Uric Acid and Cognitive Function in Older Individuals

 and
and
Abstract
1. Introduction
2. Uric Acid and Dementia: Results from Large Epidemiological Studies
2.1. Uric Acid and Alzheimer’s Disease
2.2. Uric Acid and Parkinson’s Dementia
2.3. Uric Acid and Vascular or Mixed Dementia
2.4. Uric Acid and Mild Cognitive Impairment
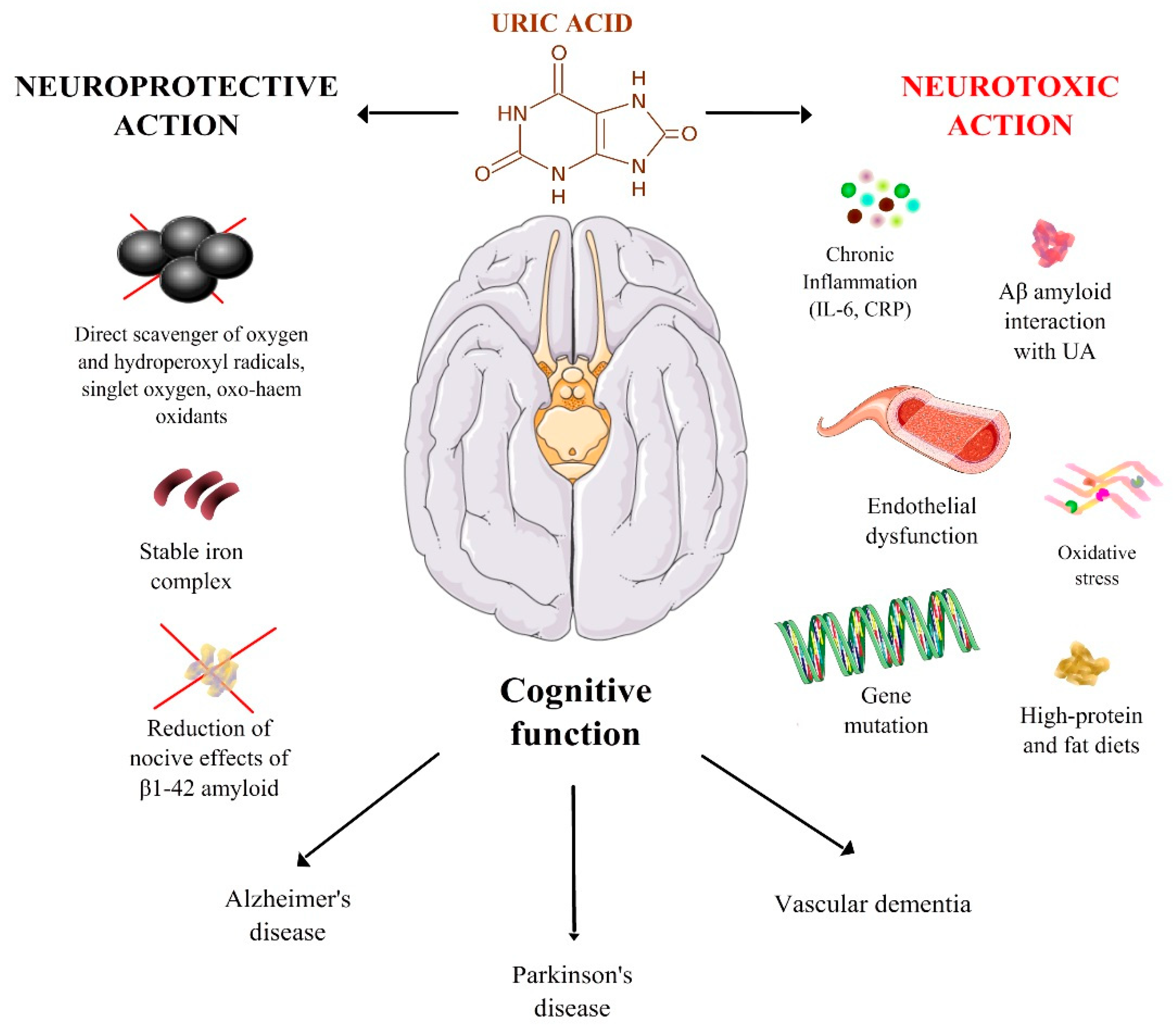
3. Mechanisms Underlying the Relation between UA and Cognitive Function
3.1. Oxidative Stress
3.2. UA and Interaction with β-Amyloid
3.3. Inflammation, Endothelial Dysfunction, and Vascular Damage
3.4. Diet, Uric Acid, and Dementia
3.5. Genetic Syndromes and Cognitive Decline
4. Study Limitations at the Basis of Conflicting Evidence
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Tana, C.; Busetto, M.; Di Vincenzo, A.; Ricci, F.; Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Giamberardino, M.A.; Cipollone, F.; Vettor, R.; et al. Management of hyperuricemia and gout in obese patients undergoing bariatric surgery. Postgrad. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Wu, C.H.; Liu, L.K.; Chou, R.H.; Kuo, C.S.; Huang, P.H.; Chen, L.K.; Lin, S.J. Association between serum uric acid and cardiovascular risk in nonhypertensive and nondiabetic individuals: The Taiwan I-Lan Longitudinal Aging Study. Sci. Rep. 2018, 8, 5234. [Google Scholar] [CrossRef] [PubMed]
- Borghi, C.; Verardi, F.M.; Pareo, I.; Bentivenga, C.; Cicero, A.F. Hyperuricemia and cardiovascular disease risk. Expert Rev. Cardiovasc. Ther. 2014, 12, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Euser, S.M.; Hofman, A.; Westendorp, R.G.; Breteler, M.M. Serum uric acid and cognitive function and dementia. Brain 2009, 132 Pt 2, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Verhaaren, B.F.; Vernooij, M.W.; Dehghan, A.; Vrooman, H.A.; de Boer, R.; Hofman, A.; Witteman, J.C.; Niessen, W.J.; Breteler, M.M.; van der Lugt, A.; et al. The relation of uric acid to brain atrophy and cognition: The Rotterdam Scan Study. Neuroepidemiology 2013, 41, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.Y.; Lan, T.Y.; Tang, G.J.; Tang, C.H.; Chen, T.J.; Lin, H.Y. Gout and the risk of dementia: A nationwide population-based cohort study. J. Arthritis Res. Ther. 2015, 17, 139. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Dubreuil, M.; Zhang, Y.; Neogi, T.; Rai, S.K.; Ascherio, A.; Hernán, M.A.; Choi, H.K. Gout and the risk of Alzheimer’s disease: A population-based, BMI-matched cohort study. Ann. Rheum. Dis. 2016, 75, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Guo, X.; Huang, R.; Chen, Y.; Zheng, Z.; Shang, H. Serum uric acid levels in patients with Alzheimer’s disease: A meta-analysis. PLoS ONE 2014, 9, e94084. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Quinn, T.J.; Hewitt, J.; Fan, Y.; Dawson, J. Serum uric acid level and association with cognitive impairment and dementia: Systematic review and meta-analysis. Age 2016, 38, 16. [Google Scholar] [CrossRef] [PubMed]
- Du, N.; Xu, D.; Hou, X.; Song, X.; Liu, C.; Chen, Y.; Wang, Y.; Li, X. Inverse Association Between Serum Uric Acid Levels and Alzheimer’s Disease Risk. Mol. Neurobiol. 2016, 53, 2594–2599. [Google Scholar] [CrossRef] [PubMed]
- Ahlskog, J.E.; Uitti, R.J.; Low, P.A.; Tyce, G.M.; Nickander, K.K.; Petersen, R.C.; Kokmen, E. No evidence for systemic oxidant stress in Parkinson’s or Alzheimer’s disease. Mov. Disord. 1995, 10, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Annanmaki, T.; Pohja, M.; Parviainen, T.; Hakkinen, P.; Murros, K. Uric acid and cognition in Parkinson’s disease: A follow-up study. Parkinsonism Relat. Disord. 2011, 17, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Guo, Y.; Luo, W.; Lin, C.; Ding, M. Serum urate and the risk of Parkinson’s disease: Results from a meta-analysis. Can. J. Neurol. Sci. 2013, 40, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; O’Reilly, É.J.; Schwarzschild, M.A.; Ascherio, A. Prospective study of plasma urate and risk of Parkinson disease in men and women. Neurology 2016, 86, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.; Zhou, B.; Chen, Y.H.; Ma, Z.L.; Gou, Y.; Zhang, C.L.; Yu, W.F.; Jiao, L. Serum uric acid levels in patients with Parkinson’s disease: A meta-analysis. PLoS ONE 2017, 12, e0173731. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Ng, S.Y.; Chia, N.S.; Acharyya, S.; Setiawan, F.; Lu, Z.H.; Ng, E.; Tay, K.Y.; Au, W.L.; Tan, E.K.; et al. Serum uric acid level and its association with motor subtypes and non-motor symptoms in early Parkinson’s disease: PALS study. Parkinsonism Relat. Disord. 2018. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Zhang, S.; Wang, D.; Fan, M.; Gao, F.; Sun, W.; Li, Z.; Li, S. The significance of uric acid in the diagnosis and treatment of Parkinson disease: An updated systemic review. Medicine 2017, 96, e8502. [Google Scholar] [CrossRef] [PubMed]
- Latourte, A.; Soumaré, A.; Bardin, T.; Perez-Ruiz, F.; Debette, S.; Richette, P. Uric acid and incident dementia over 12 years of follow-up: A population-based cohort study. Ann. Rheum. Dis. 2018, 77, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, M.C.; Raman, R.; Schwarzschild, M.A.; Becerra, L.M.; Thomas, R.G.; Peterson, R.C.; Ascherio, A.; Aisen, P.S. Plasma urate and progression of mild cognitive impairment. Neurodegener. Dis. 2009, 6, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Viazzi, F.; Leoncini, G.; Ratto, E.; Pontremoli, R. Serum uric acid as a risk factor for cardiovascular and renal disease: an old controversy revived. J. Clin. Hypertens. (Greenwich). 2006, 8, 510–518. [Google Scholar] [CrossRef]
- Schrag, M.; Mueller, C.; Zabel, M.; Crofton, A.; Kirsch, W.M.; Ghribi, O.; Squitti, R.; Perry, G. Oxidative stress in blood in Alzheimer’s disease and mild cognitive impairment: A meta-analysis. Neurobiol. Dis. 2013, 59, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhao, M.; Han, Z.; Li, D.; Zhang, S.; Zhang, Y.; Kong, X.; Sun, N.; Zhang, Q.; Lei, P. Hyperuricemia as a Protective Factor for Mild Cognitive Impairment in Non-Obese Elderly. Tohoku J. Exp. Med. 2017, 242, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Liu, Y.; Xue, H.; Xue, J.; Sun, K.; Wu, L.; Hou, P. Low uric acid is a risk factor in mild cognitive impairment. Neuropsychiatr. Dis. Treat. 2017, 13, 2363–2367. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Wang, J.; Zeng, J.; He, Y. Relationship between serum uric acid level and mild cognitive impairment in Chinese community elderly. BMC Neurol. 2017, 17, 146. [Google Scholar] [CrossRef] [PubMed]
- Cervellati, C.; Cremonini, E.; Bosi, C.; Magon, S.; Zurlo, A.; Bergamini, C.M.; Zuliani, G. Systemic oxidative stress in older patients with mild cognitive impairment or late onset Alzheimer’s disease. Curr. Alzheimer Res. 2013, 10, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, P.; Polidori, M.C.; Metastasio, A.; Mariani, E.; Mattioli, P.; Cherubini, A.; Catani, M.; Cecchetti, R.; Senin, U.; Mecocci, P. Plasma antioxidants are similarly depleted in mild cognitive impairment and in Alzheimer’s disease. Neurobiol. Aging 2003, 24, 915–919. [Google Scholar] [CrossRef]
- Kim, T.S.; Pae, C.U.; Yoon, S.J.; Jang, W.Y.; Lee, N.J.; Kim, J.J.; Lee, S.J.; Lee, C.; Paik, I.H.; Lee, C.U. Decreased plasma antioxidants in patients with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2006, 21, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Gackowski, D.; Rozalski, R.; Siomek, A.; Dziaman, T.; Nicpon, K.; Klimarczyk, M.; Araszkiewicz, A.; Olinski, R. Oxidative stress and oxidative DNA damage ischaracteristic for mixed Alzheimer disease/vascular dementia. J. Neurol. Sci. 2008, 266, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Pulido, R.; Jiménez-Escrig, A.; Orensanz, L.; Saura-Calixto, F.; Jiménez-Escrig, A. Study of plasma antioxidant status in Alzheimer’s disease. Eur. J. Neurol. 2005, 12, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Mullan, K.; Cardwell, C.R.; McGuinness, B.; Woodside, J.V.; McKay, G.J. Plasma Antioxidant Status in Patients with Alzheimer’s Disease and Cognitively Intact Elderly: A Meta-Analysis of Case-Control Studies. J. Alzheimers Dis. 2018, 62, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.K. Oxidative stress in neurodegeneration: Cause or consequence? Nat. Med. 2004, 10, S18. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Maes, M. Neurodegeneration in Parkinson’s disease: Interactions of oxidative stress, tryptophan catabolites and depression with mitochondria and sirtuins. Mol. Neurobiol. 2014, 49, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Gaki, G.S.; Papavassiliou, A.G. Oxidative stress-induced signaling pathways implicated in the pathogenesis of Parkinson’s disease. Neuromol. Med. 2014, 16, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.X.; Anjos, E.I.; Augusto, O. Uric acid oxidation by peroxynitrite: Multiple reactions, free radical formation, and amplification of lipid oxidation. Arch. Biochem. Biophys. 1999, 372, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.J.; Sevanian, A.; Muakkassah-Kelly, S.F.; Hochstein, P. Uric acid-iron ion complexes. A new aspect of the antioxidant functions of uric acid. Biochem. J. 1986, 235, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Waring, W.S.; Adwani, S.H.; Breukels, O.; Webb, D.J.; Maxwell, S.R.J. Hyperuricemia does not impair cardiovascular function in healthy adults. Heart 2004, 90, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L.; Shannon, J.; Frei, B.; Kaye, J.A.; Quinn, J.F. Uric acid as a CNS antioxidant. J. Alzheimers Dis. 2010, 19, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- McFarland, N.R.; Burdett, T.; Desjardins, C.A.; Frosch, M.P.; Schwarzschild, M.A. Postmortem brain levels of urate and precursors in Parkinson’s disease and related disorders. Neurodegener. Dis. 2013, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Bagnati, M.; Perugini, C.; Cau, C.; Bordone, R.; Albano, E.; Bellomo, G. When and why a water-soluble antioxidant becomes pro-oxidant during copper-induced low-density lipoprotein oxidation: A study using uric acid. Biochem. J. 1999, 340 Pt 1, 143–152. [Google Scholar] [CrossRef] [PubMed]
- So, A.; Thorens, B. Uric acid transport and disease. J. Clin. Investig. 2010, 120, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Desideri, G.; Gentile, R.; Antonosante, A.; Benedetti, E.; Grassi, D.; Cristiano, L.; Manocchio, A.; Selli, S.; Ippoliti, R.; Ferri, C.; et al. Uric Acid Amplifies Aβ Amyloid Effects Involved in the Cognitive Dysfunction/Dementia: Evidences From an Experimental Model In Vitro. J. Cell. Physiol. 2017, 232, 1069–1078. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.S.; Lee, W.W.; Ham, J.H.; Lee, J.J.; Lee, P.H.; Sohn, Y.H. Alzheimer’s Disease Neuroimaging Iniziative. Does serum uric acid act as a modulator of cerebrospinal fluid Alzheimer’s disease biomarker related cognitive decline? Eur. J. Neurol. 2016, 23, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Kawaguchi, A.; Tomiyama, H.; Ishizu, T.; Matsumoto, C.; Higashi, Y.; Takase, B.; Suzuki, T.; Ueda, S.; Yamazaki, T.; et al. Cross-sectional and longitudinal associations between serum uric acid and endothelial function in subjects with treated hypertension. Int. J. Cardiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Puddu, P.; Puddu, G.M.; Cravero, E.; Vizioli, L.; Muscari, A. Relationships among hyperuricemia, endothelial dysfunction and cardiovascular disease: Molecular mechanisms and clinical implications. J. Cardiol. 2012, 59, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Khosla, U.M.; Zharikov, S.; Finch, J.L.; Nakagawa, T.; Roncal, C.; Mu, W.; Krotova, K.; Block, E.R.; Prabhakar, S.; Johnson, R.J. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005, 67, 1739–1742. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.J.; Bruinsma, K.A. Uric acid is closely linked to vascular nitric oxide activity. Evidence for mechanism of association with cardiovascular disease. J. Am. Coll. Cardiol. 2001, 38, 1850–1858. [Google Scholar] [CrossRef]
- Perez-Ruiz, F.; Becker, M.A. Inflammation: A possible mechanism for a causative role of hyperuricemia/gout in cardiovascular disease. Curr. Med. Res. Opin. 2015, 31 (Suppl. 2), 9–14. [Google Scholar] [CrossRef] [PubMed]
- Satizabal, C.L.; Zhu, Y.C.; Mazoyer, B.; Dufouil, C.; Tzourio, C. Circulating IL-6 and CRP are associated with MRI findings in the elderly: The 3C-Dijon Study. Neurology 2012, 78, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.; Lu, W.; Gao, F.; Li, D.; Hu, J.; Li, Y.; Zuo, Z.; Jie, H.; Zhao, Y.; Cen, X. Uric Acid Induces Cognitive Dysfunction through Hippocampal Inflammation in Rodents and Humans. J. Neurosci. 2016, 36, 10990–11005. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Custodero, C.; Lozupone, M.; Imbimbo, B.P.; Valiani, V.; Agosti, P.; Schilardi, A.; D’Introno, A.; La Montagna, M.; Calvani, M.; et al. Relationships of dietary patterns, foods, and micro-and macronutrients with Alzheimer’s disease and late-life cognitive disorders: A systematic review. J. Alzheimers Dis. 2017, 59, 815–849. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, M.D.; Chrysohoou, C.; Panagiotakos, D.B.; Tsetsekou, E.; Zeimbekis, A.; Pitsavos, C.; Stefanadis, C. Adherence to the Mediterranean diet and serum uric acid: The ATTICA study. Scand. J. Rheumatol. 2012, 41, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Guash-Ferrè, M.; Bullò, M.; Babio, N.; Martinez-Gonzalez, M.A.; Estruch, R.; Covas, M.I.; Warnberg, J.; Aros, F.; Lapetra, J.; Serra-Majem, L.; et al. Mediterranean diet and risk of hyperuricemia in elderly participants at high cardiovascular risk. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Xiang, Y.B.; Elasy, T.; Xu, W.H.; Cai, H.; Cai, Q.; Linton, M.F.; Fazio, S.; Zheng, W.; Shu, X.O. Purine-rich foods, protein intake, and the prevalence of hyperuricemia: The Shanghai Men’s Health Study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.A.; Kang, H.H.; Kim, S.Y.; Yoo, M.K.; Kim, J.S.; Lee, C.H.; Wie, G.A. Comparison of nutrient intake and diet quality between hyperuricemia subjects and controls in Korea. Clin. Nutr. Res. 2014, 3, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Song, P.; Li, J.; Wang, P.; Li, G. Relationship between hyperuricemia and dietary risk factors in Chinese adults: A cross-sectional study. Rheumatol. Int. 2015, 35, 2079–2089. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Lauretani, F.; Ceda, G.P.; Ruggiero, C.; Ferrucci, L.; Aloe, R.; Larsson, A.; Cederholm, T.; Lind, L.; Meschi, T.; et al. Uric acid and endothelial function in elderly community-dwelling subjects. Exp. Gerontol. 2017, 89, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Nouvenne, A.; Ticinesi, A.; Maggio, M.; Lauretani, F.; Ceda, G.P.; Borghi, L.; Meschi, T. The role of malnutrition in older persons with mobility limitations. Curr. Pharm. Des. 2014, 20, 3173–3177. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Sisto, A.; Marzetti, E. Anorexia of aging: Risk factors, consequences and potential treatments. Nutrients 2016, 8, 69. [Google Scholar] [CrossRef] [PubMed]
- Beberashvili, I.; Sinuani, I.; Azar, A.; Shapiro, G.; Feldman, L.; Stav, K.; Sandbank, J.; Averbukh, Z. Serum uric acid as a clinically useful nutritional marker and predictor of outcome in maintenance hemodialysis patients. Nutrition 2015, 31, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.J.; Hwang, J.C.; Lu, Y.H.; Wang, C.T. Clinical implications and outcome prediction in chronic hemodialysis patients with lower serum potassium x uric acid product. Eur. J. Intern. Med. 2015, 26, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Saka, B.; Kaya, O.; Ozturk, G.B.; Erten, N.; Karan, M.A. Malnutrition in the elderly and its relationship with other geriatric syndromes. Clin. Nutr. 2010, 29, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Sanders, C.; Behrens, S.; Schwartz, S.; Wengreen, H.; Corcoran, C.D.; Lyketsos, C.G.; Tschanz, J.T. Nutritional status is associated with faster cognitive decline and worse functional impairment in the progression of dementia: The Cache County Dementia Progression Study. J. Alzheimers Dis. 2016, 52, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Kolobova, I.; Crapper, L.; Ernst, C. Lesch-Nyhan Syndrome: Models, Theories, and Therapies. Mol. Syndromol. 2016, 7, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Sebesta, I.; Stiburkova, B. Purine disorders with hypouricemia. Prilozi 2014, 35, 87–92. [Google Scholar] [PubMed]
- Latourte, A.; Bardin, T.; Richette, P. Uric acid and cognitive decline: A double-edge sword? Curr. Opin. Rheumatol. 2018, 30, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Fujinaga, S.; Ito, A.; Nakagawa, M.; Watanabe, T.; Ohtomo, Y.; Shimizu, T. Posterior reversible encephalopathy syndrome with exercise-induced acute kidney injury in renal hypouricemia type 1. Eur. J. Pediatr. 2013, 172, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, G.G.; Lee, Y.H. Uric acid and incident dementia: A population-based cohort study. Ann. Rheum. Dis. 2017. [Google Scholar] [CrossRef] [PubMed]
- Savva, G.M.; Arthur, A. Who has undiagnosed dementia? A cross-sectional analysis of participants of the Aging, Demographics and Memory Study. Age Ageing 2015, 44, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Lauretani, F.; Ticinesi, A.; Prati, B.; Nouvenne, A.; Meschi, T. Molecular and Clinical Issues about the Risk of Venous Thromboembolism in Older Patients: A Focus on Parkinson’s Disease and Parkinsonism. Int. J. Mol. Sci. 2018, 19, 1299. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.; Cherubini, A.; Lauretani, F.; Bandinelli, S.; Maggio, M.; Di Iorio, A.; Zuliani, G.; Dragonas, C.; Senin, U.; Ferrucci, L. Uric acid and dementia in community-dwelling older persons. Dement. Geriatr. Cogn. Disord. 2009, 27, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Lauretani, F.; Milani, C.; Nouvenne, A.; Tana, C.; Del Rio, D.; Maggio, M.; Ventura, M.; Meschi, T. Aging Gut Microbiota at the Cross-Road between Nutrition, Physical Frailty, and Sarcopenia: Is There a Gut-Muscle Axis? Nutrients 2017, 9, 1303. [Google Scholar] [CrossRef] [PubMed]
- Santos-García, D.; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; Martínez-Martín, P. COPPADIS Study Group.COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global—Clinical evaluations, serum biomarkers, genetic studies and neuroimaging—Prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar]


{kind=link}
| First Author, Journal, Year [Ref] | Type of Study | Population | Duration | Dementia Subtype | Main Results |
|---|---|---|---|---|---|
| Euser et al. 2009 [5] | Prospective | 7983 subjects | 11 years | AD | Dementia risk reduction with higher sUA levels (HR 0.89; 95% CI: 0.80–0.99, p 0.030). |
| Verhaaren et al. 2013 [6] | Cross-sectional analysis from the Rotterdam study | 814 persons of the Rotterdam Study | N/A | AD | Significant relation between hyperuricemia and worse cognitive performance (Z score difference −0.28 (−0.48; −0.08)). |
| Hong et al. 2015 [7] | Prospective | 28,769 gouty patients and 114,742 controls | 6 years | AD and VD | Lower risk of AD (HR 0.77; 95% CI: 0.72–0.83; p < 0.001) and of VD (HR: 0.76; 95% CI: 0.65–0.88; p < 0.001) in patients with hyperuricemia |
| Lu et al. 2016 [8] | Prospective | 59,224 gouty patients and 1942 controls | 5 years | AD | Higher risk of dementia in gouty patients (HR of 0.76 (95% CI 0.66 to 0.87) at multivariate and 0.71 (95% CI 0.62 to 0.80) at univariate analysis). |
| Gao et al. 2016 [15] | Prospective | 90,214 subjects | 34 years | PD | Lower risk (0.63 (95% CI 0.35, 1.10; p = 0.049)) of developing PD in men with higher sUA levels |
| Latourte et al. 2018 [19] | Prospective | 1598 subjects | 10.1 years | VD | Significant risk of VD or mixed dementia in patients with higher sUA levels (HR = 3.66, 95% CI: 1.29–10.41, p = 0.015) |
| Liu et al. 2017 [25] | Prospective | 2012 subjects | 2 years | MCI | Risk reduction of MCI with increasing sUA values (OR 1.65(95% CI: 1.12–2.43) and 1.92 (95% CI: 1.02–3.35) for the highest quarters in men and women, respectively). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tana, C.; Ticinesi, A.; Prati, B.; Nouvenne, A.; Meschi, T. Uric Acid and Cognitive Function in Older Individuals. Nutrients 2018, 10, 975. https://doi.org/10.3390/nu10080975
Tana C, Ticinesi A, Prati B, Nouvenne A, Meschi T. Uric Acid and Cognitive Function in Older Individuals. Nutrients. 2018; 10(8):975. https://doi.org/10.3390/nu10080975
Chicago/Turabian StyleTana, Claudio, Andrea Ticinesi, Beatrice Prati, Antonio Nouvenne, and Tiziana Meschi. 2018. "Uric Acid and Cognitive Function in Older Individuals" Nutrients 10, no. 8: 975. https://doi.org/10.3390/nu10080975
APA StyleTana, C., Ticinesi, A., Prati, B., Nouvenne, A., & Meschi, T. (2018). Uric Acid and Cognitive Function in Older Individuals. Nutrients, 10(8), 975. https://doi.org/10.3390/nu10080975