Intake of Sugar-Sweetened Beverages in Adolescents from Troms, Norway—The Tromsø Study: Fit Futures


Abstract
1. Introduction
2. Material and Methods
2.1. Dietary Variables
2.2. Other Variables
2.3. Statistical Analyses
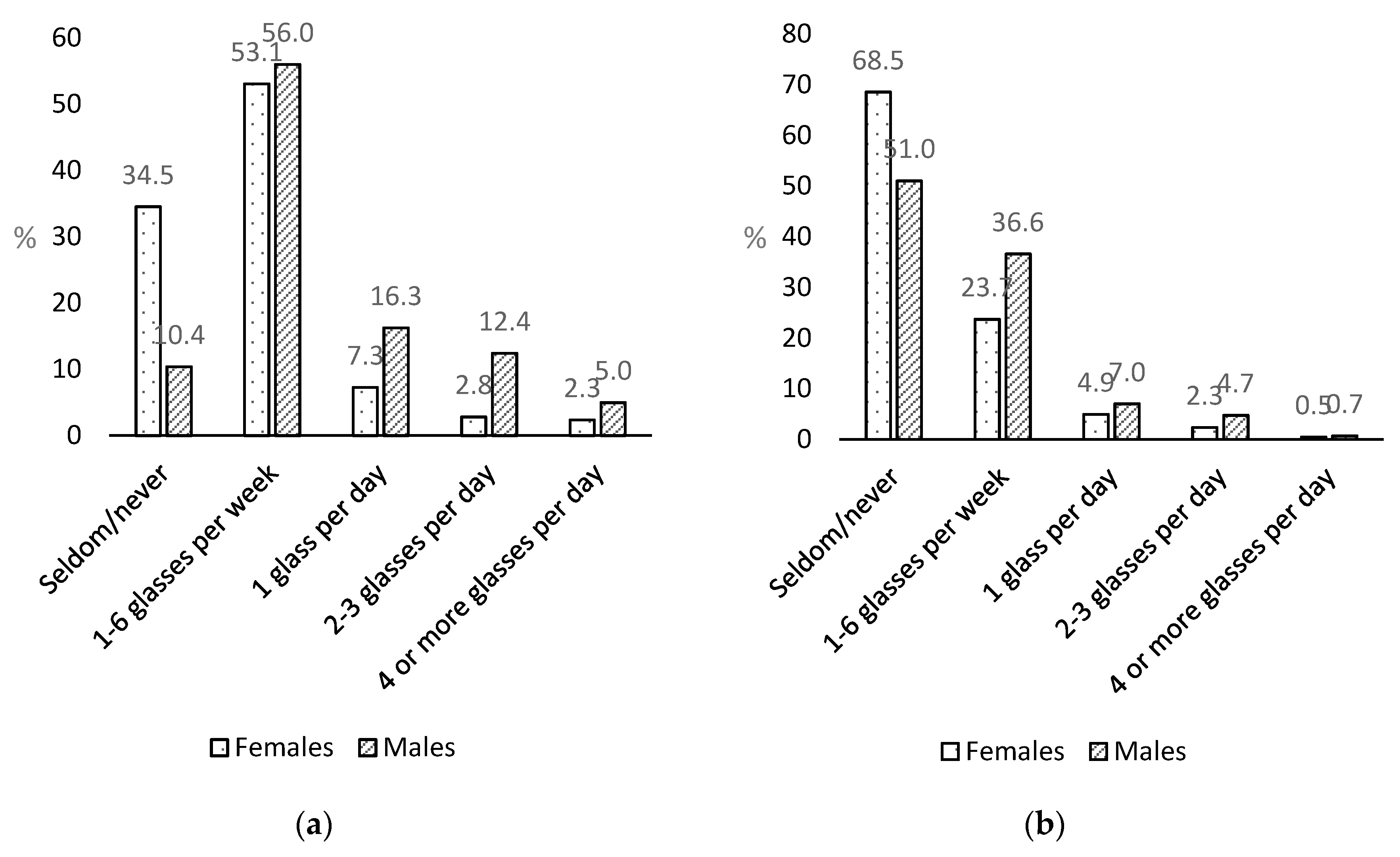
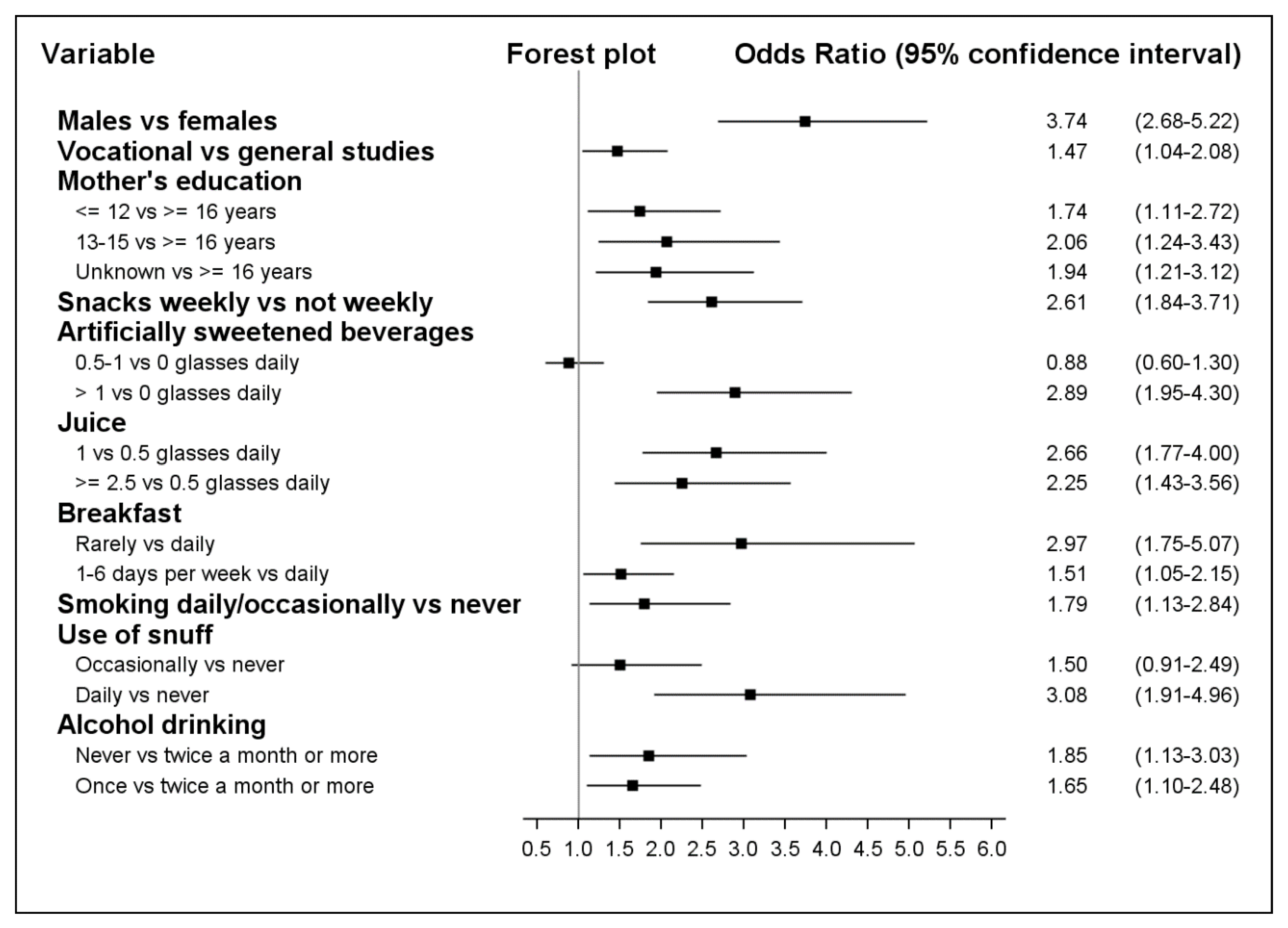
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index (kg/m2) |
| CI | Confidence interval |
| HBSC | Health Behaviour among School Children study |
| OR | Odds ratio |
| SSB | Sugar-sweetened beverages |
References
- Division of Nutrition, Physical Activity, and Obesity; National Center for Chronic Disease Prevention and Health Promotion. Get the Facts: Sugar-Sweetened Beverages and Consumption. Available online: https://www.cdc.gov/nutrition/data-statistics/sugar-sweetened-beverages-intake.html (accessed on 8 January 2018).
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Lim, S.; Ezzati, M.; Mozaffarian, D. Estimated Global, Regional, and National Disease Burdens Related to Sugar-Sweetened Beverage Consumption in 2010. Circulation 2015, 132, 639–666. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. Br. J. Sports Med. 2016, 50, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Overby, N.; Lillegaard, I.T. Intake of fruit and vegetables among Norwegian children and adolescents. Tidsskrift for den Norske Laegeforening Tidsskrift for Praktisk Medicin ny Raekke 2004, 124, 1396–1398. [Google Scholar]
- Vargas-Garcia, E.J.; Evans, C.E.L.; Prestwich, A.; Sykes-Muskett, B.J.; Hooson, J.; Cade, J.E. Interventions to reduce consumption of sugar-sweetened beverages or increase water intake: Evidence from a systematic review and meta-analysis. Obes. Rev. 2017, 18, 1350–1363. [Google Scholar] [CrossRef] [PubMed]
- Lussi, A.; Jaeggi, T.; Zero, D. The role of diet in the aetiology of dental erosion. Caries Res. 2004, 38 (Suppl. 1), 34–44. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.R.; Rivers, C.R. Systematic review of the evidence for an association between sugar-sweetened beverage consumption and risk of obesity. Nutr. Rev. 2014, 72, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef]
- Marshall, T.A.; Levy, S.M.; Broffitt, B.; Warren, J.J.; Eichenberger-Gilmore, J.M.; Burns, T.L.; Stumbo, P.J. Dental caries and beverage consumption in young children. Pediatrics 2003, 112, e184–e191. [Google Scholar] [CrossRef]
- Fismen, A.S.; Smith, O.R.; Torsheim, T.; Rasmussen, M.; Pedersen Pagh, T.; Augustine, L.; Ojala, K.; Samdal, O. Trends in Food Habits and Their Relation to Socioeconomic Status among Nordic Adolescents 2001/2002–2009/2010. PLoS ONE 2016, 11, e0148541. [Google Scholar] [CrossRef]
- Stea, T.H.; Overby, N.C.; Klepp, K.I.; Bere, E. Changes in beverage consumption in Norwegian children from 2001 to 2008. Public Health Nutr. 2012, 15, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Ministry of health and Care Services. Norwegian Action Plan on Nutrition (2007–2011)—Recipe for a Healthier Diet; Norwegian Ministries: Oslo, Norway, 2007.
- Åstrøm, A.N.; Klepp, K.I.; Samdal, O. Konsum av sukret mineralvann og søtsaker blant norske skoleelever: Sterk økning fra 1989 til 2001. Nor Tannlegeforen Tid 2004, 114, 816–821. [Google Scholar]
- Samdal, O.; Bye, H.H.; Torsheim, T.; Birkeland, M.S.; Diseth, Å.R.; Fismen, A.-S.; Haug, E.; Leversen, I.; Wold, B. Sosial Ulikhet i Helse og Læring Blant Barn og Unge. Resultater fra den Landsrepresentative Spørreskjemaundersøkelsen “Helsevaner Blant Skoleelever. En WHO-Undersøkelse i Flere Land”; HEMIL-Senteret, Universitetet i Bergen: Bergen, Norway, 2012. [Google Scholar]
- Samdal, O.; Mathisen, F.; Torsheim, T.; Diseth, Å.; Fismen, A.-S.; Larsen, T.; Wold, B.; Årdal, E. Helse og Trivsel Blant Barn og Unge. Resultater fra den Landsrepresentative Spørreundersøkelsen «Helsevaner Blant Skoleelever. En WHO-Undersøkelse i Flere Land»; HEMIL-Senteret, Universitetet i Bergen: Bergen, Norway, 2016. [Google Scholar]
- Bjelland, M.; Lien, N.; Grydeland, M.; Bergh, I.H.; Anderssen, S.A.; Ommundsen, Y.; Klepp, K.I.; Andersen, L.F. Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (HEalth In Adolescents) study. Public Health Nutr. 2011, 14, 2156–2165. [Google Scholar] [CrossRef] [PubMed]
- Kvaavik, E.; Andersen, L.F.; Klepp, K.I. The stability of soft drinks intake from adolescence to adult age and the association between long-term consumption of soft drinks and lifestyle factors and body weight. Public Health Nutr. 2005, 8, 149–157. [Google Scholar] [CrossRef]
- Greenwood, D.C.; Threapleton, D.E.; Evans, C.E.L.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Burley, V.J. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose–response meta-analysis of prospective studies. Br. J. Nutr. 2014, 112, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Lien, N.; Torheim, L.E.; Andersen, L.F.; Melbye, E.L.; Glavin, K.; Hausken, S.E.; Sleddens, E.F.; Bjelland, M. Perceived rules and accessibility: Measurement and mediating role in the association between parental education and vegetable and soft drink intake. Nutr. J. 2016, 15, 76. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Henjum, S.; Terragni, L.; Torheim, L.E. Correlates of fruit, vegetable, soft drink, and snack intake among adolescents: The ESSENS study. Food Nutr. Res. 2016, 60, 32512. [Google Scholar] [CrossRef]
- Melbye, E.L.; Bergh, I.H.; Hausken, S.E.S.; Sleddens, E.F.C.; Glavin, K.; Lien, N.; Bjelland, M. Adolescent impulsivity and soft drink consumption: The role of parental regulation. Appetite 2016, 96, 432–442. [Google Scholar] [CrossRef]
- Øvrebø, E.M. Food habits of school pupils in Tromsø, Norway, in the transition from 13 to 15 years of age. Int. J. Consum. Stud. 2011, 35, 520–528. [Google Scholar] [CrossRef]
- Statistics Norway. Dental Status by Age, 18-Year Olds. Available online: https://www.ssb.no/statistikkbanken/SelectVarVal/saveselections.asp (accessed on 19 November 2015).
- Mulic, A.; Fredriksen, O.; Jacobsen, I.D.; Tveit, A.B.; Espelid, I.; Crossner, C.G. Dental erosion: Prevalence and severity among 16-year-old adolescents in Troms, Norway. Eur. J. Paediatr. Dent. 2016, 17, 197–201. [Google Scholar]
- Winther, A.; Dennison, E.; Ahmed, L.A.; Furberg, A.S.; Grimnes, G.; Jorde, R.; Gjesdal, C.G.; Emaus, N. The Tromso Study: Fit Futures: A study of Norwegian adolescents’ lifestyle and bone health. Arch. Osteoporos. 2014, 9, 185. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Bolt-Evensen, K.; Vik, F.N.; Stea, T.H.; Klepp, K.I.; Bere, E. Consumption of sugar-sweetened beverages and artificially sweetened beverages from childhood to adulthood in relation to socioeconomic status—15 years follow-up in Norway. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Blanck, H.M.; Sherry, B.; Brener, N.; O’Toole, T. Factors Associated with Sugar-Sweetened Beverage Intake among United States High School Students. J. Nutr. 2012, 142, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Laverty, A.A.; Magee, L.; Monteiro, C.A.; Saxena, S.; Millett, C. Sugar and artificially sweetened beverage consumption and adiposity changes: National longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 137. [Google Scholar] [CrossRef] [PubMed]
- Duffey, K.J.; Huybrechts, I.; Mouratidou, T.; Libuda, L.; Kersting, M.; De Vriendt, T.; Gottrand, F.; Widhalm, K.; Dallongeville, J.; Hallstrom, L.; et al. Beverage consumption among European adolescents in the HELENA study. Eur. J. Clin. Nutr. 2012, 66, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Inchley, J.; Subramanian, S.V.; Hublet, A.; Maes, L. The relative influence of individual and contextual socio-economic status on consumption of fruit and soft drinks among adolescents in Europe. Eur. J. Public Health 2005, 15, 224–232. [Google Scholar] [CrossRef]
- Gasser, C.E.; Mensah, F.K.; Russell, M.; Dunn, S.E.; Wake, M. Confectionery consumption and overweight, obesity, and related outcomes in children and adolescents: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 103, 1344–1356. [Google Scholar] [CrossRef]
- Nordnes, E.T.; Melbye, E.L.; Pedersen, I.; Bjelland, M. Hva Betyr Kjønn, Foreldres Utdanningsnivå og Foreldrepraksis for Ungdommers Inntak av Ulike Typer Drikke? Master’s Thesis, Norwegian University of Life Sciences, Ås, Norway, 2016; pp. 6–12. [Google Scholar]
- Hansen, L.B.; Myhre, J.B.; Johansen, A.M.W.; Paulsen, M.M.; Andersen, L.F. UNGKOST 3. Landsomfattende Kostholdsundersøkelse Blant Elever i 4.—og 8. Klasse i Norge, 2015; Folkehelseinstituttet: Oslo, Norway, 2016. [Google Scholar]
- Ambrosini, G.L.; Johns, D.J.; Northstone, K.; Emmett, P.M.; Jebb, S.A. Free Sugars and Total Fat Are Important Characteristics of a Dietary Pattern Associated with Adiposity across Childhood and Adolescence. J. Nutr. 2016, 146, 778–784. [Google Scholar] [CrossRef]
- Ministries. Norwegian Action Plan for a Better Diet (2017–2021); Ministries: Oslo, Norway, 2017. [Google Scholar]
- Avery, A.; Bostock, L.; McCullough, F. A systematic review investigating interventions that can help reduce consumption of sugar-sweetened beverages in children leading to changes in body fatness. J. Hum. Nutr. Diet. 2015, 28 (Suppl. 1), 52–64. [Google Scholar] [CrossRef]
- Grieger, J.A.; Wycherley, T.P.; Johnson, B.J.; Golley, R.K. Discrete strategies to reduce intake of discretionary food choices: A scoping review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 57. [Google Scholar] [CrossRef] [PubMed]
- Battram, D.S.; Piche, L.; Beynon, C.; Kurtz, J.; He, M. Sugar-Sweetened Beverages: Children’s Perceptions, Factors of Influence, and Suggestions for Reducing Intake. J. Nutr. Educ. Behav. 2016, 48, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Riordan, F.; Ryan, K.; Perry, I.J.; Schulze, M.B.; Andersen, L.F.; Geelen, A.; Van’t Veer, P.; Eussen, S.; van Dongen, M.; Wijckmans-Duysens, N.; et al. A systematic review of methods to assess intake of sugar-sweetened beverages among healthy European adults and children: A DEDIPAC (DEterminants of DIet and Physical Activity) study. Public Health Nutr. 2017, 20, 578–597. [Google Scholar] [CrossRef] [PubMed]
- Kolodziejczyk, J.K.; Merchant, G.; Norman, G.J. Reliability and validity of child/adolescent food frequency questionnaires that assess foods and/or food groups. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.P.; Kaiser, U.B. Pubertal development and regulation. Lancet Diabetes Endocrinol. 2016, 4, 254–264. [Google Scholar] [CrossRef]
- Kantanista, A.; Osinski, W.; Borowiec, J.; Tomczak, M.; Krol-Zielinska, M. Body image, BMI, and physical activity in girls and boys aged 14–16 years. Body Image 2015, 15, 40–43. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Females (n = 426) | Males (n = 444) | |
|---|---|---|
| Age, years | 16.1 | 16.1 |
| Living with parent(s) | 85.9 | 87.8 |
| Mother’s education | ||
| Elementary or secondary school | 34.3 | 32.0 |
| College/university < 4 years | 19.0 | 16.4 |
| College/university 4 years or more | 23.5 | 22.3 |
| Unknown/missing | 23.2 | 29.3 |
| Father’s education | ||
| Elementary or secondary school | 38.7 | 39.0 |
| College/university < 4 years | 13.4 | 13.5 |
| College/university 4 years or more | 18.8 | 18.2 |
| Unknown/missing | 29.1 | 29.3 |
| General study programme (including sports) | 61.7 | 45.1 |
| Drink sugar-sweetened beverages daily | 32.2 | 61.3 |
| Servings of fruits and vegetables, daily | ||
| Less than 0.6 | 22.8 | 34.7 |
| 0.6–1.3 | 18.1 | 22.3 |
| 1.4–2.3 | 26.3 | 22.1 |
| More than 2.3 | 32.8 | 20.9 |
| Consume chocolate/sweets at least weekly | 70.2 | 68.5 |
| Consume sweet or savoury snacks at least weekly | 64.3 | 68.0 |
| Light/artificially sweetened beverages, daily | ||
| None | 40.6 | 43.9 |
| 0.5 glass | 32.6 | 26.6 |
| 1 glass or more | 26.8 | 29.5 |
| Fruit juice, daily | ||
| 0.5 glass or less | 65.5 | 63.7 |
| 1 glass | 19.2 | 21.4 |
| 2.5 glasses or more | 15.3 | 14.9 |
| Milk, daily 2 | ||
| 1 glass or less | 42.7 | 40.6 |
| 1.5–2.5 glass | 31.5 | 26.1 |
| 2.5 glasses or more | 25.8 | 33.3 |
| Water, daily | ||
| 1 glass or less | 18.3 | 31.1 |
| 2–3 glasses | 34.5 | 33.8 |
| 4 or more glasses | 47.2 | 35.1 |
| Breakfast | ||
| Seldom/never | 15.0 | 12.2 |
| 1–3 days per week | 35.2 | 35.3 |
| Every day | 49.8 | 52.5 |
| Bring lunch for school | ||
| Seldom/never | 23.0 | 34.9 |
| 1–6 days/week | 43.4 | 39.0 |
| Every school day | 33.6 | 26.1 |
| Dinner daily | 58.5 | 73.4 |
| Overweight/obese | 19.3 | 23.7 |
| Screen time, daily 3 | ||
| <2 h | 26.3 | 14.0 |
| 2–3.99 h | 38.7 | 38.3 |
| 4 h or more | 35.0 | 47.7 |
| Physical activity outside school hours, weekly | ||
| Not active | 30.0 | 33.3 |
| 3 h or less | 30.3 | 26.6 |
| 4 h or more | 39.7 | 40.1 |
| Smoking daily or occasionally | 20.0 | 23.4 |
| Use of snuff | ||
| Never | 67.1 | 60.4 |
| Occasionally | 14.3 | 12.8 |
| Daily | 18.6 | 26.8 |
| Alcohol drinking | ||
| Never | 23.5 | 32.7 |
| Once per month or less often | 46.9 | 37.1 |
| Twice per month or more often | 29.6 | 30.2 |
| Characteristic | Females (n = 426) 1 | Males (n = 444) 1 | ||
|---|---|---|---|---|
| Daily Drinkers % (n 2) | p-Value 3 | Daily Drinkers % (n 2) | p-Value 3 | |
| Living with parent(s) | 0.63 | 0.84 | ||
| Yes | 32.6 (119/365) | 61.4 (239/389) | ||
| No | 29.5 (18/61) | 60.0 (33/55) | ||
| School programme | <0.0001 | 0.0003 | ||
| Vocational | 46.6 (76/163) | 68.9 (168/244) | ||
| General (including sports) | 23.2 (61/263) | 52.0 (104/200) | ||
| Servings of fruits and vegetables, daily | 0.008 | 0.05 | ||
| Less than 0.6 | 40.2 (39/97) | 69.5 (107/154) | ||
| 0.6–1.3 | 42.9 (33/77) | 60.6 (60/99) | ||
| 1.4–2.3 | 24.1 (27/112) | 53.1 (52/98) | ||
| More than 2.3 | 27.1 (38/140) | 57.0 (53/93) | ||
| Consumption of chocolate/sweets | 0.007 | 0.007 | ||
| Not weekly | 22.8 (29/127) | 52.1 (73/140) | ||
| Weekly | 36.1 (108/299) | 65.5 (199/304) | ||
| Consumption of sweet or savoury snacks | <0.0001 | 0.004 | ||
| Not weekly | 18.4 (28/152) | 51.4 (73/142) | ||
| Weekly | 39.8 (109/274) | 65.9 (199/302) | ||
| Light/artificially sweetened beverages, daily | <0.0001 | 0.003 | ||
| None | 24.3 (42/173) | 54.4 (106/195) | ||
| 0.5 glass | 20.9 (29/139) | 56.8 (67/118) | ||
| 1 glass or more | 57.9 (66/114) | 75.6 (99/131) | ||
| Fruit juice, daily | 0.0006 | 0.002 | ||
| 0.5 glass | 25.8 (72/279) | 55.1 (156/283) | ||
| 1 glass | 43.9 (36/82) | 72.6 (69/95) | ||
| 2.5 glasses or more | 44.6 (29/65) | 71.2 (47/66) | ||
| Milk, daily 4 | 0.28 | 0.10 | ||
| 1 glass or less | 34.6 (63/182) | 67.2 (121/180) | ||
| 1.5–2.5 glass | 26.9 (36/134) | 56.0 (65/116) | ||
| 2.5 glasses or more | 34.6 (38/110) | 58.1 (86/148) | ||
| Water, daily | 0.02 | 0.0005 | ||
| 1 glass or less | 41.0 (32/78) | 74.6 (103/138) | ||
| 2–3 glasses | 36.1 (53/147) | 56.0 (84/150) | ||
| 4 glasses or more | 25.9 (52/201) | 54.5 (85/156) | ||
| Breakfast | <0.0001 | 0.002 | ||
| Seldom/never | 67.2 (43/64) | 74.1 (40/54) | ||
| 1–6 days/week | 31.3 (47/150) | 68.2 (107/157) | ||
| Every day | 22.2 (47/212) | 53.7 (125/233) | ||
| Bring lunch to school | <0.0001 | 0.0006 | ||
| Seldom/never | 50.0 (49/98) | 68.4 (106/155) | ||
| 1–4 days/week | 31.4 (58/185) | 64.7 (112/173) | ||
| Every school day | 21.0 (30/143) | 46.6 (54/116) | ||
| Dinner | 0.09 | 0.21 | ||
| Not daily | 36.7 (65/177) | 66.1 (78/118) | ||
| Daily | 28.9 (72/249) | 59.5 (194/326) | ||
| Weight class | 0.38 | 0.59 | ||
| Thin/normal weight | 33.1 (114/344) | 62.0 (210/339) | ||
| Overweight/obese | 28.1 (23/82) | 59.1 (62/105) | ||
| Screen time, daily 5 | 0.002 | 0.24 | ||
| <2 h | 22.3 (25/112) | 54.8 (34/62) | ||
| 2–3.99 h | 29.7 (49/165) | 58.8 (100/170) | ||
| 4 h or more | 42.3 (63/149) | 65.1 (138/212) | ||
| Physical activity outside school hours, weekly | 0.0001 | 0.06 | ||
| Not active | 46.9 (60/128) | 65.5 (97/148) | ||
| 3 h or less | 26.4 (34/129) | 66.1 (78/118) | ||
| 4 h or more | 25.4 (43/169) | 54.5 (97/178) | ||
| Smoking | < 0.0001 | 0.005 | ||
| Never | 26.7 (91/341) | 57.7 (196/340) | ||
| Occasionally or daily | 54.1 (46/85) | 73.1 (76/104) | ||
| Use of snuff | < 0.0001 | 0.001 | ||
| Never | 23.1 (66/286) | 54.9 (147/268) | ||
| Occasionally | 39.3 (24/61) | 63.2 (36/57) | ||
| Daily | 59.5 (47/79) | 74.8 (89/119) | ||
| Alcohol drinking | 0.1 | 0.02 | ||
| Never | 29.0 (29/100) | 52.4 (76/145) | ||
| Once a month or less often | 29.0 (58/200) | 67.9 (112/165) | ||
| Twice a month or more often | 39.7 (50/126) | 62.7 (84/134) | ||
| Females (n = 426) | Males (n = 444) | |||
|---|---|---|---|---|
| Characteristic | OR | 95% CI | OR | 95% CI |
| School programme | ||||
| General | Ref | Ref | ||
| Vocational | 1.59 | (0.94–2.68) | 1.59 | (1.03–2.46) |
| Consumption of sweet or savoury snacks | ||||
| Not weekly | Ref | Ref | ||
| Weekly | 3.67 | (2.03–6.64) | 2.03 | (1.29–3.19) |
| Light/artificially sweetened beverages, daily | ||||
| None | Ref | Ref | ||
| 0.5 glass | 0.77 | (0.41–1.46) | 0.99 | (0.60–1.64) |
| 1 glass or more | 4.05 | (2.22–7.36) | 2.20 | (1.30–3.72) |
| Fruit juice, daily | ||||
| 0.5 glass or less | Ref | Ref | ||
| 1 glass | 2.12 | (1.13–3.95) | 2.82 | (1.62–4.92) |
| 2.5 glasses or more | 2.34 | (1.18–4.64) | 2.13 | (1.13–4.03) |
| Breakfast | ||||
| Every day | Ref | Ref | ||
| 1–6 days/week | 1.19 | (0.68–2.08) | 1.68 | (1.04–2.70) |
| Seldom/never | 4.03 | (1.88–8.63) | 2.02 | (0.97–4.22) |
| Smoking | ||||
| Never | Ref | Ref | ||
| Occasionally or daily | 1.92 | (0.98–3.76) | 1.59 | (0.84–2.99) |
| Use of snuff | ||||
| Never | Ref | Ref | ||
| Occasionally | 2.35 | (1.12–4.91) | 1.14 | (0.56–2.30) |
| Daily | 4.93 | (2.40–10.14) | 2.18 | (1.14–4.16) |
| Alcohol drinking | ||||
| Twice a month or more often | Ref | Ref | ||
| Once a month or less often | 1.39 | (0.76–2.54) | 2.00 | (1.13–3.53) |
| Never | 2.59 | (1.19–5.66) | 1.60 | (0.84–3.03) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skeie, G.; Sandvær, V.; Grimnes, G. Intake of Sugar-Sweetened Beverages in Adolescents from Troms, Norway—The Tromsø Study: Fit Futures. Nutrients 2019, 11, 211. https://doi.org/10.3390/nu11020211
Skeie G, Sandvær V, Grimnes G. Intake of Sugar-Sweetened Beverages in Adolescents from Troms, Norway—The Tromsø Study: Fit Futures. Nutrients. 2019; 11(2):211. https://doi.org/10.3390/nu11020211
Chicago/Turabian StyleSkeie, Guri, Vårin Sandvær, and Guri Grimnes. 2019. "Intake of Sugar-Sweetened Beverages in Adolescents from Troms, Norway—The Tromsø Study: Fit Futures" Nutrients 11, no. 2: 211. https://doi.org/10.3390/nu11020211
APA StyleSkeie, G., Sandvær, V., & Grimnes, G. (2019). Intake of Sugar-Sweetened Beverages in Adolescents from Troms, Norway—The Tromsø Study: Fit Futures. Nutrients, 11(2), 211. https://doi.org/10.3390/nu11020211