Multiple Sclerosis Patients Show Lower Bioavailable 25(OH)D and 1,25(OH)2D, but No Difference in Ratio of 25(OH)D/24,25(OH)2D and FGF23 Concentrations

Abstract
1. Introduction
2. Materials and Methods
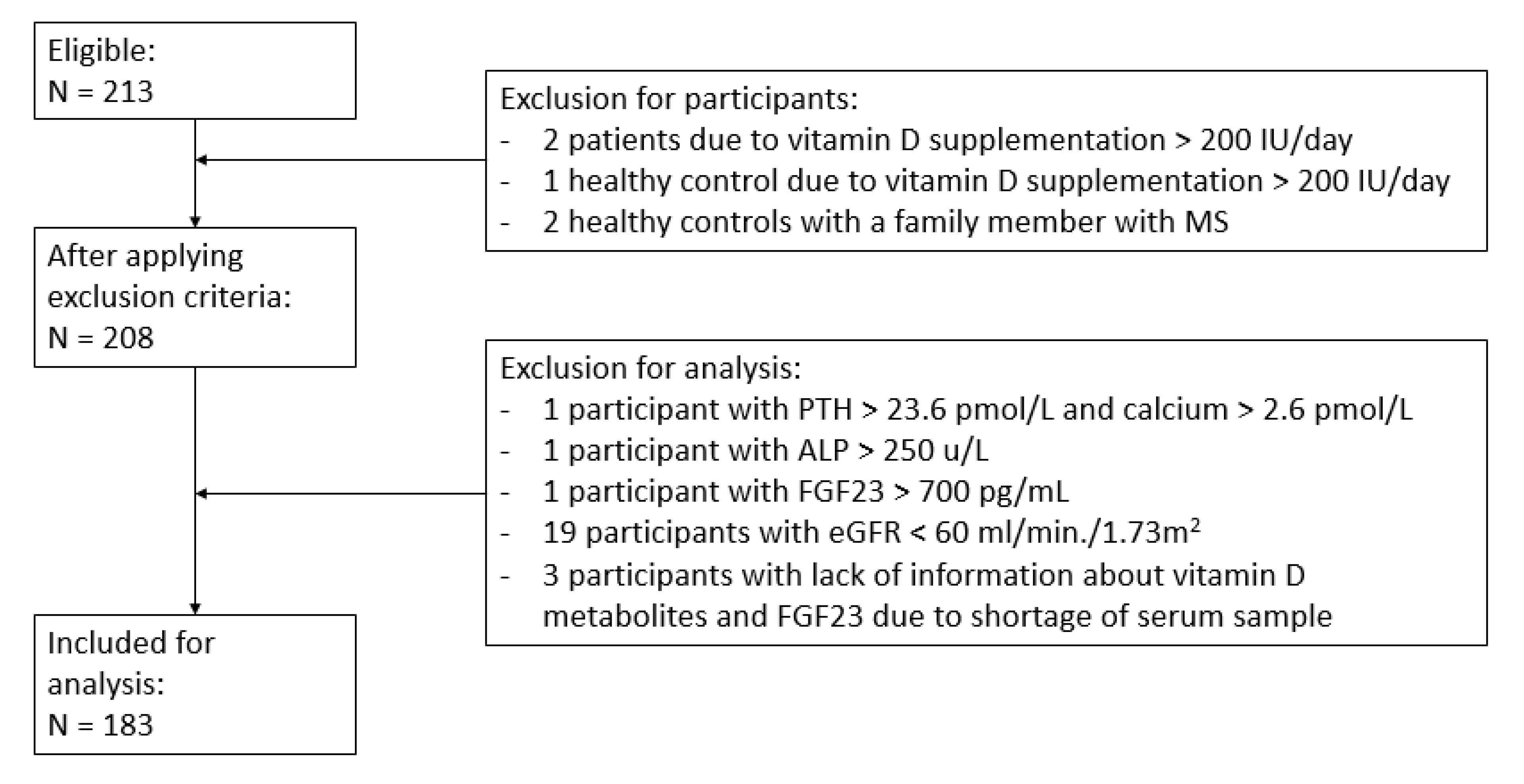
2.1. Subjects and Study Protocol
2.2. Measurements
2.2.1. General
2.2.2. Vitamin D Metabolites
2.2.3. Free and Bioavailable Vitamin D Metabolites
2.2.4. Bone Turnover Markers (BTMs)
2.2.5. Other Measurements
2.3. Statistical Analysis
3. Results
3.1. General
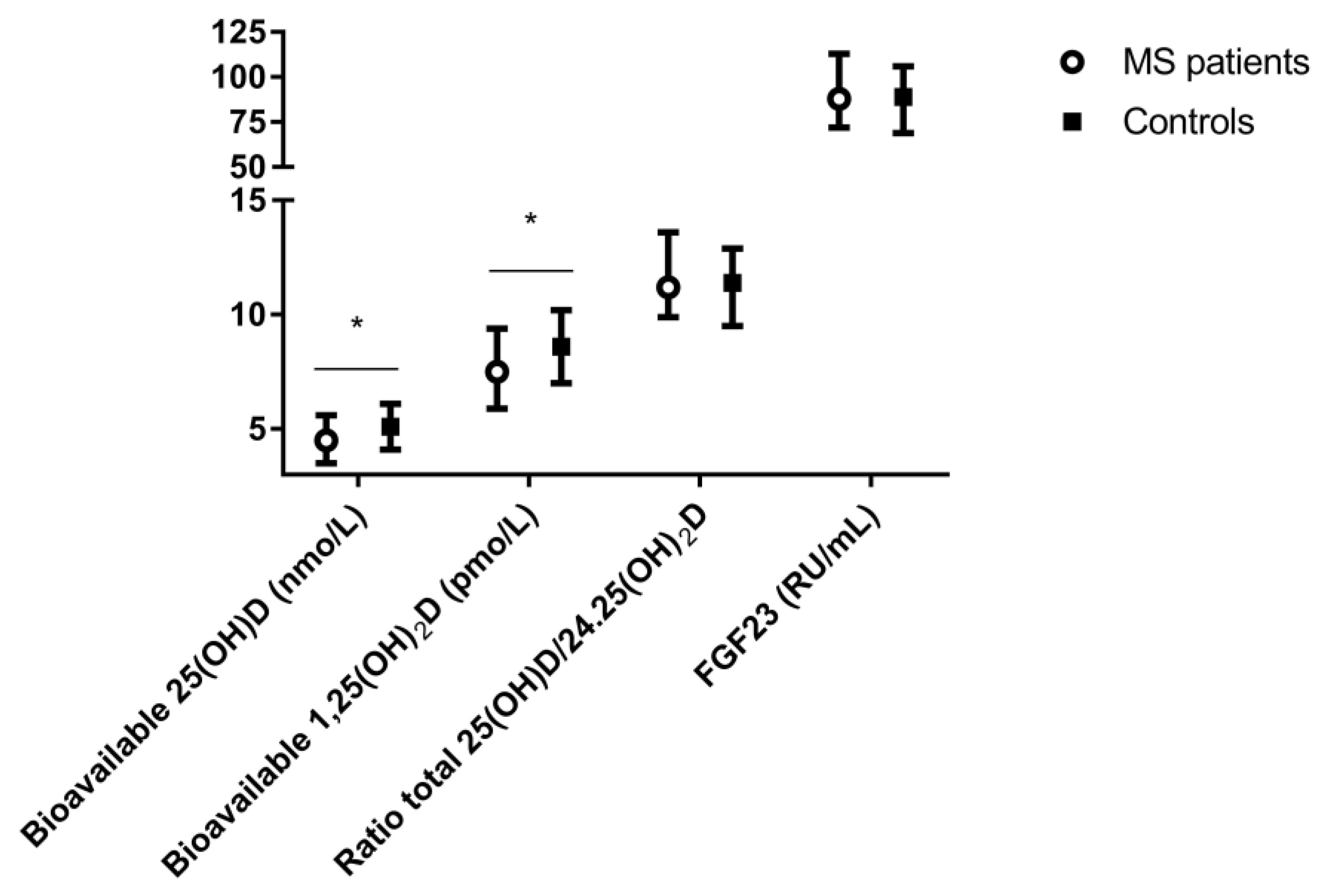
3.2. Vitamin D Metabolites, FGF23, and Bone Turnover Markers
3.3. Associations
3.3.1. Associations between Vitamin D Metabolites, FGF23, Bone Turnover Markers, and EDSS in MS Patients
3.3.2. Associations Based on Gender of MS Patients
3.3.3. Associations in Healthy Controls
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gupta, S.; Ahsan, I.; Mahfooz, N.; Abdelhamid, N.; Ramanathan, M.; Weinstock-Guttman, B. Osteoporosis and Multiple Sclerosis: Risk Factors, Pathophysiology, and Therapeutic Interventions. CNS Drugs 2014, 28, 731–742. [Google Scholar] [CrossRef]
- Holmøy, T.; Kampman, M.T.; Smolders, J. Vitamin D in multiple sclerosis: Implications for assessment and treatment. Expert Rev. Neurother. 2012, 12, 1101–1112. [Google Scholar] [CrossRef]
- Huang, Z.; Qi, Y.; Du, S.; Chen, G.; Yan, W. BMI levels with MS Bone mineral density levels in adults with multiple sclerosis: A meta-analysis. Int. J. Neurosci. 2015, 125, 904–912. [Google Scholar] [CrossRef]
- Nieves, J.; Cosman, F.; Herbert, J.; Shen, V.; Lindsay, R. High prevalence of vitamin D deficiency and reduced bone mass in multiple sclerosis. Neurology 1994, 44, 1687. [Google Scholar] [CrossRef] [PubMed]
- Moen, S.M.; Celius, E.G.; Sandvik, L.; Nordsletten, L.; Eriksen, E.F.; Holmøy, T. Low bone mass in newly diagnosed multiple sclerosis and clinically isolated syndrome. Neurology 2011, 77, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Steffensen, L.H.; Mellgren, S.I.; Kampman, M.T. Predictors and prevalence of low bone mineral density in fully ambulatory persons with multiple sclerosis. J. Neurol. 2010, 257, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Ramagopalan, S.; Giovannoni, G.; Bazelier, M.T.; De Vries, F. Risk of fractures in patients with multiple sclerosis: A population-based cohort study. Neurology 2012, 79, 1934–1935. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef]
- Tobore, T.O. Towards a Comprehensive Etiopathogenetic and Pathophysiological Theory of Multiple Sclerosis. Int. J. Neurosci. 2019, 1–41. [Google Scholar] [CrossRef]
- Acheson, E.D.; Bachrach, C.A.; Wright, F.M. Some comments on the relationship of the distribution of multiple sclerosis to latitude, solar radiation, and other variables. Acta Psychiatr. Scand. 1960, 35, 132–147. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Geography in multiple sclerosis. J. Neurol. 1977, 215, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Hemmer, B.; Kerschensteiner, M.; Korn, T. Role of the innate and adaptive immune responses in the course of multiple sclerosis. Lancet Neurol. 2015, 14, 406–419. [Google Scholar] [CrossRef]
- Kragt, J.; Van Amerongen, B.; Killestein, J.; Dijkstra, C.; Uitdehaag, B.; Polman, C.; Lips, P. Higher levels of 25-hydroxyvitamin D are associated with a lower incidence of multiple sclerosis only in women. Mult. Scler. J. 2009, 15, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Munger, K.L.; Levin, L.I.; Hollis, B.W.; Howard, N.S.; Ascherio, A. Serum 25-Hydroxyvitamin D Levels and Risk of Multiple Sclerosis. JAMA 2006, 296, 2832–2838. [Google Scholar] [CrossRef]
- Soilu-Hänninen, M.; Airas, L.; Mononen, I.; Heikkilä, A.; Viljanen, M.; Hänninen, A. 25-Hydroxyvitamin D levels in serum at the onset of multiple sclerosis. Mult. Scler. J. 2005, 11, 266–271. [Google Scholar] [CrossRef]
- Berezowska, M.; Coe, S.; Dawes, H. Effectiveness of Vitamin D Supplementation in the Management of Multiple Sclerosis: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 1301. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Munger, K.L.; Köchert, K.; Arnason, B.G.W.; Comi, G.; Cook, S.; Goodin, D.S.; Filippi, M.; Hartung, H.-P.; Jeffery, D.R.; et al. Association of Vitamin D Levels With Multiple Sclerosis Activity and Progression in Patients Receiving Interferon Beta-1b. JAMA Neurol. 2015, 72, 1458–1465. [Google Scholar] [CrossRef]
- Holmøy, T.; Lindstrøm, J.C.; Eriksen, E.F.; Steffensen, L.H.; Kampman, M.T. High dose vitamin D supplementation does not affect biochemical bone markers in multiple sclerosis—A randomized controlled trial. BMC Neurol. 2017, 17, 67. [Google Scholar] [CrossRef]
- Jagannath, V.A.; Filippini, G.; Di Pietrantonj, C.; Asokan, G.V.; Robak, E.W.; Whamond, L.; Robinson, S.A. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst. Rev. 2018, 9, CD008422. [Google Scholar] [CrossRef]
- Sintzel, M.B.; Rametta, M.; Reder, A.T. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol. Ther. 2018, 7, 59–85. [Google Scholar] [CrossRef]
- Rinaldi, A.O.; Sanseverino, I.; Purificato, C.; Cortese, A.; Mechelli, R.; Francisci, S.; Salvetti, M.; Millefiorini, E.; Gessani, S.; Gauzzi, M.C. Increased Circulating Levels of Vitamin D Binding Protein in MS Patients. Toxins 2015, 7, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Majid, K.-B.; Stefferl, A.; Bourquin, C.; Lassmann, H.; Linington, C.; Olsson, T.; Kleinau, S.; Harris, R.A. Fc receptors are critical for autoimmune inflammatory damage to the central nervous system in experimental autoimmune encephalomyelitis. Scand. J. Immunol. 2002, 55, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Binder, R.; Kress, A.; Kan, G.; Herrmann, K.; Kirschfink, M. Neutrophil priming by cytokines and vitamin D binding protein (Gc-globulin): Impact on C5a-mediated chemotaxis, degranulation and respiratory burst. Mol. Immunol. 1999, 36, 885–892. [Google Scholar] [CrossRef]
- Gauzzi, M.C. Vitamin D-binding protein and multiple sclerosis: Evidence, controversies, and needs. Mult. Scler. J. 2018, 24, 1526–1535. [Google Scholar] [CrossRef]
- Vasconcellos, C.; Lind, S. Coordinated inhibition of actin-induced platelet aggregation by plasma gelsolin and vitamin D-binding protein. Blood 1993, 82, 3648–3657. [Google Scholar] [CrossRef]
- Vogel, D.Y.; Vereyken, E.J.; Glim, J.E.; Heijnen, P.D.; Moeton, M.; Van Der Valk, P.; Amor, S.; Teunissen, C.E.; Van Horssen, J.; Dijkstra, C.D. Macrophages in inflammatory multiple sclerosis lesions have an intermediate activation status. J. Neuroinflamm. 2013, 10, 35. [Google Scholar] [CrossRef]
- Bermúdez-Morales, V.H.; Fierros, G.; Lopez, R.L.; Martínez-Nava, G.; Flores-Aldana, M.; Flores-Rivera, J.; Hernández-Girón, C. Vitamin D receptor gene polymorphisms are associated with multiple sclerosis in Mexican adults. J. Neuroimmunol. 2017, 306, 20–24. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Lucas, R.M.; Xiang, A.H.; Wu, J.; Chen, L.H.; Gonzales, E.; Haraszti, S.; Smith, J.B.; Quach, H.; Barcellos, L.F. Vitamin D-Binding Protein Polymorphisms, 25-Hydroxyvitamin D, Sunshine and Multiple Sclerosis. Nutrients 2018, 10, 184. [Google Scholar] [CrossRef]
- Weinstock-Guttman, B.; Zivadinov, R.; Qu, J.; Cookfair, D.; Duan, X.; Bang, E.; Bergsland, N.; Hussein, S.; Cherneva, M.; Willis, L.; et al. Vitamin D metabolites are associated with clinical and MRI outcomes in multiple sclerosis patients. J. Neurol. Neurosurg. Psychiatry 2011, 82, 189–195. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dietrich, T.; Orav, E.; Dawson-Hughes, B. Positive association between 25-hydroxy vitamin d levels and bone mineral density: A population-based study of younger and older adults. Am. J. Med. 2004, 116, 634–639. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Stunes, A.K.; Kubiak, J.; Joakimsen, R.; Grimnes, G.; Thorsby, P.M.; Syversen, U. Effects of vitamin D supplementation on bone turnover markers and other bone-related substances in subjects with vitamin D deficiency. Bone 2019, 124, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Bolland, M.J.; Grey, A.B.; Ames, R.W.; Horne, A.M.; Mason, B.H.; Wattie, D.J.; Gamble, G.D.; Bouillon, R.; Reid, I.R. Age-, gender-, and weight-related effects on levels of 25-hydroxyvitamin D are not mediated by vitamin D binding protein. Clin. Endocrinol. 2007, 67, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Spach, K.M.; Hayes, C.E. Vitamin D3 confers protection from autoimmune encephalomyelitis only in female mice. J. Immunol. 2005, 175, 4119–4126. [Google Scholar] [CrossRef] [PubMed]
- Woolmore, J.; Stone, M.; Pye, E.; Partridge, J.; Boggild, M.; Young, C.; Jones, P.; Fryer, A.; Hawkins, C.; Strange, R.; et al. Studies of associations between disability in multiple sclerosis, skin type, gender and ultraviolet radiation. Mult. Scler. J. 2007, 13, 369–375. [Google Scholar] [CrossRef]
- Yang, M.; Qin, Z.; Zhu, Y.; Li, Y.; Qin, Y.; Jing, Y.; Liu, S. Vitamin D-binding Protein in Cerebrospinal Fluid is Associated with Multiple Sclerosis Progression. Mol. Neurobiol. 2013, 47, 946–956. [Google Scholar] [CrossRef]
- Meyer-Moock, S.; Feng, Y.-S.; Maeurer, M.; Dippel, F.-W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef]
- Dirks, N.F.; Vesper, H.W.; Van Herwaarden, A.E.; Ouweland, J.M.V.D.; Kema, I.P.; Krabbe, J.G.; Heijboer, A.C. Various calibration procedures result in optimal standardization of routinely used 25(OH)D ID-LC-MS/MS methods. Clin. Chim. Acta 2016, 462, 49–54. [Google Scholar] [CrossRef]
- Dirks, N.F.; Ackermans, M.T.; De Jonge, R.; Heijboer, A.C. Reference values for 24,25-dihydroxyvitamin D and the 25-hydroxyvitamin D/24,25-dihydroxyvitamin D ratio. Clin. Chem. Lab. Med. 2019, 57, e259–e261. [Google Scholar] [CrossRef]
- Dirks, N.F.; Martens, F.; Vanderschueren, D.; Billen, J.; Pauwels, S.; Ackermans, M.T.; Endert, E.; Heijer, M.D.; Blankenstein, M.A.; Heijboer, A.C. Determination of human reference values for serum total 1,25-dihydroxyvitamin D using an extensively validated 2D ID-UPLC–MS/MS method. J. Steroid Biochem. Mol. Boil. 2016, 164, 127–133. [Google Scholar] [CrossRef]
- Malmstroem, S.; Rejnmark, L.; Imboden, J.B.; Shoback, D.M.; Bikle, D.D. Current Assays to Determine Free 25-Hydroxyvitamin D in Serum. J. AOAC Int. 2017, 100, 1323–1327. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D.; Siiteri, P.K.; Ryzen, E.; Haddad, J.; Gee, E. Serum Protein Binding of 1,25-Dihydroxyvitamin D: A Reevaluation by Direct Measurement of Free Metabolite Levels. J. Clin. Endocrinol. Metab. 1985, 61, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A Critical Evaluation of Simple Methods for the Estimation of Free Testosterone in Serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef] [PubMed]
- Powe, C.E.; Ricciardi, C.; Berg, A.H.; Erdenesanaa, D.; Collerone, G.; Ankers, E.; Wenger, J.; Karumanchi, S.A.; Thadhani, R.; Bhan, I. Vitamin D–Binding Protein Modifies the Vitamin D–Bone Mineral Density Relationship. J. Bone Miner. Res. 2011, 26, 1609–1616. [Google Scholar] [CrossRef]
- Heijboer, A.C.; Levitus, M.; Vervloet, M.G.; Lips, P.; Wee, P.M.T.; Dijstelbloem, H.M.; Blankenstein, M.A. Determination of fibroblast growth factor 23. Ann. Clin. Biochem. Int. J. Lab. Med. 2009, 46, 338–340. [Google Scholar] [CrossRef]
- Emami Aleagha, M.S.; Siroos, B.; Allameh, A.; Shakiba, S.; Ranji-Burachaloo, S.; Harirchian, M.H. Calcitriol, but not FGF23, increases in CSF and serum of MS patients. J. Neuroimmunol. 2018, 328, 89–93. [Google Scholar] [CrossRef]
- Ellidag, H.Y.; Yilmaz, N.; Kurtulus, F.; Aydin, O.; Eren, E.; Inci, A.; Dolu, S.; Ince, F.D.A.; Giray, Ö.; Yaman, A. The Three Sisters of Fate in Multiple Sclerosis: Klotho (Clotho), Fibroblast Growth Factor-23 (Lachesis), and Vitamin D (Atropos). Ann. Neurosci. 2016, 23, 155–161. [Google Scholar] [CrossRef]
- Stein, M.S.; Ward, G.J.; Butzkueven, H.; Kilpatrick, T.J.; Harrison, L.C. Dysequilibrium of the PTH-FGF23-vitamin D axis in relapsing remitting multiple sclerosis; a longitudinal study. Mol. Med. 2018, 24, 27. [Google Scholar] [CrossRef]
- Barnes, M.; Bonham, M.; Robson, P.; Strain, J.; Lowe-Strong, A.; Eaton-Evans, J.; Ginty, F.; Wallace, J.; Robson, P. Assessment of 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D3 concentrations in male and female multiple sclerosis patients and control volunteers. Mult. Scler. J. 2007, 13, 670–672. [Google Scholar] [CrossRef]
- Soilu-Hänninen, M.; Laaksonen, M.; Laitinen, I.; Erälinna, J.-P.; Lilius, E.-M.; Mononen, I. A longitudinal study of serum 25-hydroxyvitamin D and intact parathyroid hormone levels indicate the importance of vitamin D and calcium homeostasis regulation in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 152–157. [Google Scholar] [CrossRef]
- Correale, J.; Ysrraelit, M.C.; Gaitán, M.I. Immunomodulatory effects of Vitamin D in multiple sclerosis. Brain 2009, 132, 1146–1160. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Weinstock-Guttman, B.; Wang, H.; Bang, E.; Li, J.; Ramanathan, M.; Qu, J. Ultrasensitive Quantification of Serum Vitamin D Metabolites Using Selective Solid-Phase Extraction Coupled to Microflow Liquid Chromatography and Isotope-Dilution Mass Spectrometry. Anal. Chem. 2010, 82, 2488–2497. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Cree, B.A.C.; McElroy, J.; Oksenberg, J.; Green, R.; Mowry, E.M.; Miller, J.W.; Hauser, S.L.; Green, A.J. Vitamin D in African Americans with multiple sclerosis. Neurology 2011, 76, 1824–1830. [Google Scholar] [CrossRef] [PubMed]
- Lucas, R.M.; Ponsonby, A.-L.; Dear, K.; Valery, P.C.; Pender, M.P.; Taylor, B.V.; Kilpatrick, T.; Dwyer, T.; Coulthard, A.; Chapman, C.; et al. Sun exposure and vitamin D are independent risk factors for CNS demyelination. Neurology 2011, 76, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Ozgocmen, S.; Bulut, S.; Ilhan, N.; Gulkesen, A.; Ardicoglu, O.; Ozkan, Y. Vitamin D deficiency and reduced bone mineral density in multiple sclerosis: Effect of ambulatory status and functional capacity. J. Bone Miner. Metab. 2005, 23, 309–313. [Google Scholar] [CrossRef]
- Shaygannejad, V.; Golabchi, K.; Haghighi, S.; Dehghan, H.; Moshayedi, A. A Comparative Study of 25 (OH) Vitamin D Serum Levels in Patients with Multiple Sclerosis and Control Group in Isfahan, Iran. Int. J. Prev. Med. 2010, 1, 195–201. [Google Scholar]
- Van der Mei, I.A.; Ponsonby, A.L.; Dwyer, T.; Blizzard, L.; Taylor, B.V.; Kilpatrick, T.; Butzkueven, H.; McMichael, A.J. Vitamin D levels in people with multiple sclerosis and community controls in Tasmania, Australia. J. Neurol. 2007, 254, 581–590. [Google Scholar]
- Bhan, I.; Powe, C.E.; Berg, A.H.; Ankers, E.; Wenger, J.B.; Karumanchi, S.A.; Thadhani, R.I. Bioavailable vitamin D is more tightly linked to mineral metabolism than total vitamin D in incident hemodialysis patients. Kidney Int. 2012, 82, 84–89. [Google Scholar] [CrossRef]
- Bikle, D.D.; Gee, E.; Halloran, B.; Haddad, J.G. Free 1,25-dihydroxyvitamin D levels in serum from normal subjects, pregnant subjects, and subjects with liver disease. J. Clin. Investig. 1984, 74, 1966–1971. [Google Scholar] [CrossRef]
- Bikle, D.D.; Gee, E.; Halloran, B.; Kowalski, M.A.; Ryzen, E.; Haddad, J.G. Assessment of the Free Fraction of 25-Hydroxyvitamin D in Serum and Its Regulation by Albumin and the Vitamin D-Binding Protein. J. Clin. Endocrinol. Metab. 1986, 63, 954–959. [Google Scholar] [CrossRef]
- Jassil, N.K.; Sharma, A.; Bikle, D.; Wang, X. Vitamin d binding protein and 25-hydroxyvitamin d levels: Emerging clinical applications. Endocr. Pract. 2017, 23, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Ji, M.; Song, J.; Moon, H.-W.; Hur, M.; Yun, Y.-M. Clinical Utility of Measurement of Vitamin D-Binding Protein and Calculation of Bioavailable Vitamin D in Assessment of Vitamin D Status. Ann. Lab. Med. 2017, 37, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Mendel, C.M. Rates of dissociation of sex steroid hormones from human sex hormone-binding globulin: A reassessment. J. Steroid Biochem. Mol. Boil. 1990, 37, 251–255. [Google Scholar] [CrossRef]
- Behrens, J.R.; Rasche, L.; Gieß, R.M.; Pfuhl, C.; Wakonig, K.; Freitag, E.; Deuschle, K.; Bellmann-Strobl, J.; Paul, F.; Ruprecht, K.; et al. Low 25-hydroxyvitamin D, but not the bioavailable fraction of 25-hydroxyvitamin D, is a risk factor for multiple sclerosis. Eur. J. Neurol. 2016, 23, 62–67. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.J.; Murray, B.; Lonergan, R.; Segurado, R.; Tubridy, N.; Kilbane, M.T. Analysing the effect of multiple sclerosis on vitamin D related biochemical markers of bone remodelling. J. Steroid Biochem. Mol. Boil. 2018, 177, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Moen, S.M.; Celius, E.G.; Sandvik, L.; Brustad, M.; Nordsletten, L.; Eriksen, E.F.; Holmøy, T. Bone Turnover and Metabolism in Patients with Early Multiple Sclerosis and Prevalent Bone Mass Deficit: A Population-Based Case-Control Study. PLoS ONE 2012, 7, e45703. [Google Scholar] [CrossRef]
- Štěpán, J.J.; Havrdova, E.K.; Tyblova, M.; Horakova, D.; Tichá, V.; Nováková, I.; Zikán, V. Markers of bone remodeling predict rate of bone loss in multiple sclerosis patients treated with low dose glucocorticoids. Clin. Chim. Acta 2004, 348, 147–154. [Google Scholar] [CrossRef]
- Niino, M.; Sato, S.; Fukazawa, T.; Masaki, K.; Miyazaki, Y.; Matsuse, D.; Yamasaki, R.; Takahashi, E.; Kikuchi, S.; Kira, J.-I. Decreased serum vitamin D levels in Japanese patients with multiple sclerosis. J. Neuroimmunol. 2015, 279, 40–45. [Google Scholar] [CrossRef]
- Disanto, G.; Ramagopalan, S.V.; Para, A.E.; Handunnetthi, L. The emerging role of vitamin D binding protein in multiple sclerosis. J. Neurol. 2011, 258, 353–358. [Google Scholar] [CrossRef]
- Kułakowska, A.; Tarasiuk, J.; Kapica-Topczewska, K.; Chorąży, M.; Pogorzelski, R.; Kulczyńska-Przybik, A.; Mroczko, B.; Bucki, R. Pathophysiological implications of actin-free Gc-globulin concentration changes in blood plasma and cerebrospinal fluid collected from patients with Alzheimer’s disease and other neurological disorders. Adv. Clin. Exp. Med. 2018, 27, 1075–1080. [Google Scholar] [CrossRef]
- Adams, J.S.; Ren, S.; Liu, P.T.; Chun, R.F.; Lagishetty, V.; Gombart, A.F.; Borregaard, N.; Modlin, R.L.; Hewison, M. Vitamin d-directed rheostatic regulation of monocyte antibacterial responses. J. Immunol. 2009, 182, 4289–4295. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Lauridsen, A.L.; Suon, L.; Zella, L.A.; Pike, J.W.; Modlin, R.L.; Martineau, A.R.; Wilkinson, R.J.; Adams, J.; Hewison, M. Vitamin D-binding protein directs monocyte responses to 25-hydroxy- and 1,25-dihydroxyvitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 3368–3376. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-Like Receptor Triggering of a Vitamin D-Mediated Human Antimicrobial Response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Zella, L.A.; Shevde, N.K.; Hollis, B.W.; Cooke, N.E.; Pike, J.W. Vitamin D-binding protein influences total circulating levels of 1,25-dihydroxyvitamin D3 but does not directly modulate the bioactive levels of the hormone in vivo. Endocrinology 2008, 149, 3656–3667. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, A.G.; Errea, O.; van Wijngaarden, P.; Gonzalez, G.A.; Kerninon, C.; Jarjour, A.A.; Lewis, H.J.; Jones, C.A.; Nait-Oumesmar, B.; Zhao, C.; et al. Vitamin D receptor-retinoid X receptor heterodimer signaling regulates oligodendrocyte progenitor cell differentiation. J. Cell Biol. 2015, 211, 975–985. [Google Scholar] [CrossRef]
- Kongsbak, M.; Von Essen, M.R.; Levring, T.B.; Schjerling, P.; Woetmann, A.; Ødum, N.; Bonefeld, C.M.; Geisler, C. Vitamin D-binding protein controls T cell responses to vitamin D. BMC Immunol. 2014, 15, 35. [Google Scholar] [CrossRef]
- Yamamoto, E.; Jørgensen, T.N. Immunological effects of vitamin D and their relations to autoimmunity. J. Autoimmun. 2019, 100, 7–16. [Google Scholar] [CrossRef]
- Bar-Or, A. The Immunology of Multiple Sclerosis. Semin. Neurol. 2008, 28, 29–45. [Google Scholar] [CrossRef]
- Brown, J.; Bianco, J.I.; McGrath, J.J.; Eyles, D.W. 1,25-dihydroxyvitamin D3 induces nerve growth factor, promotes neurite outgrowth and inhibits mitosis in embryonic rat hippocampal neurons. Neurosci. Lett. 2003, 343, 139–143. [Google Scholar] [CrossRef]
- Neveu, I.; Naveilhan, P.; Baudet, C.; Brachet, P.; Metsis, M. 1,25-Dihydroxyvitamin D3 regulates NT-3, NT-4 but not BDNF mRNA in astrocytes. NeuroReport 1994, 6, 124–126. [Google Scholar] [CrossRef]
- Neveu, I.; Naveilhan, P.; Jehan, F.; Baudet, C.; Wion, D.; De Luca, H.F.; Brachet, P. 1,25-Dihydroxyvitamin D3 regulates the synthesis of nerve growth factor in primary cultures of glial cells. Mol. Brain Res. 1994, 24, 70–76. [Google Scholar] [CrossRef]
- Smolders, J.; Schuurman, K.G.; Van Strien, M.E.; Melief, J.; Hendrickx, D.; Hol, E.; Van Eden, C.; Luchetti, S.; Huitinga, I. Expression of Vitamin D Receptor and Metabolizing Enzymes in Multiple Sclerosis–Affected Brain Tissue. J. Neuropathol. Exp. Neurol. 2013, 72, 91–105. [Google Scholar] [PubMed]
- Smolders, J.; Damoiseaux, J. Vitamin D as a T-cell Modulator in Multiple Sclerosis. Vitam. Horm. 2011, 86, 401–428. [Google Scholar] [PubMed]
- Chun, R.F.; Peercy, B.E.; Orwoll, E.S.; Nielson, C.M.; Adams, J.S.; Hewison, M. Vitamin D and DBP: The free hormone hypothesis revisited. J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 132–137. [Google Scholar] [CrossRef]
- Delanghe, J.R.; Speeckaert, R.; Speeckaert, M.M. Behind the scenes of vitamin D binding protein: More than vitamin D binding. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 773–786. [Google Scholar] [CrossRef]
- Casetta, I.; Riise, T.; Nortvedt, M.W.; Economou, N.T.; De Gennaro, R.; Fazio, P.; Cesnik, E.; Govoni, V.; Granieri, E. Gender differences in health-related quality of life in multiple sclerosis. Mult. Scler. J. 2009, 15, 1339–1346. [Google Scholar] [CrossRef]
- Rojas, J.I.; Sánchez, F.; Patrucco, L.; Miguez, J.; Funes, J.; Cristiano, E. Structural sex differences at disease onset in multiple sclerosis patients. Neuroradiol. J. 2016, 29, 368–371. [Google Scholar] [CrossRef]
- Niedziela, N.; Pierzchała, K.; Zalejska-Fiolka, J.; Niedziela, J.T.; Romuk, E.; Torbus-Paluszczak, M.; Adamczyk-Sowa, M. Assessment of Biochemical and Densitometric Markers of Calcium-Phosphate Metabolism in the Groups of Patients with Multiple Sclerosis Selected due to the Serum Level of Vitamin D3. BioMed Res. Int. 2018, 2018, 9329123. [Google Scholar] [CrossRef]
- Terzi, T.; Terzi, M.; Tander, B.; Cantürk, F.; Onar, M. Changes in bone mineral density and bone metabolism markers in premenopausal women with multiple sclerosis and the relationship to clinical variables. J. Clin. Neurosci. 2010, 17, 1260–1264. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients (n = 91) | Controls (n = 92) | p Value a | Reference Range | |
|---|---|---|---|---|
| Age, yr (mean ± SD) | 45 ± 11 | 42 ± 11 | 0.30 | |
| Female of total population (%) | 67 | 41 | <0.01 * | |
| Postmenopausal of total population (%) | 34 | 16 | 0.04 * | |
| Caucasian (%) | 98 | 95 | 0.44 | |
| eGFR, mL/min/1.73m2 (median, IQR) | 71 (66–81) | 71 (67–78) | 0.42 | >60 |
| MS subtype (%) | n.a. | |||
| RRMS | 57 | |||
| SPMS | 24 | |||
| PPMS | 14 | |||
| CIS | 1 | |||
| Disease duration, yr (median, IQR) | 10 (5–16) | n.a. | ||
| EDSS (median, IQR) | 4 (3–6) | n.a. | ||
| Use of vitamin D supplements b, (%) | 40 | 14 | <0.01 * | |
| Use of using disease modifying therapy, (%) | 32 | n.a. | ||
| Total 25(OH)D, nmol/L | 75 (59–93) | 77 (67–98) | 0.06 # | >50 |
| Total 1.25(OH)2D, pmol/L | 105 (74–143) | 99 (79–133) | 0.57 | 59–159 |
| 25(OH)D2, nmol/L | 1.1 (0.8–1.5) | 1.2 (0.9–1.5) | 0.66 | |
| 25(OH)D3, nmol/L | 73 (58–92) | 76 (66–96) | 0.05 # | |
| 24.25(OH)D, nmol/L | 6.5 (4.4–9.0) | 7.1 (5.4–9.6) | 0.08 # | 0.4–8.9 |
| Free 25(OH)D (* 10−2), nmol/L | 1.2 (1.0–1.5) | 1.4 (1.2–1.7) | <0.01 * | |
| Albumin bound 25(OH)D, nmol/L | 4.5 (3.5–5.6) | 5.1 (4.1–6.1) | <0.01 * | |
| Bioavailable 25(OH)D, nmol/L | 4.5 (3.5–5.6) | 5.1 (4.1–6.1) | <0.01 * | |
| Free 1.25(OH)2D (* 10−1), pmol/L | 2.0 (2.2–2.8) | 2.5 (0.2–3.1) | <0.01 *# | |
| Albumin bound 1.25(OH)2D, pmol/L | 7.3 (5.7–9.1) | 8.4 (6.7–9.9) | <0.01 * | |
| Bioavailable 1.25(OH)2D, pmol/L | 7.5 (5.9–9.4) | 8.6 (7.0–10.2) | <0.01 * | |
| Ratio total 25(OH)D/24.25(OH)2D | 11.2 (9.9–13.6) | 11.4 (9.5–12.9) | 0.21 | 10–33 |
| VDBP, µg/L | 408 (374–445) | 388 (361–427) | 0.02 *# | 200–550 |
| Albumin, g/L | 42 (39–44) | 42 (40–43) | 0.86 | 35–52 |
| Calcium, mmol/L | 2.4 (2.3–2.4) | 2.4 (2.3–2.4) | 0.73 | 2.2–2.6 |
| Corrected calcium, mmol/L | 2.3 (2.3–2.4) | 2.3 (2.3–2.4) | 0.81 | |
| FGF23, RU/mL | 88 (72–113) | 89 (69–106) | 0.65 | <125 |
| PTH, pmol/L | 5.2 (4.0–6.6) | 5.3 (3.8–6.7) | 0.94 | <10 |
| Phosphate, mmol/L | 1.0 (0.9–1.1) | 0.8 (0.8–0.9) | <0.01 * | 0.7–1.4 |
| CTX, ng/L | 256 (183–379) | 307 (212–418) | 0.10 | <580 |
| P1NP, µg/L | 37 (27–54) | 39 (29–56) | 0.37 | 22–87 |
| ALP, U/L | 74 (53–89) | 67 (56–79) | 0.14 | <115 |
| Osteocalcin, nmol/L | 1.5 (1.1–2.1) | 1.5 (1.1–2.0) | 0.99 | 0.4–4.0 |
| Men (n = 84) | Women (n = 99) | |||||
|---|---|---|---|---|---|---|
| Patients (n = 30) | Controls (n = 54) | p values a | Patients (n = 61) | Controls (n = 38) | p values a | |
| Total 25(OH)D, nmol/L | 74 (56–97) | 75 (66–90) | 0.62 | 77 (60–90) | 88 (68–106) | 0.02 * |
| 25(OH)D3, nmol/L | 73 (55–96) | 74 (64–89) | 0.64 | 75 (58–89) | 86 (67–104) | 0.01 * |
| 24.25(OH)2D, nmol/L | 6.5 (4.5–8.8) | 6.9 (5.4–8.7) | 0.48 | 6.5 (4.4–9.1) | 7.1 (5.6–11.0) | 0.04 * |
| Free 25(OH)D (* 10−2), nmol/L | 0.013 (0.010–0.017) | 0.014 (0.012–0.017) | 0.17 | 0.012 (0.010–0.015) | 0.013 (0.011–0.017) | 0.03 * |
| Free 1.25(OH)2D (* 10−1), pmol/L | 0.23 (0.17–0.30) | 0.25 (0.22–0.31) | 0.18 | 0.21 (0.17–0.27) | 0.24 (0.21–0.31) | 0.03 * |
| Phosphate, mmol/L | 1.0 (0.9–1.0) | 0.8 (0.8–0.9) | <0.01 * | 1.0 (0.9–1.1) | 0.8 (0.8–0.9) | <0.01 * |
| N = 90 | ALP | FGF23 | Osteocalcin | CTX | P1NP | EDSS |
|---|---|---|---|---|---|---|
| Free 1.25(OH)2D | r −0.03 | r 0.10 | r 0.01 | r −0.10 | r −0.07 | r −0.28 |
| p 0.78 | p 0.33 | p 0.95 | p 0.33 | p 0.54 | p 0.01 | |
| Bioavailable 1.25(OH)2D | r −0.04 | r 0.10 | r 0.04 | r −0.06 | r −0.03 | r −0.30 |
| p 0.71 | p 0.33 | p 0.72 | p 0.59 | p 0.77 | p < 0.01 | |
| Total 1.25(OH)2D | r −0.12 | r −0.05 | r −0.24 | r −0.09 | r −0.19 | r −0.08 |
| p 0.25 | p 0.65 | p 0.02 | p 0.41 | p 0.08 | p 0.47 | |
| Free 25(OH)D | r −0.02 | r 0.10 | r 0.01 | r −0.10 | r −0.06 | r −0.28 |
| p 0.82 | p 0.34 | p 0.93 | p 0.36 | p 0.57 | p 0.01 | |
| Bioavailable 25(OH)D | r −0.03 | r 0.11 | r 0.05 | r −0.05 | r −0.02 | r −0.30 |
| p 0.77 | p 0.33 | p 0.66 | p 0.67 | p 0.84 | p < 0.01 | |
| Total 25(OH)D | r −0.16 | r 0.22 | r −0.12 | r −0.23 | r −0.19 | r −0.23 |
| p 0.14 | p 0.04 | p 0.28 | p 0.03 | p 0.08 | p 0.03 | |
| 24.25(OH)D | r −0.20 | r 0.22 | r −0.16 | r −0.31 | r −0.25 | r −0.22 |
| p 0.06 | p 0.04 | p 0.14 | p < 0.01 | p 0.02 | p 0.04 | |
| Ratio 25(OH)D/24.25(OH)2D | r 0.18 | r −0.13 | r 0.16 | r 0.31 | r 0.27 | r 0.10 |
| p 0.09 | p 0.23 | p 0.13 | p <0.01 | p 0.01 | p 0.34 | |
| PTH | r 0.09 | r −0.04 | r −0.04 | r 0.04 | r −0.08 | r 0.16 |
| p 0.40 | p 0.69 | p 0.97 | p 0.69 | p 0.46 | p 0.13 | |
| Phosphate | r 0.10 | r 0.03 | r 0.22 | r 0.13 | r 0.16 | r −0.03 |
| p 0.35 | p 0.78 | p 0.04 | p 0.24 | p 0.15 | p 0.76 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlot, M.C.; Boekel, L.; Kragt, J.; Killestein, J.; van Amerongen, B.M.; de Jonge, R.; den Heijer, M.; Heijboer, A.C. Multiple Sclerosis Patients Show Lower Bioavailable 25(OH)D and 1,25(OH)2D, but No Difference in Ratio of 25(OH)D/24,25(OH)2D and FGF23 Concentrations. Nutrients 2019, 11, 2774. https://doi.org/10.3390/nu11112774
Vlot MC, Boekel L, Kragt J, Killestein J, van Amerongen BM, de Jonge R, den Heijer M, Heijboer AC. Multiple Sclerosis Patients Show Lower Bioavailable 25(OH)D and 1,25(OH)2D, but No Difference in Ratio of 25(OH)D/24,25(OH)2D and FGF23 Concentrations. Nutrients. 2019; 11(11):2774. https://doi.org/10.3390/nu11112774
Chicago/Turabian StyleVlot, Mariska C, Laura Boekel, Jolijn Kragt, Joep Killestein, Barbara M. van Amerongen, Robert de Jonge, Martin den Heijer, and Annemieke C. Heijboer. 2019. "Multiple Sclerosis Patients Show Lower Bioavailable 25(OH)D and 1,25(OH)2D, but No Difference in Ratio of 25(OH)D/24,25(OH)2D and FGF23 Concentrations" Nutrients 11, no. 11: 2774. https://doi.org/10.3390/nu11112774
APA StyleVlot, M. C., Boekel, L., Kragt, J., Killestein, J., van Amerongen, B. M., de Jonge, R., den Heijer, M., & Heijboer, A. C. (2019). Multiple Sclerosis Patients Show Lower Bioavailable 25(OH)D and 1,25(OH)2D, but No Difference in Ratio of 25(OH)D/24,25(OH)2D and FGF23 Concentrations. Nutrients, 11(11), 2774. https://doi.org/10.3390/nu11112774