
Deep Learning-Based Visual Complexity Analysis of Electroencephalography Time-Frequency Images: Can It Localize the Epileptogenic Zone in the Brain?

 , ,
, ,  ,
,  , and
, and 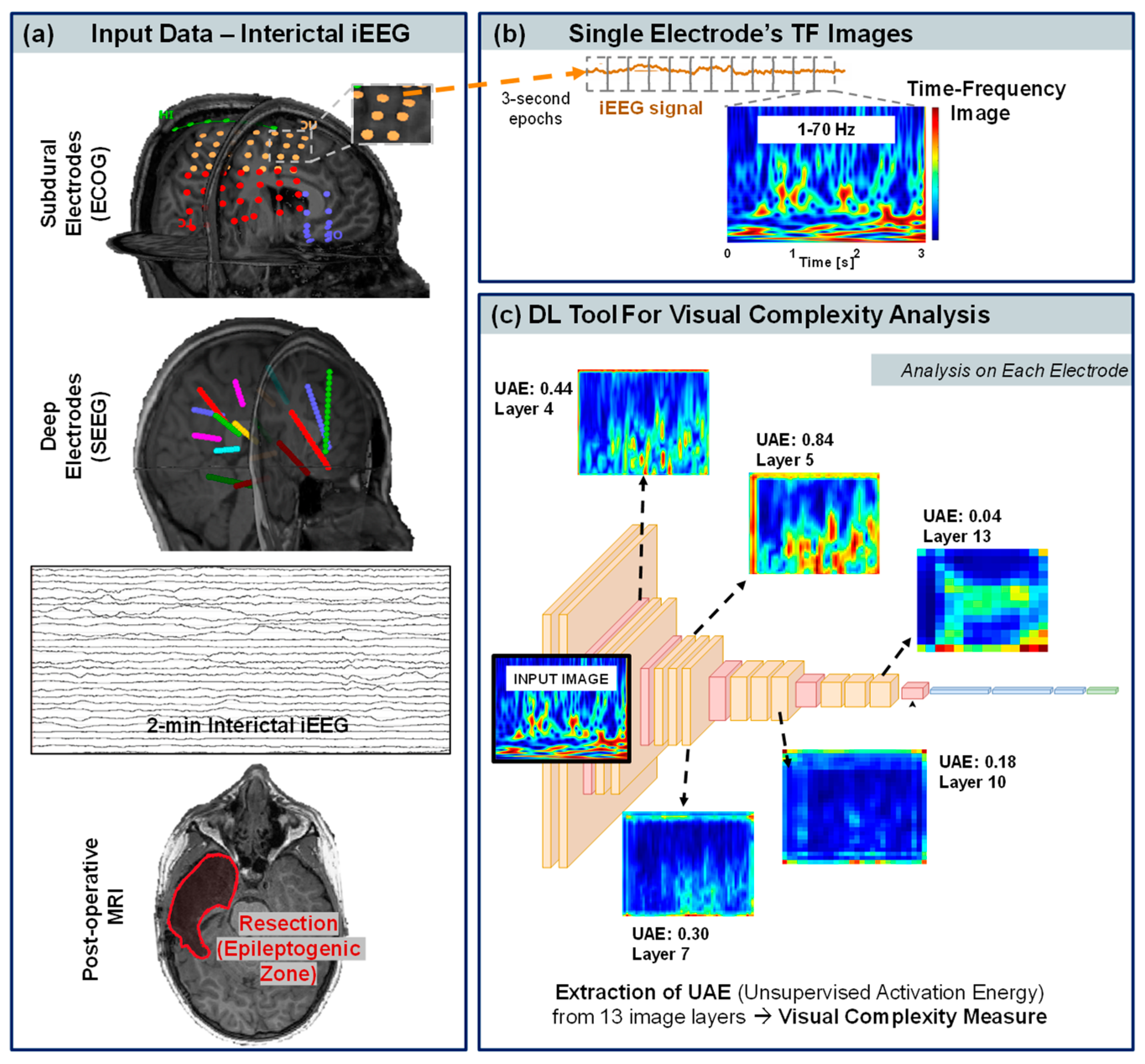{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. TF Image Analysis in Epilepsy
1.2. Deep Learning for the Analysis of Visual Complexity
1.3. Our Contribution
2. Materials and Methods
2.1. Patient Cohort
2.2. iEEG Acquisition and Data Selection
2.3. Localization and Classification of Contacts
2.4. Epileptogenic Zone (EZ), Seizure Onset Zone (SOZ), and Post-Surgical Outcome
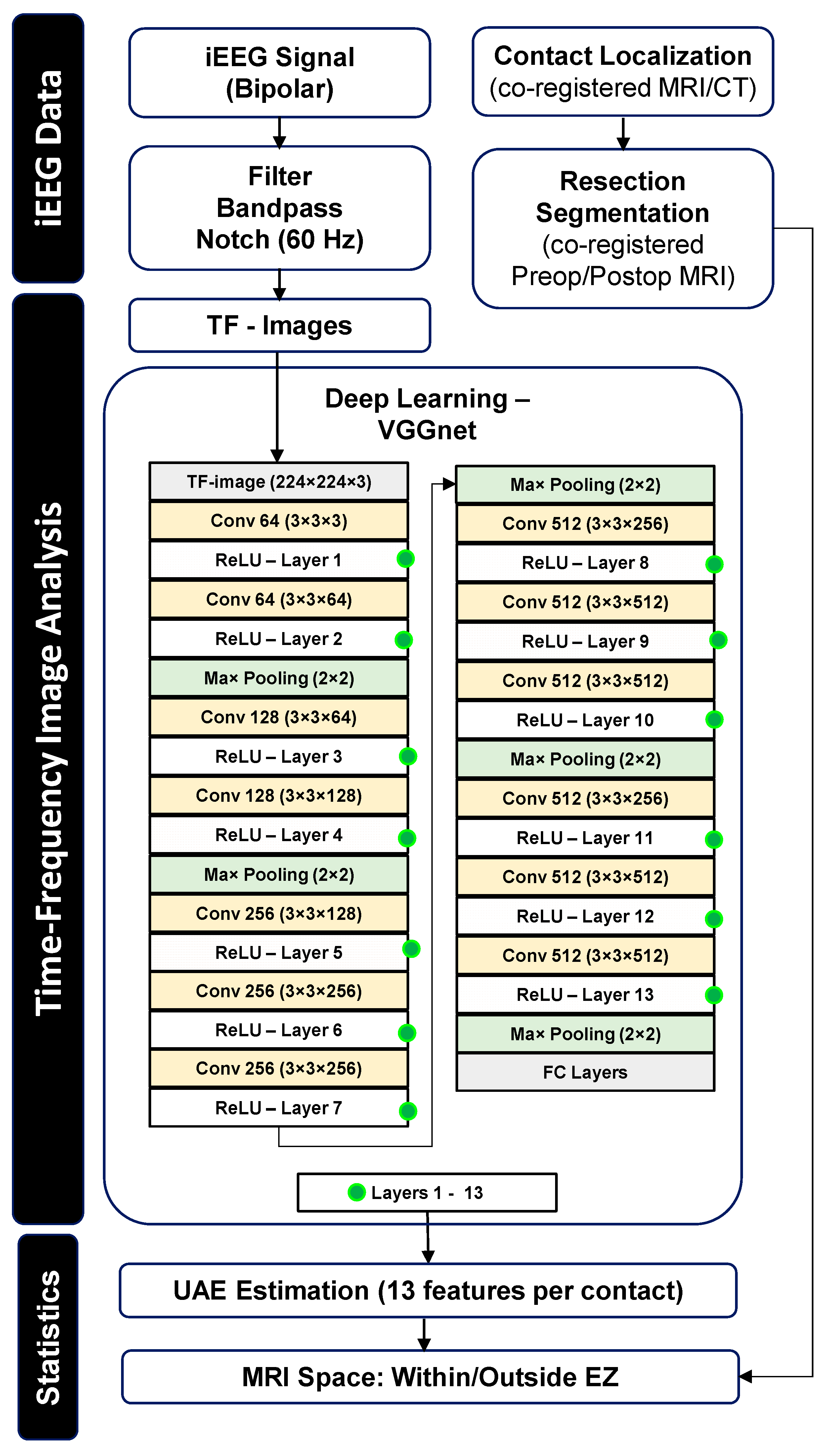
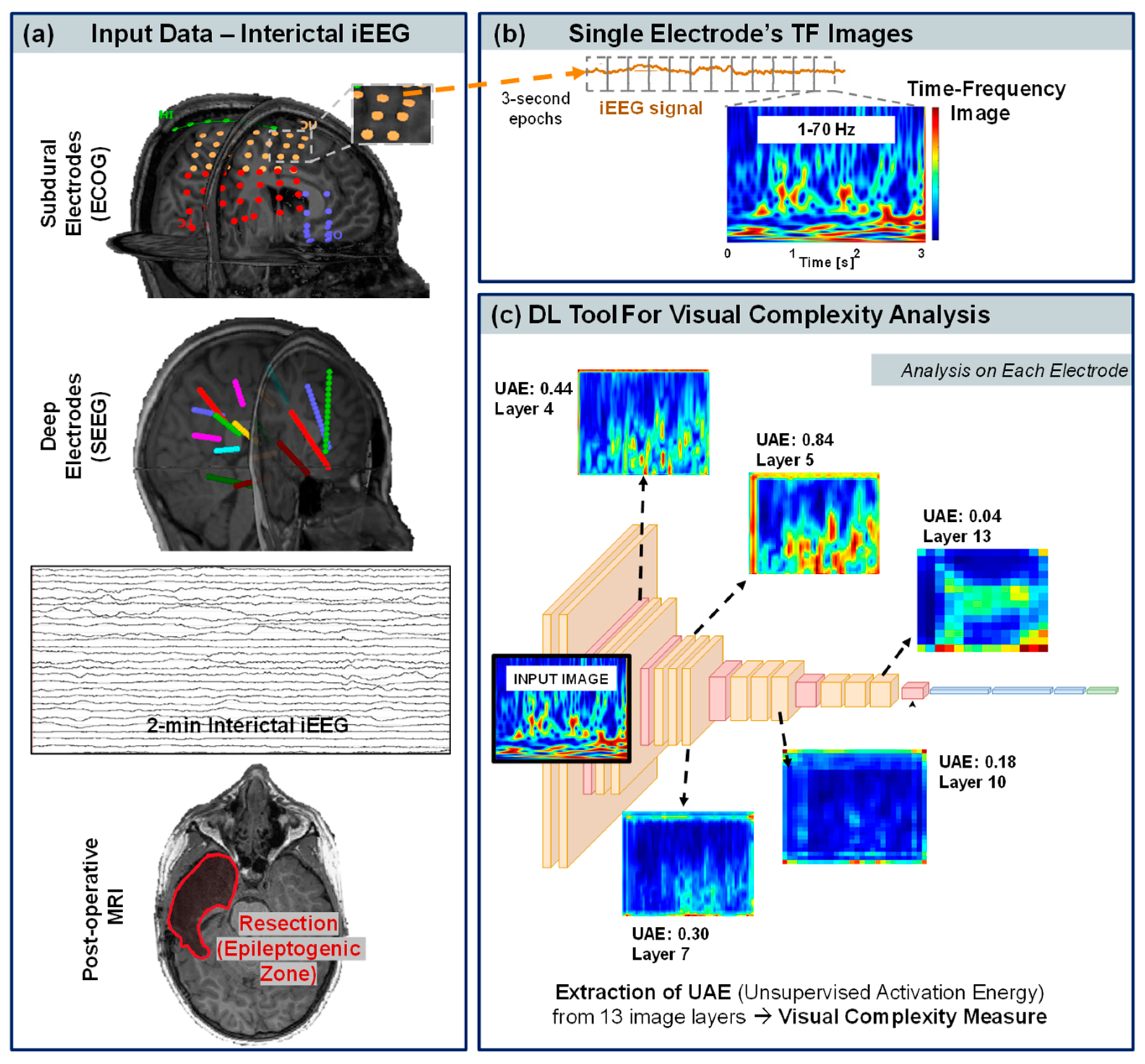
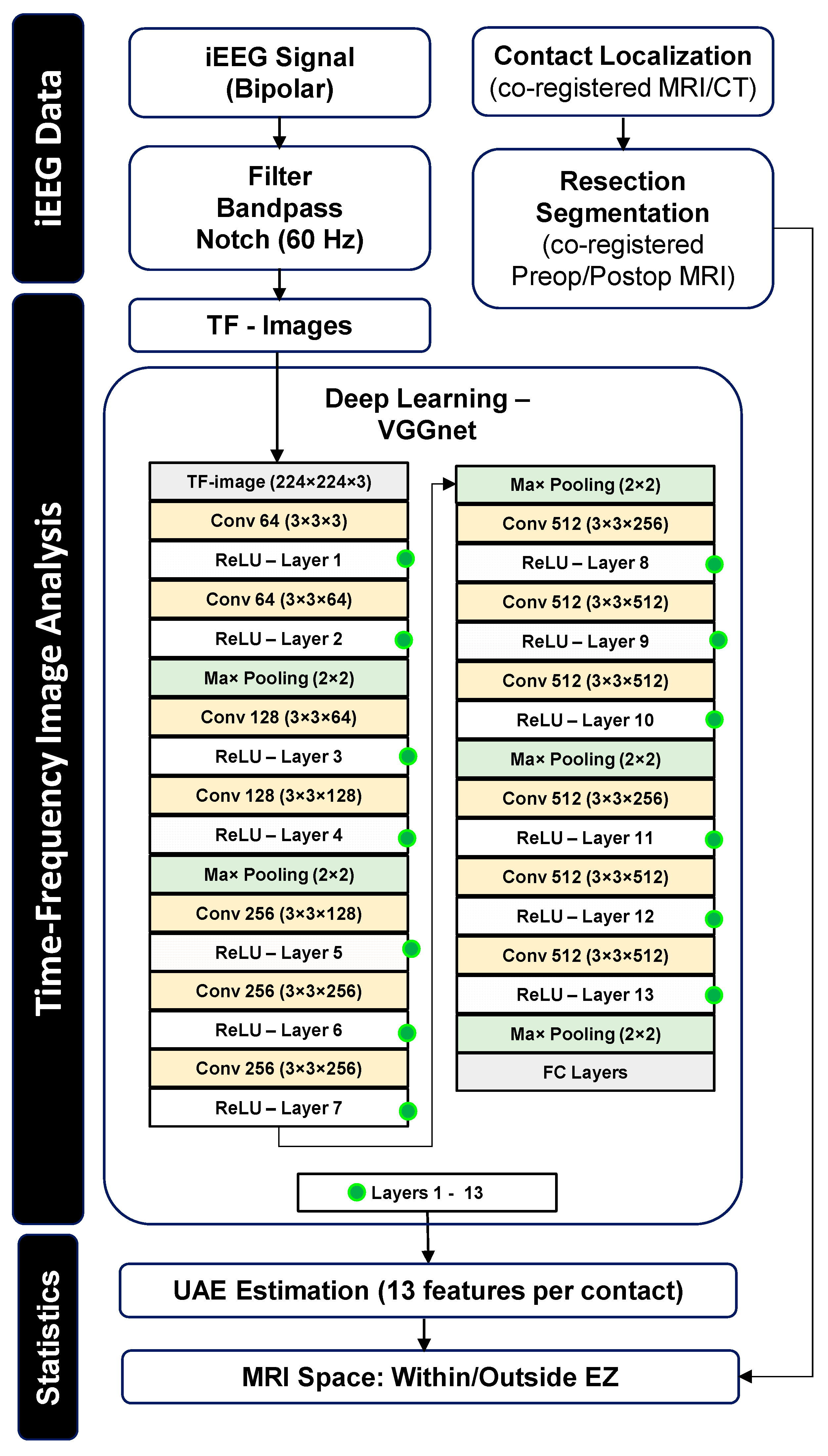
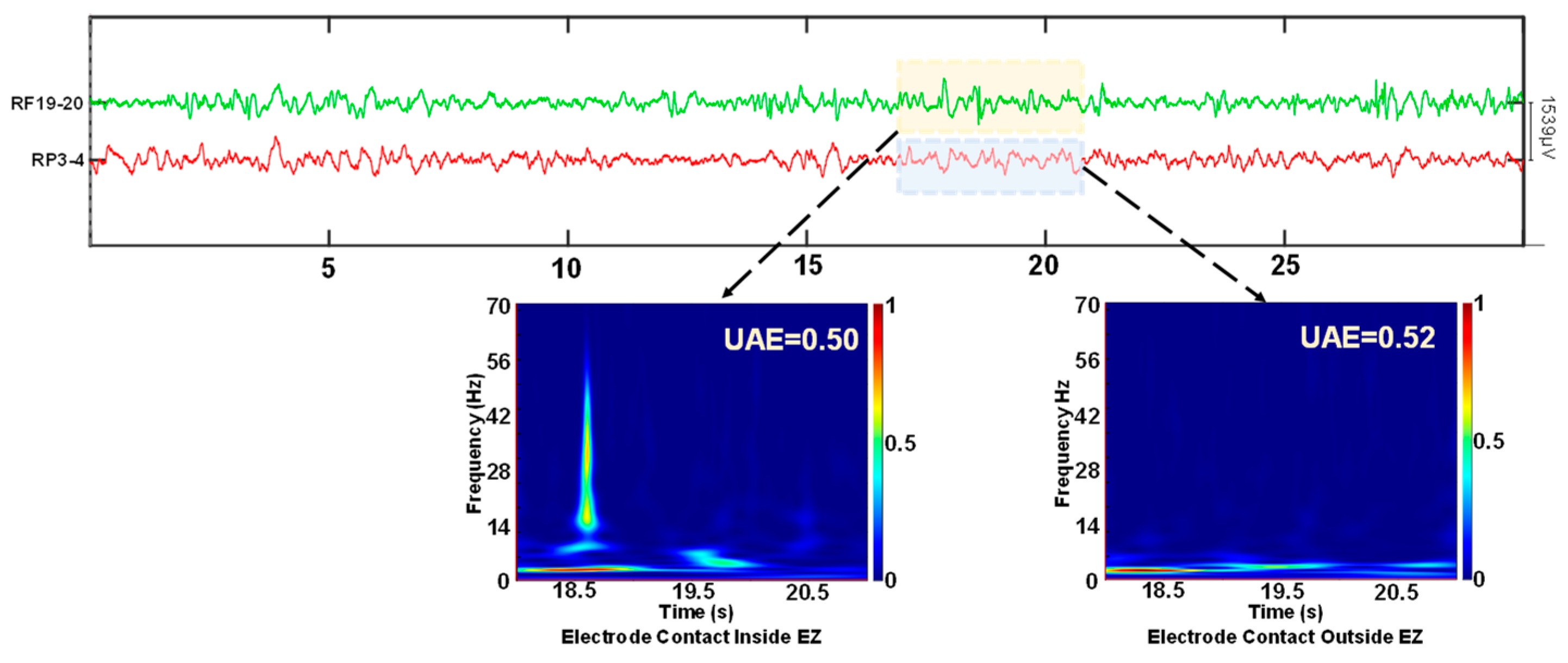
2.5. Time-Frequency Representation
2.6. Deep Learning-Based Visual Complexity
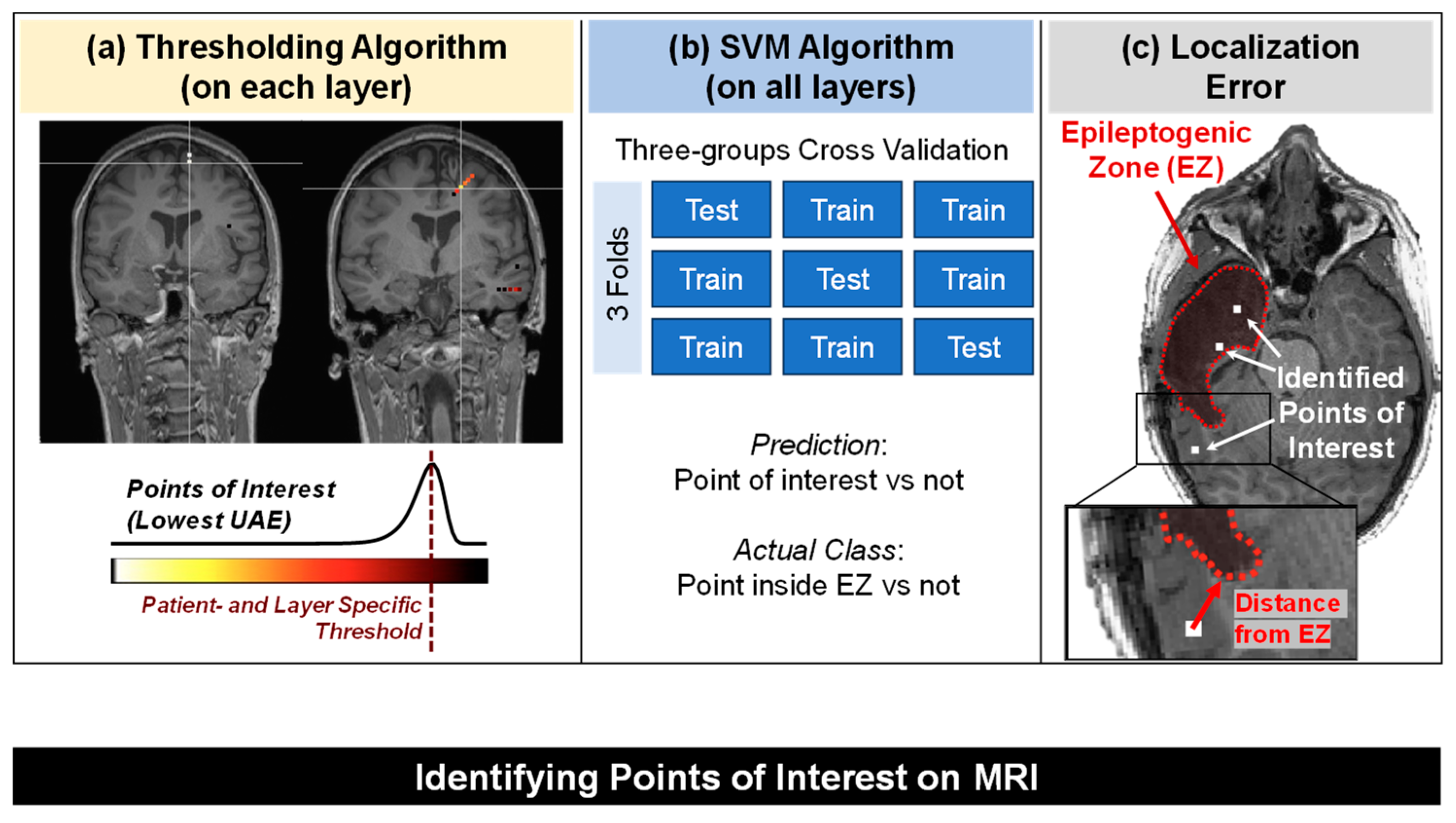
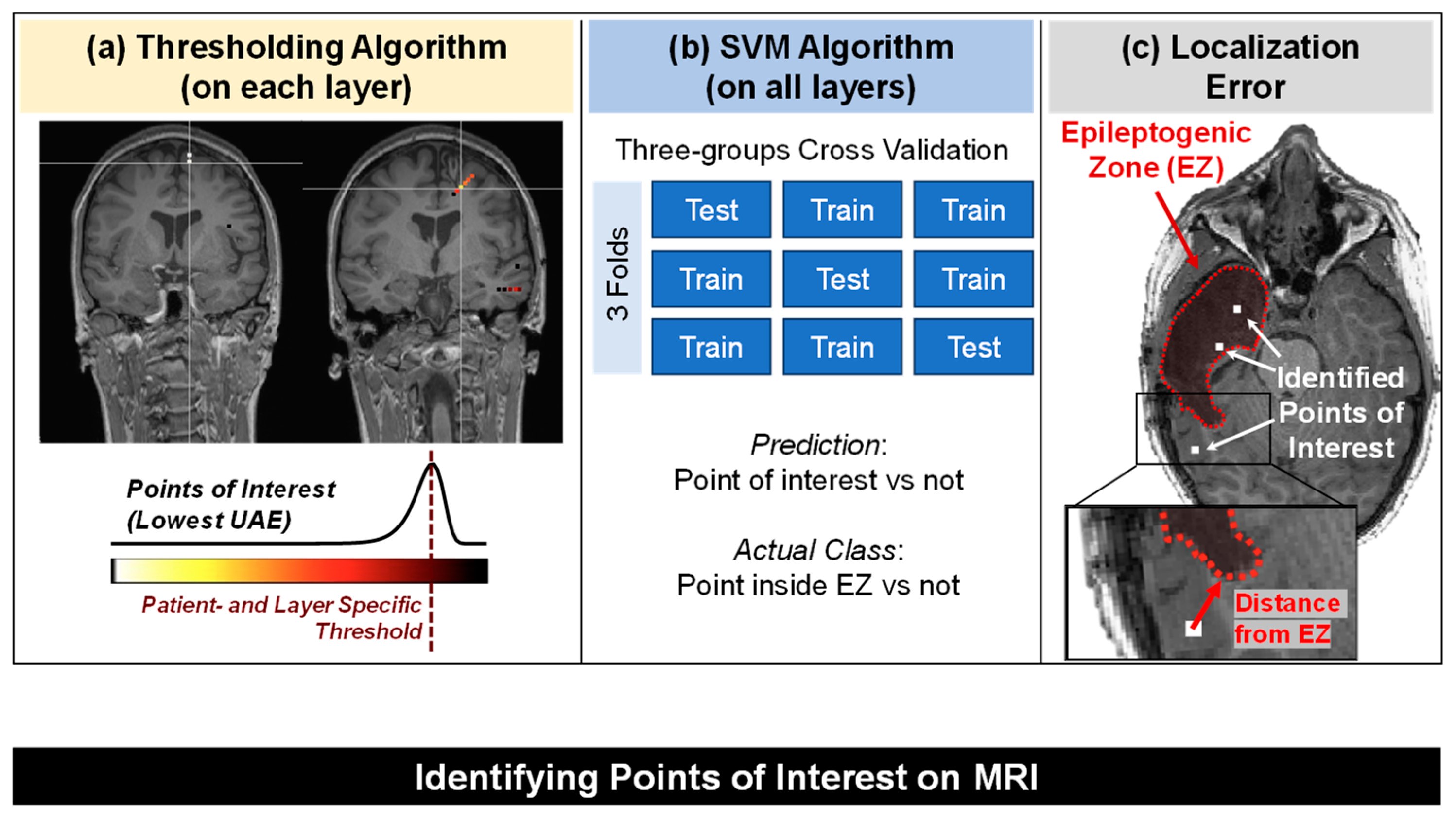
2.7. Identification of the “Points of Interest” Based on Their TF Image Visual Complexity
- (1)
- Patient- and layer-specific thresholding algorithm: thresholds were identified by fitting each layer’s UAE values to an extreme-value distribution [44,45,46]. The tail of the distribution contains the contacts with lower complexity, which we regarded as our points of interest in the brain. Extreme value theory pertains to the science of modeling and quantifying occurrences that have extremely low probabilities. Extreme value distribution can be generalized to distributions with the following probability density function (p) that depends on the location parameter (μ) and scale parameter (σ).
- (2)
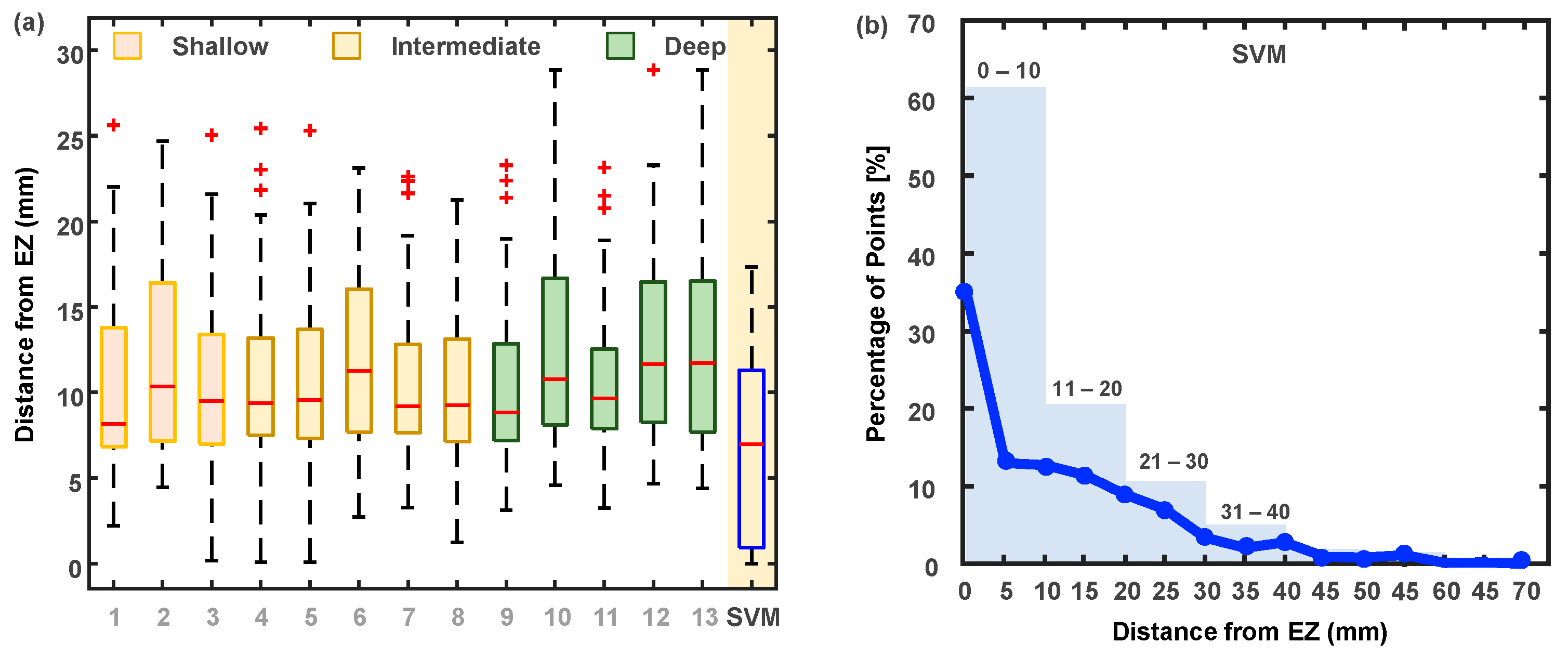
- We used the UAE values from all the layers and passed them to a support vector machine’s classifier (see Figure 3b) with a linear kernel to classify each contact as a point of interest or not, where the ground truth label consisted of whether a point (contact) was inside or outside the EZ. As a validation strategy, we adopted a three-fold cross-validation, where we split the subjects into three distinct groups with similar class distribution [47] (similar proportion of contacts inside vs. outside the EZ). The number of contacts in the two classes (inside versus outside the EZ) for each group was: for Group 1, 259 inside versus 375 outside; for Group 2, 294 versus 378; and for Group 3, 244 versus 378. The groups were defined such that the subjects in each group were distinct (number of subjects per group: 7 in G1, 7 in G2, and 6 in G3).
2.8. Statistical Analysis
3. Results
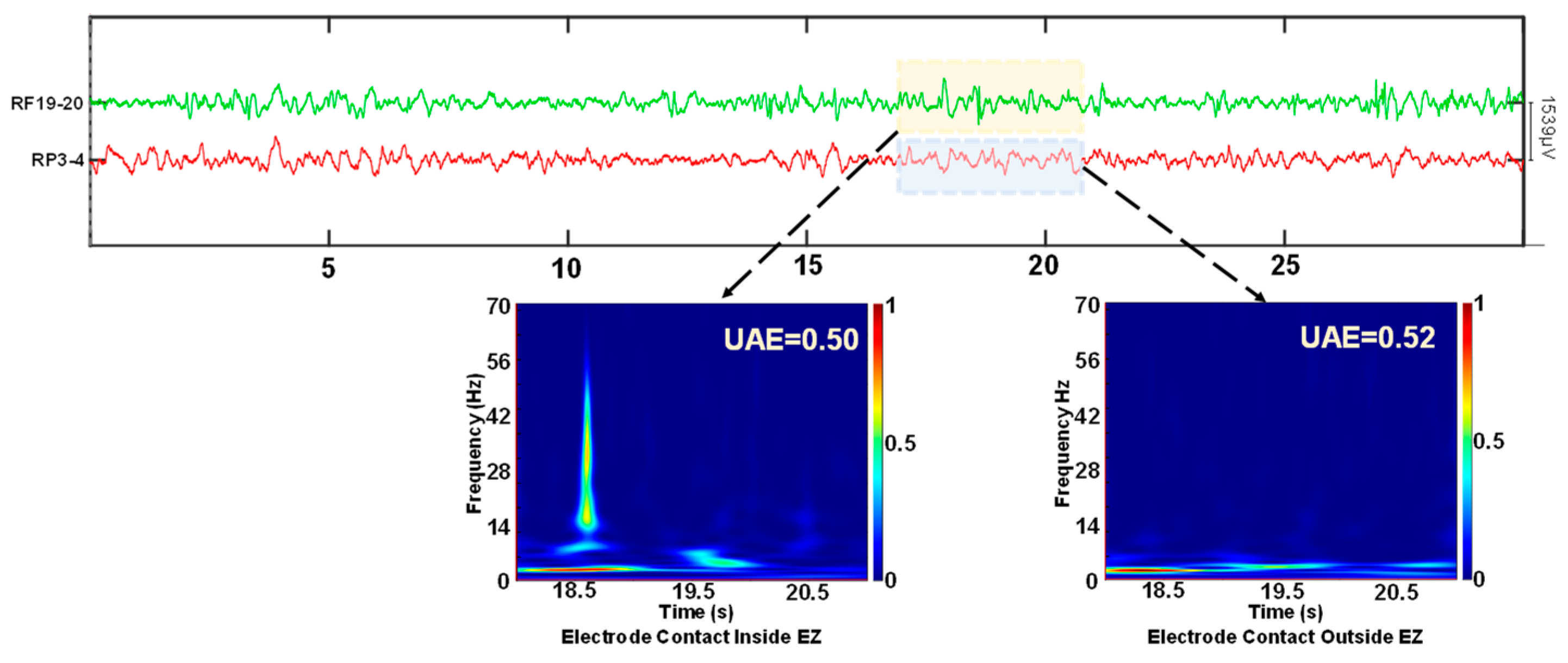
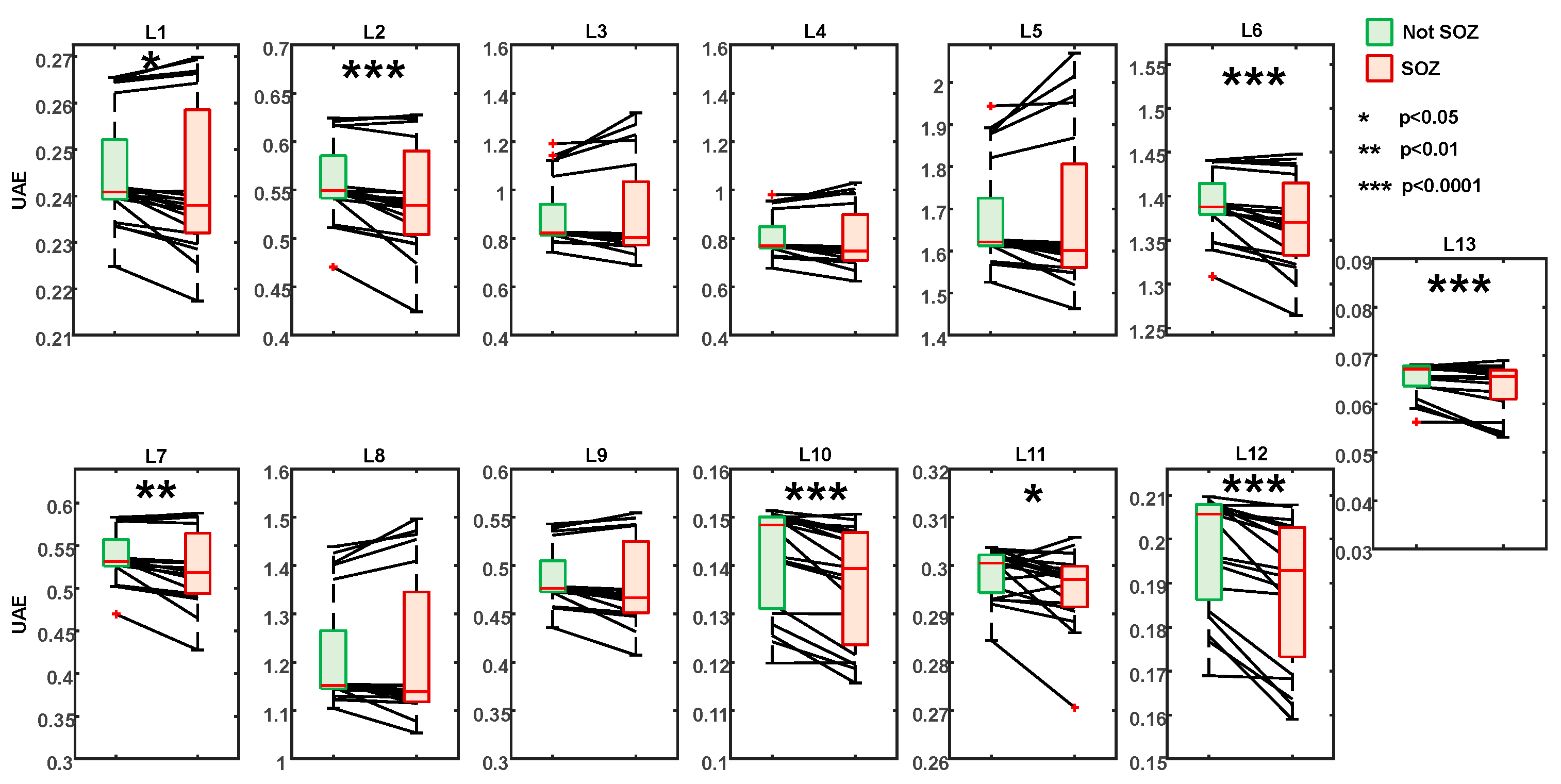
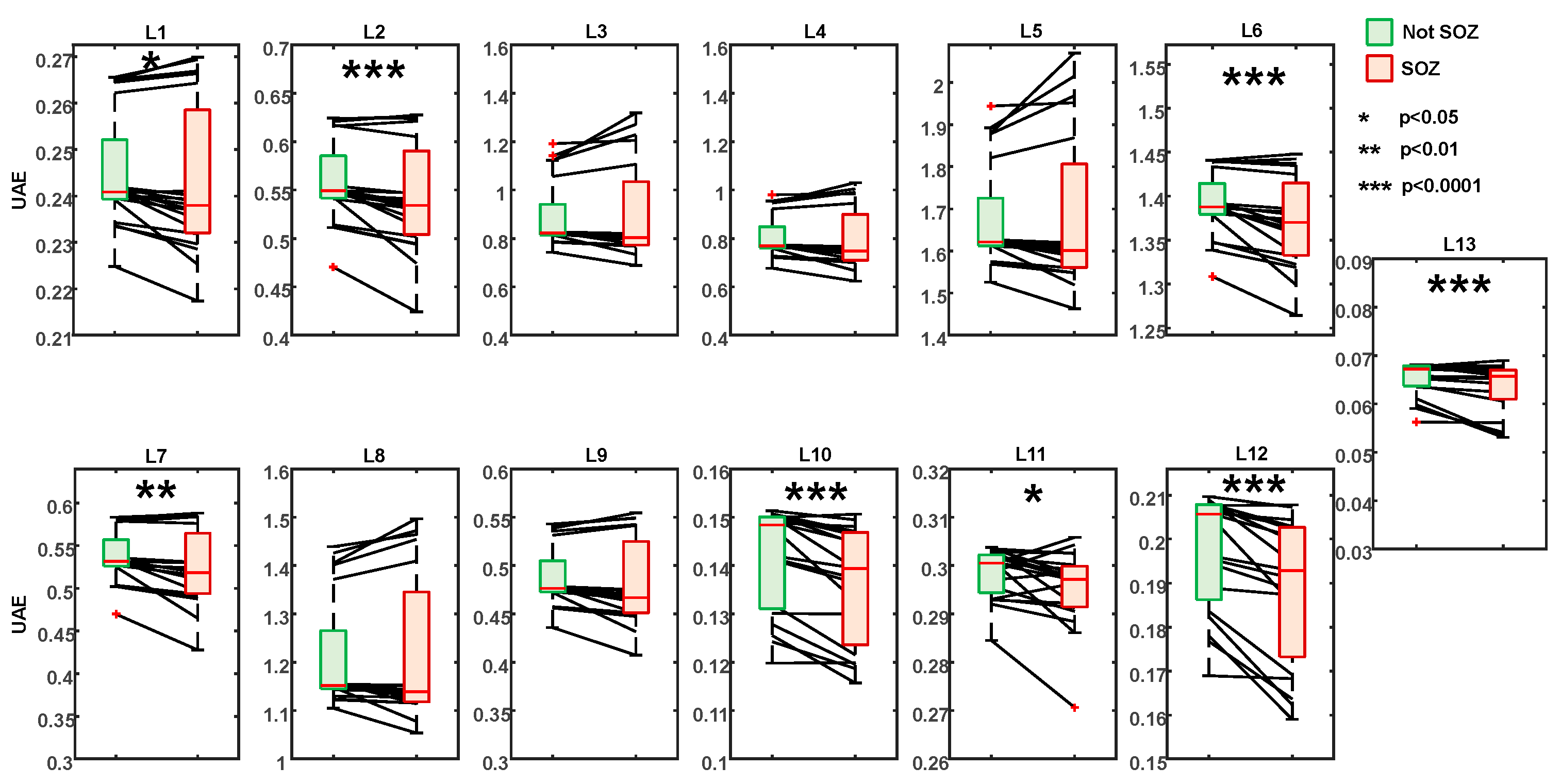
3.1. UAE Values and Their Correspondance to the Seizure Onset Zone
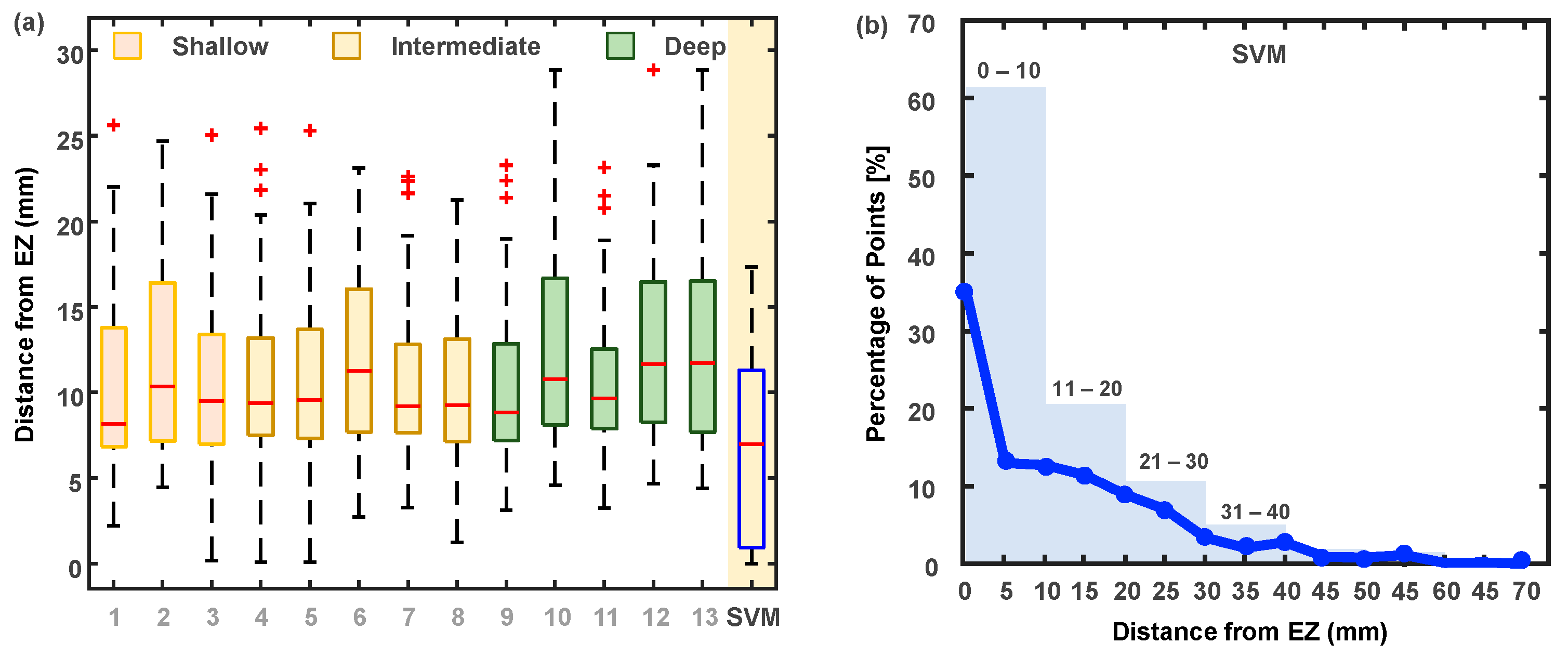
3.2. Identification of the “Points of Interest”
4. Discussion
4.1. Comparison with Existing Methods
4.2. Considerations on the Automated Approach
4.3. Limitations and Future Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Antoniades, A.; Spyrou, L.; Martin-Lopez, D.; Valentin, A.; Alarcon, G.; Sanei, S.; Cheong Took, C. Detection of Interictal Discharges With Convolutional Neural Networks Using Discrete Ordered Multichannel Intracranial EEG. IEEE Trans. Neural Syst. Rehabil. Eng. Publ. IEEE Eng. Med. Biol. Soc. 2017, 25, 2285–2294. [Google Scholar] [CrossRef]
- Lalgudi Ganesan, S.; Hahn, C.D. Spectrograms for Seizure Detection in Critically Ill Children. J. Clin. Neurophysiol. 2022, 39, 195. [Google Scholar] [CrossRef]
- Stewart, C.P.; Otsubo, H.; Ochi, A.; Sharma, R.; Hutchison, J.S.; Hahn, C.D. Seizure Identification in the ICU Using Quantitative EEG Displays(e–Pub Ahead of Print). Neurology 2010, 75, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Akman, C.I.; Micic, V.; Thompson, A.; Riviello, J.J. Seizure Detection Using Digital Trend Analysis: Factors Affecting Utility. Epilepsy Res. 2011, 93, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Pensirikul, A.D.; Beslow, L.A.; Kessler, S.K.; Sanchez, S.M.; Topjian, A.A.; Dlugos, D.J.; Abend, N.S. Density Spectral Array for Seizure Identification in Critically Ill Children. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2013, 30, 371–375. [Google Scholar] [CrossRef]
- Topjian, A.A.; Fry, M.; Jawad, A.F.; Herman, S.T.; Nadkarni, V.M.; Ichord, R.; Berg, R.A.; Dlugos, D.J.; Abend, N.S. Detection of Electrographic Seizures by Critical Care Providers Using Color Density Spectral Array after Cardiac Arrest Is Feasible. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc. 2015, 16, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Lalgudi Ganesan, S.; Stewart, C.P.; Atenafu, E.G.; Sharma, R.; Guerguerian, A.-M.; Hutchison, J.S.; Hahn, C.D. Seizure Identification by Critical Care Providers Using Quantitative Electroencephalography. Crit. Care Med. 2018, 46, e1105–e1111. [Google Scholar] [CrossRef]
- Rowberry, T.; Kanthimathinathan, H.K.; George, F.; Notghi, L.; Gupta, R.; Bill, P.; Wassmer, E.; Duncan, H.P.; Morris, K.P.; Scholefield, B.R. Implementation and Early Evaluation of a Quantitative Electroencephalography Program for Seizure Detection in the PICU. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc. 2020, 21, 543–549. [Google Scholar] [CrossRef]
- Swarnalingam, E.S.; RamachandranNair, R.; Choong, K.L.M.; Jones, K.C. Non-Neurophysiologist Physicians and Nurses Can Detect Subclinical Seizures in Children Using a Panel of Quantitative EEG Trends and a Seizure Detection Algorithm. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2022, 39, 453–458. [Google Scholar] [CrossRef]
- Pont-Thibodeau, G.D.; Sanchez, S.M.; Jawad, A.F.; Nadkarni, V.M.; Berg, R.A.; Abend, N.S.; Topjian, A.A. Seizure Detection by Critical Care Providers Using Amplitude-Integrated EEG and Color Density Spectral Array in Pediatric Cardiac Arrest Patients. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc. 2017, 18, 363–369. [Google Scholar] [CrossRef]
- Bartolomei, F.; Chauvel, P.; Wendling, F. Epileptogenicity of Brain Structures in Human Temporal Lobe Epilepsy: A Quantified Study from Intracerebral EEG. Brain 2008, 131, 1818–1830. [Google Scholar] [CrossRef]
- Grinenko, O.; Li, J.; Mosher, J.C.; Wang, I.Z.; Bulacio, J.C.; Gonzalez-Martinez, J.; Nair, D.; Najm, I.; Leahy, R.M.; Chauvel, P. A Fingerprint of the Epileptogenic Zone in Human Epilepsies. Brain 2018, 141, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Principe, A.; Tadel, F.; Hoffmann, D.; Chabardes, S.; Minotti, L.; David, O.; Kahane, P. Mapping the Insula with Stereo-Electroencephalography: The Emergence of Semiology in Insula Lobe Seizures. Ann. Neurol. 2020, 88, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Giacomo, R.D.; Uribe-San-Martin, R.; Mai, R.; Francione, S.; Nobili, L.; Sartori, I.; Gozzo, F.; Pelliccia, V.; Onofrj, M.; Russo, G.L.; et al. Stereo-EEG Ictal/Interictal Patterns and Underlying Pathologies. Seizure Eur. J. Epilepsy 2019, 72, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Lagarde, S.; Buzori, S.; Trebuchon, A.; Carron, R.; Scavarda, D.; Milh, M.; McGonigal, A.; Bartolomei, F. The Repertoire of Seizure Onset Patterns in Human Focal Epilepsies: Determinants and Prognostic Values. Epilepsia 2019, 60, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Lagarde, S.; Bonini, F.; McGonigal, A.; Chauvel, P.; Gavaret, M.; Scavarda, D.; Carron, R.; Régis, J.; Aubert, S.; Villeneuve, N.; et al. Seizure-Onset Patterns in Focal Cortical Dysplasia and Neurodevelopmental Tumors: Relationship with Surgical Prognosis and Neuropathologic Subtypes. Epilepsia 2016, 57, 1426–1435. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. ImageNet: A Large-Scale Hierarchical Image Database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Zhou, B.; Lapedriza, A.; Khosla, A.; Oliva, A.; Torralba, A. Places: A 10 Million Image Database for Scene Recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 40, 1452–1464. [Google Scholar] [CrossRef]
- Bian, L.; Song, H.; Peng, L.; Chang, X.; Yang, X.; Horstmeyer, R.; Ye, L.; Zhu, C.; Qin, T.; Zheng, D.; et al. High-Resolution Single-Photon Imaging with Physics-Informed Deep Learning. Nat. Commun. 2023, 14, 5902. [Google Scholar] [CrossRef]
- He, Y.; Varley, Z.K.; Nouri, L.O.; Moody, C.J.A.; Jardine, M.D.; Maddock, S.; Thomas, G.H.; Cooney, C.R. Deep Learning Image Segmentation Reveals Patterns of UV Reflectance Evolution in Passerine Birds. Nat. Commun. 2022, 13, 5068. [Google Scholar] [CrossRef]
- Rashid, S.; Raza, M.; Sharif, M.; Azam, F.; Kadry, S.; Kim, J. White Blood Cell Image Analysis for Infection Detection Based on Virtual Hexagonal Trellis (VHT) by Using Deep Learning. Sci. Rep. 2023, 13, 17827. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. Available online: https://arxiv.org/abs/1409.1556v6 (accessed on 27 October 2023).
- Zhang, T.; Li, K.; Chen, X.; Zhong, C.; Luo, B.; Grijalva, I.; McCornack, B.; Flippo, D.; Sharda, A.; Wang, G. Aphid Cluster Recognition and Detection in the Wild Using Deep Learning Models. Sci. Rep. 2023, 13, 13410. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Saraee, E.; Jalal, M.; Betke, M. Visual Complexity Analysis Using Deep Intermediate-Layer Features. Comput. Vis. Image Underst. 2020, 195, 102949. [Google Scholar] [CrossRef]
- Tamilia, E.; AlHilani, M.; Tanaka, N.; Tsuboyama, M.; Peters, J.M.; Grant, P.E.; Madsen, J.R.; Stufflebeam, S.M.; Pearl, P.L.; Papadelis, C. Assessing the Localization Accuracy and Clinical Utility of Electric and Magnetic Source Imaging in Children with Epilepsy. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2019, 130, 491–504. [Google Scholar] [CrossRef]
- Tamilia, E.; Matarrese, M.A.G.; Ntolkeras, G.; Grant, P.E.; Madsen, J.R.; Stufflebeam, S.M.; Pearl, P.L.; Papadelis, C. Non-invasive Mapping of Ripple Onset Predicts Outcome in Epilepsy Surgery. Ann. Neurol. 2021, 89, 911–925. [Google Scholar] [CrossRef] [PubMed]
- Tamilia, E.; Park, E.-H.; Percivati, S.; Bolton, J.; Taffoni, F.; Peters, J.M.; Grant, P.E.; Pearl, P.L.; Madsen, J.R.; Papadelis, C. Surgical Resection of Ripple Onset Predicts Outcome in Pediatric Epilepsy. Ann. Neurol. 2018, 84, 331–346. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, X.; Mo, J.; Sang, L.; Zhao, B.; Zhang, C.; Hu, W.; Zhang, J.; Shao, X.; Zhang, K. Symptomatogenic Zone and Network of Oroalimentary Automatisms in Mesial Temporal Lobe Epilepsy. Epilepsia 2019, 60, 1150–1159. [Google Scholar] [CrossRef]
- Tadel, F.; Baillet, S.; Mosher, J.C.; Pantazis, D.; Leahy, R.M. Brainstorm: A User-Friendly Application for MEG/EEG Analysis. Comput. Intell. Neurosci. 2011, 2011, 879716. [Google Scholar] [CrossRef]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical Surface-Based Analysis. I. Segmentation and Surface Reconstruction. NeuroImage 1999, 9, 179–194. [Google Scholar] [CrossRef]
- Rosenow, F.; Lüders, H. Pre-surgical Evaluation of Epilepsy. Brain 2001, 124, 1683–1700. [Google Scholar] [CrossRef]
- Billardello, R.; Ntolkeras, G.; Chericoni, A.; Madsen, J.R.; Papadelis, C.; Pearl, P.L.; Grant, P.E.; Taffoni, F.; Tamilia, E. Novel User-Friendly Application for MRI Segmentation of Brain Resection Following Epilepsy Surgery. Diagnostics 2022, 12, 1017. [Google Scholar] [CrossRef] [PubMed]
- Ntolkeras, G.; Tamilia, E.; AlHilani, M.; Bolton, J.; Ellen Grant, P.; Prabhu, S.P.; Madsen, J.R.; Stufflebeam, S.M.; Pearl, P.L.; Papadelis, C. Pre-surgical Accuracy of Dipole Clustering in MRI-Negative Pediatric Patients with Epilepsy: Validation against Intracranial EEG and Resection. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2022, 141, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Hedrich, T.; Chowdhury, R.; Hall, J.A.; Lina, J.-M.; Dubeau, F.; Kobayashi, E.; Grova, C. Source Localization of the Seizure Onset Zone from Ictal EEG/MEG Data. Hum. Brain Mapp. 2016, 37, 2528–2546. [Google Scholar] [CrossRef] [PubMed]
- Gotman, J.; Levtova, V.; Farine, B. Graphic Representation of the EEG during Epileptic Seizures. Electroencephalogr. Clin. Neurophysiol. 1993, 87, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Engel, J., Jr.; Van Ness, P.; Rasmussen, T.; Ojemann, L. Outcome with Respect to Epileptic Seizures. In Surgical Treatment of the Epilepsies, 2nd ed.; Raven Press: New York, NY, USA, 1993. [Google Scholar]
- Bertrand, O.; Tallon-Baudry, C. Oscillatory Gamma Activity in Humans: A Possible Role for Object Representation. Int. J. Psychophysiol. 2000, 38, 211–223. [Google Scholar] [CrossRef]
- Bruns, A. Fourier-, Hilbert- and Wavelet-Based Signal Analysis: Are They Really Different Approaches? J. Neurosci. Methods 2004, 137, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Le Van Quyen, M.; Foucher, J.; Lachaux, J.-P.; Rodriguez, E.; Lutz, A.; Martinerie, J.; Varela, F.J. Comparison of Hilbert Transform and Wavelet Methods for the Analysis of Neuronal Synchrony. J. Neurosci. Methods 2001, 111, 83–98. [Google Scholar] [CrossRef]
- Bruna, J.; Sprechmann, P.; LeCun, Y. Super-Resolution with Deep Convolutional Sufficient Statistics. Available online: https://arxiv.org/abs/1511.05666v4 (accessed on 27 October 2023).
- Johnson, J.; Alahi, A.; Fei-Fei, L. Perceptual Losses for Real-Time Style Transfer and Super-Resolution. In Computer Vision—ECCV 2016; Leibe, B., Matas, J., Sebe, N., Welling, M., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2016; Volume 9906, pp. 694–711. ISBN 978-3-319-46474-9. [Google Scholar]
- Ledig, C.; Theis, L.; Huszar, F.; Caballero, J.; Cunningham, A.; Acosta, A.; Aitken, A.; Tejani, A.; Totz, J.; Wang, Z.; et al. Photo-Realistic Single Image Super-Resolution Using a Generative Adversarial Network. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), IEEE, Honolulu, HI, USA, 21–26 July 2017; pp. 105–114. [Google Scholar]
- Bhattacharya, S.; Kamper, F.; Beirlant, J. Outlier Detection Based on Extreme Value Theory and Applications. Scand. J. Stat. 2023, 50, 1466–1502. [Google Scholar] [CrossRef]
- Dey, D.K.; Yan, J. Extreme Value Modeling and Risk Analysis: Methods and Applications; CRC Press: Boca Raton, FL, USA, 2016; ISBN 978-1-4987-0131-0. [Google Scholar]
- Coles, S. An Introduction to Statistical Modeling of Extreme Values; Springer Series in Statistics; Springer: London, UK, 2013; ISBN 978-1-4471-3675-0. [Google Scholar]
- Makaram, N.; Von Ellenrieder, N.; Tanaka, H.; Gotman, J. Automated Classification of Five Seizure Onset Patterns from Intracranial Electroencephalogram Signals. Clin. Neurophysiol. 2020, 131, 1210–1218. [Google Scholar] [CrossRef]
- Matarrese, M.A.G.; Loppini, A.; Fabbri, L.; Tamilia, E.; Perry, M.S.; Madsen, J.R.; Bolton, J.; Stone, S.S.D.; Pearl, P.L.; Filippi, S.; et al. Spike Propagation Mapping Reveals Effective Connectivity and Predicts Surgical Outcome in Epilepsy. Brain 2023, 146, 3898–3912. [Google Scholar] [CrossRef]
- Kim, D.; Joo, E.Y.; Seo, D.-W.; Kim, M.-Y.; Lee, Y.-H.; Kwon, H.C.; Kim, J.-M.; Hong, S.B. Accuracy of MEG in Localizing Irritative Zone and Seizure Onset Zone: Quantitative Comparison between MEG and Intracranial EEG. Epilepsy Res. 2016, 127, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Corona, L.; Tamilia, E.; Perry, M.S.; Madsen, J.R.; Bolton, J.; Stone, S.S.D.; Stufflebeam, S.M.; Pearl, P.L.; Papadelis, C. Non-Invasive Mapping of Epileptogenic Networks Predicts Surgical Outcome. Brain J. Neurol. 2023, 146, 1916–1931. [Google Scholar] [CrossRef] [PubMed]
- Önal, Ç.; Otsubo, H.; Araki, T.; Chitoku, S.; Ochi, A.; Weiss, S.; Logan, W.; Elliott, I.; Snead, O.C.; Rutka, J.T. Complications of Invasive Subdural Grid Monitoring in Children with Epilepsy. J. Neurosurg. 2003, 98, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Shu, S.; Luo, S.; Cao, M.; Xu, K.; Qin, L.; Zheng, L.; Xu, J.; Wang, X.; Gao, J.-H. Informed MEG/EEG Source Imaging Reveals the Locations of Interictal Spikes Missed by SEEG. NeuroImage 2022, 254, 119132. [Google Scholar] [CrossRef] [PubMed]
- Juárez-Martinez, E.L.; Nissen, I.A.; Idema, S.; Velis, D.N.; Hillebrand, A.; Stam, C.J.; van Straaten, E.C.W. Virtual Localization of the Seizure Onset Zone: Using Non-Invasive MEG Virtual Electrodes at Stereo-EEG Electrode Locations in Refractory Epilepsy Patients. NeuroImage Clin. 2018, 19, 758–766. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makaram, N.; Gupta, S.; Pesce, M.; Bolton, J.; Stone, S.; Haehn, D.; Pomplun, M.; Papadelis, C.; Pearl, P.; Rotenberg, A.; et al. Deep Learning-Based Visual Complexity Analysis of Electroencephalography Time-Frequency Images: Can It Localize the Epileptogenic Zone in the Brain? Algorithms 2023, 16, 567. https://doi.org/10.3390/a16120567
Makaram N, Gupta S, Pesce M, Bolton J, Stone S, Haehn D, Pomplun M, Papadelis C, Pearl P, Rotenberg A, et al. Deep Learning-Based Visual Complexity Analysis of Electroencephalography Time-Frequency Images: Can It Localize the Epileptogenic Zone in the Brain? Algorithms. 2023; 16(12):567. https://doi.org/10.3390/a16120567
Chicago/Turabian StyleMakaram, Navaneethakrishna, Sarvagya Gupta, Matthew Pesce, Jeffrey Bolton, Scellig Stone, Daniel Haehn, Marc Pomplun, Christos Papadelis, Phillip Pearl, Alexander Rotenberg, and et al. 2023. "Deep Learning-Based Visual Complexity Analysis of Electroencephalography Time-Frequency Images: Can It Localize the Epileptogenic Zone in the Brain?" Algorithms 16, no. 12: 567. https://doi.org/10.3390/a16120567
APA StyleMakaram, N., Gupta, S., Pesce, M., Bolton, J., Stone, S., Haehn, D., Pomplun, M., Papadelis, C., Pearl, P., Rotenberg, A., Grant, P. E., & Tamilia, E. (2023). Deep Learning-Based Visual Complexity Analysis of Electroencephalography Time-Frequency Images: Can It Localize the Epileptogenic Zone in the Brain? Algorithms, 16(12), 567. https://doi.org/10.3390/a16120567