Macronutrient Intake in Relation to Migraine and Non-Migraine Headaches

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
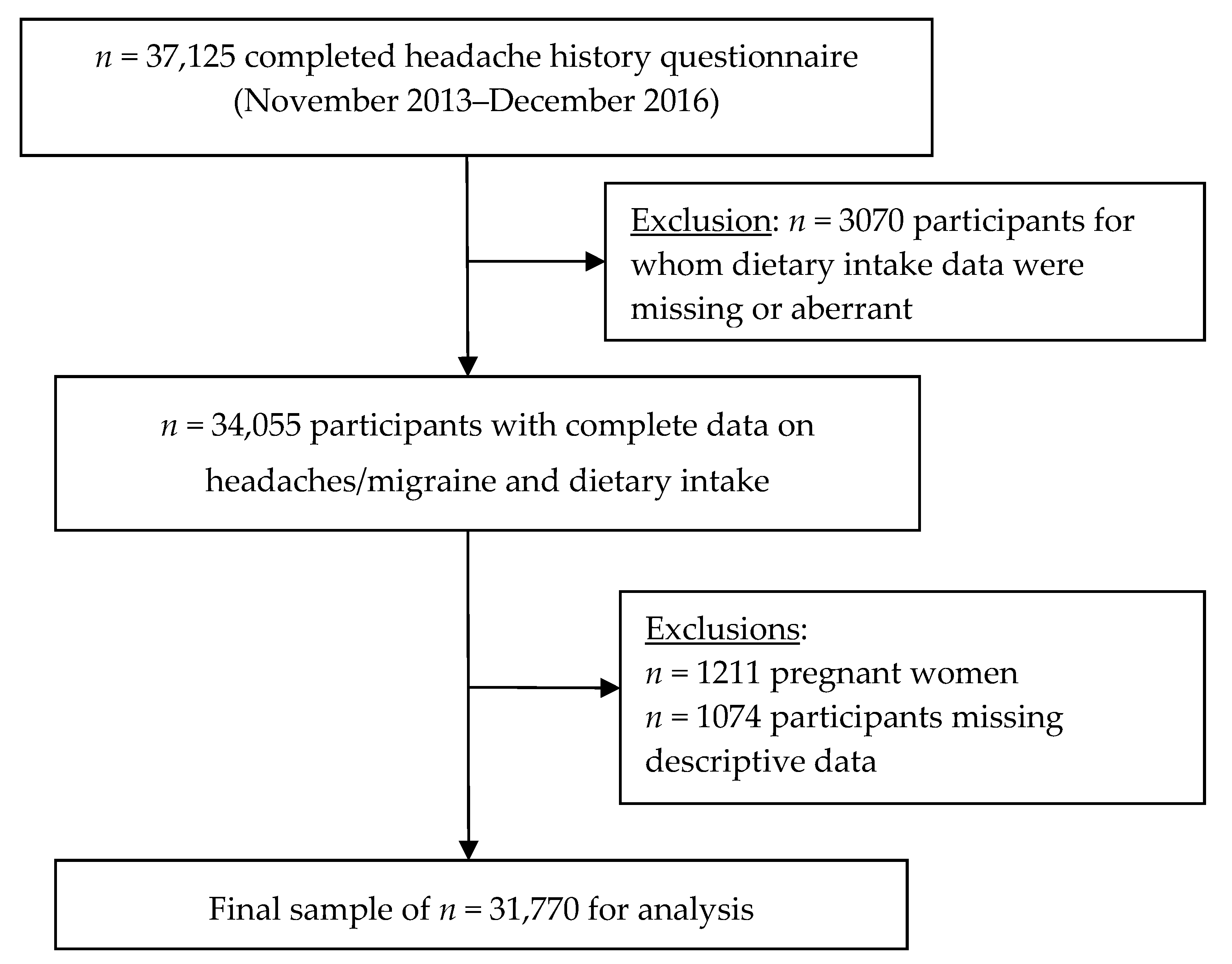
2.1. NutriNet-Santé E-Cohort
2.2. Migraine Assessment
2.3. Dietary Intake Assessment
2.4. Descriptive Characteristics
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Profiles by Headache Status
3.2. Association between Macronutrient Intake and Headache Status
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Headache Disorders Fact Sheet No. 277; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Headache Classification Committee of the International Headache Society (IHS). Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 33, 1–211. [Google Scholar] [CrossRef]
- Woldeamanuel, Y.W.; Cowan, R.P. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J. Neurol. Sci. 2017, 372, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Vetvik, K.G.; MacGregor, E.A. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017, 16, 76–87. [Google Scholar] [CrossRef]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Finkel, A.G.; Yerry, J.A.; Mann, J.D. Dietary considerations in migraine management: Does a consistent diet improve migraine? Curr. Pain Headache Rep. 2013, 17, 373. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, L.A.; Pacioni, D.; Di Fronzo, V.; Russo, B.F.; Speranza, E.; Carlino, V.; Gargiulo, F.; Ferrara, F. Low-lipid diet reduces frequency and severity of acute migraine attacks. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Vij, B. Diet and headache: Part 2. Headache 2016, 56, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Rockett, F.C.; de Oliveira, V.R.; Castro, K.; Chaves, M.L.; Perla, A.D.S.; Perry, I.D. Dietary aspects of migraine trigger factors. Nutr. Rev. 2012, 70, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Kelman, L. The triggers or precipitants of the acute migraine attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Holzhammer, J.; Wober, C. Alimentary trigger factors that provoke migraine and tension-type headache. Schmerz 2006, 20, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Finocchi, C.; Sivori, G. Food as trigger and aggravating factor of migraine. Neurol. Sci. 2012, 33, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.W.; Lipton, R.B.; Peterlin, B.L.; Raynor, H.A.; Thomas, J.G.; O’Leary, K.C.; Pavlovic, J.; Wing, R.R.; Bond, D.S. Dietary intake patterns and diet quality in a nationally representative sample of women with and without severe headache or migraine. Headache 2015, 55, 550–561. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Castetbon, K.; Czernichow, S.; Malon, A.; Mejean, C.; Kesse, E.; Touvier, M.; Galan, P. The NutriNet-Santé study: a web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health 2010, 10, 242. [Google Scholar] [CrossRef] [PubMed]
- Guichard, E.; Montagni, I.; Tzourio, C.; Kurth, T. Association between headaches and tinnitus in young adults: Cross-sectional study. Headache 2016, 56, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M. Migraine chronification-concept and risk factors. Discov. Med. 2009, 8, 145–150. [Google Scholar] [PubMed]
- Le Moullec, N.; Deheeger, M.; Preziosi, P.; Monteiro, P.; Valeix, P.; Rolland, M.; Potier De Courcy, G.; Christides, J.P.; Cherouvrier, F.; Galan, P. Validation du manuel photos utilisé pour l’enquête alimentaire de l’étude SU.VI.MAX. Cah. Nutr. Diét. 1996, 31, 158–164. (In French) [Google Scholar]
- Etude NutriNet-Santé. Table de Composition des Aliments; Économica: Paris, France, 2013; (In French). ISBN 978-2-7178-6537-0. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar] [PubMed]
- Touvier, M.; Kesse-Guyot, E.; Méjean, C.; Pollet, C.; Malon, A.; Castetbon, K.; Hercberg, S. Comparison between an interactive web-based self-administered 24 h dietary record and an interview by a dietitian for large-scale epidemiological studies. Br. J. Nutr. 2011, 105, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Lassale, C.; Castetbon, K.; Laporte, F.; Deschamps, V.; Vernay, M.; Camilleri, G.M.; Faure, P.; Hercberg, S.; Galan, P.; Kesse-Guyot, E. Correlations between fruit, vegetables, fish, vitamins, and fatty acids estimated by web-based nonconsecutive dietary records and respective biomarkers of nutritional status. J. Acad. Nutr. Diet. 2016, 116, 427–438. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Group. IPAQ Scoring Protocol. Available online: www.ipaq.ki.se (accessed on 18 August 2018).
- Agence Nationale de Sécurité Sanitaire de l’Alimentation (ANSES). Étude Individuelle Nationale des Consommations Alimentaires 3 (INCA 3). Rapport D’expertise Collective; ANSES: Maisons-Alfort, France, 2017. (In French) [Google Scholar]
- Bic, Z.; Blix, G.G.; Hopp, H.P.; Leslie, F.M.; Schell, M.J. The influence of a low-fat diet on incidence and severity of migraine headaches. J. Womens Health Gend. Based Med. 1999, 8, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Bunner, A.E.; Agarwal, U.; Gonzales, J.F.; Valente, F.; Barnard, N.D. Nutrition intervention for migraine: A randomized crossover trial. J. Headache Pain 2014, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Bic, Z.; Blix, G.G.; Hopp, H.P.; Leslie, F.M. In search of the ideal treatment for migraine headache. Med Hypotheses 1998, 50, 1–7. [Google Scholar] [CrossRef]
- Janoska, M.; Chorazka, K.; Domitrz, I. Migraine frequency and its association with dyslipidemia in women. Neurol. Neurochir. Pol. 2015, 49, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Monastero, R.; Pipia, C.; Cefalù, A.B.; Liveri, E.T.; Rosano, R.; Camarda, R.; Camarda, C. Association between plasma lipid levels and migraine in subjects aged > or =50 years: Preliminary data from the Zabut Aging Project. Neurol. Sci. 2008, 29, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Goulart, A.C.; Lotufo, P.A.; Santos, I.S.; Bittencourt, M.S.; Santos, R.D.; Blaha, M.J.; Jones, S.; Toth, P.P.; Kulkarni, K.; Benseñor, I.M. The relationship between migraine and lipid sub-fractions among individuals without cardiovascular disease: A cross-sectional evaluation in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Cephalalgia 2018, 38, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Cavestro, C.; Rosatello, A.; Micca, G.; Ravotto, M.; Pia Marino, M.; Asteggiano, G.; Beghi, E. Insulin metabolism is altered in migraineurs: A new pathogenic mechanism for migraine? Headache 2007, 47, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Hufnagl, K.N.; Peroutka, S.J. Glucose regulation in headache: Implications for dietary management. Expert Rev. Neurother. 2002, 2, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Altobelli, E.; Ornello, R.; Ripa, P.; Pistoia, F.; Carolei, A. Insulin resistance in migraineurs: Results from a case-control study. Cephalalgia 2014, 34, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Le, H.; Tfelt-Hansen, P.; Skytthe, A.; Kyvik, K.O.; Olesen, J. Increase in self-reported migraine prevalence in the Danish adult population: A prospective longitudinal population-based study. BMJ Open 2012, 2, E000962. [Google Scholar] [CrossRef] [PubMed]
- Streel, S.; Donneau, A.F.; Hoge, A.; Albert, A.; Schoenen, J.; Guillaume, M. One-year prevalence of migraine using a validated extended French version of the ID Migraine: A Belgian population-based study. Rev. Neurol. 2015, 171, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Schoonman, G.G.; Evers, D.J.; Terwindt, G.M.; van Dijk, J.G.; Ferrari, M.D. The prevalence of premonitory symptoms in migraine: A questionnaire study in 461 patients. Cephalalgia 2006, 26, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- Quintela, E.; Castillo, J.; Munoz, P.; Pascual, J. Premonitory and resolution symptoms in migraine: A prospective study in 100 unselected patients. Cephalalgia 2006, 26, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Blau, J.N. What some patients can eat during migraine attacks: Therapeutic and conceptual implications. Cephalalgia 1993, 13, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Fofi, L.; Aurilia, C.; Egeo, G.; Caprio, M. Ketogenic diet in migraine: Rationale, findings and perspectives. Neurol. Sci. 2017, 38, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Coppola, G.; Sirianni, G.; Di Lorenzo, G.; Bracaglia, M.; Di Lenola, D.; Siracusano, A.; Rossi, P.; Pierelli, F. Migraine improvement during short lasting ketogenesis: A proof-of-concept study. Eur. J. Neurol. 2015, 22, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, V.A.; Salanave, B.; Castetbon, K.; Deschamps, V.; Vernay, M.; Kesse-Guyot, E.; Hercberg, S. Comparison of the sociodemographic characteristics of the large NutriNet-Santé e-cohort with French Census data: The issue of volunteer bias revisited. J. Epidemiol. Community Health 2015, 69, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Andreeva, V.A.; Fezeu, L.K.; Hercberg, S.; Galan, P. Obesity and migraine: Effect modification by gender and perceived stress. Neuroepidemiology 2018, 51, 25–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men (n= 8042) | Women (n = 23,728) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Headache (n = 4085) | Non-Migraine Headache (n = 3220) | Migraine (n = 737) | pa | No Headache (n = 6850) | Non-Migraine Headache (n = 10,781) | Migraine (n = 6097) | pa | |||||||
| Age, year | <0.0001 | <0.0001 | ||||||||||||
| 18–39 year | 478 | (11.7) | 496 | (15.4) | 118 | (16.0) | 1313 | (19.2) | 2853 | (26.5) | 1470 | (24.1) | ||
| ≥40 year | 3607 | (88.3) | 2724 | (84.6) | 619 | (84.0) | 5537 | (80.8) | 7928 | (73.5) | 4627 | (75.9) | ||
| Mean (SD) | 59.3 | (13.5) | 55.3 | (13.4) | 54.3 | (13.3) | <0.0001 | 53.9 | (13.8) | 49.6 | (13.3) | 49.6 | (12.8) | <0.0001 |
| Body Mass Index, kg/m2 | 0.07 | <0.0001 | ||||||||||||
| Normal weight (<25.0) | 2218 | (54.3) | 1696 | (52.7) | 416 | (56.4) | 4968 | (72.5) | 7626 | (70.7) | 4100 | (67.2) | ||
| Overweight (25.0–29.9) | 1505 | (36.8) | 1186 | (36.8) | 249 | (33.8) | 1348 | (19.7) | 2162 | (20.1) | 1312 | (21.5) | ||
| Obese (≥30.0) | 362 | (8.9) | 338 | (10.5) | 72 | (9.8) | 534 | (7.8) | 993 | (9.2) | 685 | (11.2) | ||
| Mean (SD) | 25.2 | (3.6) | 25.3 | (3.8) | 25.2 | (4.2) | 0.33 | 23.5 | (4.3) | 23.8 | (4.6) | 24.0 | (4.9) | <0.0001 |
| Marital status | 0.09 | 0.09 | ||||||||||||
| Married/cohabiting | 3409 | (83.5) | 2626 | (81.6) | 602 | (81.7) | 4944 | (72.2) | 7915 | (73.4) | 4498 | (73.8) | ||
| Living alone (single/divorced/ widowed) | 676 | (16.5) | 594 | (18.4) | 135 | (18.3) | 1906 | (27.8) | 2866 | (26.6) | 1599 | (26.2) | ||
| Educational level | <0.0001 | <0.0001 | ||||||||||||
| Less than high school | 1070 | (26.2) | 690 | (21.4) | 160 | (21.7) | 1328 | (19.4) | 1715 | (15.9) | 966 | (15.8) | ||
| High school diploma or equivalent | 496 | (12.1) | 370 | (11.5) | 79 | (10.7) | 1015 | (14.8) | 1421 | (13.2) | 914 | (15.0) | ||
| Post-secondary education | 2519 | (61.7) | 2160 | (67.1) | 498 | (67.6) | 4507 | (65.8) | 7645 | (70.9) | 4217 | (69.2) | ||
| Employment status | <0.0001 | <0.0001 | ||||||||||||
| Employed, self-employed | 1541 | (37.7) | 1637 | (50.8) | 384 | (52.1) | 3459 | (50.5) | 6651 | (61.7) | 3713 | (60.9) | ||
| Homemaker/disabled/unemployed | 178 | (4.4) | 189 | (5.9) | 58 | (7.9) | 744 | (10.9) | 1400 | (13.0) | 949 | (15.6) | ||
| Retired | 2366 | (57.9) | 1394 | (43.3) | 295 | (40.0) | 2647 | (38.6) | 2730 | (25.3) | 1435 | (23.5) | ||
| Physical activity b | <0.0001 | <0.0001 | ||||||||||||
| Low | 2000 | (49.0) | 1340 | (41.6) | 307 | (41.7) | 2554 | (37.3) | 3391 | (31.5) | 2031 | (33.3) | ||
| Moderate | 1332 | (32.6) | 1208 | (37.5) | 270 | (36.6) | 2846 | (41.5) | 4673 | (43.3) | 2563 | (42.0) | ||
| Vigorous | 753 | (18.4) | 672 | (20.9) | 160 | (21.7) | 1450 | (21.2) | 2717 | (25.2) | 1503 | (24.7) | ||
| Smoking status | 0.38 | <0.0001 | ||||||||||||
| Never | 1671 | (40.9) | 1344 | (41.7) | 305 | (41.4) | 3836 | (56.0) | 5583 | (51.8) | 3096 | (50.8) | ||
| Former | 2051 | (50.2) | 1554 | (48.3) | 360 | (48.8) | 2309 | (33.7) | 3941 | (36.6) | 2278 | (37.4) | ||
| Current | 363 | (8.9) | 322 | (10.0) | 72 | (9.8) | 705 | (10.3) | 1257 | (11.7) | 723 | (11.9) | ||
| Family history of headache c | 1626 | (50.5) | 279 | (37.9) | <0.0001 | 5168 | (47.9) | 2179 | (35.7) | <0.0001 | ||||
| Men (n = 8042) | Women (n = 23,728) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Headache (n = 4085) | Non-Migraine Headache (n = 3220) | Migraine (n = 737) | p | No Headache (n = 6850) | Non-Migraine Headache (n = 10,781) | Migraine (n = 6097) | p | |||||||
| Number of 24-h records, mean (SD) | 16.7 | (6.9) | 16.3 | (6.9) | 15.8 | (7.2) | 0.002 | 16.1 | (6.8) | 15.8 | (6.8) | 15.1 | (6.8) | <0.0001 |
| Total daily energy, kcal, mean (SD) | 2254 | (436.3) | 2280 | (429.3) | 2245 | (433.9) | 0.02 | 1770 | (332.6) | 1789 | (335.5) | 1755 | (339.5) | <0.0001 |
| % total carbohydrates | 41.1 | (6.4) | 41.1 | (6.2) | 41.1 | (5.8) | 0.99 | 41.3 | (5.9) | 41.3 | (5.7) | 41.5 | (5.7) | 0.20 |
| % simple carbohydrates | 18.2 | (4.9) | 18.3 | (4.7) | 18.3 | (4.7) | 0.60 | 20.0 | (4.5) | 19.9 | (4.5) | 19.9 | (4.6) | 0.56 |
| % protein | 16.7 | (2.5) | 16.5 | (2.6) | 16.5 | (2.5) | 0.001 | 17.0 | (3.0) | 16.9 | (3.0) | 17.1 | (3.2) | <0.0001 |
| % fat | 37.0 | (5.1) | 37.6 | (5.0) | 37.9 | (4.8) | <0.0001 | 38.7 | (4.9) | 39.0 | (4.9) | 39.0 | (4.9) | <0.0001 |
| Dietary intake, g/day, mean (SD) | ||||||||||||||
| Total carbohydrates | 232.3 | (0.6) | 232.3 | (0.6) | 232.5 | (1.3) | 0.75 | 183.4 | (0.3) | 183.4 | (0.2) | 184.1 | (0.3) | 0.046 |
| Simple carbohydrates | 103.0 | (0.4) | 103.6 | (0.5) | 103.7 | (1.0) | 0.44 | 88.6 | (0.2) | 88.3 | (0.2) | 88.4 | (0.3) | 0.53 |
| Complex carbohydrates | 129.3 | (0.4) | 128.7 | (0.5) | 128.9 | (1.0) | 0.96 | 94.8 | (0.2) | 95.1 | (0.2) | 95.7 | (0.3) | 0.13 |
| Protein | 93.5 | (0.2) | 92.6 | (0.2) | 91.9 | (0.5) | 0.018 | 74.6 | (0.1) | 74.2 | (0.1) | 74.4 | (0.2) | 0.97 |
| Total fat | 93.5 | (0.2) | 94.9 | (0.2) | 95.5 | (0.5) | 0.008 | 76.6 | (0.1) | 77.2 | (0.1) | 77.4 | (0.1) | <0.0001 |
| Saturated fatty acids (SFA) | 38.3 | (0.1) | 39.0 | (0.1) | 39.7 | (0.3) | 0.006 | 31.2 | (0.1) | 31.8 | (0.1) | 31.8 | (0.1) | <0.0001 |
| Monounsaturated fatty acids (MUFA) | 34.8 | (0.1) | 35.5 | (0.1) | 35.7 | (0.2) | 0.028 | 28.8 | (0.1) | 29.0 | (0.1) | 29.1 | (0.1) | 0.001 |
| Polyunsaturated fatty acids (PUFA) | 13.4 | (0.1) | 13.4 | (0.1) | 13.2 | (0.1) | 0.51 | 10.9 | (0.0) | 10.7 | (0.0) | 10.8 | (0.0) | 0.077 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreeva, V.A.; Szabo de Edelenyi, F.; Druesne-Pecollo, N.; Touvier, M.; Hercberg, S.; Galan, P. Macronutrient Intake in Relation to Migraine and Non-Migraine Headaches. Nutrients 2018, 10, 1309. https://doi.org/10.3390/nu10091309
Andreeva VA, Szabo de Edelenyi F, Druesne-Pecollo N, Touvier M, Hercberg S, Galan P. Macronutrient Intake in Relation to Migraine and Non-Migraine Headaches. Nutrients. 2018; 10(9):1309. https://doi.org/10.3390/nu10091309
Chicago/Turabian StyleAndreeva, Valentina A., Fabien Szabo de Edelenyi, Nathalie Druesne-Pecollo, Mathilde Touvier, Serge Hercberg, and Pilar Galan. 2018. "Macronutrient Intake in Relation to Migraine and Non-Migraine Headaches" Nutrients 10, no. 9: 1309. https://doi.org/10.3390/nu10091309
APA StyleAndreeva, V. A., Szabo de Edelenyi, F., Druesne-Pecollo, N., Touvier, M., Hercberg, S., & Galan, P. (2018). Macronutrient Intake in Relation to Migraine and Non-Migraine Headaches. Nutrients, 10(9), 1309. https://doi.org/10.3390/nu10091309