1. Introduction
Healthcare buildings are major energy consumers, representing 6% of the total energy consumption in the service sector [
1]. These healthcare buildings encompass small clinics, health centers and large hospitals, and they are characterized by a high occupancy, high-energy consumption per area and strict air indoor quality (IAQ) requirements. Heating, ventilation and air conditioning (HVAC) systems are the major contributors [
1,
2]. In Spain, HVAC systems represent 40% of energy use in hospitals [
3]. In addition, hospitals account for 9% of all thermal and electrical consumption of the service sector in Spain [
4]. Therefore, the energy saving potential is large. However, this high-energy consumption stays in the background, prioritizing other issues such as safety, IAQ conditions and comfortable environment. The HVAC systems in buildings are designed to maintain adequate thermal comfort conditions and appropriate air quality [
5]. These conditions acquire special relevance in the surgical suites of a hospital, especially in operating rooms (ORs). They must be kept within limits that allow minimizing the risks of infections, preventing the growth and spread of bacteria and viruses, and maximizing the comfort of patients and health staff. The environment must remain aseptic, preventing any risk of cross-contamination [
6]. The most effective way to control these conditions is the application of ventilation systems [
7] that maintain high air changes per hour (ACH), as the adequate distribution of clean air allows the isolation and dilution of infectious particles in ORs [
8].
The environmental conditions of temperature, relative humidity, concentration of pathogenic particles and concentration of residual gases, coming from the anesthesia of the patient or other surgical procedures, within an OR are strictly delimited by international and national regulations, in order to guarantee the asepsis and comfort indoors. In particular, in Spain, the UNE 100713: 2005 standard, about air conditioning in hospital, establishes the requirements of HVAC systems in hospitals in relation to ventilation, indicating the minimum ACH [
9]. In turn, the international standard, ISO 14644-1: 2015, establishes a classification of cleanrooms according to the type of surgeries carried out, and sets ventilation conditions to guarantee low levels of pathogenic particle concentration [
10]. Recommended indoor conditions for ORs are different depending on the country considered. González et al. [
11] describe in their work different conditions for several countries. In particular, ORs in Spain must be maintained with ventilation rate of 20 ACH or 2400 m
3/h [
9]. On the other hand, the standard UNE 171340: 2012
“Validation and evaluation of controlled environment rooms in hospitals” aims to establish some fundamental control principles, criteria and a testing methodology, including its periodicity, with a standardize system, to validate the proper functioning of the controlled environment rooms in health centers [
12].
Several authors have studied energy efficiency in hospitals [
1,
3,
13,
14,
15]. Some practical recommendations for energy savings in hospitals are evaluated in [
15]. González-González et al. [
3] studied 20 hospitals in Spain to find a correlation between gross domestic product (GDP), number of beds, number of people, hospital surface area, energy use and weather conditions. García-Sanz-Calcedo et al. [
13] evaluated 70 health centers in Spain and revealed relationships between morphological and functional parameters with their energy consumption and emissions. A review about HVAC systems in hospitals [
1] revealed that variable refrigerant flow (VRF) technology allows higher energy and cost savings compared to conventional HVAC systems. Nevertheless, to determine energy savings in a hospital, first, an accurate calculation of energy consumption has to be made. Congradac et al. [
14] created a mathematical tool for the accurate calculation of energy demands in hospitals. Implementing simple energy conservation measures (ECM) in hospitals can save up to 10% of energy consumption [
15]. However, there are few studies about energy efficiency focused on surgical suites and ORs even though they are the biggest consumers, and therefore, they have a greater capacity for improvement [
5,
11,
16,
17]. In addition, the works carried out are primarily focused on ventilation systems [
5,
17], as guidelines for ORs require keeping them at overpressure with respect to adjacent rooms, but do not suggest a specific ventilation strategy to address this issue [
18]. The standards define limits for temperatures, relative humidity, ACH, types of filters, air pressure in relation to adjacent areas and the cases when the air may be recirculated [
19]. Within the IAQ in ORs, the concentration of airborne particles takes on special importance. One of the objectives of this study is the in-depth analysis of the regulations in this regard, the limits established in terms of different scenarios and the latest studies related to particles. Therefore, the state of the art of airborne particles is presented in detail in
Section 2.
Everything indicates, therefore, that there is considerable scope for improving the energy efficiency in surgical suites by decreasing their ventilation loads, but keeping standards. The main objective of the present work is to propose a methodology to assess conditions and to determine potential energy savings by reducing ventilation flow rates, without compromising patient and health staff safety or IAQ, and complying with national and international standards and codes. A dynamic energy model and a particle model were built and simulated using TRNSYS. Then, models were calibrated with the optimization tool GenOpt. The results were validated by the implementation of a continuous monitoring campaign collecting experimental data. The main novelties of this study are its originality, its multidisciplinary capacity and its accessible, exportable methodology applicable to any other area in the hospital. This would allow a holistic view of potential savings.
The structure of the paper is the following. The article starts with an introduction to the topic of energy efficiency in hospitals, specifically in ORs. Then, a section about state of the art of airborne particles in ORs is presented, describing details of the Spanish regulation. Next, materials and methods are explained, the description of the surgical area and the OR studied, the experimental setup and the dynamic energy and particle model simulated using TRNSYS and calibrated with GenOpt. Then, experimental and simulated results are discussed. Finally, some conclusions are presented.
2. State of the Art of Airborne Particles in Operating Rooms: The Case in Spain
The final energy consumption in Spain in 2016 was 82,333 ktoe, of which 10,627 ktoe (12.9%) corresponds to consumption in the service sector, where hospitals belong. Assuming that the consumption in these buildings is 1067 ktoe (1.3%), the thermal energy results in 549 ktoe [
20]. The studied hospital is located in Galicia, a northern area of Spain. In 2016, the energy consumption in the Galician Health Service was 28.09 ktoe, of which the thermal energy consumption was 14.55 ktoe. The thermal energy demand in hospitals occurs mainly in HVAC systems. These facilities of complex design must respond not only to the requirements of the comfort conditions of users and workers, which in the case of Spain are defined in the RITE (Regulation of thermal installations in buildings) [
21], but also to environmental safety conditions. The UNE 100713: 2005 standard [
9] establishes the specific conditions that must govern air conditioning installations in hospitals in terms of thermal comfort and air quality, defining the requirements in terms of airflow, temperature, humidity and sound pressure in each of the units, and the flow directions in the ORs and filtration levels.
Particle concentration is regulated by national and international standards. The international standard ISO 14644-1: 2015 [
10] establishes a classification of clean rooms to control pollution by particles transported by air, based on their size (from 0.1 μm to 5 μm) and their quantification. It is used for the control of industrial processes, pharmacological processes and in health services. This standard establishes the maximum allowable concentrations for particles considering particle sizes and considering “ISO Class number”. The standard UNE 171340: 2012 establishes this classification of spaces [
12]. It validates the controlled environment rooms in hospitals, including ORs. It establishes a classification according to their risks, types of ventilation and associated filtration. This classification establishes that the transplant ORs, placement of prostheses, etc. are considered very high-risk areas, and conventional surgery ORs are considered high-risk areas. The validation of the rooms is done by analyzing several environmental parameters such as temperature, relative humidity, microbiology, particles, noise, and other installation parameters such as differential pressure, absolute filter placement, airflow rates, ACH, airflow direction and recovery of the room. The room classification test is especially relevant. It is based on determining the cleanliness of the room by counting airborne particles as indicated in ISO 14644-1: 2015. The classification is the following: ISO 5 - ISO 6 for A-class ORs or high technology and very high risk areas, ISO 7 for B-class ORs and high risk areas, and ISO 8 for C-class ORs and medium risk areas. These established limits can be observed in
Table 1.
This set of standards determines the need to control and ensure the environmental and thermal comfort conditions of hospitals but mainly to reduce or minimize the possibility of contracting nosocomial infections in clinical events. To meet these conditions, the requirements of the standards go beyond those required for a conventional building, significantly influencing the increase in energy demand ratios compared to the latter. In the scientific literature it has not been proven that there is a direct relationship between the number of particles present in an OR and the degree of microbial contamination in the OR, although from a statistical point of view the probability of finding microbial agents increases in rooms with a high concentration of particles [
22].
Some authors have studied particles in hospitals. Appropriate ventilation is necessary for isolating and decreasing airborne particles in a hospital OR [
23]. The ventilation system of an OR is usually placed over the operating table, with downward flow, using high efficiency particulate air (HEPA) filtering and ultra-low particulate air (ULPA) filters to maintain low particle concentrations [
24,
25]. Regarding particles, in an OR, many variables have to be taken into account. A walking person has an emission ratio of approximately 10,000 particles in a minute, with a size between 2.5 μm and 20 μm; moreover, between 5% and 10% of these particles can transport bacteria [
24]. On the other hand, a standing person can release up to 1000 particles in a minute [
24]. Other authors have considered that the medical staff emit between 200 and 400 particles carrying bacteria per minute of an average size of 6 μm [
7,
26]. The patient receives a process of superficial sterilization much more exhaustive than the medical staff, and the patient movement during the operation is minimal, the reason why it is disregarded as a source of particles. In addition, to study particle concentration, obstacles and sources of heat have to be identified, as well as the speed of entry and the percentage of recirculated air. Chow et al. [
24] analyzed the airflow inside an OR and reduced the airflow to 50% during the hours of inactivity to increase energy efficiency. Rui et al. [
26] analyzed the movement of bacteria carrying particles in two ORs with ISO 5 and ISO 6 classifications using computational fluids dynamics (CFD). Liu et al. [
7] simulated airborne particles in an OR with horizontal airflow and concluded that maintaining a low particle concentration around the patient is associated with the distribution of the OR and the position of the source, making sure that this source of particles is in a downstream position of the wound area. CFD was also used to explore the influence of lamps and human body surface temperatures on particle distribution and concentration, simulating the movement of the airborne particle of size 5 μm [
23]. Results of CFD simulations demonstrate that when the surgical lamp is 45 °C and staff surface temperatures are 37 °C, more particles appear on the floor of the operating table. On average, the particle concentration in the area of the operating table rises by 16% [
23]. CFD can be used to analyze the airborne particle concentration, and Kircher et al. [
25] used TRNSYS, achieving less than 8% error in results. They validated the model based on metered steam, chilled water and electricity use.
5. Conclusions
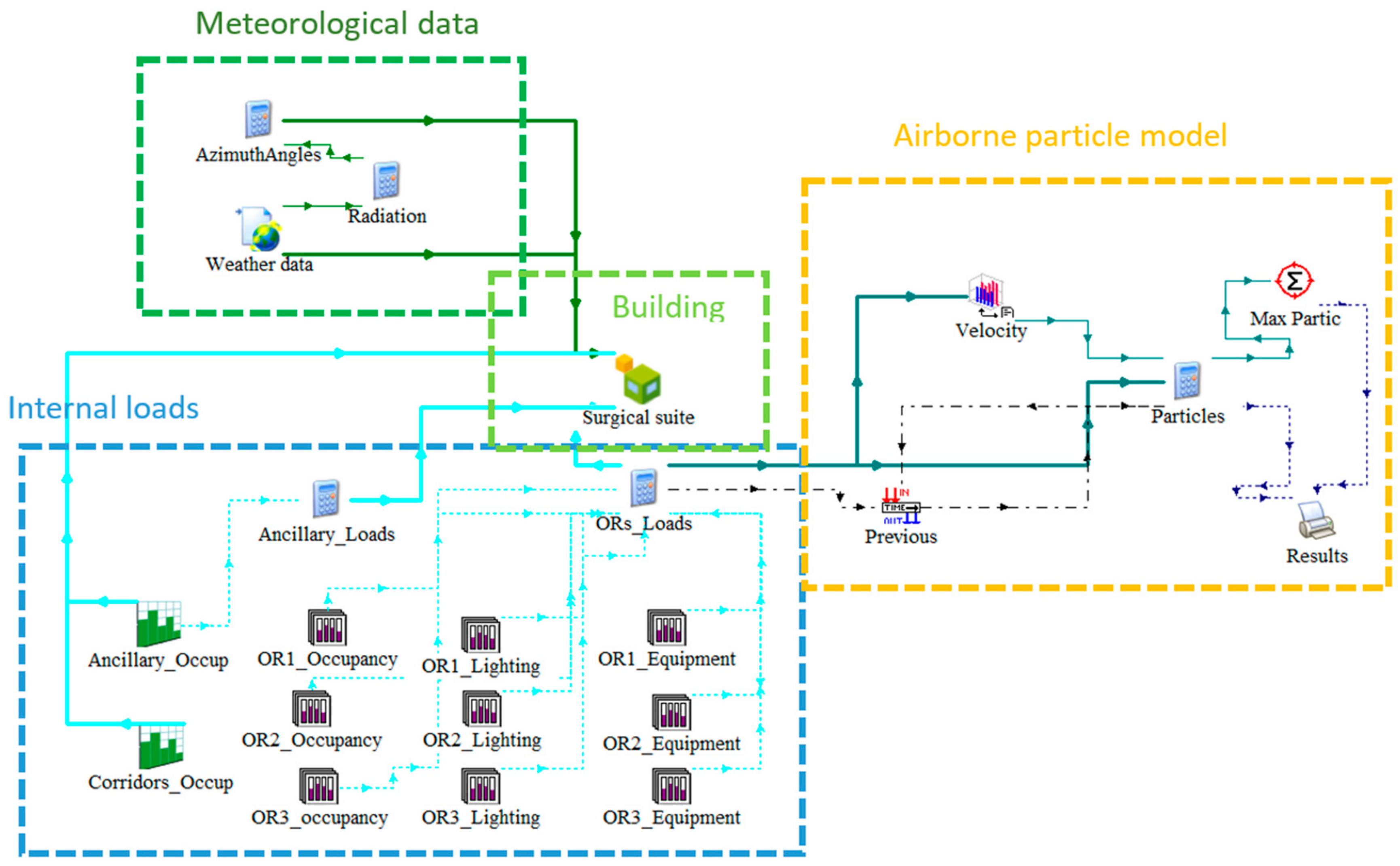
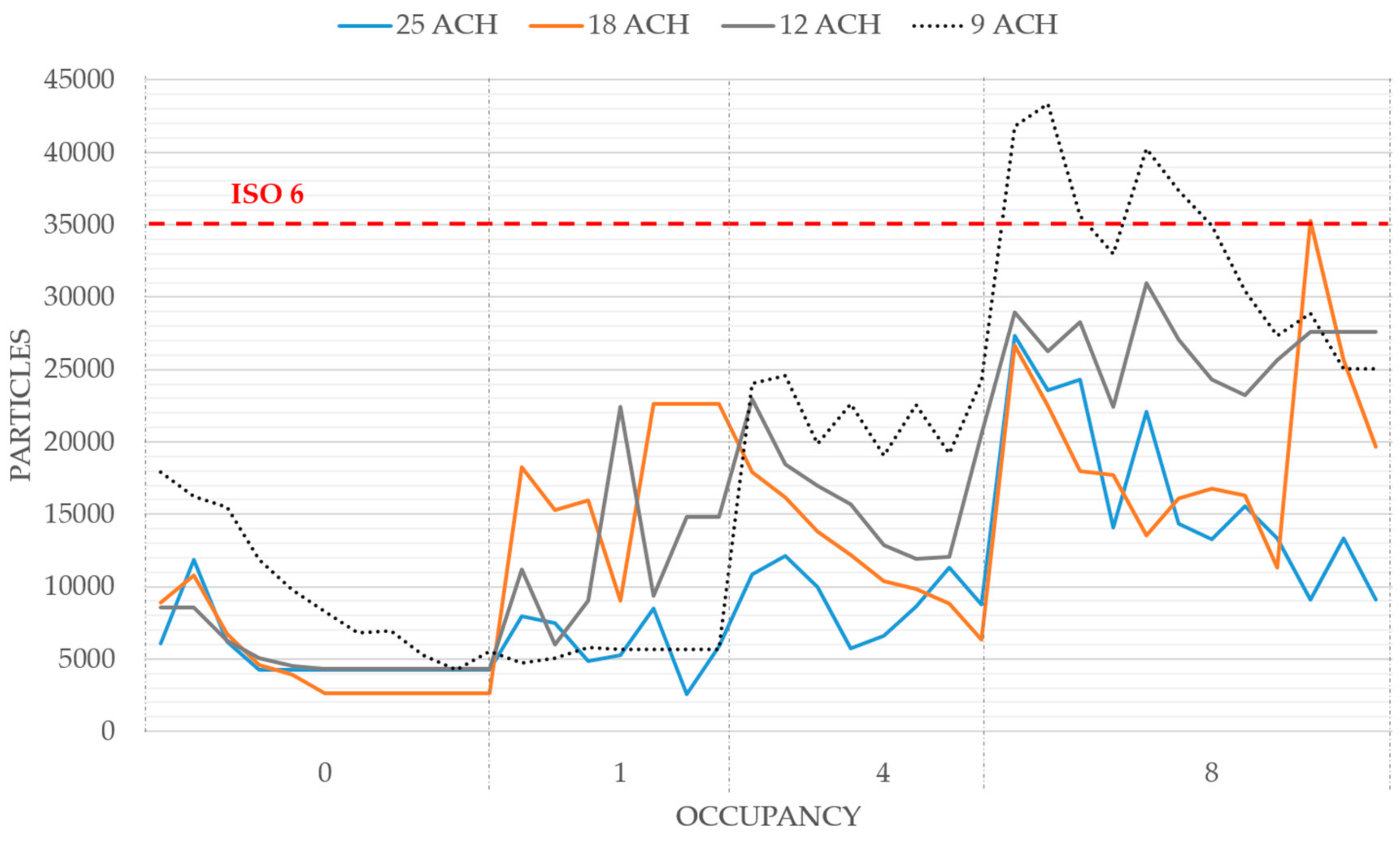
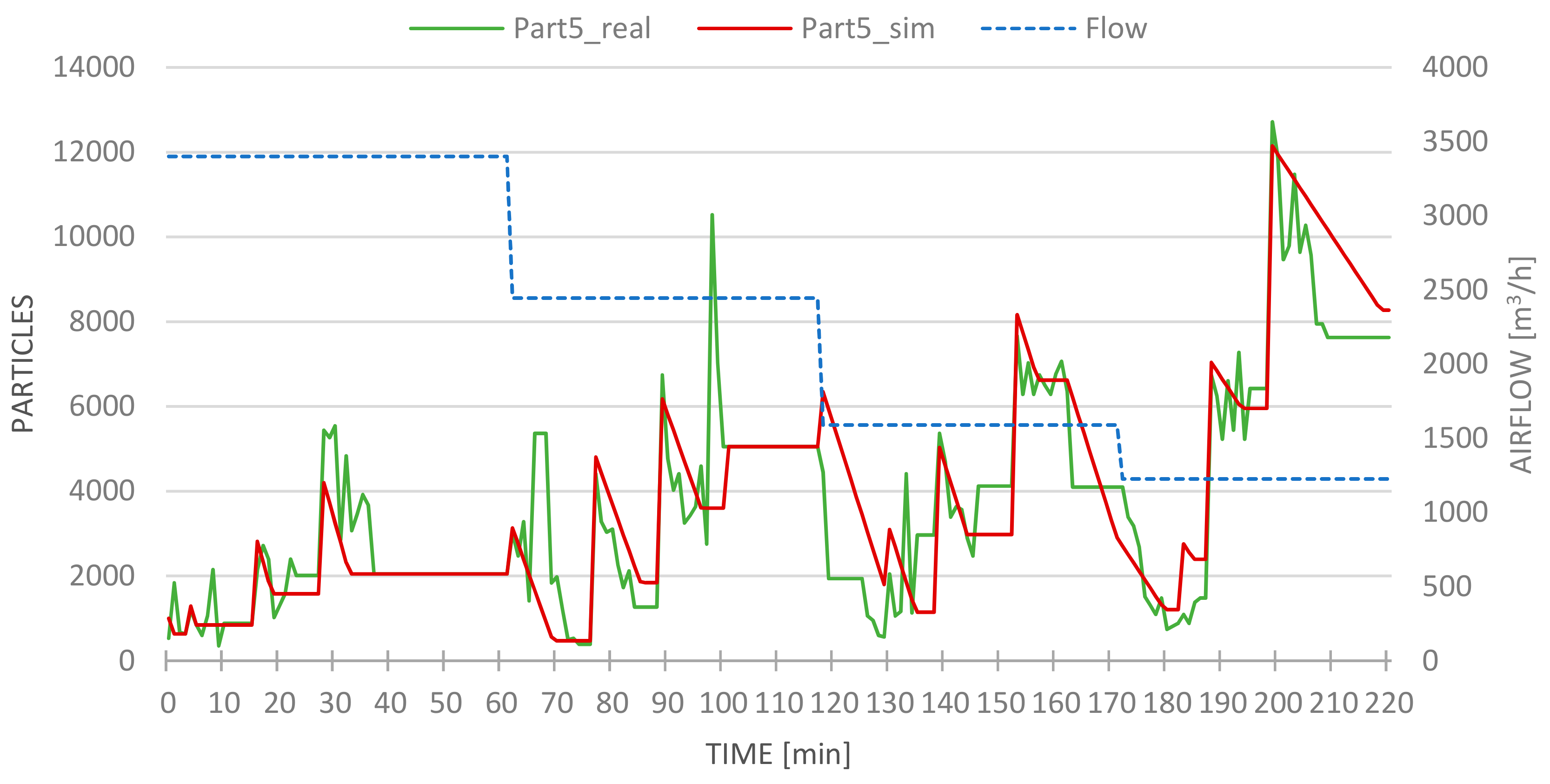
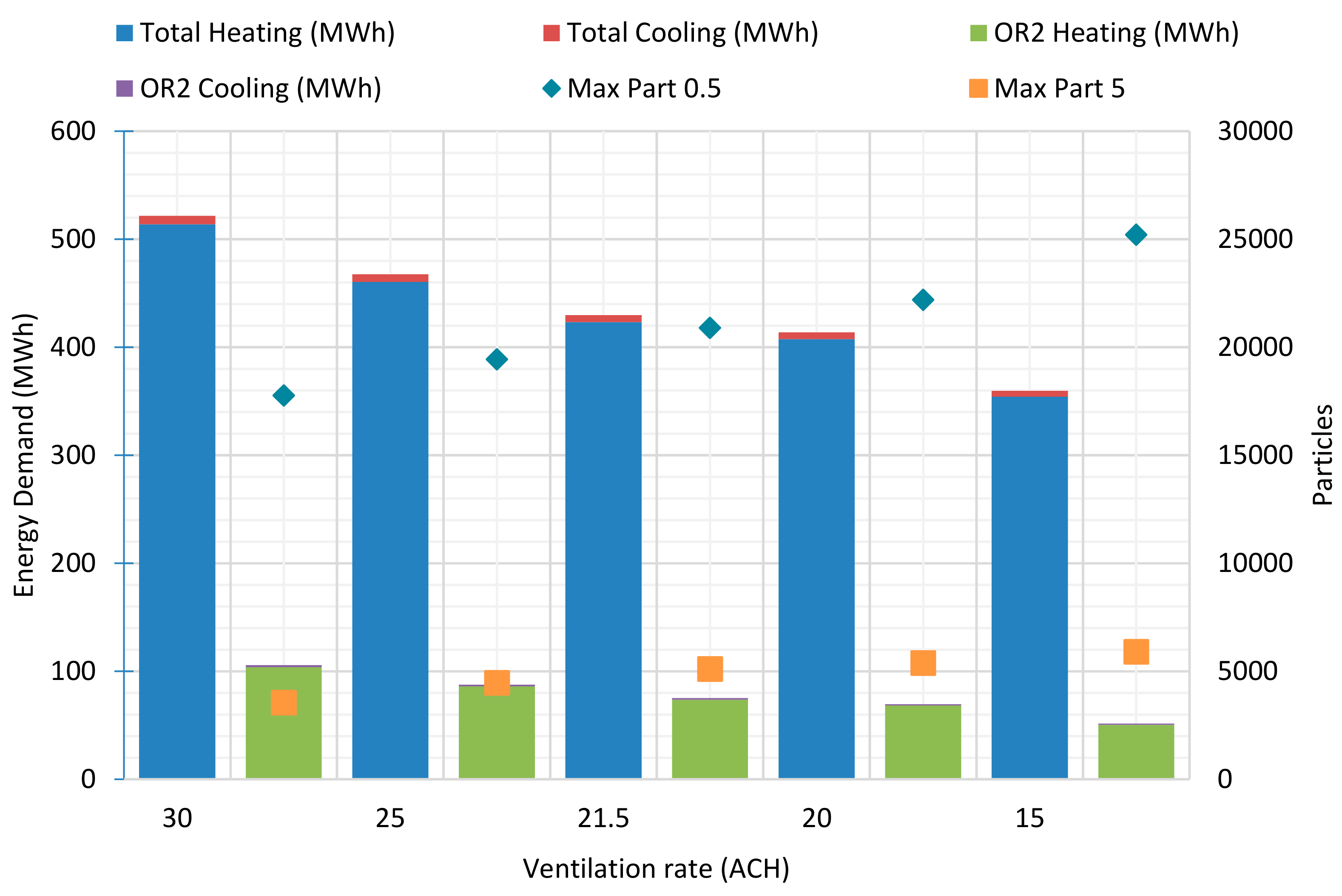
This study presents a simple and original methodology for the energy optimization of an OR while complying with airborne particle regulations. Two TRNSYS models were developed: a dynamic energy model of a surgical suite and an airborne particle model of an OR. Then, experimental measures were used to validate these models. Finally, different approaches to optimize ventilation in order to reduce energy consumption maintaining comfort and safety indoor conditions are identified and assessed. In particular, five different strategies were simulated (15, 20, 21.5, 25 and 30 ACH) and the implementation of these strategies simulations is predicted to save up to 51% of energy consumption annually, in the best of cases, keeping compliance with regulations. In addition, the ventilation requirements of OR can be reduced with respect to normative limits by performing monitoring studies. In the presented case study, even an air renovation rate of 15 ACH will keep the particle concentrations under the normative limits for an OR class ISO 6 or lower requirement. Based on experimental data, if higher than 20 ACH is maintained, even if the occupancy is increased, the regulations on particle matter continue to be fulfilled.
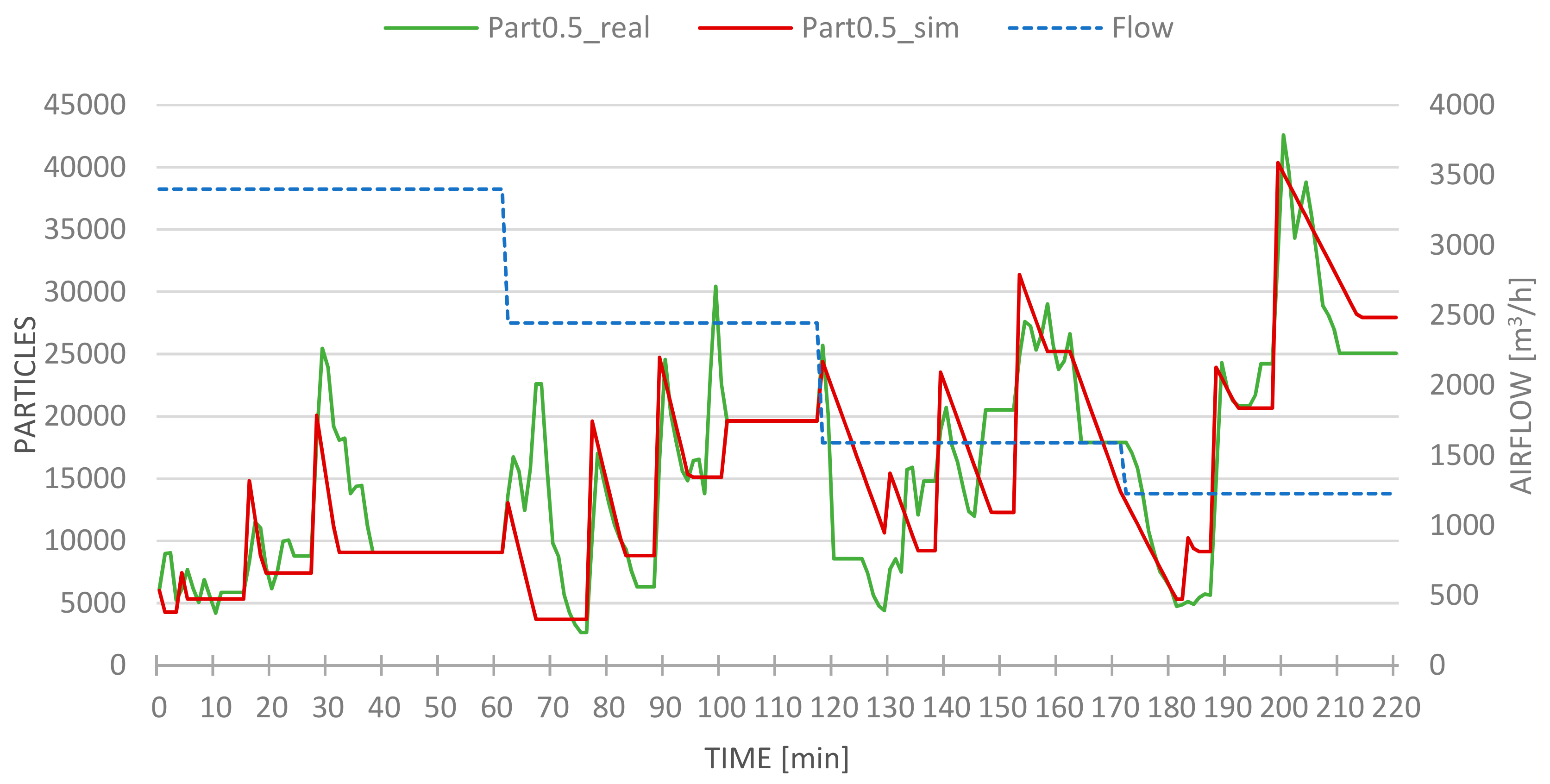
Although the models were quite complex, the simulated data agreed well with the metered data despite the multiple sources of error that can be present in simulations. The airborne particle model revealed a CV(RMSE) lower than 3%. The main limitations of the results are generated by these sources of error: weather data, uncertainty in measurements, non-exact thermophysical properties of constructive materials, and ambiguity in internal loads.
The methodology proposed is fast and useful and its applicability is wide as it can be completely transferred to any other cleanroom in the hospital. Future approaches of the procedure can be applied to a surgical suite, a laboratory or even to an entire hospital, reaching a holistic overview of the energy savings opportunities.

 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}