
PAGE-B and REACH-B Predicts the Risk of Developing Hepatocellular Carcinoma in Chronic Hepatitis B Patients from Northeast, Brazil

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Study Population
2.3. Sample
2.4. Definitions
2.4.1. Stages of Chronic HBV Infection
- Chronic HBeAg positive HBV infection (immunotolerant): presence of HBeAg, high levels of HBVDNA (>107 IU/mL) and ALT persistently within normal reference values (approximately 40 IU/mL). Histology with minimal or no necroinflammatory activity or fibrosis;
- Chronic hepatitis B HBeAg positive (immunoactive): presence of HBeAg, elevated HBVDNA (104–107 IU/mL) and ALT above the normal reference value. Histology with moderate or intense necroinflammatory activity and fibrosis;
- Chronic HBeAg negative HBV infection (inactive carrier): presence of anti-HBe antibody, undetectable or low HBVDNA (<2000 IU/mL), and normal ALT. Histology with minimal necroinflammatory activity;
- Chronic hepatitis B HBeAg negative (reactivation): absence of HBeAg, usually with the presence of antiHBe, high levels of HBVDNA (>2000 IU/mL) and ALT above the normal reference value (persistently or intermittently). Histology with moderate or intense necroinflammatory activity and fibrosis.
2.4.2. Liver Cirrhosis
2.4.3. Diagnosis of Hepatocellular Carcinoma
2.4.4. Criteria for the Treatment of Chronic Hepatitis B
2.5. Data Collection
2.6. Follow-Up
2.7. PAGE-B and REACH-B Scores
2.8. Statistical Analysis
- (I)
- ensitivity (c, t): Pr {Mi > c | δi (t) =} = Pr {Mi > c | Ti = t}
- (II)
- specificity (c, 𝑡): Pr {Mi ≤ c | δi (t) =} = Pr {Mi ≤ c | Ti > t}
- M = continuous marker
- c = truncation
- t = instant of time
- δ(t) = II(T ≤ C): failure or censoring event indicator, considering C the censoring time and T the survival time.
2.9. Ethical Aspects
3. Results
3.1. Epidemiological and Clinical Characteristics
3.2. Prevalence of HCC and Univariate Analysis of Risk Factors
3.3. Risk Scores for HCC
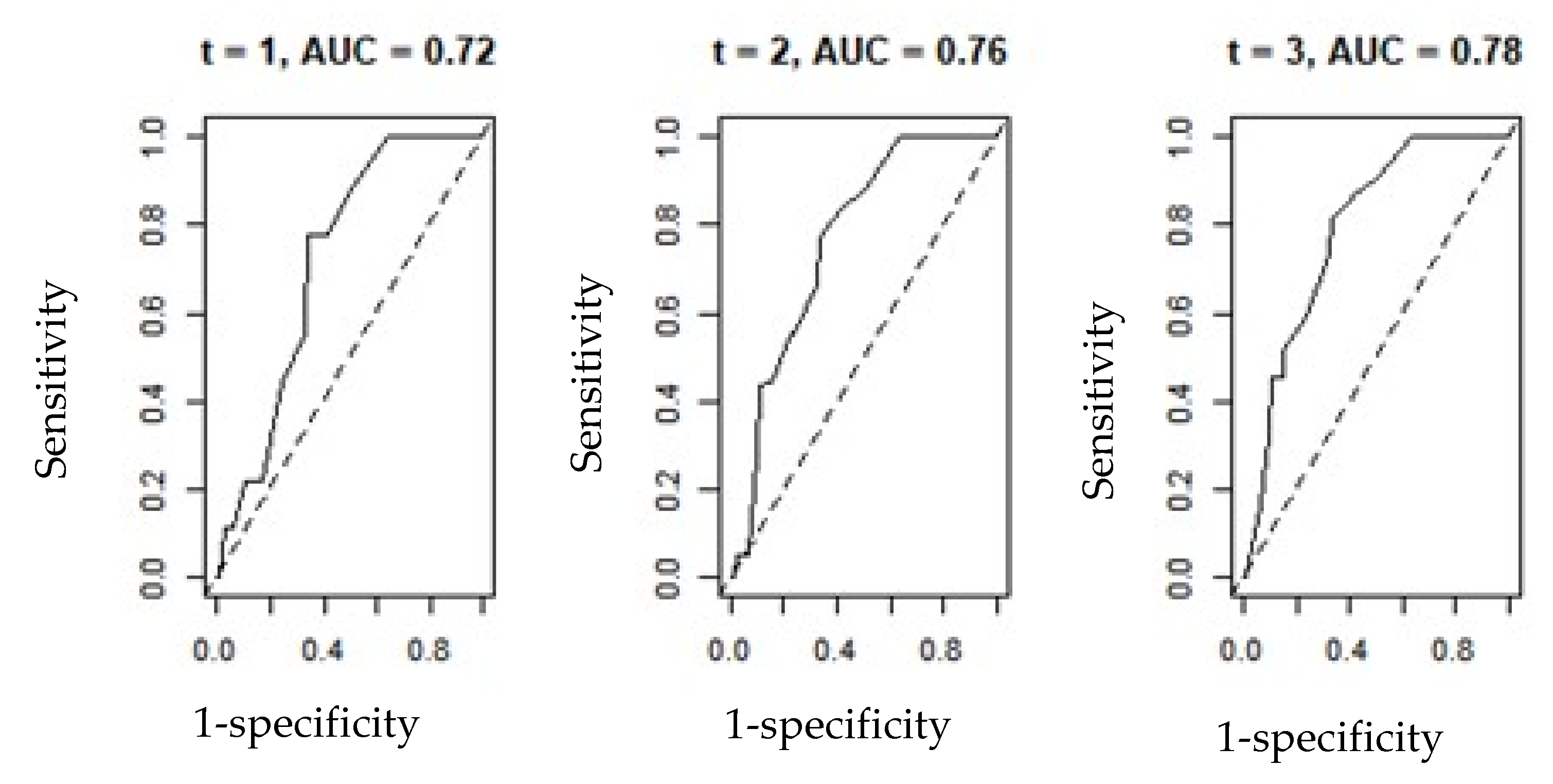
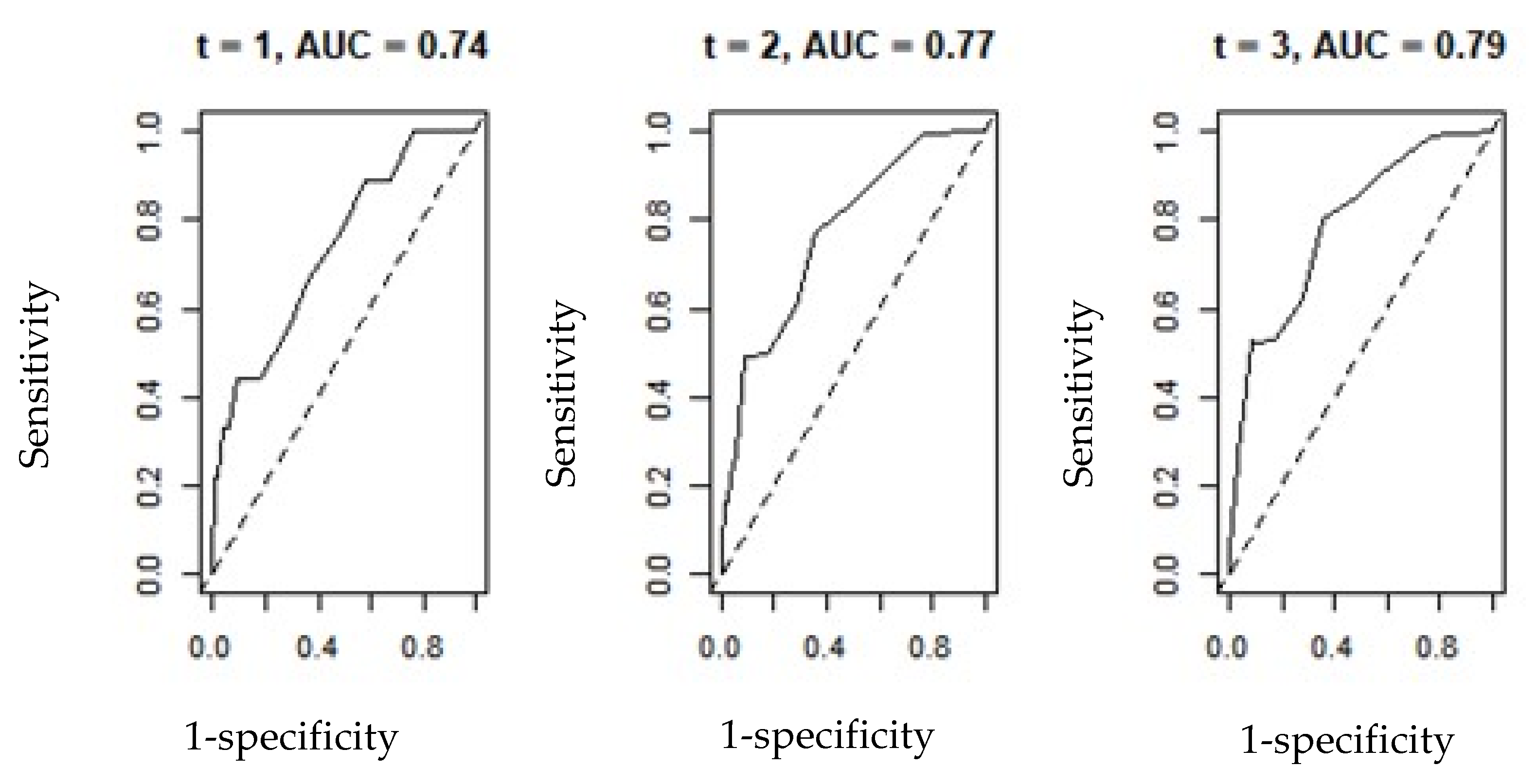
3.4. Application of the Time-Dependent ROC Curve Technique—ROC (t)
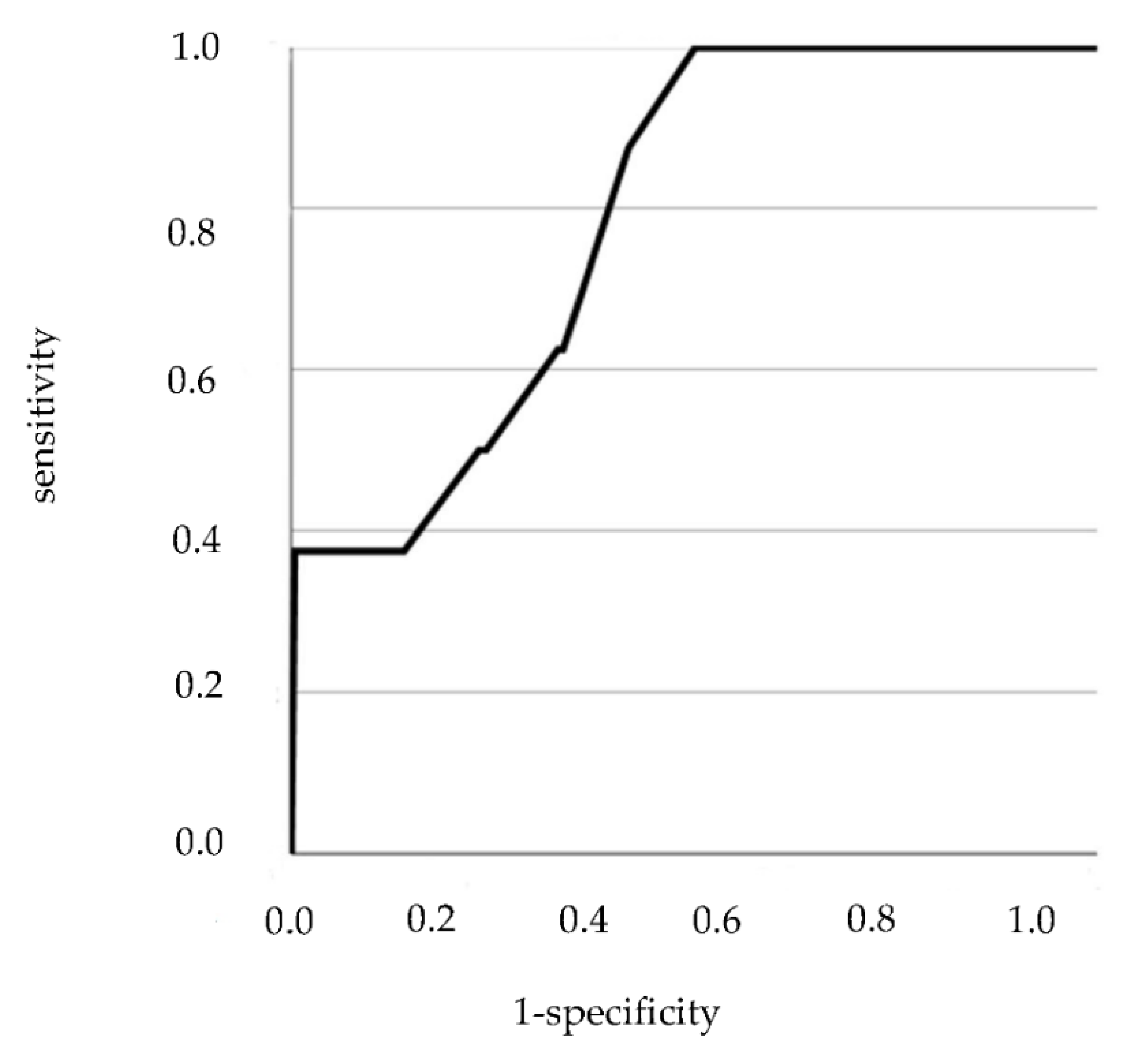
3.5. PAGE-B and REACH-B ROC Curve
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fattovich, G.; Bortolotti, F.; Donato, F. Natural history of chronic hepatitis B: Special emphasis on disease progression and prognostic factors. J. Hepatol. 2008, 48, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update 2009. Hepatology 2009, 50, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.L.; Wong, V.W. Risk prediction of hepatitis B virus-related hepatocellular carcinoma in the era of antiviral therapy. World J. Gastroenterol. 2013, 19, 6515–6522. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Yu, M.W.; Liaw, Y.F. Epidemiological characteristics and risk factors of hepatocellular carcinoma. J. Gastroenterol. Hepatol. 1997, 12, S294–S308. [Google Scholar] [CrossRef]
- Yang, H.I.; Yuen, M.F.; Chan, H.L.; Han, K.H.; Chen, P.J.; Kim, D.Y.; Ahn, S.H.; Chen, C.J.; Wong, V.W.; Seto, W.K. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B): Development and validation of a predictive score. Lancet Oncol. 2011, 12, 568–574. [Google Scholar] [CrossRef]
- Wong, V.W.; Janssen, H.L. Can we use HCC risk scores to individualize surveillance in chronic hepatitis B infection? J. Hepatol. 2015, 63, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.I.; Lu, S.N.; Liaw, Y.F.; You, S.L.; Sun, C.A.; Wang, L.Y.; Hsiao, C.K.; Chen, P.J.; Chen, D.S.; Chen, C.J. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N. Engl. J. Med. 2002, 347, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.J.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Lu, S.N.; Huang, G.T.; Iloeje, U.H. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA 2006, 295, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Andreani, T.; Serfaty, L.; Mohand, D.; Dernaika, S.; Wendum, D.; Chazouillères, O.; Poupon, R. Chronic hepatitis B virus carriers in the immunotolerant phase of infection: Histologic findings and outcome. Clin. Gastroenterol. Hepatol. 2007, 5, 636–641. [Google Scholar] [CrossRef]
- Wong, V.W.; Sung, J.J. Diagnosis and personalized management of hepatitis B including significance of genotypes. Curr. Opin. Infect. Dis. 2012, 25, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.H.; Chen, P.J.; Lai, M.Y.; Chen, D.S. Basal core promoter mutations of hepatitis B virus increase the risk of hepatocellular carcinoma in hepatitis B carriers. Gastroenterology 2003, 124, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Thompson, A.; Martinot-Peignoux, M.; Piratvisuth, T.; Cornberg, M.; Brunetto, M.R.; Tillmann, H.L.; Kao, J.H.; Jia, J.D.; Wedemeyer, H.; et al. Hepatitis B surface antigen quantification: Why and how to use it in 2011—A core group report. J. Hepatol. 2011, 55, 1121–1131. [Google Scholar] [CrossRef] [PubMed]
- Yuen, M.F.; Tanaka, Y.; Fong, D.Y.; Fung, J.; Wong, D.K.; Yuen, J.C.; But, D.Y.; Chan, A.O.; Wong, B.C.; Mizokami, M.; et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. J. Hepatol. 2009, 50, 80–88. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Yiu, K.K.; Lai, J.W.; Chan, V.K.; Cheung, K.K.; Wong, E.W.; Wong, V.W. Meta-analysis: The association of hepatitis B virus genotypes and hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2013, 37, 517–526. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.L.; Tse, C.H.; Mo, F.; Koh, J.; Wong, V.W.; Wong, G.L.; Chan, L.S.; Yeo, W.; Sung, J.J.; Mok, T.S. High viral load and hepatitis B virus subgenotype ce are associated with increased risk of hepatocellular carcinoma. J. Clin. Oncol. 2008, 26, 177–182. [Google Scholar] [CrossRef]
- Tseng, T.C.; Liu, C.J.; Yang, H.C.; Su, T.H.; Wang, C.C.; Chen, C.L.; Kuo, S.F.; Liu, C.H.; Chen, P.J.; Chen, D.S.; et al. High levels of hepatitis B surface antigen increase risk of hepatocellular carcinoma in patients with low HBV load. Gastroenterology 2012, 142, 1140–1149.e3. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.-I.; Sherman, S.J.; Su, J.; Chen, P.-J.; Liaw, Y.-F.; Iloeje, U.H.; Chen, C.J. Nomograms for risk of hepatocellular carcinoma in patients with chronic hepatitis B virus infection. J. Clin. Oncol. 2010, 28, 2437–2444. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Chan, S.L.; Mo, F.; Chan, T.-C.; Loong, H.H.-F.; Wong, G.L.-H.; Liu, Y.Y.-N.; Chan, A.T.-C.; Sung, J.J.-Y.; Yeo, W.; et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J. Clin. Oncol. 2010, 28, 1660–1665. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.L.-H.; Chan, H.L.-Y.; Wong, C.K.-Y.; Leung, C.; Chan, C.Y.; Ho, P.P.-L.; Chung, V.C.-Y.; Chan, Z.C.-Y.; Tse, Y.-K.; Chim, A.M.-L.; et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B. J. Hepatol. 2014, 60, 339–345. [Google Scholar] [CrossRef]
- Lee, H.W.; Yoo, E.J.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.-H. Prediction of development of liver-related events by transient elastography in hepatitis B patients with complete virological response on antiviral therapy. Am. J. Gastroenterol. 2014, 109, 1241–1249. [Google Scholar] [CrossRef]
- Papatheodoridis, G.; Dalekos, G.; Sypsa, V.; Yurdaydin, C.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; Mangia, C.; et al. PAGE-B: A risk score for hepatocellular carcinoma in Caucasians with chronic hepatitis B under a 5-year entecavir or tenofovir therapy. J. Hepatol. 2016, 64, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Poh, Z.; Shen, L.; Yang, H.-I.; Seto, W.-K.; Wong, V.W.; Lin, C.Y.; Goh, B.-B.G.; Chang, P.-E.J.; Chan, H.L.-Y.; Yuen, M.-F.; et al. Real-world risk score for hepatocellular carcinoma (RWS-HCC): A clinically practical risk predictor for HCC in chronic hepatitis B. Gut 2016, 65, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, Y.D.; Lee, M.; Jun, B.; Kim, T.S.; Suk, K.T.; Kang, S.H.; Kim, M.Y.; Cheon, G.J.; Kim, D.J.; et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J. Hepatol. 2018, 69, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.-C.; Yip, T.C.-F.; Ho, H.J.; Wong, V.W.-S.; Huang, Y.-T.; El-Serag, H.B.; Lee, T.-Y.; Wu, M.-S.; Lin, J.-T.; Wong, G.L.-H.; et al. Development of a scoring system to predict hepatocellular carcinoma in Asians on antivirals for chronic hepatitis B. J. Hepatol. 2018, 69, 278–285. [Google Scholar] [CrossRef]
- Yu, J.H.; Suh, Y.J.; Jin, Y.-J.; Heo, N.-Y.; Jang, J.W.; You, C.R.; An, H.Y.; Lee, J.-W. Prediction model for hepatocellular carcinoma risk in treatment-naive chronic hepatitis B patients receiving entecavir/tenofovir. Eur. J. Gastroenterol. Hepatol. 2019, 31, 865–872. [Google Scholar] [CrossRef]
- Yang, H.-I.; Yeh, M.-L.; Wong, G.L.-H.; Peng, C.-Y.; Chen, C.-H.; Trinh, H.N.; Cheung, K.-S.; Xie, Q.; Su, T.-H.; Kozuka, R.; et al. Real-world effectiveness from the Asia Pacific Rim liver consortium for HBV risk score for the prediction of hepatocellular carcinoma in chronic hepatitis B patients treated with oral antiviral therapy. J. Infect. Dis. 2020, 221, 389–399. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.P.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.-S.; Chen, H.L.; Chien, R.N.; Dokmeci, A.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Kim, G.-A.; Lee, H.C.; Kim, M.-J.; Ha, Y.; Park, E.J.; An, J.; Lee, D.; Shim, J.H.; Kim, K.M.; Lim, Y.-S. Incidence of hepatocellular carcinoma after HBsAg seroclearance in chronic hepatitis B patients: A need for surveillance. J. Hepatol. 2015, 62, 1092–1099. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Brasil, Ministério da Saúde. Portaria no 43, de 9 de Dezembro de 2016. Torna Pública a Decisão de Atualizar o Protocolo Clínico e Diretrizes Terapêuticas para Hepatite B e Coinfecções, no Ambito do Sistema Único de Saúde—SUS [Internet]. Diário Oficial da União, Brasília (DF), 2016 dez 9 [citado 2019 dez 16]; Seção 1:121. Available online: http://conitec.gov.br/images/Re-latorios/Portaria/2016/Portaria_SCTIE_47_2016.pdf (accessed on 16 January 2022).
- Heagerty, J.P.; Zheng, Y. Survival Model Predictive Accuracy and ROC Curves. Biometrics 2005, 61, 92–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- El-Serag, H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costentin, C.E.; Layese, R.; Bourcier, V.; Cagnot, C.; Marcellin, P.; Guyader, D.; Pol, S.; Larrey, D.; De Lédinghen, V.; Ouzan, D.; et al. Compliance with hepatocellular carcinoma surveillance guidelines associated with increased Lead-time adjusted survival of patients with compensated viral cirrhosis: A multi-center cohort study. Gastroenterology 2018, 155, 431–442.e410. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Protzer, U.; Petersen, J.; Wedemeyer, H.; Berg, T.; Jilg, W.; Erhardt, A.; Wirth, S.; Sarrazin, C.; Dollinger, M.M.; et al. Prophylaxis, diagnosis and therapy of hepatitis B virus infection—The German guideline. Z. Gastroenterol. 2011, 49, 871–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liaw, Y.-F.; Sung, J.J.Y.; Chow, W.C.; Farrell, G.; Lee, C.-Z.; Yuen, H.; Tanwandee, T.; Tao, Q.-M.; Shue, K.; Keene, O.; et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N. Engl. J. Med. 2004, 351, 1521–1531. [Google Scholar] [CrossRef]
- Riveiro-Barciela, M.; Tabernero, D.; Calleja-Panero, J.L.; Lens, S.; Manzano, M.L.; Rodríguez, F.G.; Crespo, J.; Piqueras, B.; Pascasio, J.M.; Comas, C.; et al. Effectiveness and safety of Entecavir or Tenofovir in a Spanish cohort of chronic hepatitis B patients: Validation of the page-B score to predict hepatocellular carcinoma. Dig. Dis. Sci. 2017, 62, 784–793. [Google Scholar] [CrossRef]
- Brouwer, W.P.; Van Der Meer, A.J.P.; Boonstra, A.; Plompen, E.P.C.; Pas, S.D.; De Knegt, R.J.; De Man, R.A.; Kate, F.J.W.T.; Janssen, H.L.A.; Hansen, B.E. Prediction of long-term clinical outcome in a diverse chronic hepatitis B population: Role of the PAGE-B score. J. Viral. Hepat. 2017, 24, 1023–1031. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. European Association for the Study of the L: EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Sprinzl, M.F.; Feist, C.; Koch, S.; Kremer, W.M.; Lackner, K.J.; Weinmann, A.; Galle, P.R. Cost evaluation of PAGE-B risk score guided HCC surveillance in patients with treated chronic hepatitis B. BMC Health Serv. Res. 2021, 21, 846. [Google Scholar] [CrossRef]
- Wu, S.; Zeng, N.; Sun, F.; Jia, J.; You, H.; Yang, H.I. Hepatocellular Carcinoma Prediction Models in Chronic Hepatitis B: A Systematic Review of 14 Models and External Validation. Clin. Gastroenterol. Hepatol. 2021, 19, 2499–2513. [Google Scholar] [CrossRef]
- Guo, J.; Gao, X.S. Prediction models for development of hepatocellular carcinoma in chronic hepatitis B patients. World J. Clin. Cases 2021, 9, 3238–3251. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Points | 3 Years Risk | 5 Years Risk | 10 Years Risk |
|---|---|---|---|
| 0 | 0.0% | 0.0% | 0.0% |
| 1 | 0.0% | 0.0% | 0.1% |
| 2 | 0.0% | 0.0% | 0.1% |
| 3 | 0.0% | 0.1% | 0.2% |
| 4 | 0.0% | 0.1% | 0.3% |
| 5 | 0.1% | 0.2% | 0.5% |
| 6 | 0.1% | 0.3% | 0.7% |
| 7 | 0.2% | 0.5% | 1.2% |
| 8 | 0.3% | 0.8% | 2.0% |
| 9 | 0.5% | 1.2% | 3.2% |
| 10 | 0.9% | 2.0% | 5.2% |
| 11 | 1.4% | 3.3% | 8.4% |
| 12 | 2.3% | 5.3% | 13.4% |
| 13 | 3.7% | 8.5% | 21.0% |
| 14 | 6.0% | 13.6% | 32.0% |
| 15 | 9.6% | 21.3% | 46.8% |
| 16 | 15.2% | 32.4% | 64.4% |
| 17 | 23.6% | 47.4% | 81.6% |
| Variables | N (%) |
|---|---|
| Age(years)* | 47.0 (14.0–92.0) |
| Gender | |
| Female | 531 (54.3) |
| Male | 447 (45.7) |
| Alcohol | |
| No | 561 (57,4) |
| Yes | 417 (42,6) |
| Diabetes(DM) | |
| No | 884 (90.4) |
| Yes | 94 (9.6) |
| Hypertension(HAS) | |
| No | 786 (80.4) |
| Yes | 192 (19.6) |
| Cirrhosis | |
| No | 795 (81.3) |
| Yes | 183 (18.7) |
| FamilyhistoryofHBV | |
| No | 804 (82.2) |
| Yes | 174 (17.8) |
| FamilyhistoryofHCC | |
| No | 961 (98.3) |
| Yes | 17 (1.7) |
| Variables | N (%) |
|---|---|
| HBsAg | |
| Positive | 978 (100) |
| TotalAnti-HBc | |
| Positive | 978 (100) |
| HBeAg | |
| Negative | 847 (86.6) |
| Positive | 131 (13.4) |
| Anti-HBe | |
| Negative | 243 (24.8) |
| Positive | 735 (75.2) |
| HBV-DNA | |
| <300 | 403 (41.2) |
| 300–9.999 | 351 (35.9) |
| 10.000–99.999 | 73 (7.5) |
| 100.000–999.999 | 37 (3.7) |
| >1000.000 | 114 (11.7) |
| Platelets | |
| ≥200.000 | 571 (58.4) |
| 100.000–199.999 | 329 (33.6) |
| <100.000 | 78 (8.0) |
| ALT(xULN)* | 0.63 (0.12–12.80) |
| Variables | N (%) |
|---|---|
| Treatment | |
| No | 592 (60.5) |
| Yes | 386 (39.5) |
| Tenofovir | 189 (48.9) |
| Entecavir | 187 (48.4) |
| Adefovir | 01 (0.3) |
| Lamivudine | 04 (1.1) |
| Interferon | 05 (1.3) |
| HCC | |||
|---|---|---|---|
| Variables | No n (%) | Yes n (%) | p-Value |
| Gender | |||
| Female | 521 (98.1) | 10 (1.9) | 0.003 * |
| Male | 423 (94.6) | 24 (5.4) | |
| Age(years, median) | |||
| Median | 47.0 | 60.5 | <0.001@ |
| Alcohol | |||
| No | 541 (96.4) | 20 (3.6) | 0.861 * |
| Yes | 403 (96.6) | 14 (3.4) | |
| Diabetes | |||
| No | 857 (96.9) | 27 (3.1) | 0.037# |
| Yes | 87 (92.6) | 07 (7.4) | |
| Hypertension | |||
| No | 762 (96.9) | 24 (3.1) | 0.144 * |
| Yes | 182 (94.8) | 10 (5.2) | |
| Cirrhosis | |||
| No | 795 (100.0) | 00 (0.0) | <0.001 * |
| Yes | 149 (81.4) | 34 (18.6) | |
| FamilyhistoryofHBV | |||
| No | 770 (95.8) | 34 (4.2) | 0.006 * |
| Yes | 174 (100.0) | 0 (0.0) | |
| FamilyhistoryofHCC | |||
| No | 927 (91.8) | 34 (3.5) | 0.545 # |
| Yes | 17 (100.0) | 0 (0.0) | |
| HCC | |||
|---|---|---|---|
| Variables | No n (%) | Yes n (%) | p-Value |
| HbeAg | |||
| Negative | 828 (97.8) | 19 (2.2) | <0.001# |
| Positive | 116 (88.5) | 15 (11.5) | |
| anti-HBe | |||
| Negative | 228 (93.8) | 15 (6.2) | 0.008 * |
| Positive | 716 (97.4) | 19 (2.6) | |
| Platelets | |||
| ≥200.000 | 564 (98.8) | 07 (1.2) | <0.001 * |
| 199.999–100.000 | 313 (95.1) | 16 (4.9) | |
| <100.000 | 67 (85.9) | 11 (14.1) | |
| HBVDNA | |||
| ≤300 | 389 (96.5) | 14 (3.5) | 0.007# |
| 300–9.999 | 345 (98.3) | 06 (1.7) | |
| 10.000–99.999 | 69 (94.5) | 04 (5.5) | |
| 100.000–999.999 | 32 (86.5) | 05 (13.5) | |
| >1000.000 | 109 (95.6) | 05 (4.4) | |
| CI 95% | ||||
|---|---|---|---|---|
| Score | Area | Lower Limit | Upper Limit | p-Value |
| PAGE-B | 0.788 | 0.661 | 0.915 | 0.005 |
| REACH-B | 0.794 | 0.695 | 0.893 | <0.001 |
| HCC | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Total | |||||||||
| PAGE-B | <11 | 1 | 274 | 275 | |||||||
| ≥11 | 7 | 197 | 204 | ||||||||
| Sensitivity | Specificity | PPV | NPV | PLR | NLR | Accuracy | |||||
| PAGE-B ≥ 11 | 0.875 | 0.582 | 0.034 | 0.996 | 2.09 | 0.214 | 0.586 | ||||
| HCC | |||
|---|---|---|---|
| Yes | No | ||
| REACH-B | ≥7.5 | 13 | 255 |
| <7.5 | 03 | 411 | |
| ≥9.5 | 10 | 129 | |
| <9.5 | 06 | 537 | |
| Sensitivity | Specificity | PPV | NPV | PLR | NLR | Accuracy | |
|---|---|---|---|---|---|---|---|
| REACH-B ≥ 7.5 | 0.812 | 0.617 | 0.048 | 0.992 | 2.122 | 0.303 | 0.621 |
| REACH-B ≥ 9.5 | 0.625 | 0.806 | 0.071 | 0.988 | 3.226 | 0.465 | 0.802 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.P.d.M.; da Silva, M.A.C.N.; Castro, R.S.; Sampaio, A.L.d.O.; Alencar Júnior, A.M.; da Silva, M.C.; Ferreira, A.d.S.P. PAGE-B and REACH-B Predicts the Risk of Developing Hepatocellular Carcinoma in Chronic Hepatitis B Patients from Northeast, Brazil. Viruses 2022, 14, 732. https://doi.org/10.3390/v14040732
Costa APdM, da Silva MACN, Castro RS, Sampaio ALdO, Alencar Júnior AM, da Silva MC, Ferreira AdSP. PAGE-B and REACH-B Predicts the Risk of Developing Hepatocellular Carcinoma in Chronic Hepatitis B Patients from Northeast, Brazil. Viruses. 2022; 14(4):732. https://doi.org/10.3390/v14040732
Chicago/Turabian StyleCosta, Alessandra Porto de Macedo, Marcos Antonio Custódio Neto da Silva, Rogério Soares Castro, Ana Leatrice de Oliveira Sampaio, Antônio Machado Alencar Júnior, Márcia Costa da Silva, and Adalgisa de Souza Paiva Ferreira. 2022. "PAGE-B and REACH-B Predicts the Risk of Developing Hepatocellular Carcinoma in Chronic Hepatitis B Patients from Northeast, Brazil" Viruses 14, no. 4: 732. https://doi.org/10.3390/v14040732
APA StyleCosta, A. P. d. M., da Silva, M. A. C. N., Castro, R. S., Sampaio, A. L. d. O., Alencar Júnior, A. M., da Silva, M. C., & Ferreira, A. d. S. P. (2022). PAGE-B and REACH-B Predicts the Risk of Developing Hepatocellular Carcinoma in Chronic Hepatitis B Patients from Northeast, Brazil. Viruses, 14(4), 732. https://doi.org/10.3390/v14040732