
Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review

 ,
, 
Abstract
1. Introduction
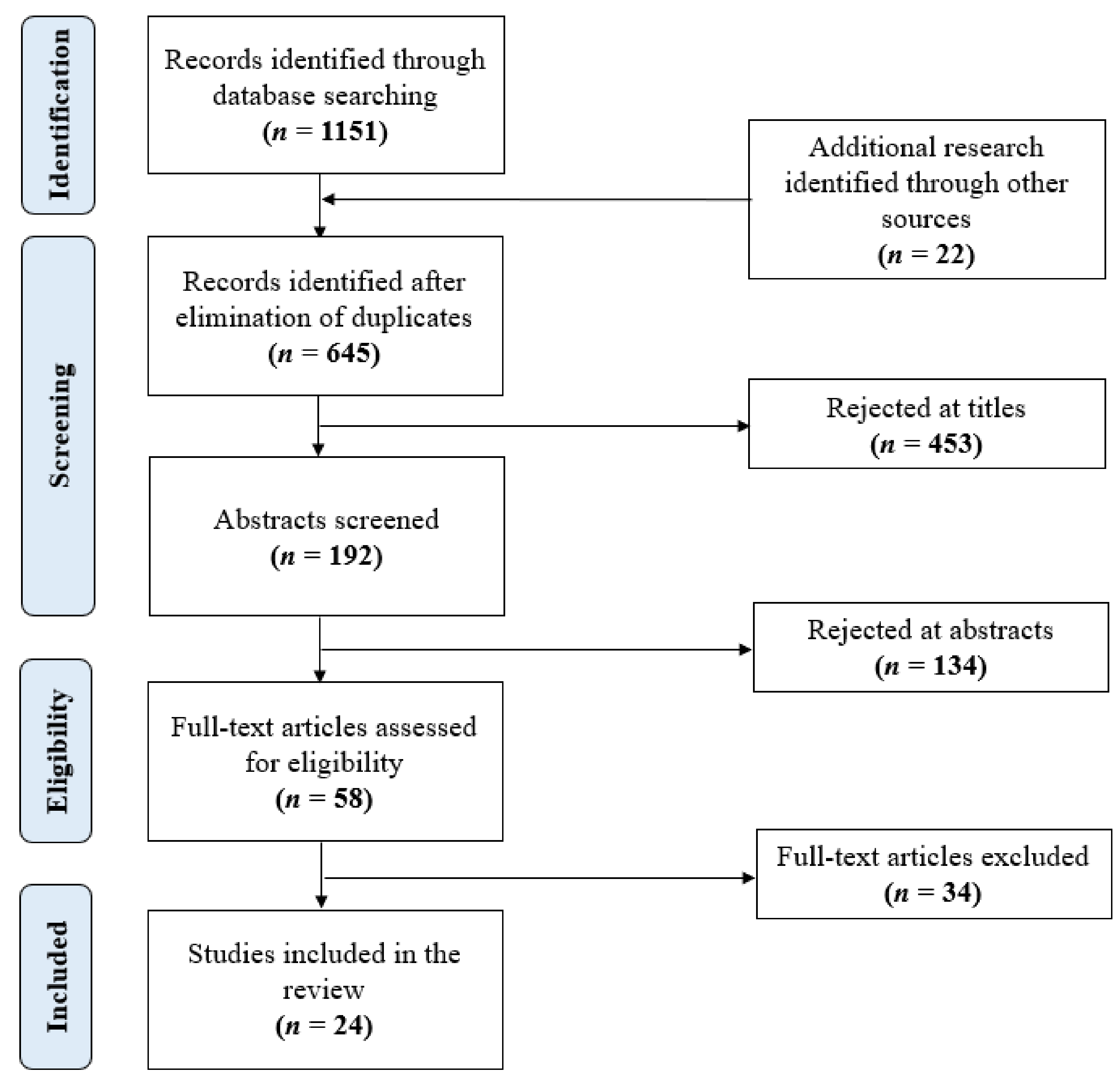
2. Materials and Methods
2.1. Data Collection
2.2. Search Terms
2.3. Inclusion/Exclusion Criteria
2.4. Quality Assessment and Data Extraction
3. Results
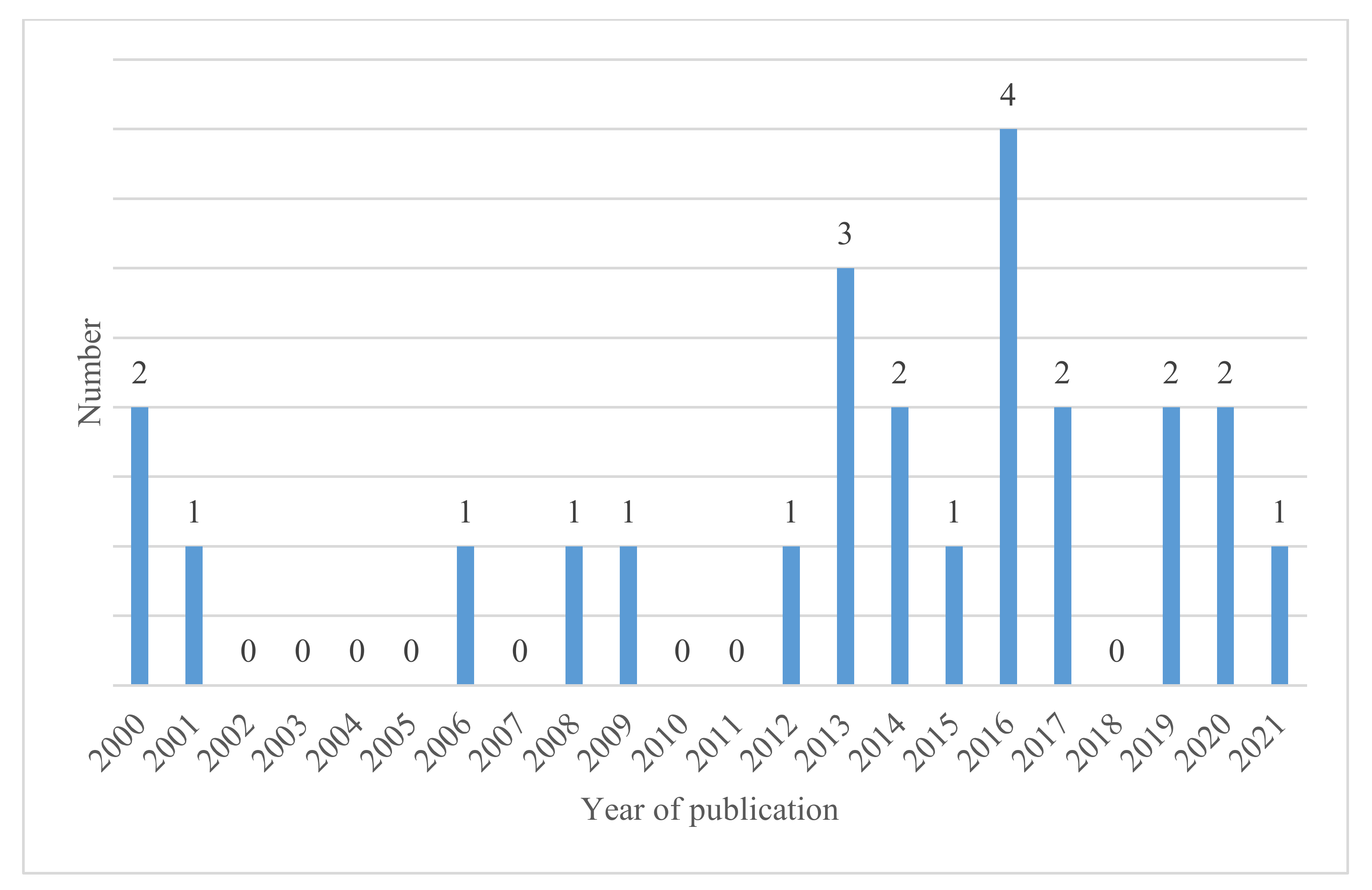
3.1. Study Authors, Year of Publication, and Country of Origin
3.2. Population, Sample Size, and Study Type
3.3. Objectives of the Studies
3.4. Technology Used
3.5. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haththotuwa, R.N.; Wijeyaratne, C.N.; Senarath, U. Worldwide epidemic of obesity. In Obesity and Obstetrics; Elsevier: Amsterdam, The Netherlands, 2020; pp. 3–8. [Google Scholar]
- Mqnsia BIOTECH. Obesity and Diabetes in the World. Available online: https://www.a-mansia.com/obesity-and-diabetes-in-the-world/ (accessed on 5 February 2021).
- World Health Organization. Obesity and Overweight. 2021. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 28 June 2021).
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Agha, M.; Agha, R. The rising prevalence of obesity: Part B—Public health policy solutions. Int. J. Surg. Oncol. 2017, 2, e19. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.; Le Roux, C.W.; Docherty, N. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef]
- Hill, J.O.; Peters, J.C. Environmental contributions to the obesity epidemic. Science 1998, 280, 1371–1374. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, A.G.; Després, J.-P.; Frank, B.H. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Popkin, B.M. Urbanization, lifestyle changes and the nutrition transition. World Dev. 1999, 27, 1905–1916. [Google Scholar] [CrossRef]
- Raziani, Y.; Raziani, S. Investigating the predictors of overweight and obesity in children. Int. J. Adv. Stud. Humanit. Soc. Sci. 2020, 9, 262–280. [Google Scholar]
- LeBlanc, E.S.; Patnode, C.D.; Webber, E.M.; Redmond, N.; Rushkin, M.; O’Connor, E.A. Behavioral and pharmacotherapy weight loss interventions to prevent obesity-related morbidity and mortality in adults: Updated evidence repevidence report and systematic review for the US Preventive Services Task Force. JAMA 2018, 320, 1172–1191. [Google Scholar] [CrossRef]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef]
- Gorini, A.; Gaggioli, A.; Vigna, C.; Riva, G. A second life for eHealth: Prospects for the use of 3-D virtual worlds in clinical psychology. J. Med. Internet Res. 2008, 10, e21. [Google Scholar] [CrossRef]
- Thomas, J.G.; Goldstein, C.M.; Bond, D.S.; Lillis, J.; Hekler, E.B.; Emerson, J.A.; Espel-Huynh, H.M.; Goldstein, S.P.; Dunsiger, S.I.; Evans, E.W.; et al. Evaluation of intervention components to maximize outcomes of behavioral obesity treatment delivered online: A factorial experiment following the multiphase optimization strategy framework. Contemp. Clin. Trials 2021, 100, 106217. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J.; Hill, D. The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care; Basic Books: New York, NY, USA, 2012. [Google Scholar]
- Meskó, B.; Drobni, Z.D.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital health is a cultural transformation of traditional healthcare. mHealth 2017, 3, 38. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Gaggioli, A. Virtual clinical therapy. In Digital Human Modeling; Springer: Berlin/Heidelberg, Germany, 2008; pp. 90–107. [Google Scholar]
- Pillai, A.S.; Mathew, P.S. Impact of virtual reality in healthcare: A review. In Virtual and Augmented Reality in Mental Health Treatment; IGI Global: Hershey, PA, USA, 2019; pp. 17–31. [Google Scholar]
- Kohler, T.; Matzler, K.; Füller, J. Avatar-based innovation: Using virtual worlds for real-world innovation. Technovation 2009, 29, 395–407. [Google Scholar] [CrossRef]
- Mantovani, F.; Castelnuovo, G.; Gaggioli, A.; Riva, G. Virtual reality training for health-care professionals. CyberPsychol. Behav. 2003, 6, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Garcia, M.; Gutiérrez-Maldonado, J.; Riva, G. Virtual reality based treatments in eating disorders and obesity: A review. J. Contemp. Psychother. 2013, 43, 207–221. [Google Scholar] [CrossRef]
- Slater, M.; Lotto, B.; Arnold, M.M.; Sánchez-Vives, M.V. How we experience immersive virtual environments: The concept of presence and its measurement. Anu. Psicol. 2009, 40, 193–210. [Google Scholar]
- Riva, G.; Malighetti, C.; Serino, S. Virtual reality in the treatment of eating disorders. Clin. Psychol. Psychother. 2021, 28, 477–488. [Google Scholar] [CrossRef]
- Ossolinski, G.; Jiwa, M.; McManus, A.; Parsons, R. Do images of a personalised future body shape help with weight loss? A randomised controlled study. Trials 2017, 18, 1. [Google Scholar] [CrossRef]
- Behm-Morawitz, E.; Lewallen, J.; Choi, G. A second chance at health: How a 3D virtual world can improve health self-efficacy for weight loss management among adults. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 74–79. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Cesa, G.L.; Bacchetta, M.; Castelnuovo, G.; Conti, S.; Gaggioli, A.; Mantovani, F.; Molinari, E.; Cárdenas-López, G.; Riva, G. Virtual reality–enhanced cognitive–behavioral therapy for morbid obesity: A randomized controlled study with 1 year follow-up. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 134–140. [Google Scholar] [CrossRef]
- Cesa, G.L.; Manzoni, G.M.; Bacchetta, M.; Castelnuovo, G.; Conti, S.; Gaggioli, A.; Mantovani, F.; Molinari, E.; Cárdenas-López, G.; Riva, G. Virtual reality for enhancing the cognitive behavioral treatment of obesity with binge eating disorder: Randomized controlled study with one-year follow-up. J. Med. Internet Res. 2013, 15, e113. [Google Scholar] [CrossRef] [PubMed]
- Wiederhold, B.K. The Potential for Virtual Reality to Improve Health Care; The Virtual Reality Medical Centre (VRMC): San Diego, CA, USA, 2006. [Google Scholar]
- Boulos, M.N.K.; Hetherington, L.; Wheeler, S. Second Life: An overview of the potential of 3-D virtual worlds in medical and health education. Health Inf. Libr. J. 2007, 24, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Alturki, R.; Gay, V. Augmented and virtual reality in mobile fitness applications: A survey. In Applications of Intelligent Technologies in Healthcare; Springer: Cham, Switzerland, 2019; pp. 67–75. [Google Scholar] [CrossRef]
- Heide, V.D.; Brandon, E.M.S.; Peterson, A.M.; Jones, E.B. The Proteus effect in dyadic communication: Examining the effect of avatar appearance in computer-mediated dyadic interaction. Commun. Res. 2013, 40, 838–860. [Google Scholar] [CrossRef]
- Scarpina, F.; Serino, S.; Keizer, A.; Chirico, A.; Scacchi, M.; Castelnuovo, G.; Mauro, A.; Riva, G. The effect of a virtual-reality full-body illusion on body representation in obesity. J. Clin. Med. 2019, 8, 1330. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Goldstein, C.M.; Bond, D.S.; Hadley, W.; Tuerk, P.W. Web-based virtual reality to enhance behavioural skills training and weight loss in a commercial online weight management programme: The Experience Success randomized trial. Obes. Sci. Pract. 2020, 6, 587–595. [Google Scholar] [CrossRef]
- Phelan, S.; Peruvemba, S.; Levinson, D.; Stulberg, N.; Lacy, A.; Legato, M.; Werner, J.P. Feasibility of a virtual reality-based approach to improve behavioral weight management outcomes. Pilot Feasibility Stud. 2021, 7, 129. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Bond, D.S. Review of innovations in digital health technology to promote weight control. Curr. Diabetes Rep. 2014, 14, 485. [Google Scholar] [CrossRef]
- Tufano, J.T.; Karras, B.T.; Buchan, I. Mobile eHealth interventions for obesity: A timely opportunity to leverage convergence trends. J. Med. Internet Res. 2005, 7, e58. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; pp. 1–12. [Google Scholar]
- Navarro, J.; Cebolla, A.; Llorens, R.; Borrego, A.; Baños, R.M. Manipulating self-avatar body dimensions in virtual worlds to complement an internet-delivered intervention to increase physical activity in overweight women. Int. J. Environ. Res. Public Health 2020, 17, 4045. [Google Scholar] [CrossRef] [PubMed]
- Nosek, M.A.; Robinson-Whelen, S.; Ledoux, T.A.; Hughes, R.B.; O’Connor, D.P.; Lee, R.E.; Goe, R.; Silveira, S.L.; Markley, R.; Nosek, T.M.; et al. A pilot test of the GoWoman weight management intervention for women with mobility impairments in the online virtual world of Second Life®. Disabil. Rehabilit. 2019, 41, 2718–2729. [Google Scholar] [CrossRef] [PubMed]
- Sgobbi, F.S.; Tarouco, L.M.R.; Reategui, E.B. The pedagogical use of the Internet of Things in virtual worlds to encourage a behavior change in obese individuals. In Proceedings of the 2017 IEEE International Conference on Internet of Things (iThings) and IEEE Green Computing and Communications (GreenCom) and IEEE Cyber, Physical and Social Computing (CPSCom) and IEEE Smart Data (SmartData), Exeter, UK, 21–23 June 2017. [Google Scholar]
- Perpiñá, C.; Roncero, M. Similarities and differences between eating disorders and obese patients in a virtual environment for normalizing eating patterns. Compr. Psychiatry 2016, 67, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Scarpina, F.; Keizer, A.; Pedroli, E.; Dakanalis, A.; Castelnuovo, G.; Chirico, A.; Novelli, M.; Gaudio, S.; Riva, G. A novel technique for improving bodily experience in a non-operable super–super obesity case. Front. Psychol. 2016, 7, 837. [Google Scholar] [CrossRef] [PubMed]
- Lopez, G.C.; Martinez, P.; Riva, G.; Duran-Baca, X.; Torres, G. Virtual reality environments as auxiliaries in the treatment of obesity. In Proceedings of the 2015 Virtual Reality International Conference, Laval, France, 8–10 April 2015. [Google Scholar] [CrossRef]
- Lopez, G.C.; Torres-Villalobos, G.; Martinez, P.; Carreño, V.; Duran, X.; Dakanalis, A.; Gaggioli, A.; Riva, G. Virtual reality for improving body image disorders and weight loss after gastric band surgery: A case series. In Medicine Meets Virtual Reality 21; IOS Press: Amsterdam, The Netherlands, 2014; pp. 43–47. [Google Scholar]
- Thomas, J.G.; Spitalnick, J.S.; Hadley, W.; Bond, D.S.; Wing, R.R. Development of and feedback on a fully automated virtual reality system for online training in weight management skills. J. Diabetes Sci. Technol. 2014, 9, 145–148. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Hayes, S.; Russo, G.; Muresu, D.; Giordano, A.; Foster, G.D. Using avatars to model weight loss behaviors: Participant attitudes and technology development. J. Diabetes Sci. Technol. 2013, 7, 1057–1065. [Google Scholar] [CrossRef]
- Sullivan, D.K.; Goetz, J.R.; Gibson, C.A.; Washburn, R.A.; Smith, B.K.; Lee, J.; Gerald, S.; Fincham, T.; Donnelly, J.E. Improving weight maintenance using virtual reality (second life). J. Nutr. Educ. Behav. 2013, 45, 264–268. [Google Scholar] [CrossRef]
- Johnston, J.D.; Massey, A.P.; DeVaneaux, C. Innovation in weight loss intervention programs: An examination of a 3D virtual world approach. In Proceedings of the 2012 45th Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2012. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Pagnini, F.; Gorini, A.; Preziosa, A.; Castelnuovo, G.; Molinari, E.; Riva, G. Can relaxation training reduce emotional eating in women with obesity? An exploratory study with 3 months of follow-up. J. Am. Diet. Assoc. 2009, 109, 1427–1432. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Gorini, A.; Preziosa, A.; Pagnini, F.; Castelnuovo, G.; Molinari, E.; Riva, G. New technologies and relaxation: An explorative study on obese patients with emotional eating. J. Cyberther. Rehabilit. 2008, 1, 182–192. [Google Scholar]
- Riva, G.; Bacchetta, M.; Cesa, G.; Conti, S.; Castelnuovo, G.; Mantovani, F.; Molinari, E. Is severe obesity a form of addiction?: Rationale, clinical approach, and controlled clinical trial. Cyberpsychol. Behav. 2006, 9, 457–479. [Google Scholar] [CrossRef]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Molinari, E. Virtual Reality–based multidimensional therapy for the treatment of body image disturbances in obesity: A controlled study. CyberPsychol. Behav. 2001, 4, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Cirillo, G.; Molinari, E. Virtual reality environment for body image modification: A multidimensional therapy for the treatment of body image in obesity and related pathologies. CyberPsychol. Behav. 2000, 3, 421–431. [Google Scholar] [CrossRef]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Rinaldi, S.; Vincelli, F.; Molinari, E. Virtual reality-based experiential cognitive treatment of obesity and binge-eating disorders. Clin. Psychol. Psychother. 2000, 7, 209–219. [Google Scholar] [CrossRef]
- Horne, M.; Hill, A.; Murells, T.; Ugail, H.; Irving; Chinnadorai, R.; Hardy, M. Using avatars in weight management settings: A systematic review. Internet Interv. 2020, 19, 100295. [Google Scholar] [CrossRef] [PubMed]
- Rumbo-Rodríguez, L.; Sánchez-SanSegundo, M.; Ruiz-Robledillo, N.; Albaladejo-Blázquez, N.; Ferrer-Cascales, R.; Zaragoza-Martí, A. Use of technology-based interventions in the treatment of patients with overweight and obesity: A systematic review. Nutrients 2020, 12, 3634. [Google Scholar] [CrossRef]
- Castelnuovo, G.; Pietrabissa, G.; Manzoni, G.M.; Cattivelli, R.; Rossi, A.; Novelli, M.; Varallo, G.; Molinari, E. Cognitive behavioral therapy to aid weight loss in obese patients: Current perspectives. Psychol. Res. Behav. Manag. 2017, 10, 165–173. [Google Scholar] [CrossRef]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 35. [Google Scholar] [CrossRef]
- Dascal, J.; Reid, M.; Ishak, W.W.; Spiegel, B.; Recacho, J.; Rosen, B.; Danovitch, I. Virtual reality and medical inpatients: A systematic review of randomized, controlled trials. Innov. Clin. Neurosci. 2017, 14, 14. [Google Scholar]
- Kuo, H.-C.; Lee, C.-C.; Chiou, W.-B. The power of the virtual ideal self in weight control: Weight-reduced avatars can enhance the tendency to delay gratification and regulate dietary practices. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 80–85. [Google Scholar] [CrossRef]
- Matsangidou, M.; Otkhmezuri, B.; Ang, C.S.; Avraamides, M.; Riva, G.; Gaggioli, A.; Iosif, D.; Karekla, M. “Now I can see me” designing a multi-user virtual reality remote psychotherapy for body weight and shape concerns. Hum.-Comput. Interact. 2020, 1–27. [Google Scholar] [CrossRef]
- Young, K.S.; Rennalls, S.J.; Leppanen, J.; Mataix-Cols, D.; Simmons, A.; Suda, M.; Campbell, I.C.; O’Daly, O.; Cardi, V. Exposure to food in anorexia nervosa and brain correlates of food-related anxiety: Findings from a pilot study. J. Affect. Disord. 2020, 274, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, M.R.; Dias, T.R.D.S.; Duchesne, M.; Nardi, A.E.; Appolinario, J.C. Virtual reality as a promising strategy in the assessment and treatment of bulimia nervosa and binge eating disorder: A systematic review. Behav. Sci. 2017, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Botvinick, M.; Cohen, J. Rubber hands ‘feel’ touch that eyes see. Nature 1998, 391, 756. [Google Scholar] [CrossRef] [PubMed]
- Tagini, S.; Scarpina, F.; Bruni, F.; Scacchi, M.; Mauro, A.; Zampini, M. The virtual hand illusion in obesity: Dissociation between multisensory interactions supporting illusory experience and self-location recalibration. Multisens. Res. 2020, 33, 337–361. [Google Scholar] [CrossRef]
- Crea, S.; D’Alonzo, M.; Vitiello, N.; Cipriani, C. The rubber foot illusion. J. Neuro Eng. Rehabilit. 2015, 12, 77. [Google Scholar] [CrossRef]
- Robertson, C.; Archibald, D.; Avenell, A.; Douglas, F.; Hoddinott, P.; van Teijlingen, E.; Boyers, D.; Stewart, F.; Boachie, C.; Fioratou, E.; et al. Systematic reviews of and integrated report on the quantitative, qualitative and economic evidence base for the management of obesity in men. Health Technol. Assess. 2014, 18, 35. [Google Scholar] [CrossRef]
- Dombrowski, S.U.; Knittle, K.; Avenell, A.; Araujo-Soares, V.; Sniehotta, F.F. Long term maintenance of weight loss with non-surgical interventions in obese adults: Systematic review and meta-analyses of randomised controlled trials. BMJ 2014, 348, g2646. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Ref. | Country | Mean Age | Mean Weight | Sample | Objective | Study Type |
|---|---|---|---|---|---|---|
| [34] | USA | 43 | BMI ≥ 25 | 15 participants | Testing the viability of using VR in a traditional behavioral weight-loss program. | Pilot randomized study |
| [40] | Spain | 31.9 | BMI = 28.7 | 42 women | Analyzing the impact of avatar body dimensions on the efficacy of an online intervention to raise PA levels as well as the impact on other related variables (self-efficacy, enjoyment, anxiety, PA motivation, and PA goals). | Randomized controlled study |
| [33] | USA | 18–70 | BMI = 25–45 | Total: 146 Men: 32 Women: 114 | Evaluating the impact of a web-based VR program on behavioral skill training and weight loss when used in conjunction with a commercially available online weight-loss program. | Randomized controlled study |
| [41] | USA | 49.62 | BMI = 31.67 | 13 women | (i) Comparing weight, waist circumference, nutrition knowledge, and self-efficacy for diet and PA before and after the GoWoman intervention; (ii) assessing intervention feasibility (fidelity, attrition, engagement, and acceptability). | Non-controlled study Pilot test |
| [32] | Italy | 32 obese 29 healthy | BMI = 45 obese 22 healthy | Total: 30 15 obese 15 healthy | Investigating whether patients with obesity can successfully experience ownership of a virtual body with a thin abdomen. | Non-randomized controlled study |
| [24] | Australia | 18–79 | BMI ≥ 25 | Total: 145 Men: 27 Women:118 | Evaluating the impact of a personalized future self-image developed by a computer on weight loss. | Randomized controlled study |
| [42] | Brazil | 40 | BMI ≥ 25 | Men The number is N/A | Discussing how the Internet of Things (IoT) can be used in the virtual world to assist obese individuals in learning more about self-care and losing weight. | Non-controlled study |
| [25] | USA | 18–61 | BMI ≥ 25 | 90 women | Examining the usefulness of VR and play in a virtual social world (Second Life) in promoting health self-efficacy in overweight people. | Randomized controlled study |
| [26] | Italy | 18–50 | BMI > 40 | 163 women | Testing the long-term efficacy of VR-based CBT to open the body’s negative memories and changing its emotional and behavioral associations with obesity. | Randomized controlled study |
| [43] | Spain | 39.26 obese 24.75 ED 23 NC | BMI = 36.33 obese 20.45 ED 21.16 NC | 62 women 19 obese 20 ED 23 NC | Comparing the reality judgments of ED and obese patients in a virtual environment meant to normalize their eating patterns. | Non-randomized controlled study |
| [44] | Italy | 37 | BMI = 62.2 | One woman | Discussing the impact of the illusion of body ownership over a different body (a virtual body with a little tummy) on the recovery of motivation for change with a severely obese patient. | Case study/report |
| [45] | Mexico | 18–50 | BMI > 30 | Total: 24 women and men | Discussing the role of VR in tackling obesity as part of a comprehensive cognitive behavioral approach. | Randomized controlled study |
| [46] | Mexico | M = 37 | BMI ≥ 25 | Total: 3 Men: 1 Women: 2 | Discussing the potential impact of VR in improving body image after LAGB surgery within the context of an integrated cognitive behavioral approach. | Case study/report |
| [47] | USA | M = 55 | BMI = 34.6 | 37 women | Developing a system for building and distributing automated VR scenarios for online BWL skill training as well as collecting feedback from test users using a social dining scenario as an example. | Randomized controlled study |
| [27] | Italy | 18–50 | BMI > 40 | 66 women | Testing short- and long-term clinical efficacy of enhanced CBT including VR in obese patients with BED compared with standard CBT and IP on weight loss, weight loss maintenance, BED reduction, and improvement in body satisfaction. | Randomized controlled study |
| [48] | USA | Phase 1: 34.10 Phase 2: 44.13 | Phase 1: 34.30 Phase 2: 33.32 | 136 women Phase 1: 128 Phase 2: 8 | Examining using avatar-based technologies to model weight-loss behaviors. | Non-controlled study |
| [49] | USA | M = 31.1 | BMI = 32.8 | Total: 20 Men: 3 Women:17 | Comparing between an FtF weight management clinic and a VR clinic regarding weight loss and maintenance. | Randomized control study |
| [50] | USA | 46.3 COI 37.5 FtF | BMI = 32.0 | Total: 54 Men: 9 Women: 45 | Examining the weight reduction and behavior modification effectiveness of a virtual weight loss program. | Quasi experiment |
| [51] | Italy | 18–60 | BMI = 30 | 60 women | Evaluating the effectiveness of a relaxation treatment augmented by VR and portable mp3 players in reducing emotional eating. | Randomized controlled study |
| [52] | Italy | 18–60 | BMI ≥ 30 | 60 women | Developing a relaxation routine employing VR and portable mp3 players to decrease stress and accompanying emotional eating episodes in obese individuals. | Randomized controlled study |
| [53] | Italy | 18–50 | BMI > 40 | 211 women | Proposing a biopsychosocial treatment strategy ECT for severely obese patients (BMI > 40). | Controlled study |
| [54] | Italy | 18–45 | BMI = 43.97 | 28 women | Evaluating the efficacy of a multi-dimensional VR-based strategy to treating body image attitudes and related components. | Controlled study |
| [55] | Italy | 18–45 | BMI = 42.11obese 41.82 BED 39.01 EDNOS | 57 women 18 obese 25 BEDS 14 EDNOS | Investigating the possibility of causing a significant shift in behavior and body image perception in obesity and related disorders using a psychological VR-based approach. | Non-controlled study |
| [56] | Italy | 18–45 | BMI = 41.82 | 25 women | Describing and evaluating a VR-based approach for the treatment and assessment of obesity and binge eating disorders (ExCT). | Non-controlled study |
| Ref. | Intervention Duration | No. of Groups | Technology | Study Design | Results |
|---|---|---|---|---|---|
| [34] | 4 weeks | 2 groups: G1: intervention G2: control) | SW: VR scenarios via an app (Restaurant, food cue, activity cue) HW: iPhone6+ VR headsets | -G1: 4 weeks BWLT + 3 weeks 15 min weight related VR scenario 3 times a week + 3 weight-control lessons -G2: 4 weeks BWLT + 3 weeks 15 min non-weight related VR scenario 3 times a week | Throughout the trial, both groups lost statistically significant amounts of weight. Over the course of four weeks, the control group and the intervention group shed an average (SD) unadjusted mean of 2.3% (3.6) and 3.4% (2.7), respectively, as a percentage of their original body weight. When comparing the proportion of participants who lost 5% or more of their primary body weight, 16% (1/6) of those in the control group and 43% (3/7) of those in the intervention group met this criterion. |
| [40] | 4 weeks | 3 groups: IAC: avatars with ideal body dimensions RAC: avatars with existing body dimensions NAC: no avatars | SW: The VR scenario representing a park where an avatar runs | - IAC: 1-week online PA + 1-week daily PA in the VR scenario for 4 min (default avatar) + 1-week PA 3 times a week. - RAC: same instructions, with changing avatar dimensions. - NAC: same instructions, with no avatar. | The online intervention was successful in increasing PA practice and self-efficacy expectations among overweight and obese women. Manipulation of avatar body dimensions had no effect on the outcome of this intervention. The use of ideal avatars appears to minimize anxiety during PA and the use of avatars that are identical to the individual themselves may have a stronger impact on PA and variables related to long-term practice. |
| HW: Kinect and 150 × 150 cm screen | |||||
| [33] | 6 months | 2 groups: Participants accessed (WW) program alone Participants accessed (WW + ES) | SW: WW ES | - WW: 6 months access to WW program. - (WW+ES): WW+ 4 scenarios at weeks 2, 4, 6, 8 (home, work, gym, social situations) | Both groups lost statistically significant amounts of weight, with no difference in mean standard error weight loss between WW and WW+ES at three months (2.7 ± 1.1 kg vs. 4.2 ± 1.1 kg, respectively), but greater weight loss in WW+ES at six months (2.6 ± 1.3 kg vs. 4.9 ± 1.3 respectively). After a six-month trial, 20% of the WW group and 23% of the WW+ES group had lost 5% of their baseline weight. |
| HW: PC and/or mobile device with online connectivity | |||||
| [41] | 6 months | Single group | SW: GoWoman program based on SL MyFitnessPal App | 16 weekly virtual meetings in SL. The workshops included speaking exercises, discussion, and question/answer sessions. Participants created weekly action plans at the end of each session and used MyFitnessPal to track food intake and exercise. | Thirteen women attended eight of the sixteen GoWoman weekly sessions and lost an average of 5.97 pounds (2.71 kg) (3.31%) and 1.44 inches (3.66 cm) (3.58%) in body weight and waist circumference. Diet, PA, and self-efficacy for diet and PA all improved significantly. GoWoman demonstrated feasibility (fidelity = 97.81%, attrition= 46%, engagement (SD = 2.44), acceptability (SD = 0.48)). |
| HW: PC with Internet connection | |||||
| [32] | N/A | 2 groups: G1: experimental G2: control | SW: Unity3D MakeHuman | - G1: synchronization between tactile and visual stimulation. - G2: asynchronization between tactile and visual stimulation. | Obese as well as healthy-weight subjects claimed to have experienced the illusion. In terms of the body size estimation task, neither group reported any variations other than alterations in the estimation of the abdomen’s circumference following the experimental condition. |
| HW: HMD Portable computer | |||||
| [24] | 6 months | 2 groups: G1: Early image G2: delayed image | SW: “Future Me” app | - G1: hard copy of future self-image at the time of recruitment. - G2: hard copy of future self-image after 8 weeks. | In the delayed-image group, more than a fifth of those who completed the study lost 5% or more of their primary weight. Those in the group with the delayed image lost more weight than those in the group with the immediate image. In addition, men lost weight more quickly than women. Between the early and late image groups, there was no significant difference in the change in waist circumference or the proportion of people who lost 5% of their body weight. |
| HW: iPad | |||||
| [42] | NA | One group | SW: HIGIA system (Individual Habitat and Attitude Interactive Guide) | - Stage 1: visiting the virtual world to experience a fitness virtual environment. - Stage 2: performing PA through the user’s avatar. | There was a significant weight loss. In the first stage, the average weight loss was 5 kg, and in the second stage, the average weight loss was 2.5 kg. In addition, there was a 70% increase in body motion compared to the average amount stated by the participants in the initial interview. |
| HW: Smartphone Motion Sensor | |||||
| [25] | 4 weeks | 3 groups: 3D social virtual world 2D social networking No intervention group | SW: SL (using an avatar) + virtual health social networking site | - 3D: users utilized SL sessions at least twice a week in groups of 3–4. - 2D: users engaged in a virtual health community. - No intervention: no virtual interaction. | There was an increase in the exercise efficacy of the SL group, but not that of the control group. However, the SL intervention had no effect on nutrition efficacy—F (1, 38) = 1.99, p = 0.17. Weight loss was significantly different between the experimental and control groups: t (18) = 2.15, p = 0.04. Participants in the SL group lost 1.75 pounds compared to 0.91 pounds lost by participants in the control group. The weight reduction difference is insignificant, and the use of SL for long-term weight loss is only cautiously optimistic. Further, self-presence was associated with improved nutrition (p= 0.05), but not with exercise efficacy. Self-presence and avatar efficacy items had significantly positive relationships (p= 0.01). |
| HW: 2D screen Desktop computer | |||||
| [26] | 6 weeks + 1 year follow-up | 3 groups: SBP CBT VR-enhanced CBT | SW: NeuroVR | - SPB: 6 weeks standard treatment. - CBT: SPB + 5 weekly group weight loss sessions + 10 biweekly individual sessions (body image + weight maintenance). - VR-enhanced CBT: SPB + 5 weekly group weight loss sessions + 10 biweekly individual VR sessions. | The entire group lost a large amount of weight. On average, the control group lost 6.2% of their baseline body weight, whereas the CBT group lost 7.4% and the VR group lost 6.25% of their baseline body weight. After inpatient therapy, psychological variables such as eating behavior features and body satisfaction increased significantly (effect size 0.16–0.26). Surprisingly, despite the VR group demonstrating greater increases across the board, there was no statistically significant difference between the three conditions. At the one-year follow-up, the VR group is more likely than the SBP group (48 percent vs. 11 percent; p = 0.004) and the CBT group (48 percent vs. 29 percent; p = 0.08) to maintain or enhance weight reduction. |
| HW: HMD | |||||
| [43] | NA | 3 groups: Obese ED NC | SW: Non-immersive VE (graded exposure to feared foods in a virtual kitchen) | One VR session. The VE comprised of a kitchen where the participant could make, serve, and consume a meal “virtually.” The VR session lasted for 30 min. | - The ED group had the highest ratings in attention, presence, emotional involvement, reality judgment, and unpleasant feelings about the “forbidden” meal. - Obese people have the lowest ratings in terms of judging reality and presence, satisfaction, and a sense of physical space in a virtual world. In VR food, obese people are in a middle position. - The level of participation in the virtual world for ED patients and the level of attention for obese patients predicts the likelihood of consumption of the “forbidden” virtual meal. |
| HW: Laptop with 2D mouse | |||||
| [44] | 5 weeks | Single patient | SW: VR body-swapping illusion protocol | Multidisciplinary program (PA + psychological counseling). VR treatments (optical and the tactile estimation of body parts + VR body swap illusion). | Full-body illusion successfully induced identification with a thinner body in an individual suffering from severe obesity, improving body satisfaction, increasing motivation to engage in healthy behavior, and reducing anxious feelings related to the clinical condition. The woman lost 5.1 kg, which equates to a decrease of 3.7% of her baseline weight. |
| HW: HMD | |||||
| [45] | 12 weeks + 3-month follow up | 3 groups: CBT ECT CTRL | SW: Neuro VR 2.0 | - CBT: weekly group sessions + 10 biweekly individual sessions. - ECT: 12 individual discovery sessions in 12 weeks. | The findings suggest that adding VR therapy to an obesity treatment program improved the cognitive-behavioral approach, increased weight loss (15–20% of beginning weight) and improved psychological well-being. This decrease was accompanied by an overall improvement in mental health. After a three-month follow-up, both the weight loss and the level of well-being had improved even more. |
| HW: NA | |||||
| [46] | 6 weeks + 3-month follow up | Single group | SW: Neuro-VR 2.0 HW: PC | ECT treatment (5 weekly group sessions + 10 biweekly VR sessions). | The patients lost an additional 15–20% of their weight by the completion of the regimen. This decrease was accompanied by a general increase in psychological well-being: clinical data revealed significant improvements in anxiety and body image. As a result of this alteration, the number of avoidance behaviors decreased, while the number of adaptive behaviors increased. |
| [47] | 18 months | A single group | SW: ES | The ES social eating scenario: - Selecting a virtual coach. - Entering a virtual house. - Facing two categories of difficulties: interpersonal and practical. - Providing comments and suggestions on the total calorie content. | Participants described the scenario as “very realistic,” and mentioned that they had improved their capacity to deal with the issues it posed. Acceptability and feasibility were rated 6.5 out of 7 on a scale that included comprehensibility, believability, relevance, usefulness, applicability, ease of use, likeability, and likelihood of suggesting the VR scenario to others. |
| HW: PC + mouse | |||||
| [27] | 6 weeks + one-year follow-up | 3 groups: ECT CBT IP | SW: Neuro-VR 2.0 | CBT: routine care + 15 weekly sessions in 5 weeks. ECT: routine care + 5 weekly group sessions + 10 biweekly VR sessions. IP: 5-week hospital stays for routine care. | Weight loss was significant in all three treatments (ECT: 6.17 kg, CBT: 7.1 kg, IP: 6.6 kg), with no significant differences among groups. All groups witnessed significant increases in body satisfaction, with no variations among them. Both ECT and CBT were successful in maintaining or enhancing weight loss during the one-year follow-up. The majority of the weight lost throughout the inpatient program was recovered by control subjects. Binge eating episodes reduced to zero during the in-patient program; however, at the one-year follow-up, they were reported again in all three groups, but there was no discernible difference among the groups. |
| HW: PC | |||||
| [48] | 4 weeks | One group in each phase | SW: SL | Phase 1: online survey to obtain feedback about using avatars for modeling weight loss behaviors. Phase 2: 4-week usability test using 4 virtual environments (supermarket, home gym, dining room/kitchen, living room). | The average weight loss after four weeks was 1.6 kg (SD = 1.7). Usability: 100% of users indicated that they would recommend the program to others and that it has changed their eating and exercise habits. User preference: 25% of users stated they did not want an avatar that looked like them, but 75% stated they wanted an avatar that changed size and shape as they progressed through the program. |
| HW: PC + mouse + Internet connection | |||||
| [49] | 9 months | 2 groups: VR FtF | SW: SL | VR: 3 months SL classes and activities (e.g., grocery shopping, dining in a restaurant, working out in the gym). FtF: 3 months BWL program delivered FtF in a weight loss clinic. + 6-month maintenance program delivered via SL for all participants. | While the weight loss achieved through SL (7.6% of initial body weight) was smaller than that achieved through FtF treatment (10.8% of initial body weight), the degree of weight loss achieved through SL was equivalent to that of numerous FtF programs. Furthermore, individuals who got SL for the full six months lost more weight, thereby resulting in a total weight loss of 14% of their baseline body weight, compared to those who were initially randomized to FtF and regained some weight, thereby resulting in a 9.5% end-of-treatment weight loss. |
| HW: Computer + internet connection + headset | |||||
| [50] | 12 weeks | 2 groups: VR FtF | SW: COI | - VR: COI users (4 h/week), taking classes on nutrition, movement, and emotional issues regarding weight via their avatar. - Ftf: normal gym users. | Patients in both groups had dropped a significant amount of weight after 12 weeks (VR: 3.9 kg; FtF: 2.8 kg). When compared to their initial weight, the VR group lost an average of 4.3% of their body weight, with 33% of the patients losing a clinically significant (5%) amount of weight while FtF participants lost an average of 3.0%, with 29% losing a clinically significant amount of weight (5%). In addition, COI participants showed significant improvements in almost all behavioral change indicators except sleep (i.e., increased physical activity, fruit and vegetable intake, and the number of days on which breakfast is eaten). On the other hand, FtF participants exhibited no significant gains in any of the indicators. Participants in the COI group increased their confidence in their capacity to engage in physical exercise and resist eating, whereas those in the FtF group did not. |
| HW: PC + mouse + Internet connection | |||||
| [51] | 3 months | 3 groups: VR (relaxation protocol enhanced by VR) IM (relaxation protocol using imagery) CTRL | SW: VE (Green Valley) showed mountain landscape with relaxing lake scenes | - CTRL: 5-week hospital-based weight-loss program and rehabilitation program. -VR and IM: CTRL program + 12 individual relaxation training sessions provided traditionally (IM condition) or virtually (VR condition). | In all groups, emotional eating episodes dropped to zero and weight loss was significant. The VR and IM conditions increased self-efficacy for eating control and depression, whereas the CTRL group showed no change. Three-month follow-up revealed significant improvements in all variables in the VR and IM conditions. When compared to IM, VR resulted in a larger reduction in emotional eating. In the CTRL group, there were no noteworthy changes. |
| HW: HMD | |||||
| [52] | 3 weeks | 3 groups: VR (relaxation protocol enhanced by VR IM (relaxation protocol using imagery) WL | SW: Green Valley (mountain landscape with relaxing lake scenes) | - WL: 5-week hospital-based weight-loss and rehabilitation program. - VR and IM: WL program + 12 individual relaxation training sessions provided traditionally (IM condition) or virtually (VR condition). | The VR and IM treatments improved food management self-efficacy and reduced depression levels. The WL condition did not lead to these changes. During stressful scenarios, the VR and IM conditions both reduced state anxiety, improved a feeling of calmness, and decreased heart rate. There were no differences between VR and IM. All the situations resulted in significant weight loss. |
| HW: - laptop - HMD + (visual and an audio device) - position tracker - joystick | |||||
| [53] | 6 weeks + 6-months follow-up | 3 groups: ExCT CBT NT | SW: VREDIM (Enhanced version of VEBIM) | - NT: 5 weekly nutritional sessions held by dieticians (low calories diet and physical activity). - CBT: NT + 5 weekly group sessions on weight and primary goals + 10 biweekly individual sessions on maintaining weight loss. - ExCT: NT + 5 weekly group sessions on improving motivation to change and assertiveness + 10 biweekly VR sessions. | Each of the three therapy groups lost significantly more weight than those on the waiting list, but there was no difference among groups in terms of weight reduction or the primary psychological characteristics (e.g., anxiety and body satisfaction). In contrast to the other approaches, experiential CT resulted in improvements in body image satisfaction and self-efficacy at the six-month follow-up. ExCT was the only method that was able to significantly improve both BI satisfaction and self-efficacy at the six-month follow-up, thereby implying a decrease in avoidance behaviors and an increase in adaptive behaviors. |
| HW: PC-based workstation graphic card HMD | |||||
| [54] | 6.5 weeks | 2 groups: VR PNI | SW: VREDIM | - VR: 7 VREDIM sessions + low-calorie diet + exercise (walking for 30 min at least twice a week). - PNI: low-calorie diet + exercise + PNI sessions (3/week). | The VREDIM group outperformed PNI in terms of enhancing body satisfaction, self-efficacy, and motivation to change (although the difference was not significant). After therapy, those in the VREDIM group underwent a significant decrease in body dissatisfaction, anxiety, and overeating, as well as a significant gain in self-efficacy. Only the PNI group showed a significant reduction in anxiety and increased exercise. Those in the VREDIM group lost 11.33 kg on average, compared to 7.58 kg in the PNI group. |
| HW: HMD Motion tracker joystick. | |||||
| [55] | 6 months | 3 groups: Obese BED ENDOS | SW: VEBIM 2 (Enhanced version of VEBIM system) | Biweekly 5 individual VR sessions associated with CBT + Diet + biweekly psycho nutritional group sessions + weekly psychological support. | Respondents in all three samples reported lower overall body satisfaction, more realistic limb impressions, higher social activity, and less use of apparel that disguises body obesity. |
| HW: HMD joystick | |||||
| [56] | 6–8 weeks | 2 groups: Obese BED | SW: VEBIM 2 | Biweekly 5 VR sessions associated with CBT + Diet + biweekly psycho-nutritional group sessions. The VE comprises several zones, each of which is employed by the therapist during a patient session. | Body dissatisfaction level was significantly reduced, social activity was improved, and use of disguising clothes was reduced in both groups. |
HW: HMD joystick |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Rasheed, A.; Alabdulkreem, E.; Alduailij, M.; Alduailij, M.; Alhalabi, W.; Alharbi, S.; Lytras, M.D. Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review. Sustainability 2022, 14, 3324. https://doi.org/10.3390/su14063324
Al-Rasheed A, Alabdulkreem E, Alduailij M, Alduailij M, Alhalabi W, Alharbi S, Lytras MD. Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review. Sustainability. 2022; 14(6):3324. https://doi.org/10.3390/su14063324
Chicago/Turabian StyleAl-Rasheed, Amal, Eatedal Alabdulkreem, Mai Alduailij, Mona Alduailij, Wadee Alhalabi, Seham Alharbi, and Miltiadis D. Lytras. 2022. "Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review" Sustainability 14, no. 6: 3324. https://doi.org/10.3390/su14063324
APA StyleAl-Rasheed, A., Alabdulkreem, E., Alduailij, M., Alduailij, M., Alhalabi, W., Alharbi, S., & Lytras, M. D. (2022). Virtual Reality in the Treatment of Patients with Overweight and Obesity: A Systematic Review. Sustainability, 14(6), 3324. https://doi.org/10.3390/su14063324