

Aspects and Principles of Material Connections in Restorative Dentistry—A Comprehensive Review

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
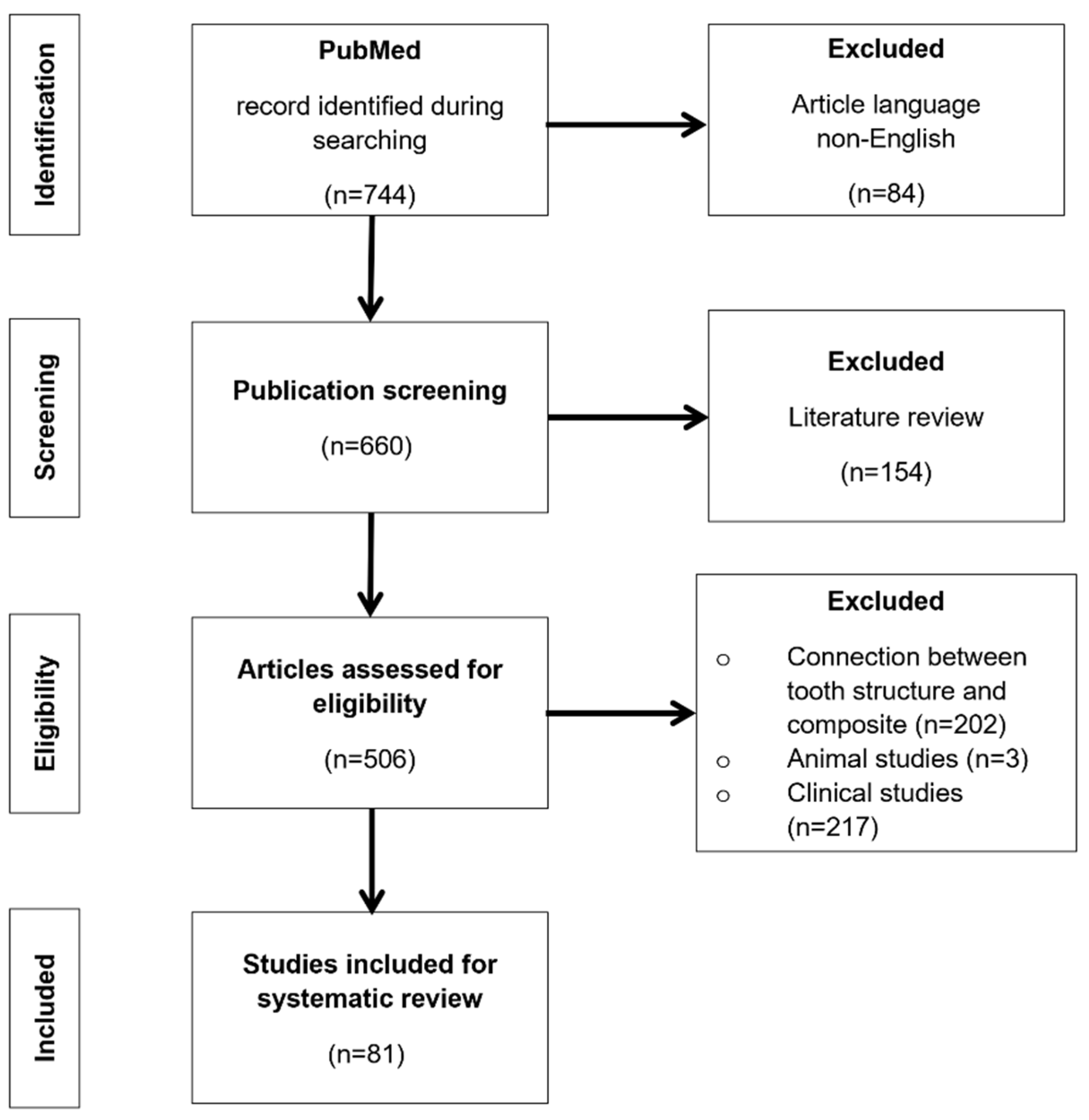
2. Methodology
3. Study
3.1. Principles of Connections and Connection Strength
3.2. Composite Systems for Dental Restorations and Methodology of Establishing a Connection
3.3. Additives for Composite Systems
4. Establishing Connections between Composite Systems and Other Materials
4.1. Connection to Zirconium Oxide
4.2. Connections between Two Composites
4.3. Connection to Feldspar Ceramics (Silicates)
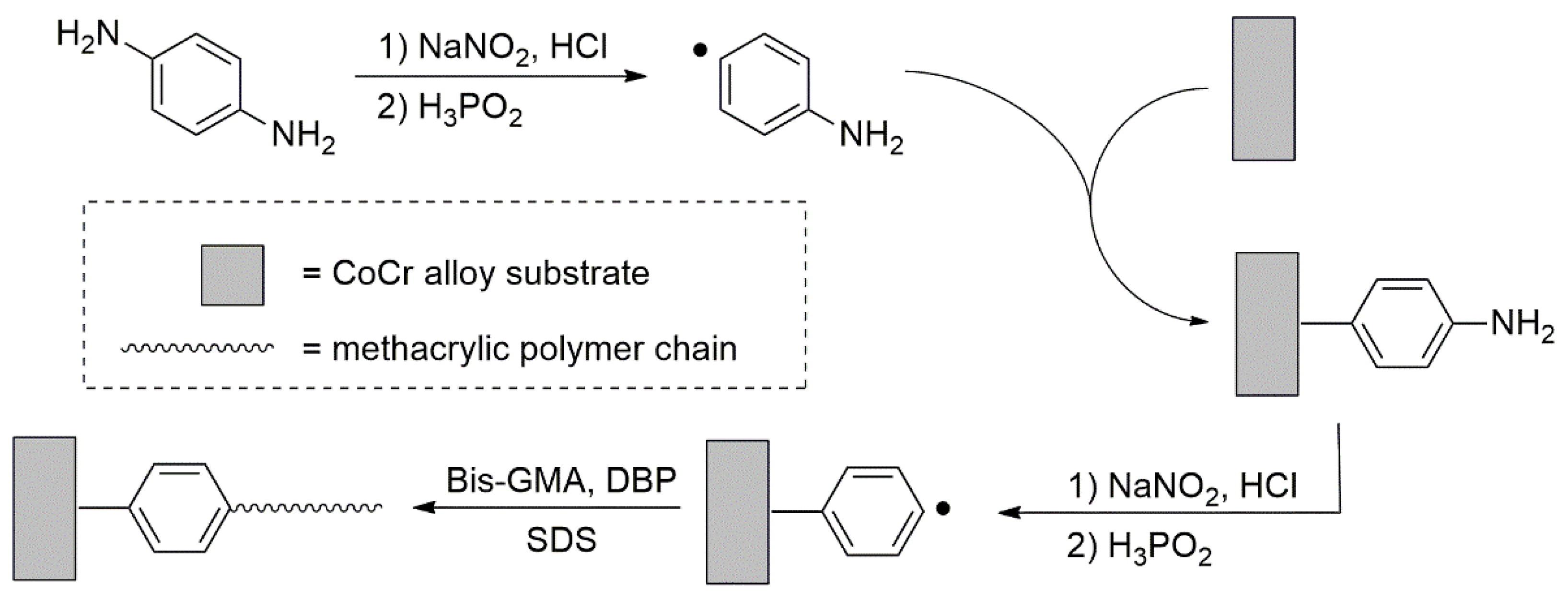
4.4. Adhesion to Non-Precious Metals
4.5. Adhesion to Precious Metal Alloys
4.6. Silanes as Adhesion Promoters
4.7. Functional Methacrylic Monomers
4.7.1. 10-MDP–10-(methacryloyloxy)decyl Dihydrogen Phosphate
4.7.2. 4-MET–4-(2-Methacryloyloxyethyl) Trimellitic Acid Monoester
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 134. [Google Scholar] [CrossRef] [PubMed]
- Hazem, A.S. Dental Composite Properties Evaluation: From Experimental Approaches to the Prerequisite of a Chewing Bench, Human Health and Pathology; Université de Lyon: Lyon, France, 2017. [Google Scholar]
- Iftikhar, S.; Jahanzeb, N.; Saleem, M.; Ur, R.S.; Matinlinna, J.P.; Khan, A.S. The trends of dental biomaterials research and future directions: A mapping review. Saudi Dent. J. 2021, 33, 229–238. [Google Scholar] [CrossRef] [PubMed]
- John, K.R.S. Biocompatibility of Dental Materials. Dent. Clin. N. Am. 2007, 51, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.R.; Zheng, J. Tribology of dental materials: A review. J. Phys. D Appl. Phys. 2008, 41, 113001. [Google Scholar] [CrossRef]
- Vaderhobli, R.M. Advances in Dental Materials. Dent. Clin. N. Am. 2011, 55, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, H.R.; Rizi, H.B.; Khamseh, M.M.R.; Öchsner, A. A Review on Dental Materials; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Condò, R.; Mampieri, G.; Cioffi, A.; Cataldi, M.E.; Frustaci, I.; Giancotti, A.; Campanella, V.; Mussi, V.; Convertino, A.; Maiolo, L.; et al. Physical and chemical mechanisms involved in adhesion of orthodontic bonding composites: In vitro evaluations. BMC Oral Health 2021, 16, 350. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Zhang, H.; Yang, J.; Chen, C. Evaluating the Bonding Performance of a Novel Dual-curing Composite Cement to Zirconia. J. Adhes. Dent. 2021, 23, 569–578. [Google Scholar] [CrossRef]
- Deprá, M.B.; De Almeida, J.X.; da Cunha Tde, M.; Lon, L.F.; Retamoso, L.B.; Tanaka, O.M. Effect of saliva contamination on bond strength with a hydrophilic composite resin. Dent. Press J. Orthod. 2013, 18, 63–68. [Google Scholar] [CrossRef]
- Piest, C.; Wille, S.; Strunskus, T.; Polonskyi, O.; Kern, M. Efficacy of Plasma Treatment for Decontaminating Zirconia. J. Adhes. Dent. 2018, 20, 289–297. [Google Scholar] [CrossRef]
- Güers, P.; Wille, S.; Strunskus, T.; Polonskyi, O.; Kern, M. Durability of resin bonding to zirconia ceramic after contamination and the use of various cleaning methods. Dent. Mater. 2019, 35, 1388–1396. [Google Scholar] [CrossRef]
- Uno, M.; Kawaki, H.; Ishigami, H.; Yokogawa, Y.; Doi, Y. Effects of silica sputtering on adhesion between zirconia and composite resin cores. Dent. Mater. J. 2021, 40, 1014–1019. [Google Scholar] [CrossRef]
- Hammad, S.M.; El Banna, M.S. Effects of cyclic loading on the shear bond strength of metal orthodontic brackets bonded to resin composite veneer surface using different conditioning protocols. Prog. Orthod. 2013, 14, 14. [Google Scholar] [CrossRef]
- Alovisi, M.; Scotti, N.; Comba, A.; Manzon, E.; Farina, E.; Pasqualini, D.; Michelotto Tempesta, R.; Breschi, L.; Cadenaro, M. Influence of polymerization time on properties of dual-curing cements in combination with high translucency monolithic zirconia. J. Prosthodont. Res. 2018, 62, 468–472. [Google Scholar] [CrossRef]
- Sabatini, C.; Patel, M.; D’Silva, E. In vitro shear bond strength of three self-adhesive resin cements and a resin-modified glass ionomer cement to various prosthodontic substrates. Oper. Dent. 2013, 38, 186–196. [Google Scholar] [CrossRef]
- Ona, M.; Wakabayashi, N.; Yamazaki, T.; Takaichi, A.; Igarashi, Y. The influence of elastic modulus mismatch between tooth and post and core restorations on root fracture. Int. Endod. J. 2013, 46, 47–52. [Google Scholar] [CrossRef]
- Costa, A.R.; Vedovello-Filho, M.; Correr, A.B.; Vedovello, S.A.; Puppin-Rontani, R.M.; Ogliari, F.A.; Moraes, R.R.; Correr-Sobrinho, L. Bonding orthodontics brackets to enamel using experimental composites with an iodonium salt. Eur. J. Orthod. 2014, 36, 297–302. [Google Scholar] [CrossRef][Green Version]
- Magne, P.; Malta, D.A.; Enciso, R.; Monteiro-Junior, S. Heat Treatment Influences Monomer Conversion and Bond Strength of Indirect Composite Resin Restorations. J. Adhes. Dent. 2015, 17, 559–566. [Google Scholar] [CrossRef]
- Carrilho, E.; Cardoso, M.; Ferreira, M.M.; Marto, C.M.; Paula, A.; Coelho, A.S. 10-MDP Based Dental Adhesives: Adhesive Interface Characterization and Adhesive Stability—A Systematic Review. Materials 2019, 12, 790. [Google Scholar] [CrossRef]
- Wang, R.; Shi, Y.; Li, T.; Pan, Y.; Cui, Y.; Xia, W. Adhesive interfacial characteristics and the related bonding performance of four self-etching adhesives with different functional monomers applied to dentin. J. Dent. 2017, 62, 72–80. [Google Scholar] [CrossRef]
- Eliades, A.; Birpou, E.; Eliades, T.; Eliades, G. Self-adhesive restoratives as pit and fissure sealants: A comparative laboratory study. Dent. Mater. 2013, 29, 752–762. [Google Scholar] [CrossRef]
- Papadogiannis, D.; Dimitriadi, M.; Zafiropoulou, M. Universal Adhesives: Setting Characteristics and Reactivity with Dentin. Materials 2019, 12, 1720. [Google Scholar] [CrossRef] [PubMed]
- Rahul, M.; Kumar, P.A.; Nair, A.S.; Mathew, S.; Amaladas, A.S.; Ommen, A. Effects of at-home and in-office bleaching agents on the shear bond strength of metal, ceramic, and composite brackets to enamel. Indian J. Dent Res. 2017, 28, 566–573. [Google Scholar] [PubMed]
- Fatemeh, K.; Mohammad Javad, M.; Samaneh, K. The effect of silver nanoparticles on composite shear bond strength to dentin with different adhesion protocols. J. Appl. Oral Sci. 2017, 25, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.A.; Cheng, L.; Zhang, K.; Weir, M.D.; Rodrigues, L.K.; Xu, H.H. Novel dental adhesives containing nanoparticles of silver and amorphous calcium phosphate. Dent. Mater. 2013, 29, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Behnaz, M.; Dalaie, K.; Mirmohammadsadeghi, H.; Salehi, H.; Rakhshan, V.; Aslani, F. Shear bond strength and adhesive remnant index of orthodontic brackets bonded to enamel using adhesive systems mixed with TiO2 nanoparticles. Dent. Press J. Orthod. 2018, 23, 43.e1–43.e7. [Google Scholar] [CrossRef] [PubMed]
- Kotta, M.; Gorantla, S.; Muddada, V.; Lenka, R.R.; Karri, T.; Kumar, S.; Tivanani, M. Antibacterial activity and debonding force of different lingual retainers bonded with conventional composite and nanoparticle containing composite: An in vitro study. J. World Fed. Orthod. 2020, 9, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Abbatepaulo, G.L.; Gangana, T.M.M.C.; Martinez, E.F.; Turssi, C.P.; França, F.M.G.; Amaral, F.L.B.; Basting, R.T. TiF4 Incorporated into a Self-etching Primer in Different Concentrations: Antimicrobial Properties and Effects on Demineralisation Inhibition Around the Restoration/Enamel-Dentin Interface. Oral Health Prev. Dent. 2019, 17, 57–67. [Google Scholar] [CrossRef]
- Jowkar, Z.; Farpour, N.; Koohpeima, F.; Mokhtari, M.J.; Shafiei, F. Effect of Silver Nanoparticles, Zinc Oxide Nanoparticles and Titanium Dioxide Nanoparticles on Microshear Bond Strength to Enamel and Dentin. J. Contemp. Dent. Pract. 2018, 19, 1404–1411. [Google Scholar]
- Rubin Cocco, A.; de Oliveira da Rosa, W.L.; Luque Peralta, S.; Timm Maske, T.; da Silva, A.F.; Andrade Hartwig, C.; Foster Mesko, M.; Piva, E.; Guerra Lund, R. New adhesive system based in metals cross-linking methacrylate. J. Mech. Behav. Biomed. Mater. 2018, 77, 519–526. [Google Scholar] [CrossRef]
- Li, R.; Wang, C.; Ma, S.Q.; Liu, Z.H.; Zang, C.C.; Zhang, W.Y.; Sun, Y.C. High bonding strength between zirconia and composite resin based on combined surface treatment for dental restorations. J. Appl. Biomater. Funct. Mater. 2020, 18, 8655. [Google Scholar] [CrossRef]
- Mehari, K.; Parke, A.S.; Gallardo, F.F.; Vandewalle, K.S. Assessing the Effects of Air Abrasion with Aluminum Oxide or Glass Beads to Zirconia on the Bond Strength of Cement. J. Contemp. Dent. Pract. 2020, 21, 713–717. [Google Scholar]
- Tanış, M.C.; Akay, C.; Şen, M. Effect of selective infiltration etching on the bond strength between zirconia and resin luting agents. J. Esthet. Restor. Dent. 2019, 31, 257–262. [Google Scholar] [CrossRef]
- Al-Akhali, M.; Al-Dobaei, E.; Wille, S.; Mourshed, B.; Kern, M. Influence of elapsed time between airborne-particle abrasion and bonding to zirconia bond strength. Dent. Mater. 2021, 37, 516–522. [Google Scholar] [CrossRef]
- Shimoe, S.; Peng, T.; Otaku, M.; Tsumura, N.; Satoda, S.I.T. Influence of various airborne-particle abrasion conditions on bonding between zirconia ceramics and an indirect composite resin material. J. Prosthet. Dent. 2019, 122, 491.e1–491.e9. [Google Scholar] [CrossRef]
- Grasel, R.; Santos, M.J.; Hm Rêgo, H.C.h.; Rippe, M.P.; Valandro, L.F. Effect of Resin Luting Systems and Alumina Particle Air Abrasion on Bond Strength to Zirconia. Oper. Dent. 2018, 43, 282–290. [Google Scholar] [CrossRef]
- Altan, B.; Cinar, S.; Tuncelli, B. Evaluation of shear bond strength of zirconia-based monolithic CAD-CAM materials to resin cement after different surface treatments. Niger. J. Clin. Pract. 2019, 22, 1475–1482. [Google Scholar] [CrossRef]
- Ruales-Carrera, E.; Cesar, P.F.; Henriques, B.; Fredel, M.C.; Özcan, M.; Volpato, C.A.M. Adhesion behavior of conventional and high-translucent zirconia: Effect of surface conditioning methods and aging using an experimental methodology. J. Esthet. Restor. Dent. 2019, 31, 388–397. [Google Scholar] [CrossRef]
- Chen, B.; Yan, Y.; Xie, H.; Meng, H.; Zhang, H.; Chen, C.H. Effects of Tribochemical Silica Coating and Alumina-Particle Air Abrasion on 3Y-TZP and 5Y-TZP: Evaluation of Surface Hardness, Roughness, Bonding, and Phase Transformation. J. Adhes. Dent. 2020, 22, 373–382. [Google Scholar] [CrossRef]
- Iwasaki, T.; Komine, F.; Fushiki, R.; Kubochi, K.; Shinohara, M.; Matsumura, H. Shear bond strengths of an indirect composite layering material to a tribochemically silica-coated zirconia framework material. Dent. Mater. J. 2016, 35, 461–469. [Google Scholar] [CrossRef]
- Otani, A.S.; Amaral, M.; May, L.G.; Cesar, P.F.; Valandro, L.F. A critical evaluation of bond strength tests for the assessment of bonding to Y-TZP. Dent Mater. 2015, 31, 648–656. [Google Scholar] [CrossRef]
- Cadore-Rodrigues, A.C.; Prochnow, C.; Burgo, T.A.L.; Oliveira, J.S.; Jahn, S.L.; Foletto, E.L.; Rippe, M.P.; Pereira, G.K.R.; Valandro, L.F. Stable Resin Bonding to Y-TZP Ceramic with Air Abrasion by Alumina Particles Containing 7% Silica. J. Adhes. Dent. 2020, 22, 149–159. [Google Scholar] [CrossRef]
- Libecki, W.; Elsayed, A.; Lehmann, F.; Kern, M. Efficacy of Different Surface Treatments for Intraoral Repair of Veneered Zirconia Frameworks. J. Adhes. Dent. 2017, 19, 323–329. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Ragab, H.; Arnaot, M. Ultrastructural Analysis and Long-term Evaluation of Composite-Zirconia Bond Strength. J. Adhes. Dent. 2018, 20, 33–39. [Google Scholar] [CrossRef]
- Fushiki, R.; Komine, F.; Blatz, M.B.; Koizuka, M.; Taguchi, K.; Matsumura, H. Shear bond strength between an indirect composite layering material and feldspathic porcelain-coated zirconia ceramics. Clin. Oral Investig. 2012, 16, 1401–1411. [Google Scholar] [CrossRef]
- Noro, A.; Kameyama, A.; Haruyama, A.; Takahashi, T. Influence of hydrophilic pre-treatment on resin bonding to zirconia ceramics. Bull. Tokyo Dent. Coll. 2015, 56, 33–39. [Google Scholar] [CrossRef]
- Egoshi, T.; Taira, Y.; Sakihara, M.; Kamada, K.; Sawase, T.; Murata, H. Effects of air abrasion and glow-discharge plasma treatment on bonding resin cement to ceria-stabilized zirconia/alumina nanocomposite. Dent. Mater. J. 2019, 38, 437–443. [Google Scholar] [CrossRef]
- Lümkemann, N.; Eichberger, M.; Stawarczyk, B. Different surface modifications combined with universal adhesives: The impact on the bonding properties of zirconia to composite resin cement. Clin. Oral Investig. 2019, 23, 3941–3950. [Google Scholar] [CrossRef]
- Elias, A.B.; Simão, R.A.; Prado, M.; Cesar, P.F.; Botelho Dos Santos, G.; Moreira da Silva, E. Effect of different times of nonthermal argon plasma treatment on the microtensile bond strength of self-adhesive resin cement to yttria-stabilized tetragonal zirconia polycrystal ceramic. J. Prosthet. Dent. 2019, 121, 485–491. [Google Scholar] [CrossRef]
- Barquete, C.G.; Simão, R.A.; Almeida Fonseca, S.S.; Elias, A.B.; Antunes Guimarães, J.G.; Herrera, E.Z.; Mello, A.; Moreira da Silva, E. Effect of cementation delay on bonding of self-adhesive resin cement to yttria-stabilized tetragonal zirconia polycrystal ceramic treated with nonthermal argon plasma. J. Prosthet. Dent. 2021, 125, 693.e1–693.e7. [Google Scholar] [CrossRef]
- Piascik, J.R.; Swift, E.J.; Braswell, K.; Stoner, B.R. Surface fluorination of zirconia: Adhesive bond strength comparison to commercial primers. Dent. Mater. 2012, 28, 604–608. [Google Scholar] [CrossRef]
- Su, Z.; Li, M.; Zhang, L.; Wang, C.; Zhang, L.; Xu, J.; Fu, B. A novel porous silica-zirconia coating for improving bond performance of dental zirconia. J. Zhejiang Univ. Sci. B. 2021, 22, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Park, S.W.; Lee, K.; Oh, G.J.; Lim, H.P. Shear bond strength between resin cement and colored zirconia made with metal chlorides. J. Prosthet. Dent. 2015, 113, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, Z.; Qian, M.; Zhang, H.; Xie, H.; Chen, C. Effect of 10-Methacryloxydecyl Dihydrogen Phosphate Concentration on Chemical Coupling of Methacrylate Resin to Yttria-stabilized Zirconia. J. Adhes. Dent. 2017, 19, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Lin, J.C.; Kang, L.L.; Li, C.L.; Hou, S.S.; Lee, T.L.; Chuang, S.F. Investigations of silane-MDP interaction in universal adhesives: A ToF-SIMS analysis. Dent. Mater. 2022, 38, 183–193. [Google Scholar] [CrossRef]
- Zarif, N.H.; Mousavi, M.; Nouri, N.; Torkan, S. Evaluation of the effect of different surface conditioning methods on shear bond strength of metal brackets bonded to aged composite restorations. Int. Orthod. 2019, 17, 80–88. [Google Scholar] [CrossRef]
- Espinar-Escalona, E.; Barrera-Mora, J.M.; Llamas-Carreras, J.M.; Solano-Reina, E.; Rodríguez, D.; Gil, F.J. Improvement in adhesion of the brackets to the tooth by sandblasting treatment. J. Mater. Sci. Mater. Med. 2012, 23, 605–611. [Google Scholar] [CrossRef]
- Sobouti, F.; Dadgar, S.; Sanikhaatam, Z.; Nateghian, N.; Saravi, M.G. Effects of two erbium-doped yttrium aluminum garnet lasers and conventional treatments as composite surface abrasives on the shear bond strength of metal brackets bonded to composite resins. J. Orthodont. Sci. 2016, 5, 18–24. [Google Scholar]
- Shaymaa, E.E. Influence of surface treatments on bond strength of metal and ceramic brackets to a novel CAD/CAM hybrid ceramic material. Odontology 2016, 104, 68–76. [Google Scholar] [CrossRef]
- Park, H.; Cho, J.H.; Jung, J.H.; Duy, P.P. A Review of Wet Chemical Etching of Glasses in Hydrofluoric Acid based Solution for Thin Film Silicon Solar Cell Application. Curr. Photovolt. Res. 2017, 5, 75–82. [Google Scholar] [CrossRef]
- Pompeo, D.D.; Rosário, H.D.; Lopes, B.M.; Cesar, P.F.; Paranhos, L.R. Can 10% hydrofluoric acid be used for reconditioning of orthodontic brackets? Indian J. Dent. Res. 2016, 27, 383–387. [Google Scholar] [CrossRef]
- Komine, F.; Kubochi, K.; Kimura, F.; Kusaba, K.; Takano, R.; Matsumura, H. Shear bond strength between gingival composite resin and glazed gingival porcelain for implant-supported prostheses. Eur. J. Oral. Sci. 2021, 129, e12762. [Google Scholar] [CrossRef]
- Leyva Del Rio, D.; Sandoval-Sanchez, E.; Campos-Villegas, N.E.; Azpiazu-Flores, F.X.; Zavala-Alonso, N.V. Influence of Heated Hydrofluoric Acid Surface Treatment on Surface Roughness and Bond Strength to Feldspathic Ceramics and Lithium-Disilicate Glass-Ceramics. J. Adhes. Dent. 2021, 23, 549–555. [Google Scholar] [CrossRef]
- Koko, M.; Takagaki, T.; Abdou, A.; Inokoshi, M.; Ikeda, M.; Wada, T.; Uo, M.; Nikaido, T.; Tagami, J. Effects of the ratio of silane to 10-methacryloyloxydecyl dihydrogenphosphate (MDP) in primer on bonding performance of silica-based and zirconia ceramics. J. Mech. Behav. Biomed. Mater. 2020, 112, 104026. [Google Scholar] [CrossRef]
- Patil, S.S.; Kontham, U.R.; Kamath, A.; Kontham, R. Shear bond strength of composite resin bonded to preformed metal crowns for primary molars using a universal adhesive and two different surface treatments: An in vitro study. Eur. Arch. Paediatr. Dent. 2016, 17, 377–380. [Google Scholar] [CrossRef]
- Madani, A.S.; Astaneh, P.A.; Nakhaei, M.; Bagheri, H.G.; Moosavi, H.; Alavi, S.; Najjaran, N.T. Effectiveness of silica-lasing method on the bond strength of composite resin repair to Ni-Cr alloy. J. Prosthodont. 2015, 24, 225–232. [Google Scholar] [CrossRef]
- Kamada, K.; Taira, Y.; Sumi, T.; Sawase, T. Retention strength between veneering resin composites and laser-sintered cobalt-chromium alloy. Odontology 2017, 105, 23–28. [Google Scholar] [CrossRef]
- Kawashima, S.; Nagai, Y.; Shinkai, K. Effect of silane coupling treatment and airborne-particle abrasion on shear bond strength between photo-cured bulk-fill flowable composite resin and silverpalladium-copper-gold alloy using self-adhesive resin cement. Dent. Mater. J. 2019, 38, 418–423. [Google Scholar] [CrossRef]
- Hattan, M.A.; Pani, S.C.; Alomari, M. Composite bonding to stainless steel crowns using a new universal bonding and single-bottle systems. Int. J. Dent. 2013, 2013, 607405. [Google Scholar] [CrossRef]
- Almilhatti, H.J.; Neppelenbroek, K.H.; Vergani, C.E.; Machado, A.L.; Pavarina, A.C.; Giampaolo, E.T. Adhesive bonding of resin composite to various titanium surfaces using different metal conditioners and a surface modification system. J. Appl. Oral. Sci. 2013, 21, 590–596. [Google Scholar] [CrossRef]
- Taira, Y.; Egoshi, T.; Kamada, K.; Sawase, T. Surface modification with alumina blasting and H2SO4-HCl etching for bonding two resin-composite veneers to titanium. Eur. J. Oral. Sci. 2014, 122, 84–88. [Google Scholar] [CrossRef]
- Lung, C.Y.; Liu, D.; Matinlinna, J.P. Surface treatment of titanium by a polydimethylsiloxane coating on bond strength of resin to titanium. J. Mech. Behav. Biomed. Mater. 2015, 41, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kawaguchi, T.; Ikeda, H.; Karntiang, P.; Kakura, K.; Taniguchi, Y.; Toyoda, K.; Shimizu, H.; Kido, H. Bond durability and surface states of titanium, Ti-6Al-4V alloy, and zirconia for implant materials. J. Prosthodont. Res. 2022, 66, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.G.; Ko, K.H.; Park, C.J.; Cho, L.R.; Huh, Y.H. Composite Cement Components Stabilize the Bond between a Lithium-Disilicate Glass-Ceramic and the Titanium Abutment. J. Adhes. Dent. 2021, 23, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Oweis, Y.; Alageel, O.; Kozak, P.; Abdallah, M.N.; Retrouvey, J.M.; Cerruti, M.; Tamimi, F. Metal-composite adhesion based on diazonium chemistry. Dent. Mater. 2017, 33, e393–e404. [Google Scholar] [CrossRef]
- Baeza-Robleto, S.J.; Villa-Negrete, D.M.; García-Contreras, R.; Scougall-Vílchis, R.J.; Guadarrama-Quiroz, L.J.; Robles-Bermeo, N.L. Effects of ultraviolet irradiation on the bond strength of a composite resin adhered to stainless steel crowns. Pediatr. Dent. 2013, 35, 23–26. [Google Scholar]
- Kiatsirirote, K.; Northeast, S.E.; van Noort, R. Bonding procedures for intraoral repair of exposed metal with resin composite. J. Adhes. Dent. 2012, 4, 315–321. [Google Scholar]
- Lee, Y.; Kim, K.H.; Kim, Y.K.; Son, J.S.; Lee, E.; Kwon, T.Y. The Effect of Novel Mercapto Silane Systems on Resin Bond Strength to Dental Noble Metal Alloys. J. Nanosci. Nanotechnol. 2015, 15, 4851–4854. [Google Scholar] [CrossRef]
- Pilo, R.; Brosh, T.; Geron, V.; Levartovsky, S.; Eliades, G. Effect of Silane Reaction Time on the Repair of a Nanofilled Composite Using Tribochemical Treatment. J. Adhes. Dent. 2016, 18, 125–134. [Google Scholar] [CrossRef]
- Lung, C.Y.; Kukk, E.; Matinlinna, J.P. Shear bond strength between resin and zirconia with two different silane blends. Acta Odontol. Scand. 2012, 70, 405–413. [Google Scholar] [CrossRef]
- Zhou, J.; Wurihan Shibata, Y.; Tanaka, R.; Zhang, Z.; Zheng, K.; Li, Q.; Ikeda, S.; Gao, P.; Miyazaki, T. Quantitative/qualitative analysis of adhesive-dentin interface in the presence of 10-methacryloyloxydecyl dihydrogen phosphate. J. Mech. Behav. Biomed. Mater. 2019, 92, 71–78. [Google Scholar] [CrossRef]
- Komura, I.; Yamauchi, J.; Nagase, Y.; Uemura, F. Production of Phosphoric Monoester. JPS59139392A, 10 August 1984. [Google Scholar]
- Llerena-Icochea, A.E.; Costa, R.M.; Borges, A.; Bombonatti, J.; Furuse, A.Y. Bonding Polycrystalline Zirconia With 10-MDP-containing Adhesives. Oper. Dent. 2017, 42, 335–341. [Google Scholar] [CrossRef]
- Tsuchimoto, Y.; Yoshida, Y.; Mine, A.; Nakamura, M.; Nishiyama, N.; Van Meerbeek, B.; Suzuki, K.; Kuboki, T. Effect of 4-MET- and 10-MDP-based primers on resin bonding to titanium. Dent. Mater. J. 2016, 25, 120–124. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raszewski, Z.; Brząkalski, D.; Derpeński, Ł.; Jałbrzykowski, M.; Przekop, R.E. Aspects and Principles of Material Connections in Restorative Dentistry—A Comprehensive Review. Materials 2022, 15, 7131. https://doi.org/10.3390/ma15207131
Raszewski Z, Brząkalski D, Derpeński Ł, Jałbrzykowski M, Przekop RE. Aspects and Principles of Material Connections in Restorative Dentistry—A Comprehensive Review. Materials. 2022; 15(20):7131. https://doi.org/10.3390/ma15207131
Chicago/Turabian StyleRaszewski, Zbigniew, Dariusz Brząkalski, Łukasz Derpeński, Marek Jałbrzykowski, and Robert E. Przekop. 2022. "Aspects and Principles of Material Connections in Restorative Dentistry—A Comprehensive Review" Materials 15, no. 20: 7131. https://doi.org/10.3390/ma15207131
APA StyleRaszewski, Z., Brząkalski, D., Derpeński, Ł., Jałbrzykowski, M., & Przekop, R. E. (2022). Aspects and Principles of Material Connections in Restorative Dentistry—A Comprehensive Review. Materials, 15(20), 7131. https://doi.org/10.3390/ma15207131