer in older women. PLoS ONE 2018, 13, e0198017. [Google Scholar] [CrossRef]
- Newton, C.J.; Samuel, D.L.; James, V.H. Aromatase activity and concentrations of cortisol, progesterone and testosterone in breast and abdominal adipose tissue. J. Steroid Biochem. 1986, 24, 1033–1039. [Google Scholar] [CrossRef]
- Folkerd, E.J.; James, V.H. Aromatization of steroids in peripheral tissues. J. Steroid Biochem. 1983, 19, 687–690. [Google Scholar] [CrossRef]
- Key, T.; Appleby, P.; Barnes, I.; Reeves, G.; Endogenous, H.; Breast Cancer Collaborative, G. Endogenous sex hormones and breast cancer in postmenopausal women: Reanalysis of nine prospective studies. J. Natl. Cancer Inst. 2002, 94, 606–616. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Subcohort (n = 933) | Case (n = 414) |
|---|---|---|
| Median (P5–P95) or n (%) | ||
| Age at study entry (2001/01/01) (year) | 60.8 (54.9–69.0) | 61.4 (55.0–69.0) |
| Waist-hip ratio 1 | 0.8 (0.7–0.9) | 0.8 (0.7–0.9) |
| Body mass index (kg/m2) 1 | ||
| <20 | 52 (6%) | 15 (4%) |
| 20–25 | 453 (49%) | 213 (51%) |
| >25 | 428 (46%) | 186 (45%) |
| Alcohol intake (g/day) 1 | 8.6 (0.5–40.2) | 10.8 (0.6–41.5) |
| Whole grain intake (g/day) 1 | ||
| Wheat | 3.4 (0.1–13.0) | 3.3 (0.1–13.5) |
| Rye | 21.3 (6.4–53.5) | 21.3 (6.4–53.3) |
| Energy intake (kJ/day) 1 | 8583 (5594–12712) | 8574 (5641–12426) |
| Alkylresorcinols in adipose tissue 1 | ||
| Total alkylresorcinol (nmol/g) | 0.90 (0.31–2.11) | 0.88 (0.32–1.95) |
| C17:0/C21:0 | 0.21 (0.06–0.45) | 0.23 (0.08–0.46) |
| Estrogen receptor | ||
| Positive | - | 56 (14%) |
| Negative | - | 345 (83%) |
| Unknown | - | 13 (3%) |
| Years in school (years) 1 | ||
| <8.0 | 308 (33%) | 125 (30%) |
| 8.0–10.0 | 467 (50%) | 212 (51%) |
| >10 | 158 (17%) | 77 (19%) |
| Parity 1 | ||
| Nulliparous | 124 (13%) | 62 (15%) |
| 1 | 142 (15%) | 76 (18%) |
| 2 | 428 (46%) | 185 (45%) |
| 3 | 192 (21%) | 69 (17%) |
| 4 | 42 (5%) | 18 (4%) |
| ≥5 | 5 (1%) | 4 (1%) |
| Age at first period (years) 1 | ||
| <12 | 224 (24%) | 102 (25%) |
| ≥12 | 673 (72%) | 297 (72%) |
| Unknown | 36 (4%) | 15 (4%) |
| Age at first birth (years) 1 | ||
| <25 | 619 (66%) | 255 (62%) |
| 25–29 | 233 (25%) | 130 (31%) |
| >29 | 81 (9%) | 29 (7%) |
| Menopause status 1 | ||
| Post- | 781 (84%) | 344 (83%) |
| Pre- | 152 (16%) | 70 (17%) |
| Use of menopausal hormones 1 | ||
| Never | 511 (55%) | 177 (43%) |
| Former | 145 (16%) | 53 (13%) |
| Current | 277 (30%) | 183 (44%) |
| Unknown | 0 (0%) | 1 (0%) |
| Exercise (min/day) 1 | ||
| <30 | 379 (41%) | 162 (39%) |
| ≥30 | 554 (59%) | 252 (61%) |
| Smoking status 1 | ||
| Never | 407 (44%) | 194 (47%) |
| Former | 214 (23%) | 92 (22%) |
| Current | 312 (33%) | 128 (31%) |
| Exposure | All Breast Cancer | ER+ Breast Cancer | ER- Breast Cancer | |||
|---|---|---|---|---|---|---|
| Crude Model HR (95%CI) | Multivariable- Adjusted Model HR (95%CI) 1 | Crude Model HR (95%CI) | Multivariable- Adjusted Model HR (95%CI) 1 | Crude Model HR (95%CI) | Multivariable- Adjusted Model HR (95%CI) 1 | |
| FFQ models | ||||||
| WGRWGW (g/day) | ||||||
| Q1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Q2 | 0.85(0.59–1.22) | 0.98(0.68–1.41) | 0.77(0.52–1.13) | 0.95(0.65–1.39) | 1.71(0.68–4.29) | 1.24(0.53–2.93) |
| Q3 | 0.86(0.62–1.20) | 1.10(0.76–1.60) | 0.77(0.54–1.09) | 0.98(0.66–1.45) | 1.70(0.75–3.84) | 1.30(0.56–3.00) |
| Q4 | 0.98(0.69–1.38) | 0.97(0.67–1.40) | 0.89(0.62–1.29) | 0.93(0.63–1.37) | 1.55(0.64–3.75) | 1.34(0.57–3.14) |
| Per 10 g/day | 1.00(0.92–1.09) | 1.01(0.91–1.11) | 0.99(0.90–1.08) | 1.01(0.90–1.12) | 1.02(0.88–1.19) | 0.98(0.8–1.21) |
| WGR% | ||||||
| Q1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Q2 | 1.11(0.77–1.60) | 1.10(0.77–1.58) | 1.17(0.79–1.73) | 1.17(0.79–1.71) | 0.83(0.33–2.09) | 0.86(0.36–2.05) |
| Q3 | 1.15(0.78–1.69) | 1.18(0.81–1.72) | 1.19(0.79–1.80) | 1.18(0.78–1.77) | 1.03(0.42–2.54) | 1.18(0.52–2.66) |
| Q4 | 1.44(1.03–2.03) | 1.60(1.10–2.35) | 1.50(1.05–2.15) | 1.62(1.09–2.42) | 1.31(0.59–2.89) | 1.48(0.62–3.52) |
| Per 10% | 1.06(0.98–1.14) | 1.06(0.97–1.16) | 1.07(0.98–1.16) | 1.06(0.97–1.16) | 1.06(0.91–1.24) | 1.10(0.91–1.34) |
| Biomarker models | ||||||
| Total AR (nmol/g) | ||||||
| Q1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Q2 | 0.95(0.68–1.32) | 1.01(0.71–1.44) | 0.78(0.54–1.10) | 0.84(0.58–1.22) | 2.38(1.07–5.28) | 2.25(1.01–5.00) |
| Q3 | 0.80(0.57–1.12) | 0.86(0.60–1.24) | 0.69(0.49–0.99) | 0.77(0.52–1.13) | 1.53(0.66–3.57) | 1.37(0.57–3.29) |
| Q4 | 0.89(0.64–1.23) | 0.93(0.65–1.32) | 0.84(0.59–1.18) | 0.91(0.63–1.32) | 1.03(0.41–2.56) | 0.93(0.38–2.31) |
| Per 1 nmol/g | 0.99(0.81–1.21) | 1.00(0.80–1.24) | 1.02(0.81–1.27) | 1.05(0.82–1.33) | 0.81(0.55–1.20) | 0.75(0.49–1.16) |
| C17:0/C21:0 | ||||||
| Q1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Q2 | 1.40(0.99–1.98) | 1.46(1.01–2.09) | 1.38(0.95–1.99) | 1.40(0.95–2.07) | 1.48(0.65–3.39) | 1.54(0.65–3.65) |
| Q3 | 1.63(1.16–2.30) | 1.65(1.16–2.36) | 1.61(1.12–2.32) | 1.60(1.09–2.33) | 2.12(0.97–4.63) | 2.25(0.99–5.09) |
| Q4 | 1.87(1.33–2.63) | 1.96(1.38–2.79) | 1.95(1.36–2.80) | 2.01(1.39–2.92) | 1.25(0.53–2.97) | 1.29(0.54–3.07) |
| Per 0.1 | 1.07(1.03–1.12) | 1.09(1.04–1.14) | 1.08(1.03–1.13) | 1.10(1.04–1.16) | 1.01(0.95–1.08) | 1.03(0.96–1.11) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.; Kyrø, C.; Tjønneland, A.; Boll, K.; Olsen, A.; Overvad, K.; Landberg, R. Long-Term Whole Grain Wheat and Rye Intake Reflected by Adipose Tissue Alkylresorcinols and Breast Cancer: A Case-Cohort Study. Nutrients 2019, 11, 465. https://doi.org/10.3390/nu11020465
Wu H, Kyrø C, Tjønneland A, Boll K, Olsen A, Overvad K, Landberg R. Long-Term Whole Grain Wheat and Rye Intake Reflected by Adipose Tissue Alkylresorcinols and Breast Cancer: A Case-Cohort Study. Nutrients. 2019; 11(2):465. https://doi.org/10.3390/nu11020465
Chicago/Turabian StyleWu, Huaxing, Cecilie Kyrø, Anne Tjønneland, Katja Boll, Anja Olsen, Kim Overvad, and Rikard Landberg. 2019. "Long-Term Whole Grain Wheat and Rye Intake Reflected by Adipose Tissue Alkylresorcinols and Breast Cancer: A Case-Cohort Study" Nutrients 11, no. 2: 465. https://doi.org/10.3390/nu11020465
APA StyleWu, H., Kyrø, C., Tjønneland, A., Boll, K., Olsen, A., Overvad, K., & Landberg, R. (2019). Long-Term Whole Grain Wheat and Rye Intake Reflected by Adipose Tissue Alkylresorcinols and Breast Cancer: A Case-Cohort Study. Nutrients, 11(2), 465. https://doi.org/10.3390/nu11020465