
Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES

 ,
,  ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Details of Data
2.2. Demographic Characteristics of the Study Population
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics and Comorbidities
3.2. Multivariable Logistic Regression Showing Association between Stroke and Smoking Habits
4. Discussion

{kind=link}
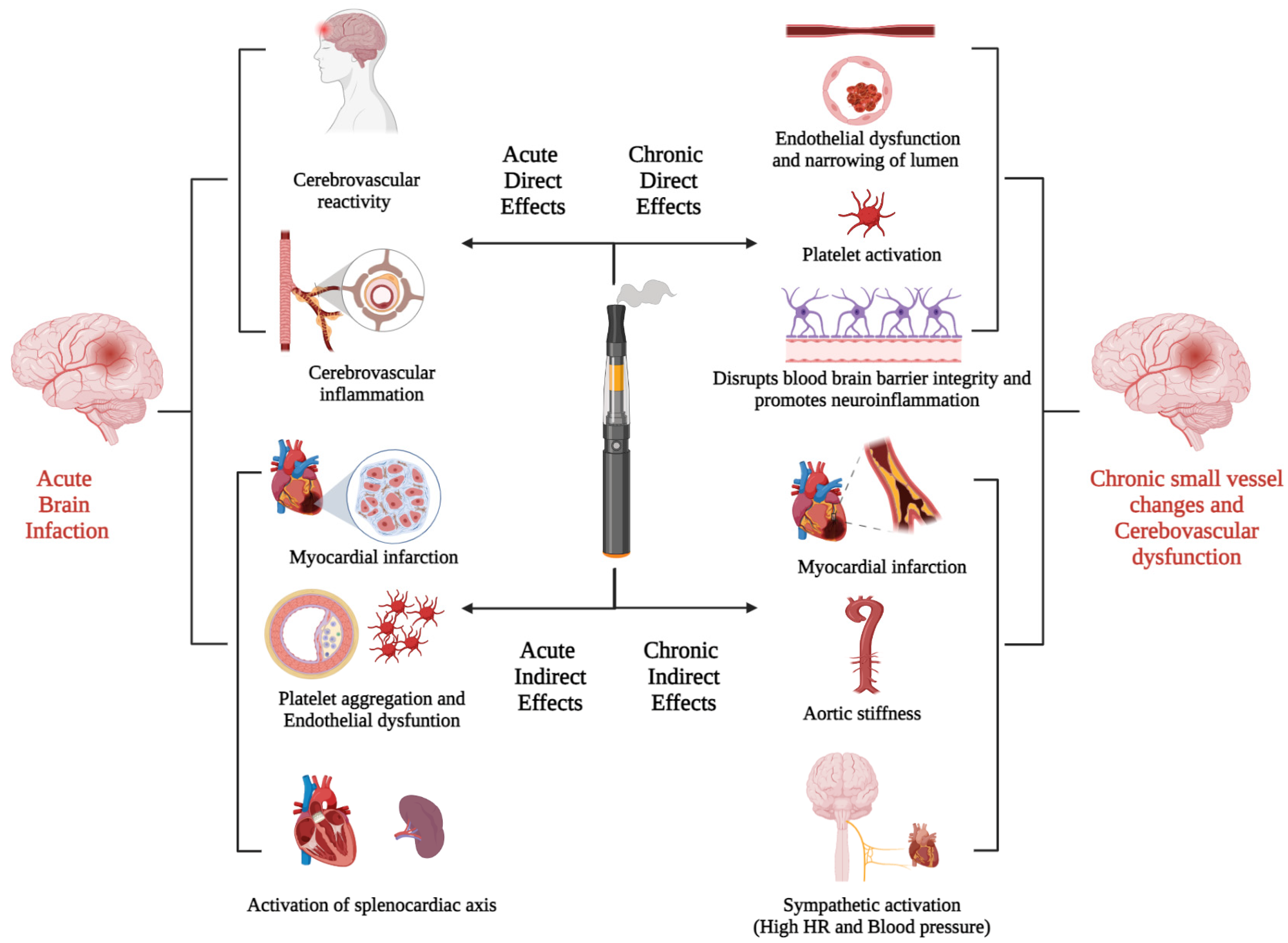
| Acute Direct Effect | |
| Kuntic et al. [35] | E-cigarette product acrolein (reactive aldehydes) mediated NOX-2-driven oxidative stress and cerebrovascular inflammation |
| Caporale et al. [43] | Transient impairment of cerebrovascular reactivity and endothelial function |
| Sifat et al. [8] | Induces a state of glucose deprivation at the neurovascular unit, leading to enhanced ischemic brain injury and/or stroke risk |
| Acute Indirect Effect | |
| Antoniewicz et al., Mitchelle et al. [44,45] | Increased HR; increased arterial stiffness is an independent risk factor for cardio and cerebrovascular events such as myocardial infarctions and stroke |
| Nocella et al. [46] | Increase the soluble CD40L and P-selectin; enhance platelet aggregation |
| Boas et al. [47] | Activation of splenocardiac axis (increase oxidative stress and increase sympathetic activity) |
| Carnevale et al. [40] | Increase oxidative stress and endothelial dysfunction by increasing soluble NOX-mediated peptides and decreasing NO bioavailability and vitamin E |
| Chronic Direct Effect | |
| Kuntic et al. [35] | Endothelial dysfunction and narrowing of vessels |
| Kaisar et al. [25] | Alter blood-brain barrier (BBB) permeability and vascular inflammation |
| Qasim et al. [48] | In mice, alter physiological hemostasis and increase the risk of thrombogenic events; platelet activation |
| Chronic Indirect Effect | |
| Alzahrani et al. [49] | Increased odds of having myocardial infarction (OR = 1.79, 95% CI = 1.20, 2.66, p = 0.004) |
| Moheimani et al. [50] | Increases in cardiac sympathetic activity and oxidative stress, both of which increase the risk of vascular disease |
| Frederik Franzen et al. [51] | Increase peripheral and central blood pressure and pulse wave velocity |
| Vlachopoulos et al. [52] | Increase aortic stiffness and increase blood pressure |
5. Strength and Limitations
6. Future Directions
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Drug Abuse (NIDA). Cigarettes and Other Tobacco Products DrugFacts. Available online: https://www.drugabuse.gov/publications/drugfacts/cigarettes-other-tobacco-products (accessed on 30 August 2021).
- Parekh, T.; Pemmasani, S.; Desai, R. Risk of Stroke With E-Cigarette and Combustible Cigarette Use in Young Adults. Am. J. Prev. Med. 2020, 58, 446–452. [Google Scholar] [CrossRef]
- Heart and Stroke Foundation. Vaping What You Need to Know. Available online: https://www.heartandstroke.ca/articles/vaping-what-you-need-to-know (accessed on 30 August 2021).
- Yatsuya, H.; Folsom, A.R. Risk of Incident Cardiovascular Disease among Users of Smokeless Tobacco in the Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 2010, 172, 600–605. [Google Scholar] [CrossRef]
- Sifat, A.E.; Vaidya, B.; Kaisar, M.A.; Cucullo, L.; Abbruscato, T.J. Nicotine and Electronic Cigarette (E-Cig) Exposure Decreases Brain Glucose Utilization in Ischemic Stroke. J. Neurochem. 2018, 147, 204. [Google Scholar] [CrossRef]
- Bhatnagar, A.; Whitsel, L.P.; Ribisl, K.M.; Bullen, C.; Chaloupka, F.; Piano, M.R.; Robertson, R.M.; McAuley, T.; Goff, D.; Benowitz, N. Electronic Cigarettes: A Policy Statement from the American Heart Association. Circulation 2014, 130, 1418–1436. [Google Scholar] [CrossRef]
- Ndunda, P.M.; Muutu, T.M. Abstract 9: Electronic Cigarette Use Is Associated with a Higher Risk of Stroke. Stroke 2019, 50 (Suppl. 1), A9. [Google Scholar] [CrossRef]
- Qasim, H.; Karim, Z.A.; Rivera, J.O.; Khasawneh, F.T.; Alshbool, F.Z. Impact of Electronic Cigarettes on the Cardiovascular System. J. Am. Heart Assoc. 2017, 6, e006353. [Google Scholar] [CrossRef]
- FDA. 2018 NYTS Data: A Startling Rise in Youth E-Cigarette Use. Available online: https://www.fda.gov/tobacco-products/youth-and-tobacco/2018-nyts-data-startling-rise-youth-e-cigarette-use (accessed on 30 August 2021).
- Euromonitor.com. Growth in Vapour Products. Available online: https://www.euromonitor.com/article/growth-vapour-products (accessed on 30 August 2021).
- Gentzke, A.S.; Creamer, M.; Cullen, K.A.; Ambrose, B.K.; Willis, G.; Jamal, A.; King, B.A. Vital Signs: Tobacco Product Use Among Middle and High School Students—United States, 2011–2018. MMWR. Morb. Mortal. Wkly. Rep. 2019, 68, 157–164. [Google Scholar] [CrossRef]
- Bullen, C.; Howe, C.; Laugesen, M.; McRobbie, H.; Parag, V.; Williman, J.; Walker, N. Electronic Cigarettes for Smoking Cessation: A Randomised Controlled Trial. Lancet 2013, 382, 1629–1637. [Google Scholar] [CrossRef]
- Harrell, P.T.; Simmons, V.N.; Correa, J.; Padhya, T.A.; Brandon, T.H. Electronic Nicotine Delivery Systems (“e-Cigarettes”): Review of Safety and Smoking Cessation Efficacy. Otolaryngol. Head Neck Surg. 2014, 151, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Spyrou, A.; Tsimopoulou, K.; Stefopoulos, C.; Romagna, G.; Voudris, V. Nicotine Absorption from Electronic Cigarette Use: Comparison between First and New-Generation Devices. Sci. Rep. 2014, 4, 4133. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.; Filippidis, F.T.; Agaku, I.T. Determinants and Prevalence of E-Cigarette Use throughout the European Union: A Secondary Analysis of 26 566 Youth and Adults from 27 Countries. Tob. Control 2015, 24, 442–448. [Google Scholar] [CrossRef]
- Lee, S.; Grana, R.A.; Glantz, S.A. Electronic Cigarette Use among Korean Adolescents: A Cross-Sectional Study of Market Penetration, Dual Use, and Relationship to Quit Attempts and Former Smoking. J. Adolesc. Health 2014, 54, 684–690. [Google Scholar] [CrossRef]
- Lee, H.-W.; Park, S.-H.; Weng, M.; Wang, H.-T.; Huang, W.C.; Lepor, H.; Wu, X.-R.; Chen, L.-C.; Tang, M. E-Cigarette Smoke Damages DNA and Reduces Repair Activity in Mouse Lung, Heart, and Bladder as Well as in Human Lung and Bladder Cells. Proc. Natl. Acad. Sci. USA 2018, 115, E1560–E1569. [Google Scholar] [CrossRef]
- Hutzler, C.; Paschke, M.; Kruschinski, S.; Henkler, F.; Hahn, J.; Luch, A. Chemical Hazards Present in Liquids and Vapors of Electronic Cigarettes. Arch. Toxicol. 2014, 88, 1295–1308. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of Selected Carcinogens and Toxicants in Vapour from Electronic Cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef]
- Palmisani, J.; Abenavoli, C.; Famele, M.; Gilio, A.D.; Palmieri, L.; Gennaro, G.d.; Draisci, R. Chemical Characterization of Electronic Cigarette (e-Cigs) Refill Liquids Prior to EU Tobacco Product Directive Adoption: Evaluation of BTEX Contamination by HS-SPME-GC-MS and Identification of Flavoring Additives by GC-MS-O. Atmosphere 2020, 11, 374. [Google Scholar] [CrossRef]
- Bradford, S.; Stamatovic, S.M.; Dondeti, R.S.; Keep, R.; Andjelkovic, A.V. Nicotine Aggravates the Brain Postischemic Inflammatory Response. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1518–H1529. [Google Scholar] [CrossRef]
- Kaisar, M.A.; Villalba, H.; Prasad, S.; Liles, T.; Sifat, A.E.; Sajja, R.K.; Abbruscato, T.J.; Cucullo, L. Offsetting the Impact of Smoking and E-Cigarette Vaping on the Cerebrovascular System and Stroke Injury: Is Metformin a Viable Countermeasure? Redox Biol. 2017, 13, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.M.; Hazari, M.S.; Ledbetter, A.D.; Haykal-Coates, N.; Carll, A.P.; Cascio, W.E.; Winsett, D.W.; Costa, D.L.; Farraj, A.K. Acrolein Inhalation Alters Arterial Blood Gases and Triggers Carotid Body-Mediated Cardiovascular Responses in Hypertensive Rats. Inhal. Toxicol. 2015, 27, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Hazari, M.S.; Haykal-Coates, N.; Winsett, D.W.; Krantz, Q.T.; King, C.; Costa, D.L.; Farraj, A.K. TRPA1 and Sympathetic Activation Contribute to Increased Risk of Triggered Cardiac Arrhythmias in Hypertensive Rats Exposed to Diesel Exhaust. Environ. Health Perspect. 2011, 119, 951. [Google Scholar] [CrossRef] [PubMed]
- Wheat, L.A.; Haberzettl, P.; Hellmann, J.; Baba, S.P.; Bertke, M.; Lee, J.; McCracken, J.; O’Toole, T.E.; Bhatnagar, A.; Conklin, D.J. Acrolein Inhalation Prevents Vascular Endothelial Growth Factor-Induced Mobilization of Flk-1+/Sca-1+ Cells in Mice. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1598–1606. [Google Scholar] [CrossRef]
- Sithu, S.D.; Srivastava, S.; Siddiqui, M.A.; Vladykovskaya, E.; Riggs, D.; Conklin, D.J.; Haberzettl, P.; O’Toole, T.E.; Bhatnagar, A.; D’Souza, S.E. Exposure to Acrolein by Inhalation Causes Platelet Activation. Toxicol. Appl. Pharmacol. 2010, 248, 100–110. [Google Scholar] [CrossRef]
- Peters, A.; Dockery, D.W.; Muller, J.E.; Mittleman, M.A. Increased Particulate Air Pollution and the Triggering of Myocardial Infarction. Circulation 2001, 103, 2810–2815. [Google Scholar] [CrossRef]
- Sullivan, J.; Sheppard, L.; Schreuder, A.; Ishikawa, N.; Siscovick, D.; Kaufman, J. Relation between Short-Term Fine-Particulate Matter Exposure and Onset of Myocardial Infarction. Epidemiology 2005, 16, 41–48. [Google Scholar] [CrossRef]
- Wang, T.; Lang, G.D.; Moreno-Vinasco, L.; Huang, Y.; Goonewardena, S.N.; Peng, Y.J.; Svensson, E.C.; Natarajan, V.; Lang, R.M.; Linares, J.D.; et al. Particulate Matter Induces Cardiac Arrhythmias via Dysregulation of Carotid Body Sensitivity and Cardiac Sodium Channels. Am. J. Respir. Cell Mol. Biol. 2012, 46, 524–531. [Google Scholar] [CrossRef]
- Conklin, D.J.; Barski, O.A.; Lesgards, J.-F.; Juvan, P.; Rezen, T.; Rozman, D.; Prough, R.A.; Vladykovskaya, E.; Liu, S.; Srivastava, S.; et al. Acrolein Consumption Induces Systemic Dyslipidemia and Lipoprotein Modification. Toxicol. Appl. Pharmacol. 2009, 243, 1–12. [Google Scholar] [CrossRef]
- Srivastava, S.; Sithu, S.D.; Vladykovskaya, E.; Haberzettl, P.; Hoetker, D.J.; Siddiqui, M.A.; Conklin, D.J.; D’Souza, S.E.; Bhatnagar, A. Oral exposure to acrolein exacerbates atherosclerosis in apoE-null mice. Atherosclerosis 2011, 215, 301–308. [Google Scholar] [CrossRef]
- Kuntic, M.; Oelze, M.; Steven, S.; Kröller-Schön, S.; Stamm, P.; Kalinovic, S.; Frenis, K.; Vujacic-Mirski, K.; Bayo Jimenez, M.T.; Kvandova, M.; et al. Short-Term e-Cigarette Vapour Exposure Causes Vascular Oxidative Stress and Dysfunction: Evidence for a Close Connection to Brain Damage and a Key Role of the Phagocytic NADPH Oxidase (NOX-2). Eur. Heart J. 2020, 41, 2472–2483. [Google Scholar] [CrossRef] [PubMed]
- Vansickel, A.R.; Eissenberg, T. Electronic Cigarettes: Effective Nicotine Delivery After Acute Administration. Nicotine Tob. Res. 2013, 15, 267. [Google Scholar] [CrossRef]
- Nides, M.A.; Leischow, S.J.; Bhatter, M.; Simmons, M. Nicotine Blood Levels and Short-Term Smoking Reduction with an Electronic Nicotine Delivery System. Am. J. Health Behav. 2014, 38, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.S.; D’Ruiz, C. Effects of Using Electronic Cigarettes on Nicotine Delivery and Cardiovascular Function in Comparison with Regular Cigarettes. Regul. Toxicol. Pharmacol. 2015, 71, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Vlachopoulos, C.; Ioakeimidis, N.; Abdelrasoul, M.; Terentes-Printzios, D.; Georgakopoulos, C.; Pietri, P.; Stefanadis, C.; Tousoulis, D. Electronic Cigarette Smoking Increases Aortic Stiffness and Blood Pressure in Young Smokers. J. Am. Coll. Cardiol. 2016, 67, 2802–2803. [Google Scholar] [CrossRef] [PubMed]
- Carnevale, R.; Sciarretta, S.; Violi, F.; Nocella, C.; Loffredo, L.; Perri, L.; Peruzzi, M.; Marullo, A.G.; De Falco, E.; Chimenti, I.; et al. Acute Impact of Tobacco vs Electronic Cigarette Smoking on Oxidative Stress and Vascular Function. Chest 2016, 150, 606–612. [Google Scholar] [CrossRef]
- Antoniewicz, L.; Bosson, J.A.; Kuhl, J.; Abdel-Halim, S.M.; Kiessling, A.; Mobarrez, F.; Lundbäck, M. Electronic Cigarettes Increase Endothelial Progenitor Cells in the Blood of Healthy Volunteers. Atherosclerosis 2016, 255, 179–185. [Google Scholar] [CrossRef]
- Hom, S.; Chen, L.; Wang, T.; Ghebrehiwet, B.; Yin, W.; Rubenstein, D.A. Platelet Activation, Adhesion, Inflammation, and Aggregation Potential Are Altered in the Presence of Electronic Cigarette Extracts of Variable Nicotine Concentrations. Platelets 2016, 27, 694–702. [Google Scholar] [CrossRef]
- Caporale, A.; Langham, M.C.; Guo, W.; Johncola, A.; Chatterjee, S.; Wehrli, F.W. Acute Effects of Electronic Cigarette Aerosol Inhalation on Vascular Function Detected at Quantitative MRI. Radiology 2019, 293, 97–106. [Google Scholar] [CrossRef]
- Antoniewicz, L.; Brynedal, A.; Hedman, L.; Lundbäck, M.; Bosson, J.A. Acute Effects of Electronic Cigarette Inhalation on the Vasculature and the Conducting Airways. Cardiovasc. Toxicol. 2019, 19, 441–450. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Nocella, C.; Biondi-Zoccai, G.; Sciarretta, S.; Peruzzi, M.; Pagano, F.; Loffredo, L.; Pignatelli, P.; Bullen, C.; Frati, G.; Carnevale, R. Impact of Tobacco Versus Electronic Cigarette Smoking on Platelet Function. Am. J. Cardiol. 2018, 122, 1477–1481. [Google Scholar] [CrossRef]
- Boas, Z.; Gupta, P.; Moheimani, R.S.; Bhetraratana, M.; Yin, F.; Peters, K.M.; Gornbein, J.; Araujo, J.A.; Czernin, J.; Middlekauff, H.R. Activation of the “Splenocardiac Axis” by Electronic and Tobacco Cigarettes in Otherwise Healthy Young Adults. Physiol. Rep. 2017, 5, e13393. [Google Scholar] [CrossRef] [PubMed]
- Qasim, H.; Karim, Z.A.; Silva-Espinoza, J.C.; Khasawneh, F.T.; Rivera, J.O.; Ellis, C.C.; Bauer, S.L.; Almeida, I.C.; Alshbool, F.Z. Short-Term E-Cigarette Exposure Increases the Risk of Thrombogenesis and Enhances Platelet Function in Mice. J. Am. Heart Assoc. 2018, 7, e009264. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, T.; Pena, I.; Temesgen, N.; Glantz, S.A. Association between Electronic Cigarette Use and Myocardial Infarction. Am. J. Prev. Med. 2018, 55, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Moheimani, R.S.; Bhetraratana, M.; Yin, F.; Peters, K.M.; Gornbein, J.; Araujo, J.A.; Middlekauff, H.R. Increased Cardiac Sympathetic Activity and Oxidative Stress in Habitual Electronic Cigarette Users: Implications for Cardiovascular Risk. JAMA Cardiol. 2017, 2, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Franzen, K.F.; Willig, J.; Talavera, S.C.; Meusel, M.; Sayk, F.; Reppel, M.; Dalhoff, K.; Mortensen, K.; Droemann, D. E-Cigarettes and Cigarettes Worsen Peripheral and Central Hemodynamics as Well as Arterial Stiffness: A Randomized, Double-Blinded Pilot Study. Vasc. Med. 2018, 23, 419–425. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Kosmopoulou, F.; Panagiotakos, D.; Ioakeimidis, N.; Alexopoulos, N.; Pitsavos, C.; Stefanadis, C. Smoking and Caffeine Have a Synergistic Detrimental Effect on Aortic Stiffness and Wave Reflections. J. Am. Coll. Cardiol. 2004, 44, 1911–1917. [Google Scholar] [CrossRef][Green Version]
- Besaratinia, A.; Tommasi, S. Vaping: A Growing Global Health Concern. EClinicalMedicine 2019, 17, 100208. [Google Scholar] [CrossRef]
- George, J.; Hussain, M.; Vadiveloo, T.; Ireland, S.; Hopkinson, P.; Struthers, A.D.; Donnan, P.T.; Khan, F.; Lang, C.C. Cardiovascular Effects of Switching from Tobacco Cigarettes to Electronic Cigarettes. J. Am. Coll. Cardiol. 2019, 74, 3112. [Google Scholar] [CrossRef]

| E-Cigarette Smokers n = 7756 (9.72%) | Dual E-Cigarette + Traditional Smokers n = 23,444 (29.37) | Traditional Smokers n = 48,625 (60.91%) | Total n = 79,825 (100) | p Values | |
|---|---|---|---|---|---|
| Stroke (n) (Prevalence %) (Column % comparison between different smoking habits) | 66 (1.57) (1.09) | 855 (20.39) (3.72) | 3273 (78.04) (6.75) | 4194 (100) (5.41) | <0.0001 |
| Age of onset of stroke in years (Median + IQR) | 48 (42–58) | 50 (40–58) | 59 (50–69) | <0.0001 |
| E-Cigarette Smokers with History of Stroke n = 66 (1.57%) | Dual E-Cigarette + Traditional Smokers with History of Stroke n = 855 (20.39%) | Traditional Smokers with History of Stroke n = 3273 (78.04%) | Total n = 4194 (100) | p Value | |
|---|---|---|---|---|---|
| Age in years at screening (Median + IQR) | 50 (45–63) | 55 (47–64) | 69 (62–80) | <0.0001 | |
| Sex (%) | <0.0001 | ||||
| Female | 36.36 | 51.93 | 33.91 | 37.63 | |
| Male | 63.64 | 48.07 | 66.09 | 62.37 | |
| Race (%) | <0.0001 | ||||
| Mexican-American | 21.21 | 11.58 | 6.02 | 7.39 | |
| Other Hispanic | 24.24 | 5.15 | 7.70 | 7.44 | |
| Non-Hispanic White | 37.88 | 47.13 | 42.77 | 43.59 | |
| Non-Hispanic Black | 0.00 | 24.09 | 31.29 | 29.33 | |
| Non-Hispanic Asian | 0.00 | 0.00 | 3.79 | 2.96 | |
| Other Race—Including Multi-Racial | 16.67 | 12.05 | 8.43 | 9.30 | |
| Annual Household Income (%) | <0.0001 | ||||
| $0–$25,000 | 57.58 | 59.15 | 50.67 | 52.44 | |
| $25,000–$65,000 | 16.67 | 32.18 | 32.49 | 32.16 | |
| $65,000–$100,000 | 25.76 | 4.27 | 7.99 | 7.57 | |
| >$100,000 | 0.00 | 4.41 | 8.85 | 7.83 | |
| Comorbidities (%) | |||||
| Coronary Heart Disease (%) | 25.76 | 15.32 | 27.62 | 25.08 | <0.0001 |
| Congestive Heart Failure (%) | 25.76 | 21.75 | 16.59 | 17.79 | <0.0001 |
| High Blood Pressure—2+ Times (%) | 60.98 | 98.02 | 80.91 | 84.11 | <0.0001 |
| Recent Systolic Blood Pressure in mmHg (Median) * | 118 | 120 | 134 | <0.0001 | |
| Recent Diastolic Blood Pressure in mmHg (Median) * | 70 | 80 | 80 | <0.0001 | |
| Taking Prescribed Medicine For HBP (%) | 100.00 | 81.66 | 89.33 | 87.89 | <0.0001 |
| High Cholesterol Level (%) | 25.76 | 60.58 | 58.11 | 58.11 | <0.0001 |
| Taking Prescribed Medicine High Cholesterol (%) | 100.00 | 82.52 | 84.39 | 81.83 | 0.2876 |
| LDL-Cholesterol, NIH Equation 2 (mg/dL) (Median) * | 112 | 101 | 110 | <0.0001 | |
| Diabetes (%) | 50.00 | 19.06 | 36.63 | 33.26 | <0.0001 |
| Last Hb A1C Level (Median) * | 5.7 | 7.2 | 7.9 | <0.0001 | |
| Feeling Down, Depressed, Or Hopeless (%) | <0.0001 | ||||
| Several Days | 12.12 | 17.56 | 18.24 | 17.99 | |
| More Than Half The Days | 0.00 | 13.59 | 8.91 | 9.73 | |
| Nearly Every Day | 21.21 | 19.87 | 7.46 | 10.29 | |
| Liver Disorders (%) | 21.21 | 6.43 | 9.84 | 9.32 | <0.0001 |
| Cancer Or Malignancy (%) | 25.76 | 17.19 | 24.35 | 22.91 | <0.0001 |
| Alcohol use disorder—Heavy drinking (%) † | 30.91 | 41.97 | 61.24 | 56.03 | <0.0001 |
| Marijuana or Hashish (%) | 100.00 | 92.15 | 66.20 | 78.61 | <0.0001 |
| Cocaine/Heroin/Methamphetamin (%) | 71.21 | 38.85 | 31.64 | 34.93 | <0.0001 |
| Inject Illegal Drug (%) | 21.21 | 1.77 | 4.63 | 4.63 | <0.0001 |
| Variable | Multivariable Analysis * Odds Ratio (95% Confidence Interval); p Value | c-Value (Area under ROC) |
|---|---|---|
| Possibility of having history of stroke = 1 | ||
| Non-smokers | Reference | |
| E-cigarette smokers vs. Traditional smokers | 1.15 (1.15–1.16); p < 0.0001 | 0.733 |
| Dual smokers vs. Traditional smokers | 1.14 (1.14–1.15); p < 0.0001 | |
| E-cigarette smoking in last 30-days vs. no-E-cigarette smoking in last 30-days | 1.60 (1.60–1.61); p < 0.0001 | 0.894 |
| Component Potentially Involved | Effect [11,26,27,28,29,30,31,32,33,34] |
|---|---|
| Acrolein, PMs, nicotine | Increased blood pressure |
| Acrolein | Myocardial dysfunction and cardiomyopathy, impaired vascular repair, and vascular injury |
| Acrolein, PMs | Reduced cardiac contractility, Increased risk of thrombosis, increased risk of ventricular arrhythmias |
| PMs, nicotine | Coronary artery disease and myocardial infarction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, U.; Patel, N.; Khurana, M.; Parulekar, A.; Patel, A.; Ortiz, J.F.; Patel, R.; Urhoghide, E.; Mistry, A.; Bhriguvanshi, A.; et al. Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES. Neurol. Int. 2022, 14, 441-452. https://doi.org/10.3390/neurolint14020037
Patel U, Patel N, Khurana M, Parulekar A, Patel A, Ortiz JF, Patel R, Urhoghide E, Mistry A, Bhriguvanshi A, et al. Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES. Neurology International. 2022; 14(2):441-452. https://doi.org/10.3390/neurolint14020037
Chicago/Turabian StylePatel, Urvish, Neel Patel, Mahika Khurana, Akshada Parulekar, Amrapali Patel, Juan Fernando Ortiz, Rutul Patel, Eseosa Urhoghide, Anuja Mistry, Arpita Bhriguvanshi, and et al. 2022. "Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES" Neurology International 14, no. 2: 441-452. https://doi.org/10.3390/neurolint14020037
APA StylePatel, U., Patel, N., Khurana, M., Parulekar, A., Patel, A., Ortiz, J. F., Patel, R., Urhoghide, E., Mistry, A., Bhriguvanshi, A., Abdulqader, M., Mehta, N., Arumaithurai, K., & Shah, S. (2022). Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES. Neurology International, 14(2), 441-452. https://doi.org/10.3390/neurolint14020037