Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study



Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Measurement
2.2.1. Vascular Functions
2.2.2. Other Cardiovascular Risk Parameters
2.2.3. Body Composition
2.2.4. Outcome Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fact Sheets-Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 20 June 2019).
- World Health Organization. Q & As on Hypertension. Available online: https://www.who.int/features/qa/82/en/ (accessed on 20 June 2019).
- Bonetti, P.O.; Lerman, L.O.; Lerman, A. Endothelial dysfunction: A marker of atherosclerotic risk. Arter. Thromb. Vasc. Biol. 2003, 23, 168–175. [Google Scholar] [CrossRef]
- Endemann, D.H.; Schiffrin, E.L. Endothelial dysfunction. J. Am. Soc. Nephrol. 2004, 15, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Panza, J.A.; Quyyumi, A.A.; Brush, J.E., Jr.; Epstein, S.E. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. N. Engl. J. Med. 1990, 323, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Daiber, A.; Steven, S.; Weber, A.; Shuvaev, V.V.; Muzykantov, V.R.; Laher, I.; Li, H.; Lamas, S.; Münzei, T. Targeting vascular (endothelial) dysfunction. Br. J. Pharm. 2017, 174, 1591–1619. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.G. Cellular and molecular mechanisms of endothelial cell dysfunction. J. Clin Investig. 1997, 100, 2153–2157. [Google Scholar] [CrossRef] [PubMed]
- Ignarro, L.J.; Buga, G.M.; Wood, K.S.; Byrns, R.E.; Chaudhuri, G. Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Proc. Natl. Acad. Sci. USA 1987, 84, 9265–9269. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M. Oxidative stress and vascular damage in hypertension. Curr. Hypertens. Rep. 2000, 2, 98–105. [Google Scholar] [CrossRef]
- Münzel, T.; Sinning, C.; Post, F.; Warnholtz, A.; Schulz, E. Pathophysiology, diagnosis and prognostic implications of endothelial dysfunction. Ann. Med. 2008, 40, 180–196. [Google Scholar] [CrossRef]
- Duffy, S.J.; Gokce, N.; Holbrook, M.; Hunter, L.M.; Biegelsen, E.S.; Huang, A.; Keaney, J.F., Jr.; Vita, J.A. Effect of ascorbic acid treatment on conduit vessel endothelial dysfunction in patients with hypertension. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H528–H534. [Google Scholar] [CrossRef]
- Ulker, S.; McKeown, P.P.; Bayraktutan, U. Vitamins reverse endothelial dysfunction through regulation of eNOS and NAD(P)H oxidase activities. Hypertension 2003, 41, 534–539. [Google Scholar] [CrossRef]
- Bauersachs, J.; Fleming, I.; Fraccarollo, D.; Busse, R.; Ertl, G. Prevention of endothelial dysfunction in heart failure by vitamin E: Attenuation of vascular superoxide anion formation and increase in soluble guanylyl cyclase expression. Cardiovasc. Res. 2001, 51, 344–350. [Google Scholar] [CrossRef]
- Si, H.; Liu, D. Genistein, a soy phytoestrogen, upregulates the expression of human endothelial nitric oxide synthase and lowers blood pressure in spontaneously hypertensive rats. J. Nutr. 2009, 138, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Loke, W.M.; Proudfoot, J.M.; Hodgson, J.M.; McKinley, A.J.; Hime, N.; Magat, M.; Stocker, R.; Croft, K.D. Specific dietary polyphenols attenuate atherosclerosis in apolipoprotein E-knockout mice by alleviating inflammation and endothelial dysfunction. Arter. Thromb. Vasc. Biol. 2010, 30, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Sitim, H.N.; Kamisah, Y.; Kamsiah, J. The role of oxidative stress, antioxidants and vascular inflammation in cardiovascular disease (a review). Vasc. Pharm. 2015, 71, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.A.; Yuan Yuan, D.; Nawaz, W.; Ze, H.; Zhuo, C.X.; Talal, B.; Mais, E.; Qilong, D. Antioxidant therapy for management of oxidative stress induced hypertension. Free Radic. Res. 2017, 51, 428–438. [Google Scholar] [CrossRef]
- Vivekananthan, D.P.; Penn, M.S.; Sapp, S.K.; Hsu, A.; Topol, E.J. Use of antioxidant vitamins for the prevention of cardiovascular disease: Meta-analysis of randomised trials. Lancet 2003, 361, 2017–2023. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. JAMA 2007, 297, 842–857. [Google Scholar] [CrossRef]
- Myung, S.K.; Ju, W.; Cho, B.; Oh, S.W.; Park, S.M.; Koo, B.K.; Park, B.J. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: Systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 346, f10. [Google Scholar] [CrossRef]
- Ariga, T. The antioxidative function, preventive action on disease and utilization of proanthocyanidins. Biofactors 2004, 21, 197–201. [Google Scholar] [CrossRef]
- Dixon, R.A.; Xie, D.Y.; Sharma, S.B. Proanthocyanidins—A final frontier in flavonoid research? New Phytol. 2005, 165, 9–28. [Google Scholar] [CrossRef]
- Bagchi, D.; Bagchi, M.; Stohs, S.J.; Das, D.K.; Ray, S.D.; Kuszynski, C.A.; Joshi, S.S.; Pruess, H.G. Free radicals and grape seed proanthocyanidin extract: Importance in human health and disease prevention. Toxicology 2000, 148, 187–197. [Google Scholar] [CrossRef]
- Bagchi, D.; Garg, A.; Krohn, R.L.; Bagchi, M.; Bagchi, D.J.; Balmoori, J.; Stohs, S.J. Protective effects of grape seed proanthocyanidins and selected antioxidants against TPA-induced hepatic and brain lipid peroxidation and DNA fragmentation, and peritoneal macrophage activation in mice. Gen. Pharm. 1998, 30, 771–776. [Google Scholar] [CrossRef]
- Terauchi, M.; Horiguchi, N.; Kajiyama, A.; Akiyoshi, M.; Owa, Y.; Kato, K.; Kubota, T. Effects of grape seed proanthocyanidin extract on menopausal symptoms, body composition, and cardiovascular parameters in middle-aged women: A randomized, double-blind, placebo-controlled pilot study. Menopause 2014, 21, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Stadler, R.W.; Ibrahim, S.F.; Lees, R.S. Measurement of the time course of peripheral vasoactivity: Results in cigarette smokers. Atherosclerosis 1998, 138, 197–205. [Google Scholar] [CrossRef]
- Gori, T.; Dragoni, S.; Lisi, M.; Di Stolfo, G.; Sonnati, S.; Fineschi, M.; Parker, J.D. Conduit artery constriction mediated by low flow a novel noninvasive method for the assessment of vascular function. J. Am. Coll. Cardiol. 2008, 51, 1953–1958. [Google Scholar] [CrossRef]
- Kaiser, D.R.; Mullen, K.; Bank, A.J. Brachial artery elastic mechanics in patients with heart failure. Hypertension 2001, 38, 1440–1445. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Maruhashi, T.; Fujii, Y.; Idei, N.; Fujimura, N.; Mikami, S.; Kajikawa, M.; Matsumoto, T.; Kihara, Y.; Chayama, K.; et al. Intima-media thickness of brachial artery, vascular function, and cardiovascular risk factors. Arter. Thromb. Vasc. Biol. 2012, 32, 2295–2303. [Google Scholar] [CrossRef]
- Asmar, R.; Benetos, A.; Topouchian, J.; Laurent, P.; Pannier, B.; Brisac, A.M.; Taeget, R.; Levy, B.I. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension 1995, 26, 485–490. [Google Scholar] [CrossRef]
- Ogawa, T.; Shimada, M.; Ishida, H.; Matsuda, N.; Fujiu, A.; Ando, Y.; Nitta, K. Relation of stiffness parameter beta to carotid arteriosclerosis and silent cerebral infarction in patients on chronic hemodialysis. Int. Urol. Nephrol. 2009, 41, 739–745. [Google Scholar] [CrossRef]
- Ohkuma, T.; Ninomiya, T.; Tomiyama, H.; Kario, K.; Hoshide, S.; Kita, Y.; Inoguchi, T.; Maeda, Y.; Kohara, K.; Tabara, Y.; et al. Brachial-ankle pulse wave velocity and the risk prediction of cardiovascular disease: An individual participant data meta-analysis. Hypertension 2017, 69, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Shen, F.; Liu, J.; Yang, G.Y. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc. Neurol. 2017, 2, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.Y.; Dixon, R.A. Proanthocyanidin biosynthesis—Still more questions than answers? Phytochemistry 2005, 66, 2127–2144. [Google Scholar] [CrossRef] [PubMed]
- Brian, D.C.; Adrian, L.K.; Ryszard, A.; Ronald, B.P. Phenol-based antioxidants and the in vitro methods used for their assessment. Compr. Rev. Food Sci. Food Saf. 2012, 11, 148–173. [Google Scholar] [CrossRef]
- Juana, M.C.C.; Magdalena, B.; Francisco, J.B.; María, J.E.; Ana, F. Analytical methods for determining bioavailability and bioaccessibility of bioactive compounds from fruits and vegetables: A review. Compr. Rev. Food Sci. Food Saf. 2014, 13, 155–171. [Google Scholar] [CrossRef]
- Yamakoshi, J.; Kataoka, S.; Koga, T.; Ariga, T. Proanthocyanidin-rich extract from grape seeds attenuates the development of aortic atherosclerosis in cholesterol-fed rabbits. Atherosclerosis 1999, 142, 139–149. [Google Scholar] [CrossRef]
- Subarnas, A.; Wagner, H. Analgesic and anti-inflammatory activity of the proanthocyanidin shellegueain A from Polypodium feei METT. Phytomedicine 2000, 7, 401–405. [Google Scholar] [CrossRef]
- Kozikowski, A.P.; Tückmantel, W.; Böttcher, G.; Romanczyk, L.J., Jr. Studies in polyphenol chemistry and bioactivity. 4.(1) Synthesis of trimeric, tetrameric, pentameric, and higher oligomeric epicatechin-derived procyanidins having all-4beta, 8-interflavan connectivity and their inhibition of cancer cell growth through cell cycle arrest. J. Org. Chem. 2003, 68, 1641–1658. [Google Scholar] [CrossRef]
- Corder, R.; Mullen, W.; Khan, N.Q.; Marks, S.C.; Wood, E.G.; Carrier, M.J.; Crozier, A. Oenology: Red wine procyanidins and vascular health. Nature 2006, 444, 566. [Google Scholar] [CrossRef]
- Barona, J.; Aristizabal, J.C.; Blesso, C.N.; Volek, J.S.; Fernandez, M.L. Grape polyphenols reduce blood pressure and increase flow-mediated vasodilation in men with metabolic syndrome. J. Nutr. 2012, 142, 1626–1632. [Google Scholar] [CrossRef]
- Clifton, P.M. Effect of grape seed extract and quercetin on cardiovascular and endothelial parameters in high-risk subjects. J. Biomed. Biotechnol. 2004, 2004, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Van Mierlo, L.A.; Zock, P.L.; van der Knaap, H.C.; Draijer, R. Grape polyphenols do not affect vascular function in healthy men. J. Nutr. 2010, 140, 1769–1773. [Google Scholar] [CrossRef] [PubMed]
- Mellen, P.B.; Daniel, K.R.; Brosnihan, K.B.; Hansen, K.J.; Herrington, D.M. Effect of muscadine grape seed supplementation on vascular function in subjects with or at risk for cardiovascular disease: A randomized crossover trial. J. Am. Coll. Nutr. 2010, 29, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Gori, T.; Grotti, S.; Dragoni, S.; Lisi, M.; Di Stolfo, G.; Sonnati, S.; Fineschi, M.; Parker, J.D. Assessment of vascular function: Flow-mediated constriction complements the information of flow-mediated dilatation. Heart 2010, 96, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Spieker, L.E.; Lüscher, T.F.; Noll, G. ETA receptors mediate vasoconstriction of large conduit arteries during reduced flow in humans. J. Cardiovasc. Pharm. 2003, 42, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.O.; Alsalahi, S.; Fisher, J.P. Impact of acute dynamic exercise on radial artery low-flow mediated constriction in humans. Eur. J. Appl. Physiol. 2018, 118, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, R.E.; Green, D.J.; Cable, N.T.; Thijssen, D.H.; Dawson, E.A. Low-flow mediated constriction: The yin to FMD’s yang? Expert Rev. Cardiovasc. 2014, 12, 557–564. [Google Scholar] [CrossRef]
- Gori, T.; Parker, J.D.; Münzel, T. Flow-mediated constriction: Further insight into a new measure of vascular function. Eur. Heart J. 2011, 32, 784–787. [Google Scholar] [CrossRef]
- Harrison, M.; Parkhurst, K.; Tarumi, T.; Lin, H.F.; Tanaka, H. Low flow-mediated constriction: Prevalence, impact and physiological determinant. Clin. Physiol. Funct. Imaging 2011, 31, 394–398. [Google Scholar] [CrossRef]
- Chen, Q.Z.; Han, W.Q.; Chen, J.; Zhu, D.L.; Chen-Yan Gao, P.J. Anti-stiffness effect of apocynin in deoxycorticosterone acetate-salt hypertensive rats via inhibition of oxidative stress. Hypertens. Res. 2013, 36, 306–312. [Google Scholar] [CrossRef]
- Li, W.G.; Zhang, X.Y.; Wu, Y.J.; Tian, X. Anti-inflammatory effect and mechanism of proanthocyanidins from grape seeds. Acta Pharm. Sin. 2001, 22, 1117–1120. [Google Scholar]
- Terra, X.; Pallarés, V.; Ardèvol, A.; Bladé, C.; Fernández-Larrea, J.; Pujadas, G.; Salvadó, J.; Arola, L.; Blay, M. Modulatory effect of grape-seed procyanidins on local and systemic inflammation in diet-induced obesity rats. J. Nutr. Biochem. 2011, 22, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, S.; Knirel, D.; Dietrich, H.; Flesch, M.; Erdmann, E.; Böhm, M. Inhibition of the PDGF receptor by red wine flavonoids provides a molecular explanation for the “French paradox”. FASEB J. 2002, 16, 1958–1960. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhu, L.H.; Jiang, H.; Tang, Q.Z.; Yan, L.; Wang, D.; Liu, C.; Bian, Z.Y.; Li, H. Grape seed proanthocyanidins attenuate vascular smooth muscle cell proliferation via blocking phosphatidylinositol 3-kinase-dependent signaling pathways. J. Cell. Physiol. 2010, 223, 713–726. [Google Scholar] [CrossRef] [PubMed]
- Vitseva, O.; Varghese, S.; Chakrabarti, S.; Folts, J.D.; Freedman, J.E. Grape seed and skin extracts inhibit platelet function and release of reactive oxygen intermediates. J. Cardiovasc. Pharm. 2005, 46, 445–451. [Google Scholar] [CrossRef]
- De Lange, D.W.; Verhoef, S.; Gorter, G.; Kraaijenhagen, R.J.; van de Wiel, A.; Akkerman, J.W. Polyphenolic grape extract inhibits platelet activation through PECAM-1: An explanation for the French paradox. Alcohol. Clin. Exp. Res. 2007, 31, 1308–1314. [Google Scholar] [CrossRef]
- Actis-Goretta, L.; Ottaviani, J.I.; Keen, C.L.; Fraga, C.G. Inhibition of angiotensin converting enzyme (ACE) activity by flavan-3-ols and procyanidins. Febs Lett. 2003, 555, 597–600. [Google Scholar] [CrossRef]
- Quiñones, M.; Guerrero, L.; Fernández-Vallinas, S.; Pons, Z.; Arola, L.; Aleixandre, A.; Muguerza, B. Involvement of nitric oxide and prostacyclin in the antihypertensive effect of low-molecular-weight procyanidin rich grape seed extract in male spontaneously hypertensive rats. J. Funct. Foods 2014, 6, 419–427. [Google Scholar] [CrossRef]
- Liu, X.; Qiu, J.; Zhao, S.; You, B.; Ji, X.; Wang, Y.; Cui, X.; Wang, Q.; Gao, H. Grape seed proanthocyanidin extract alleviates ouabain-induced vascular remodeling through regulation of endothelial function. Mol. Med. Rep. 2012, 6, 949–954. [Google Scholar] [CrossRef]
- Ghosh, J.; Murphy, M.O.; Turner, N.; Khwaja, N.; Halka, A.; Kielty, C.M.; Walker, M.G. The role of transforming growth factor beta1 in the vascular system. Cardiovasc. Pathol. 2005, 14, 28–36. [Google Scholar] [CrossRef]
- Huang, L.L.; Pan, C.; Wang, L.; Ding, L.; Guo, K.; Wang, H.Z.; Xu, A.M.; Gao, S. Protective effects of grape seed proanthocyanidins on cardiovascular remodeling in DOCA-salt hypertension rats. J. Nutr. Biochem. 2015, 26, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Pons, Z.; Margalef, M.; Bravo, F.I.; Arola-Arnal, A.; Muguerza, B. Grape seed flavanols decrease blood pressure via Sirt-1 and confer a vasoprotective pattern in rats. J. Funct. Foods 2016, 24, 164–172. [Google Scholar] [CrossRef]
- Church, D.F.; Pryor, W.A. Free-radical chemistry of cigarette smoke and its toxicological implications. Environ. Health Perspect. 1985, 64, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Georgakopoulos, D.; Bull, C.; Thomas, O.; Robinson, J.; Deanfield, J.E. Cigarette smoking is associated with dose-related and potentially reversible impairment of endothelium-dependent dilation in healthy young adults. Circulation 1993, 88, 2149–2155. [Google Scholar] [CrossRef]
- Lekakis, J.; Papamichael, C.; Vemmos, C.; Nanas, J.; Kontoyannis, D.; Stamatelopoulos, S.; Moulopoulos, S. Effect of acute cigarette smoking on endothelium-dependent brachial artery dilatation in healthy individuals. Am. J. Cardiol. 1997, 79, 529–531. [Google Scholar] [CrossRef]
- Burke, A.; Fitzgerald, G.A. Oxidative stress and smoking-induced vascular injury. Prog. Cardiovasc. Dis. 2013, 46, 79–90. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 10) | Low Dose (n = 10) | High Dose (n = 10) | Pc | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0w | 12w | Pa | 0w | 12w | Pa | P b | 0w | 12w | Pa | Pb | ||
| Age, years | 55.5 (6.9) | 53.5 (8.0) | 52.2 (8.6) | 0.644 d | ||||||||
| Smoker | 2 | 3 | 4 | 0.621 e | ||||||||
| Vascular functions | ||||||||||||
| Resting vascular diameter, mm | 3.82 (0.70) | 3.69 (0.67) | 0.182 | 3.68 (0.52) | 3.75 (0.56) | 0.492 | 0.163 | 3.85 (0.56) | 3.64 (0.44) | 0.236 | 0.764 | 0.809 d |
| Flow-mediated dilation (FMD), % | 4.2 (1.5) | 4.3 (1.7) | 0.262 | 5.4 (1.6) | 4.5 (3.1) | 0.349 | 0.362 | 4.6 (1.3) | 3.4 (2.4) | 0.162 | 0.189 | 0.187d |
| Baseline vascular diameter, mm | 3.84 (0.69) | 3.70 (0.70) | 0.132 | 3.69 (0.54) | 3.76 (0.55) | 0.399 | 0.083 | 3.85 (0.58) | 3.57 (0.46) | 0.136 | 0.538 | 0.799 d |
| Flow-mediated dilation from baseline (FMDb), % | 3.6 (1.9) | 4.2 (2.0) | 0.451 | 5.4 (2.4) | 4.3 (2.5) | 0.290 | 0.347 | 4.6 (2.2) | 5.6 (2.7) | 0.422 | 0.722 | 0.208 d |
| Intima-media thickness, mm | 0.33 (0.08) | 0.29 (0.08) | 0.192 | 0.27 (0.04) | 0.29 (0.06) | 0.469 | 0.103 | 0.27 (0.05) | 0.26 (0.04) | 0.832 | 0.250 | 0.068 d |
| Wall thickness-to-vascular diameter ratio | 0.09 (0.02) | 0.08 (0.02) | 0.355 | 0.08 (0.02) | 0.08 (0.02) | 0.741 | 0.287 | 0.07 (0.02) | 0.07 (0.01) | 0.726 | 0.248 | 0.126 d |
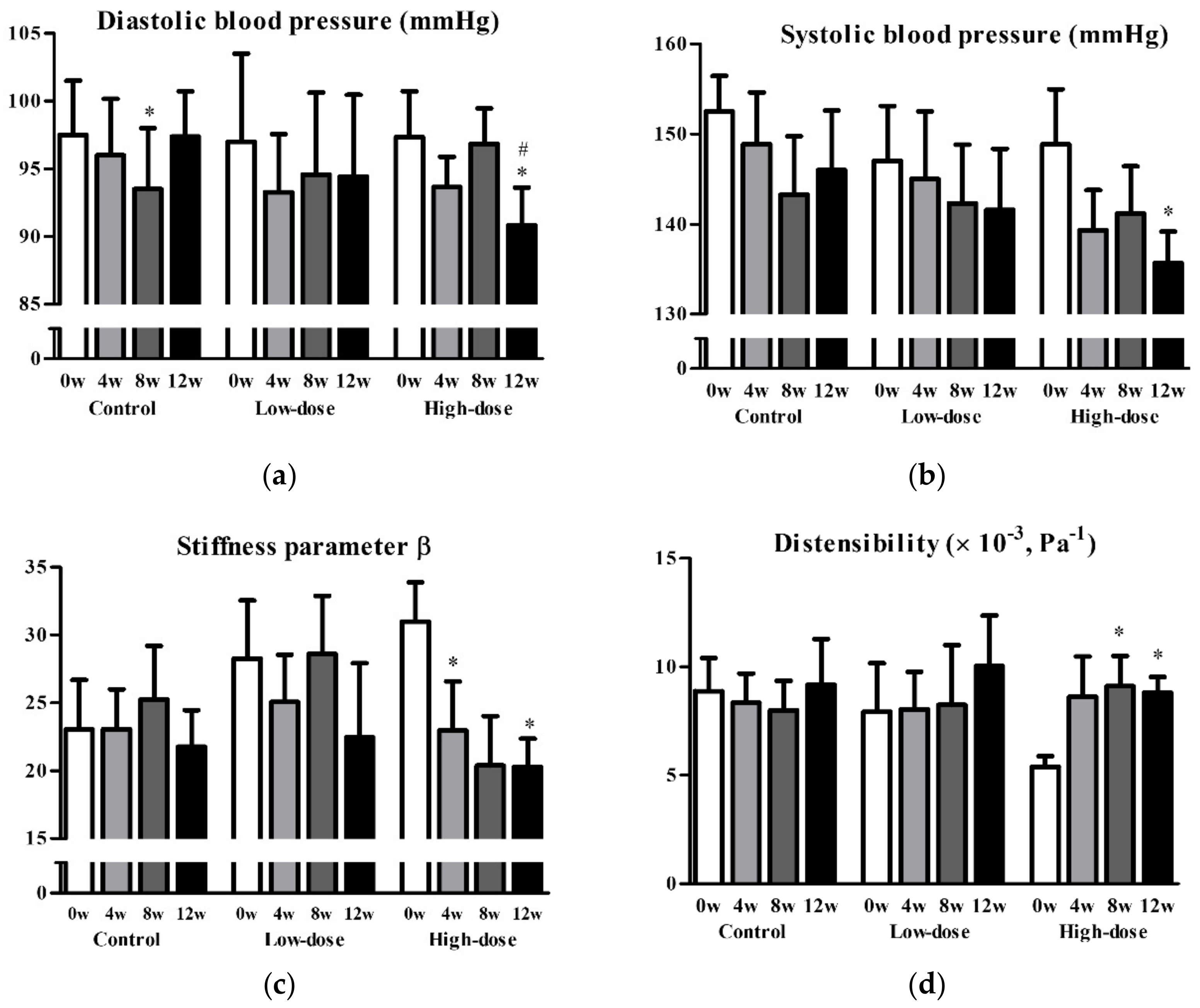
| Stiffness parameter β | 23.1 (9.4) | 19.8 (7.9) | 0.301 | 25.5 (11.1) | 21.7 (12.1) | 0.340 | 0.866 | 28.0 (7.1) | 20.6 (5.0) | 0.025 * | 0.353 | 0.426 d |
| Compliance (×10-2), mm2/Pa | 10.2 (5.8) | 10.3 (5.3) | 0.953 | 8.9 (5.2) | 10.7 (6.1) | 0.355 | 0.580 | 7.4 (3.5) | 8.9 (1.8) | 0.239 | 0.662 | 0.503 d |
| Distensibility (×10-3), Pa-1 | 8.8 (3.9) | 10.0 (5.6) | 0.510 | 8.4 (5.0) | 9.6 (5.2) | 0.463 | 0.859 | 6.1 (1.6) | 8.6 (1.7) | 0.004 ** | 0.654 | 0.387 d |
| Incremental elastic modulus (Einc), kPa | 1.6 (0.6) | 1.7 (0.8) | 0.931 | 2.1 (1.0) | 1.9 (1.1) | 0.309 | 0.380 | 2.53 (0.9) | 1.7 (0.4) | 0.018 * | 0.243 | 0.162 d |
| Pulse wave velocity (PWV), m/sec | 12.3 (2.5) | 11.6 (2.5) | 0.417 | 12.9 (3.2) | 12.2 (3.4) | 0.515 | 0.896 | 14.1 (2.0) | 11.7 (1.3) | 0.009 ** | 0.290 | 0.440 d |
| Other cardiovascular parameters | ||||||||||||
| Systolic blood pressure (SBP), mmHg | 150.1 (11.1) | 144.0 (17.0) | 0.201 | 144.0 (18.1) | 142.5 (17.1) | 0.706 | 0.411 | 148 (13.0) | 135.0 (12.6) | 0.028 * | 0.334 | 0.634 d |
| Diastolic blood pressure (DBP), mmHg | 98.4 (10.2) | 97.1 (8.4) | 0.489 | 95.9 (15.4) | 94.3 (13.6) | 0.637 | 0.991 | 96.0 (6.9) | 89.9 (7.9) | 0.062 | 0.150 | 0.858 d |
| Heart rate, min-1 | 69.9 (12.4) | 68.8 (9.4) | 0.685 | 72.6 (9.4) | 71.8 (11.4) | 0.837 | 1.000 | 67.0 (11.3) | 69.9 (13.9) | 0.375 | 0.404 | 0.537 d |
| Cardio-ankle vascular index | 8.5 (0.7) | 8.5 (0.7) | 1.000 | 8.1 (1.3) | 8.0 (1.1) | 0.885 | 0.738 | 7.6 (1.1) | 8.1 (0.9) | 0.067 | 0.577 | 0.749 d |
| Ankle-brachial pressure index | 1.12 (0.05) | 1.13 (0.08) | 0.686 | 1.10 (0.06) | 1.12 (0.06) | 0.336 | 0.711 | 1.13 (0.08) | 1.18 (0.06) | 0.135 | 0.290 | 0.551 d |
| High-density lipoprotein cholesterol, mg/dL | 63.3 (19.4) | 61.7 (10.0) | 0.647 | 70.6 (16.0) | 66.8 (15.7) | 0.244 | 0.416 | 77.9 (14.7) | 75.6 (11.7) | 0.375 | 0.573 | 0.171 d |
| Low-density lipoprotein cholesterol, mg/dL | 111.0 (25.4) | 115.6 (25.7) | 0.301 | 128.2 (37.1) | 126.1 (35.9) | 0.694 | 0.426 | 110.8 (32.5) | 112.1 (21.2) | 0.835 | 0.913 | 0.391 d |
| Oxidized low-density lipoprotein cholesterol, U/L | 116.6 (47.2) | 97.7 (38.2) | 0.262 | 115.8 (45.6) | 110.1 (48.4) | 0.705 | 0.608 | 106.2 (34.8) | 113.3 (29.5) | 0.507 | 0.171 | 0.834 d |
| Triglyceride, mg/dL | 99.9 (55.2) | 114.9 (46.8) | 0.234 | 87.9 (55.3) | 149.5 (125.6) | 0.096 | 0.262 | 103.5 (71.7) | 121.3 (74.4) | 0.116 | 0.917 | 0.838 d |
| Total cholesterol, mg/dL | 192.5 (26.5) | 196.2 (22.8) | 0.459 | 219.1 (31.8) | 219.1 (32.1) | 1.000 | 0.543 | 207.5 (41.1) | 207.4 (33.1) | 0.987 | 0.700 | 0.226 d |
| Body composition | ||||||||||||
| Height, cm | 158.7 (11.6) | 158.8 (11.4) | 0.986 | 159.1 (8.5) | 158.9 (8.4) | 0.963 | 0.154 | 159.6 (10.5) | 159.4 (10.4) | 0.961 | 0.117 | 0.982 d |
| Weight, kg | 59.4 (13.1) | 59.2 (13.1) | 0.524 | 58.9 (8.6) | 59.7 (8.6) | 0.076 | 0.060 | 57.6 (13.7) | 57.5 (12.6) | 0.844 | 0.558 | 0.945 d |
| Body mass index, kg/m2 | 23.4 (3.4) | 23.3 (3.5) | 0.311 | 23.4 (3.7) | 23.7 (3.8) | 0.050 * | 0.024 * | 22.5 (3.9) | 22.5 (3.7) | 0.751 | 0.299 | 0.586 d |
| Fat mass, kg | 17.5 (7.1) | 17.1 (7.4) | 0.175 | 17.9 (7.2) | 17.9 (7.6) | 0.969 | 0.340 | 15.4 (7.9) | 15.5 (7.4) | 0.744 | 0.842 | 0.722 d |
| Lean body mass, kg | 41.9 (9.7) | 42.1 (9.4) | 0.050 | 41.0 (5.1) | 41.8 (5.7) | 0.744 | 0.219 | 42.2 (9.2) | 42.0 (8.9) | 0.444 | 0.242 | 0.944 d |
| Muscle mass, kg | 39.6 (9.2) | 39.8 (8.9) | 0.331 | 38.7 (4.9) | 39.5 (5.4) | 0.047 * | 0.210 | 39.9 (8.8) | 39.7 (8.5) | 0.961 | 0.228 | 0.882 d |
| Water mass, kg | 30.0 (5.8) | 30.1 (5.6) | 0.512 | 29.5 (3.0) | 30.6 (3.7) | 0.035 * | 0.508 | 29.7 (5.2) | 29.6 (5.0) | 0.771 | 0.537 | 0.942 d |
| Basal metabolic rate, MJ/day | 5.04 (1.06) | 5.05 (1.04) | 0.574 | 4.95 (0.53) | 5.04 (0.57) | 0.027 * | 0.085 | 5.05 (1.04) | 5.02 (0.98) | 0.500 | 0.432 | 0.966 d |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odai, T.; Terauchi, M.; Kato, K.; Hirose, A.; Miyasaka, N. Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2019, 11, 2844. https://doi.org/10.3390/nu11122844
Odai T, Terauchi M, Kato K, Hirose A, Miyasaka N. Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients. 2019; 11(12):2844. https://doi.org/10.3390/nu11122844
Chicago/Turabian StyleOdai, Tamami, Masakazu Terauchi, Kiyoko Kato, Asuka Hirose, and Naoyuki Miyasaka. 2019. "Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study" Nutrients 11, no. 12: 2844. https://doi.org/10.3390/nu11122844
APA StyleOdai, T., Terauchi, M., Kato, K., Hirose, A., & Miyasaka, N. (2019). Effects of Grape Seed Proanthocyanidin Extract on Vascular Endothelial Function in Participants with Prehypertension: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients, 11(12), 2844. https://doi.org/10.3390/nu11122844