Esophagitis and Pneumonitis Related to Concurrent Chemoradiation ± Durvalumab Consolidation in Unresectable Stage III Non-Small-Cell Lung Cancer: Risk Assessment and Management Recommendations Based on a Modified Delphi Process

 , , ,
, , , 
Abstract
1. Introduction
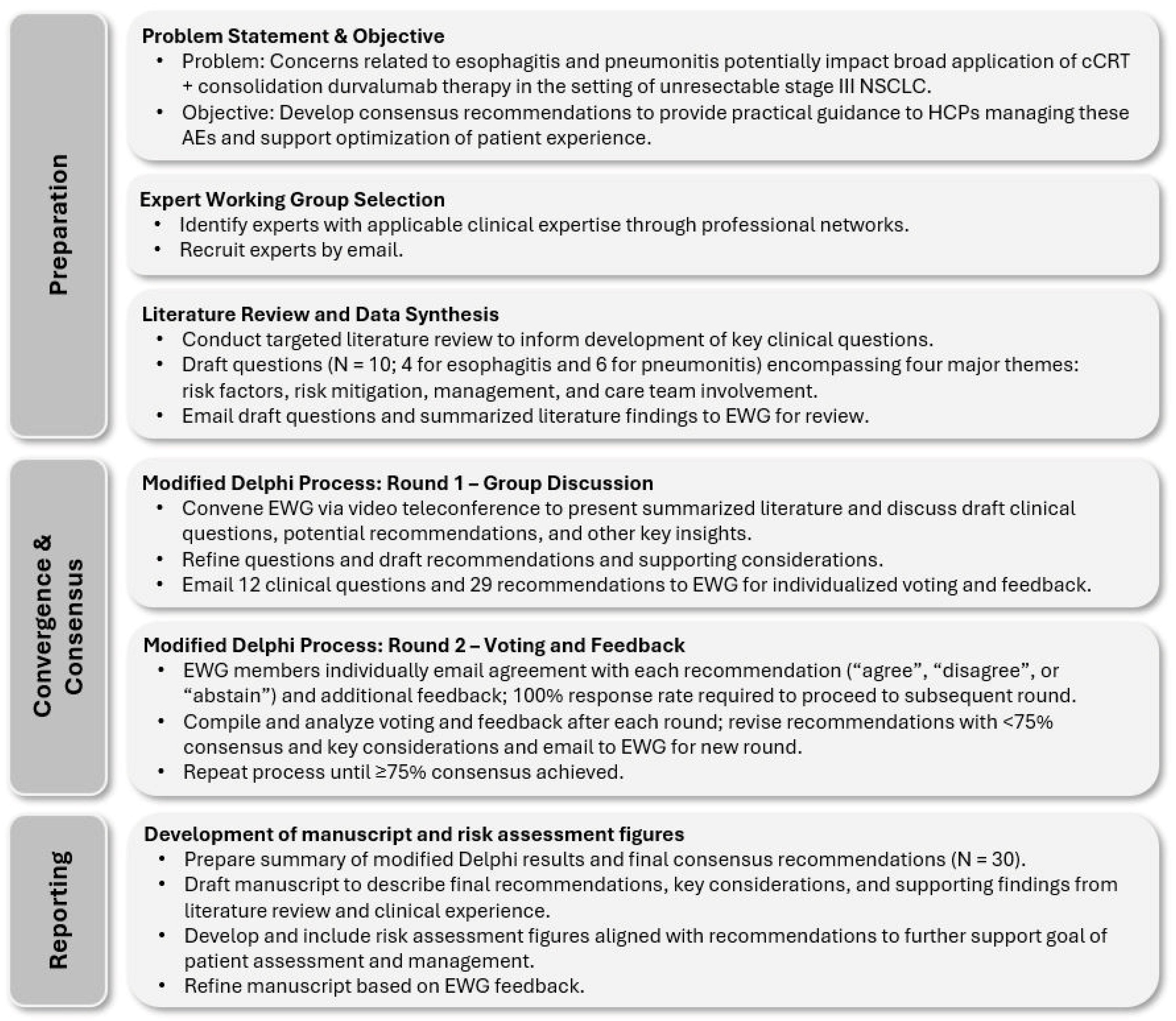
2. Materials and Methods
2.1. Expert Working Group Selection
2.2. Preparation, Convergence, Consensus, and Reporting
3. Results and Discussion
3.1. Esophagitis
- Question E1: How should patients be evaluated to ascertain the risk of developing esophagitis during or after cCRT?
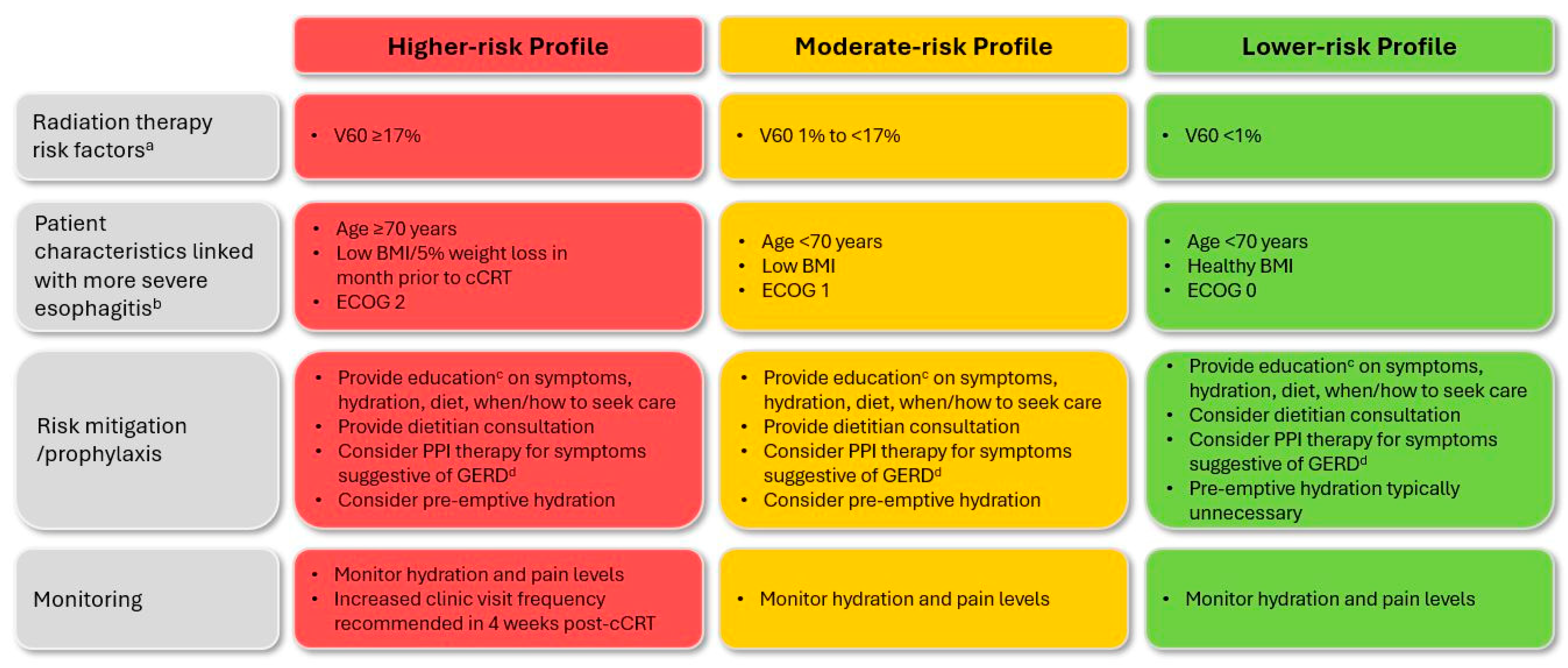
- Recommendation E1.1: Before cCRT, all patients should be assessed for risk of developing esophagitis to inform a risk-adapted treatment approach. (Level of agreement: 8 agree, 1 abstains)
- Recommendation E1.2: Radiation exposure to the esophagus is the most critical risk factor contributing to esophagitis during and/or after cCRT. (Level of agreement: unanimous)
- Question E2: What measures should be undertaken to prevent or mitigate the risk of esophagitis during or after cCRT?
- Recommendation E2.1: Early education of patients and caregivers/family members is critical to provide information on potential signs and symptoms of esophagitis, hydration requirements, dietary management, and when to seek care. (Level of agreement: unanimous)
- Recommendation E2.2: Appropriate planning techniques should be used to minimize exposure to radiation therapy. (Level of agreement: unanimous)
- Recommendation E2.3: Dietitian consultation is recommended early in the course of cCRT for patients with high or moderate esophagitis risk. (Level of agreement: unanimous)
- Recommendation E2.4: Proton pump inhibitor therapy should be considered for patients with symptoms suggestive of GERD. (Level of agreement: unanimous)
- Question E3: What treatments are effective for management of esophagitis?
- Recommendation E3.1: For symptomatic esophagitis, provide analgesics and consider dietitian support and PPI therapy if not already initiated; outpatient intravenous hydration can be initiated if patient is clinically dehydrated. Consider temporarily holding cCRT if initial measures prove ineffective. (Level of agreement: unanimous).
- Recommendation E3.2: For esophagitis requiring hospitalization, consider holding or discontinuing cCRT (if ongoing), provide continuous intravenous hydration, optimize pain management, and increase dietitian support. (Level of agreement: unanimous)
- Question E4: Which HCPs should be involved in the care of patients who experience esophagitis?
- Recommendation E4.1: Multidisciplinary team care is essential for optimizing management of esophagitis and must involve shared responsibilities, clear communication, and collaboration. (Level of agreement: 8 agree, 1 disagree)
- Recommendation E4.2: Patient follow-up frequency and HCP responsibility should be determined by esophagitis severity and timing of presentation. (Level of agreement: unanimous)
- Recommendation E4.3: Healthcare professionals should share clear follow-up care instructions, including point-of-care contacts at the cancer center, during cCRT and consolidation treatment phases. (Level of agreement: unanimous)
3.2. Pneumonitis
- Question P1: How should patients be evaluated to ascertain the risk of developing pneumonitis after cCRT ± durvalumab consolidation?
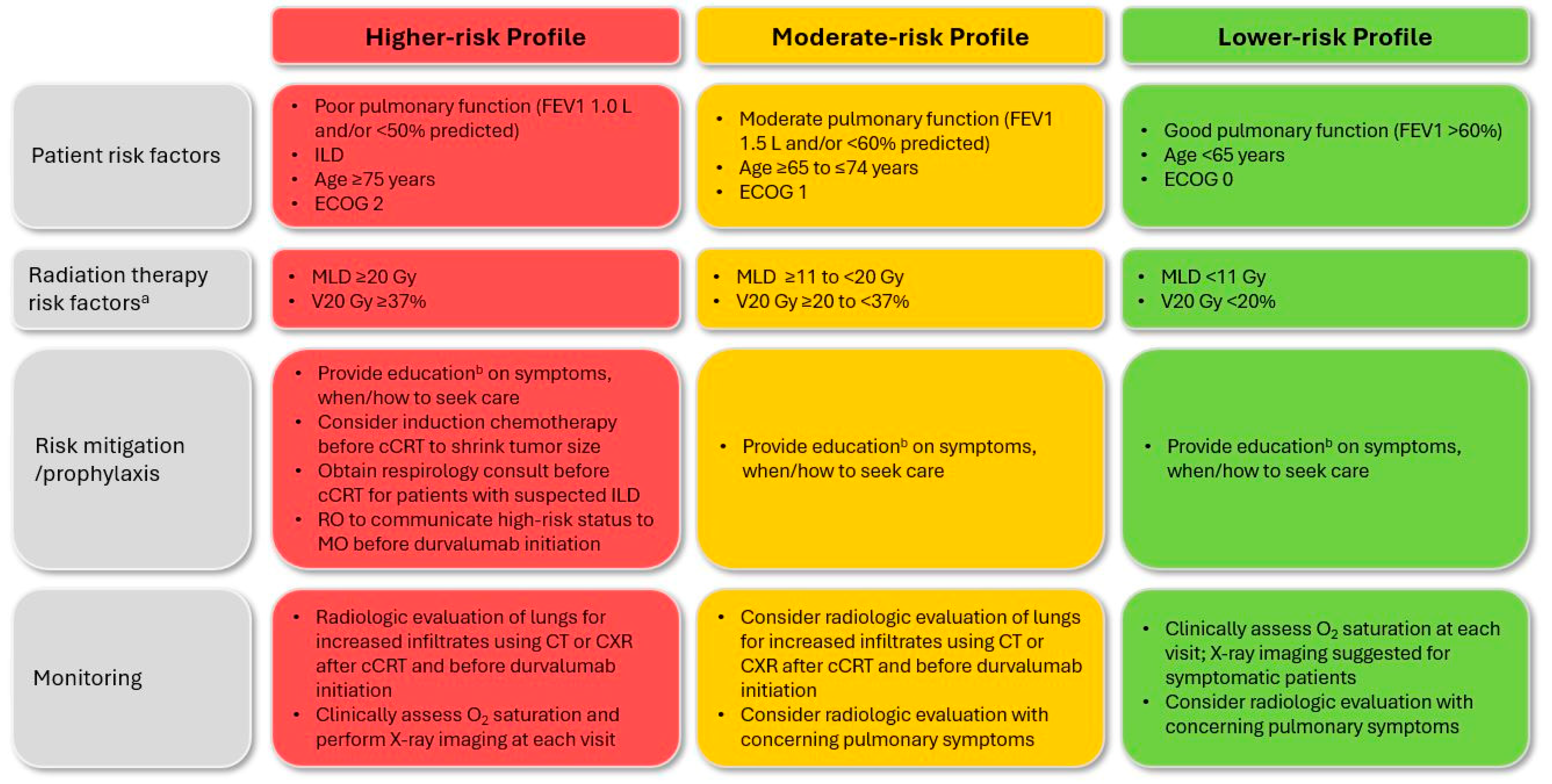
- Recommendation P1.1: Before initiating cCRT ± durvalumab, all patients should be assessed for risk of developing pneumonitis to inform a risk-adapted treatment approach. (Level of agreement: unanimous)
- Recommendation P1.2: Key factors identified to increase risk of symptomatic pneumonitis include large radiation volume (V20, mean lung dose) and poor lung function or the presence of interstitial lung disease at baseline. (Level of agreement: unanimous)
- Question P2: What measures should be undertaken to prevent or mitigate the risk of pneumonitis after cCRT ± durvalumab consolidation?
- Recommendation P2.1: Strategies should be implemented to reduce the volume of radiation delivered to normal structures and to address other modifiable risk factors. (Level of agreement: 8 agree, 1 abstains)
- Recommendation P2.2: For patients at very high risk of pneumonitis, determine whether definitive cCRT ± durvalumab consolidation is appropriate and safe to deliver on a case-by-case basis. (Level of agreement: unanimous)
- Question P3: What approach is recommended to determine the etiology of symptomatic pneumonitis?
- Recommendation: P3.1: Presentation of pneumonitis during durvalumab consolidation therapy may reflect RP or IO-related pneumonitis. Patients should be assessed by the treating radiation oncologist to help determine underlying etiology. (Level of agreement: 8 agree, 1 disagree)
- Recommendation P3.2: The radiation oncologist should compare the radiation plan with changes on CT imaging. In RP, lung parenchymal changes generally conform to the radiation treatment field, while IO-related pneumonitis is more likely to present with bilateral or diffuse lung changes. (Level of agreement: unanimous)
- Question P4: What treatments are effective for management of RP?
- Recommendation P4.1: Asymptomatic (grade 1) RP is common after cCRT and does not warrant investigation or treatment; however, increased monitoring may be warranted for patients presenting with new radiological changes after initiation of durvalumab consolidation therapy. (Level of agreement: unanimous)
- Recommendation P4.2: Patients with confirmed grade 2 RP should be followed under close observation. Prompt initiation of corticosteroid therapy should be considered in the event of worsening symptoms, as well as supplemental oxygen as clinically appropriate. Consider holding durvalumab if patient has initiated consolidation therapy. (Level of agreement: unanimous)
- Recommendation P4.3: Patients with confirmed grade 3/4 RP should promptly receive corticosteroid therapy and supplemental oxygen as clinically appropriate. Consider whether referral to respirology and/or hospitalization are warranted. Hold durvalumab if patient has initiated consolidation therapy. (Level of agreement: unanimous)
- Recommendation P4.4: Recommended corticosteroid therapy is oral prednisone 1 mg/kg/day up to 60 mg. Treatment should be tapered slowly over a duration of at least 6 weeks once RP has clinically improved. Simultaneous initiation of PPI therapy is also recommended, as well as consideration of prophylaxis for PJP. (Level of agreement: unanimous)
- Question P5: What treatments are effective for management of IO-related pneumonitis?
- Recommendation P5.1: Patients with asymptomatic (grade 1) IO-related pneumonitis should receive more frequent follow-up with oxygen saturation and chest X-ray. Consider holding durvalumab on a case-by-case basis. (Level of agreement: 8 agree, 1 abstains)
- Recommendation P5.2: Patients with confirmed grade 2 IO-related pneumonitis should have durvalumab suspended, corticosteroid therapy promptly initiated, and supplemental oxygen provided as clinically appropriate. Monitor closely; if pneumonitis persists or worsens after 48 to 72 h, treat as grade 3 or 4. (Level of agreement: 7 agree, 2 abstain)
- Recommendation P5.3: Patients with confirmed grade 3/4 IO-related pneumonitis should have durvalumab suspended or discontinued and corticosteroid therapy promptly initiated. Supplemental oxygen, hospitalization, and respirology referral are warranted. If pneumonitis persists or worsens after 48 h, consider initiating a non-steroidal immunosuppressive agent. (Level of agreement: 8 agree, 1 abstains)
- Recommendation P5.4: Recommended outpatient corticosteroid therapy is oral prednisone 1–2 mg/kg/day; treatment should be tapered slowly over a duration of at least 6 weeks once pneumonitis has clinically improved. Simultaneous initiation of PPI therapy is recommended, as well as consideration of prophylaxis for PJP. (Level of agreement: 8 agree, 1 abstains)
- Question P6: Which patients with RP are suitable for initiation of durvalumab consolidation?
- Recommendation P6.1: Consider initiating durvalumab for patients with asymptomatic RP after cCRT; more frequent follow-up with chest X-ray may be warranted. (Level of agreement: unanimous)
- Question P7: Which patients are suitable for durvalumab re-initiation after resolution of pneumonitis?
- Recommendation P7.1: For patients with confirmed RP who have resolution of symptoms and corticosteroids tapered to ≤10 mg/day, consider re-initiating durvalumab. (Level of agreement: unanimous)
- Recommendation P7.2: For patients with IO-related pneumonitis who have symptom resolution and corticosteroids tapered to ≤10 mg/day, the decision to re-initiate durvalumab should be individualized on the basis of patient characteristics and shared decision-making. (Level of agreement: 8 agree, 1 disagree)
- Question P8. Which HCPs should be involved in the care of patients who experience pneumonitis?
- Recommendation P8.1: Multidisciplinary team care is essential for optimizing follow-up of pneumonitis and must involve shared responsibilities, clear communication, and collaboration. (Level of agreement: 8 agree, 1 disagree)
- Recommendation P8.2: Radiation and medical oncologists should communicate regarding patient status and classification of pneumonitis etiology. If RP, the radiation oncologist should be responsible for management and follow-up until resolution; if IO-related, the medical oncologist should be responsible. (Level of agreement: unanimous)
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2024; Available online: https://gco.iarc.who.int/today (accessed on 20 March 2023).
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-year survival outcomes from the PACIFIC trial: Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J. Clin. Oncol. 2022, 40, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.E.; Singh, N.; Ismaila, N.; Antonoff, M.B.; Arenberg, D.A.; Bradley, J.; David, E.; Detterbeck, F.; Fruh, M.; Gubens, M.A.; et al. Management of stage III non-small-cell lung cancer: ASCO guideline. J. Clin. Oncol. 2022, 40, 1356–1384. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Non-Small Cell Lung Cancer. Version 7.2024-26 June 2024. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450 (accessed on 29 July 2024).
- European Society for Medical Oncology Guidelines Committee. eUpdate—Early and Locally Advanced Non-Small-Cell LungCancer (NSCLC) Treatment Recommendations. 4 May 2020. Available online: https://www.esmo.org/guidelines/lung-and-chest-tumours/early-stage-and-locally-advanced-non-metastatic-non-small-cell-lung-cancer/eupdate-early-and-locally-advanced-non-small-cell-lung-cancer-nsclc-treatment-recommendations (accessed on 20 March 2024).
- Park, K.; Vansteenkiste, J.; Lee, K.H.; Pentheroudakis, G.; Zhou, C.; Prabhash, K.; Seto, T.; Voon, P.J.; Tan, D.S.W.; Yang, J.C.H.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with locally-advanced unresectable non-small-cell lung cancer: A KSMO-ESMO initiative endorsed by CSCO, ISMPO, JSMO, MOS, SSO and TOS. Ann. Oncol. 2020, 31, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.; Vella, E.T.; Ellis, P.M.; Goffin, R.; Hanna, W.; Maziak, D.; Swaminath, A.; Ung, Y.C. Cancer Care Ontario. Recommendations for the Treatment of Patients with Clinical Stage III Non-Small Cell Lung Cancer: Endorsement of the 2019 National Institute for Health and Care Excellence Guidance and the 2018 Society for Immunotherapy of Cancer Guidance. Version 4. 27 April 2020. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/43311 (accessed on 5 April 2024).
- Spigel, D.R.; Cheng, Y.; Cho, B.C.; Laktionov, K.K.; Chen, Y.; Zenke, Y.; Lee, K.H.; Wang, Q.; Navarro, A.; Caro, R.B.; et al. ADRIATIC: Durvalumab (D) as consolidation treatment (tx) for patients (pts) with limited-stage small-cell lung cancer (LS-SCLC). In Proceedings of the American Society of Clinical Oncology Annual Meeting 2024, Chicago, IL, USA, 31 May–4 June 2024. Abstract LBA5. [Google Scholar]
- Yusuf, D.; Walton, R.N.; Hurry, M.; Farrer, C.; Bebb, D.G.; Cheung, W.Y. Population-based treatment patterns and outcomes for stage III non-small cell lung cancer patients: A real-world evidence study. Am. J. Clin. Oncol. 2020, 43, 615–620. [Google Scholar] [CrossRef]
- Seung, S.J.; Hurry, M.; Walton, R.N.; Evans, W.K. Retrospective cohort study of unresectable stage III non-small-cell lung cancer in Canada. Curr. Oncol. 2020, 27, e354–e360. [Google Scholar] [CrossRef]
- Evans, W.; Flanagan, W.; Gauvreau, C.; Manivong, P.; Memon, S.; Fitzgerald, N.; Goffin, J.; Garner, R.; Khoo, E.; Mittmann, N. MA18.03 How in the real world are lung cancer patients treated? The Ontario, Canada experience. J. Thorac. Oncol. 2018, 13, S419. [Google Scholar] [CrossRef]
- Kuang, S.; Liu, M.; Ho, C.; Berthelet, E.; Laskin, J.; Sun, S.; Zhang, T.; Melosky, B. 1247P–Uptake of durvalumab in the management of stage III NSCLC: The real-world application of PACIFIC. Ann. Oncol. 2020, 31, S807–S808. [Google Scholar] [CrossRef]
- Langberg, C.W.; Horndalsveen, H.; Helland, Å.; Haakensen, V.D. Factors associated with failure to start consolidation durvalumab after definitive chemoradiation for locally advanced NSCLC. Front. Oncol. 2023, 13, 1217424. [Google Scholar] [CrossRef]
- Brade, A.; Jao, K.; Yu, S.; Cheema, P.; Doucette, S.; Christofides, A.; Schellenberg, D. A Canadian perspective on the challenges for delivery of curative-intent therapy in stage III unresectable non-small cell lung cancer. Curr. Oncol. 2021, 28, 1618–1629. [Google Scholar] [CrossRef]
- Verma, V.; Simone, C.B.; Werner-Wasik, M. Acute and late toxicities of concurrent chemoradiotherapy for locally-advanced non-small cell lung cancer. Cancers 2017, 9, 120. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Senan, S.; Oberije, C.; Belderbos, J.; de Dios, N.R.; Bradley, J.D.; Barriger, R.B.; Moreno-Jiménez, M.; Kim, T.H.; Ramella, S.; et al. Predicting esophagitis after chemoradiation therapy for non-small cell lung cancer: An individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 690–696. [Google Scholar] [CrossRef]
- Palma, D.A.; Senan, S.; Tsujino, K.; Barriger, R.B.; Rengan, R.; Moreno, M.; Bradley, J.D.; Kim, T.H.; Ramella, S.; Marks, L.B.; et al. Predicting radiation pneumonitis after chemoradiation therapy for lung cancer: An international individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Saito, G.; Oya, Y.; Taniguchi, Y.; Kawachi, H.; Daichi, F.; Matsumoto, H.; Iwasawa, S.; Suzuki, H.; Niitsu, T.; Miyauchi, E.; et al. Real-world survey of pneumonitis and its impact on durvalumab consolidation therapy in patients with non-small cell lung cancer who received chemoradiotherapy after durvalumab approval (HOPE-005/CRIMSON). Lung Cancer 2021, 161, 86–93. [Google Scholar] [CrossRef]
- Desilets, A.; Blanc-Durand, F.; Lau, S.; Hakozaki, T.; Kitadai, R.; Malo, J.; Belkaid, W.; Richard, C.; Messaoudene, M.; Cvetkovic, L.; et al. Durvalumab therapy following chemoradiation compared with a historical cohort treated with chemoradiation alone in patients with stage III non-small cell lung cancer: A real-world multicentre study. Eur. J. Cancer 2021, 142, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Horinouchi, H.; Atagi, S.; Oizumi, S.; Ohashi, K.; Kato, T.; Kozuki, T.; Seike, M.; Sone, T.; Sobue, T.; Tokito, T.; et al. Real-world outcomes of chemoradiotherapy for unresectable Stage III non-small cell lung cancer: The SOLUTION study. Cancer Med. 2020, 9, 6597–6608. [Google Scholar] [CrossRef]
- Verfaillie, S.; Lambrecht, M.; Berkovic, P.; Dooms, C.; Nackaerts, K.; Van de Velde, A.-S.; Vansteenkiste, J.; Wauters, E. Treatment of unresectable stage III NSCLC: Real world cohort study and literature review. Cancer Treat. Res. Commun. 2023, 36, 100727. [Google Scholar] [CrossRef]
- Shintani, T.; Kishi, N.; Matsuo, Y.; Ogura, M.; Mitsuyoshi, T.; Araki, N.; Fujii, K.; Okumura, S.; Nakamatsu, K.; Kishi, T.; et al. Incidence and risk factors of symptomatic radiation pneumonitis in non-small-cell lung cancer patients treated with concurrent chemoradiotherapy and consolidation durvalumab. Clin. Lung Cancer 2021, 22, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Mayahara, H.; Uehara, K.; Harada, A.; Kitatani, K.; Yabuuchi, T.; Miyazaki, S.; Ishihara, T.; Kawaguchi, H.; Kubota, H.; Okada, H.; et al. Predicting factors of symptomatic radiation pneumonitis induced by durvalumab following concurrent chemoradiotherapy in locally advanced non-small cell lung cancer. Radiat. Oncol. 2022, 17, 7. [Google Scholar] [CrossRef]
- Naidoo, J.; Vansteenkiste, J.F.; Faivre-Finn, C.; Özgüroğlu, M.; Murakami, S.; Hui, R.; Quantin, X.; Broadhurst, H.; Newton, M.; Thiyagarajah, P.; et al. Characterizing immune-mediated adverse events with durvalumab in patients with unresectable stage III NSCLC: A post-hoc analysis of the PACIFIC trial. Lung Cancer 2022, 166, 84–93. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Faivre-Finn, C.; Nackaerts, K.; Jordan, K.; Arends, J.; Douillard, J.Y.; Ricardi, U.; Peters, S. Recommendation for supportive care in patients receiving concurrent chemotherapy and radiotherapy for lung cancer. Ann. Oncol. 2020, 31, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Kasmann, L.; Dietrich, A.; Staab-Weijnitz, C.A.; Manapov, F.; Behr, J.; Rimner, A.; Jeremic, B.; Senan, S.; De Ruysscher, D.; Lauber, K.; et al. Radiation-induced lung toxicity-cellular and molecular mechanisms of pathogenesis, management, and literature review. Radiat. Oncol. 2020, 15, 214. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Dahele, M.; Lagerwaard, F.J.; Senan, S. A critical review of recent developments in radiotherapy for non-small cell lung cancer. Radiat. Oncol. 2016, 11, 115. [Google Scholar] [CrossRef]
- Billiet, C.; Peeters, S.; De Ruysscher, D. Focus on treatment complications and optimal management: Radiation oncology. Transl. Lung Cancer Res. 2014, 3, 187–191. [Google Scholar]
- Naidoo, J.; Nishino, M.; Patel, S.P.; Shankar, B.; Rekhtman, N.; Illei, P.; Camus, P. Immune-related pneumonitis after chemoradiotherapy and subsequent immune checkpoint blockade in unresectable stage III non-small-cell lung cancer. Clin. Lung Cancer 2020, 21, e435–e444. [Google Scholar] [CrossRef]
- Qiu, Q.; Xing, L.; Wang, Y.; Feng, A.; Wen, Q. Development and validation of a radiomics nomogram using computed tomography for differentiating immune checkpoint inhibitor-related pneumonitis from radiation pneumonitis for patients with non-small cell lung cancer. Front. Immunol. 2022, 13, 870842. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; National Institutes of Health; National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0. 27 November 2017. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_60 (accessed on 19 March 2024).
- Kea, B.; Sun, B.C. Consensus development for healthcare professionals. Intern. Emerg. Med. 2015, 10, 373–383. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Faivre-Finn, C.; Moeller, D.; Nestle, U.; Hurkmans, C.W.; Le Péchoux, C.; Belderbos, J.; Guckenberger, M.; Senan, S. European Organization for Research and Treatment of Cancer (EORTC) recommendations for planning and delivery of high-dose, high precision radiotherapy for lung cancer. Radiother. Oncol. 2017, 124, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Campbell, J.; Stenmark, M.H.; Stanton, P.; Zhao, J.; Matuszak, M.M.; Ten Haken, R.K.; Kong, F.M. A model combining age, equivalent uniform dose and IL-8 may predict radiation esophagitis in patients with non-small cell lung cancer. Radiother. Oncol. 2018, 126, 506–510. [Google Scholar] [CrossRef]
- Ahn, S.J.; Kahn, D.; Zhou, S.; Yu, X.; Hollis, D.; Shafman, T.D.; Marks, L.B. Dosimetric and clinical predictors for radiation-induced esophageal injury. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 335–347. [Google Scholar] [CrossRef]
- Challand, T.; Thureau, S.; Dubray, B.; Giraud, P. Esophageal toxicity of radiation therapy: Clinical risk factors and management. Cancer Radiother. 2012, 16, 364–371. [Google Scholar] [CrossRef]
- Patel, A.B.; Edelman, M.J.; Kwok, Y.; Krasna, M.J.; Suntharalingam, M. Predictors of acute esophagitis in patients with non-small-cell lung carcinoma treated with concurrent chemotherapy and hyperfractionated radiotherapy followed by surgery. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1106–1112. [Google Scholar] [CrossRef]
- Uyterlinde, W.; Chen, C.; Nijkamp, J.; Obbink, M.G.; Sonke, J.J.; Belderbos, J.; van den Heuvel, M. Treatment adherence in concurrent chemoradiation in patients with locally advanced non-small cell lung carcinoma: Results of daily intravenous prehydration. Radiother. Oncol. 2014, 110, 488–492. [Google Scholar] [CrossRef]
- Maguire, P.D.; Sibley, G.S.; Zhou, S.M.; Jamieson, T.A.; Light, K.L.; Antoine, P.A.; Herndon, J.E., 2nd; Anscher, M.S.; Marks, L.B. Clinical and dosimetric predictors of radiation-induced esophageal toxicity. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 97–103. [Google Scholar] [CrossRef]
- Lopes, S.; Pabst, L.; Dory, A.; Klotz, M.; Gourieux, B.; Michel, B.; Mascaux, C. Do proton pump inhibitors alter the response to immune checkpoint inhibitors in cancer patients? A meta-analysis. Front. Immunol. 2023, 14, 1070076. [Google Scholar] [CrossRef]
- Chen, B.; Yang, C.; Dragomir, M.P.; Chi, D.; Chen, W.; Horst, D.; Calin, G.A.; Li, Q. Association of proton pump inhibitor use with survival outcomes in cancer patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Ther. Adv. Med. Oncol. 2022, 14, 17588359221111703. [Google Scholar] [CrossRef]
- Sun, G.Y.; Edwards, D.M.; Miller, S.R.; Elliott, D.A.; Hamstra, D.A.; Chen, A.C.; Green, M.; Bryant, A.K. Association of proton pump inhibitor use and severe pneumonitis in stage III non-small-cell lung cancer treated with primary chemoradiation and adjuvant durvalumab. Int. J. Rad. Oncol. Biol. Phys. 2023, 117, e61. [Google Scholar] [CrossRef]
- Wei, N.; Zheng, B.; Que, W.; Zhang, J.; Liu, M. The association between proton pump inhibitor use and systemic anti-tumour therapy on survival outcomes in patients with advanced non-small cell lung cancer: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2022, 88, 3052–3063. [Google Scholar] [CrossRef]
- Miao, J.; Herrmann, S.M. Immune checkpoint inhibitors and their interaction with proton pump inhibitors-related interstitial nephritis. Clin. Kidney J. 2023, 16, 1834–1844. [Google Scholar] [CrossRef]
- Jaiswal, A.; Shergill, K.; Boppana, K.; Almansouri, N.E.; Bakkannavar, S.; Faheem, Y.; Nath, T.S. Nephrological detrimental impacts resulting from novel immunotherapy drugs used in the treatment of cancer: A systematic review. Cureus 2024, 16, e54487. [Google Scholar] [CrossRef]
- Wang, W.H.; Huang, J.Q.; Zheng, G.F.; Xia, H.H.; Wong, W.M.; Lam, S.K.; Wong, B.C. Head-to-head comparison of H2-receptor antagonists and proton pump inhibitors in the treatment of erosive esophagitis: A meta-analysis. World J. Gastroenterol. 2005, 11, 4067–4077. [Google Scholar] [CrossRef]
- Seres, D.S.; Valcarcel, M.; Guillaume, A. Advantages of enteral nutrition over parenteral nutrition. Ther. Adv. Gastroenterol. 2013, 6, 157–167. [Google Scholar] [CrossRef]
- de Castro, G.; Souza, F.H.; Lima, J.; Bernardi, L.P.; Teixeira, C.H.A.; Prado, G.F. Does multidisciplinary team management improve clinical outcomes in NSCLC? A systematic review with meta-analysis. JTO Clin. Res. Rep. 2023, 4, 100580. [Google Scholar] [CrossRef]
- Zhou, C.; Yu, J. Chinese expert consensus on diagnosis and treatment of radiation pneumonitis. Precis. Radiat. Oncol. 2022, 6, 262–271. [Google Scholar] [CrossRef]
- Gao, R.W.; Day, C.N.; Yu, N.Y.; Bush, A.; Amundson, A.C.; Prodduturvar, P.; Majeed, U.; Butts, E.; Oliver, T.; Schwecke, A.J.; et al. Dosimetric predictors of pneumonitis in locally advanced non-small cell lung cancer patients treated with chemoradiation followed by durvalumab. Lung Cancer 2022, 170, 58–64. [Google Scholar] [CrossRef]
- Harada, D.; Shimonishi, A.; Saeki, K.; Ninomiya, T.; Kanzaki, H.; Nagasaki, K.; Ogura, C.; Tsutsui, Y.; Kojin, K.; Hamamoto, Y.; et al. Early administration of durvalumab after chemoradiotherapy increased risk of pneumonitis in patients with locally advanced non-small cell lung cancer. Asia Pac. J. Clin. Oncol. 2023, 19, e111–e117. [Google Scholar] [CrossRef]
- Bradley, J.D.; Sugawara, S.; Lee, K.H.H.; Ostoros, G.; Demirkazik, A.; Zemanova, M.; Sriuranpong, V.; Gelatti, A.; De Menezes, J.J.; Zurawski, B.; et al. LBA1-Durvalumab in combination with chemoradiotherapy for patients with unresectable stage III NSCLC: Final results from PACIFIC-2. Ann. Oncol. 2024, 9, 102986. [Google Scholar] [CrossRef]
- Zhang, M.; Fan, Y.; Nie, L.; Wang, G.; Sun, K.; Cheng, Y. Clinical outcomes of immune checkpoint inhibitor therapy in patients with advanced non-small cell lung cancer and preexisting interstitial lung diseases: A systematic review and meta-analysis. Chest 2022, 161, 1675–1686. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Ohguri, T.; Matsuki, Y.; Yahara, K.; Oki, H.; Imada, H.; Narisada, H.; Korogi, Y. Radiotherapy for thoracic tumors: Association between subclinical interstitial lung disease and fatal radiation pneumonitis. Int. J. Clin. Oncol. 2015, 20, 45–52. [Google Scholar] [CrossRef]
- Altan, M.; Soto, F.; Xu, T.; Wilson, N.; Franco-Vega, M.C.; Simbaqueba Clavijo, C.A.; Shannon, V.R.; Faiz, S.A.; Gandhi, S.; Lin, S.H.; et al. Pneumonitis after concurrent chemoradiation and immune checkpoint inhibition in patients with locally advanced non-small cell lung cancer. Clin. Oncol. 2023, 35, 630–639. [Google Scholar] [CrossRef]
- Kawanaka, Y.; Yasuda, Y.; Tanizaki, J.; Iwashima, D.; Nonagase, Y.; Uemasu, K.; Hirayama, Y.; Ogura, M.; Ozaki, T.; Takahashi, K.I. The safety and efficacy of durvalumab consolidation therapy in the management of patients with stage III non-small-cell lung cancer and preexisting interstitial lung disease. Respir. Investig. 2022, 60, 667–673. [Google Scholar] [CrossRef]
- Li, F.; Liu, H.; Wu, H.; Liang, S.; Xu, Y. Risk factors for radiation pneumonitis in lung cancer patients with subclinical interstitial lung disease after thoracic radiation therapy. Radiat. Oncol. 2021, 16, 70. [Google Scholar] [CrossRef]
- Higo, H.; Kubo, T.; Makimoto, S.; Makimoto, G.; Ihara, H.; Masaoka, Y.; Ninomiya, T.; Ichihara, E.; Ohashi, K.; Sato, A.; et al. Chemoradiotherapy for locally advanced lung cancer patients with interstitial lung abnormalities. Jap. J. Clin. Oncol. 2019, 49, 458–464. [Google Scholar] [CrossRef]
- Vansteenkiste, J.; Naidoo, J.; Faivre-Finn, C.; Özgüroğlu, M.; Villegas, A.; Daniel, D.; Murakami, S.; Hui, R.; Lee, K.; Cho, B.C.; et al. MA05.02 PACIFIC subgroup analysis: Pneumonitis in stage III, unresectable NSCLC patients treated with durvalumab vs. placebo after CRT. J. Thorac. Oncol. 2018, 13, S370–S371. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, T.; Huang, Y.; Li, W.; Zhao, J.; Yang, Y.; Li, C.; Wang, L.; Bi, N. Real-world safety and efficacy of consolidation durvalumab after chemoradiation therapy for stage III non-small cell lung cancer: A systematic review and meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 1154–1164. [Google Scholar] [CrossRef]
- Liu, T.; Li, S.; Ding, S.; Qiu, J.; Ren, C.; Chen, J.; Wang, H.; Wang, X.; Li, G.; He, Z.; et al. Comparison of post-chemoradiotherapy pneumonitis between Asian and non-Asian patients with locally advanced non-small cell lung cancer: A systematic review and meta-analysis. EClinicalMedicine 2023, 64, 102246. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Abu-Sbeih, H.; Ascierto, P.A.; Brufsky, J.; Cappelli, L.C.; Cortazar, F.B.; Gerber, D.E.; Hamad, L.; Hansen, E.; Johnson, D.B.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J. Immunother. Cancer 2021, 9, e002435. [Google Scholar] [CrossRef]
- Zhou, Y.; Yan, T.; Zhou, X.; Cao, P.; Luo, C.; Zhou, L.; Xu, Y.; Liu, Y.; Xue, J.; Wang, J.; et al. Acute severe radiation pneumonitis among non-small cell lung cancer (NSCLC) patients with moderate pulmonary dysfunction receiving definitive concurrent chemoradiotherapy: Impact of pre-treatment pulmonary function parameters. Strahlenther. Onkol. 2020, 196, 505–514. [Google Scholar] [CrossRef]
- Chun, S.G.; Hu, C.; Choy, H.; Komaki, R.U.; Timmerman, R.D.; Schild, S.E.; Bogart, J.A.; Dobelbower, M.C.; Bosch, W.; Galvin, J.M.; et al. Impact of intensity-modulated radiation therapy technique for locally advanced non-small-cell lung cancer: A secondary analysis of the NRG Oncology RTOG 0617 randomized clinical trial. J. Clin. Oncol. 2017, 35, 56–62. [Google Scholar] [CrossRef]
- Choi, Y.W.; Munden, R.F.; Erasmus, J.J.; Park, K.J.; Chung, W.K.; Jeon, S.C.; Park, C.-K. Effects of radiation therapy on the lung: Radiologic appearances and differential diagnosis. RadioGraphics 2004, 24, 985–997. [Google Scholar] [CrossRef]
- Knoll, M.A.; Salvatore, M.; Sheu, R.D.; Knoll, A.D.; Kerns, S.L.; Lo, Y.-C.; Rosenzweig, K.E. The use of isodose levels to interpret radiation induced lung injury: A quantitative analysis of computed tomography changes. Quant. Imaging Med. Surg. 2016, 6, 35–41. [Google Scholar]
- Smesseim, I.; Mets, O.M.; Daniels, J.M.A.; Bahce, I.; Senan, S. Diagnosis and management of pneumonitis following chemoradiotherapy and immunotherapy in stage III non-small cell lung cancer. Radiother. Oncol. 2024, 194, 110147. [Google Scholar] [CrossRef]
- Cheng, J.; Pan, Y.; Huang, W.; Huang, K.; Cui, Y.; Hong, W.; Wang, L.; Ni, D.; Tan, P. Differentiation between immune checkpoint inhibitor-related and radiation pneumonitis in lung cancer by CT radiomics and machine learning. Med. Phys. 2022, 49, 1547–1558. [Google Scholar] [CrossRef]
- Hindocha, S.; Hunter, B.; Linton-Reid, K.; George Charlton, T.; Chen, M.; Logan, A.; Ahmed, M.; Locke, I.; Sharma, B.; Doran, S.; et al. Validated machine learning tools to distinguish immune checkpoint inhibitor, radiotherapy, COVID-19 and other infective pneumonitis. Radiother. Oncol. 2024, 195, 110266. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Management of Immunotherapy-related Toxicities. Version 1.2024-7 December 2023. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=3&id=1486 (accessed on 1 April 2024).
- BC Cancer. BC Cancer Protocol Summary for Management of Immune-Mediated Adverse Reactions to Checkpoint Inhibitor Immunotherapy. Revised 1 February 2022. Available online: http://www.bccancer.bc.ca/health-professionals/clinical-resources/chemotherapy-protocols/immunotherapy (accessed on 5 April 2024).
- Cancer Care Ontario. Immune Checkpoint Inhibitor Toxicity Management. Clinical Practice Guideline. Available online: https://www.cancercareontario.ca/en/guidelines-advice (accessed on 4 April 2024).
- Shaverdian, N.; Offin, M.; Shepherd, A.F.; Hellmann, M.D.; Gomez, D.R.; Chaft, J.E.; Rimner, A. Association between the early discontinuation of durvalumab and poor survival in patients with stage III NSCLC. JTO Clin. Res. Rep. 2021, 2, 100197. [Google Scholar] [CrossRef]
- Moore, R.; Lau, S.; Bezjak, A.; Sacher, A.G.; Liu, Z.; Hope, A.J.; Lok, B.; Giuliani, M.E.; Cho, J.; Sun, A. 133: Incidence, severity and managment of pneumonitis in stage III non-small cel lung cancer patients on adjuvant durvalumab. Radiother. Oncol. 2020, 150, S58. [Google Scholar] [CrossRef]
- Hassanzadeh, C.; Sita, T.; Savoor, R.; Samson, P.P.; Bradley, J.; Gentile, M.; Roach, M.; Mohindra, N.; Waqar, S.; Kruser, T.J.; et al. Implications of pneumonitis after chemoradiation and durvalumab for locally advanced non-small cell lung cancer. J. Thorac. Dis. 2020, 12, 6690–6700. [Google Scholar] [CrossRef]
- Dolladille, C.; Ederhy, S.; Sassier, M.; Cautela, J.; Thuny, F.; Cohen, A.A.; Fedrizzi, S.; Chrétien, B.; Da-Silva, A.; Plane, A.F.; et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Esophagitis | Pneumonitis | |
|---|---|---|
| Frequency | Symptomatic grade ≥ 2: ~50% [17] | Grade ≥ 2 RP: 30–44% [18,23,24] Any-grade IO-related: 11–22% a (grade 3/4: 1.9%) [20,25] |
| Typical time to onset (any grade) | 2–3 weeks after initiation of cCRT [26] b | RP: 1–6 months after cCRT [26,27] IO-related: 54 days (median) after durvalumab initiation (range, 2–342 days) [25] |
| Typical time to resolution | ~8 weeks after end of cCRT [26] | 53 days (median; range, 22–588 days) [25] |
| Signs and symptoms [16,26,28] c |
|
|
| Risks and complications [16,26,27,28,29] |
|
|
| Differentiation of etiology [30,31] e | N/A | RP: Changes typically conform to radiation treatment field with sharp border. IO-related pneumonitis: Typically, bilateral or diffuse lung changes. |
| Grade | Esophagitis a | Pneumonitis |
|---|---|---|
| 1 | Asymptomatic Clinical or diagnostic observations only—intervention not indicated. | Asymptomatic Clinical or diagnostic observations only—intervention not indicated. |
| 2 | Symptomatic; altered eating or swallowing Oral supplements indicated | Symptomatic; limiting instrumental ADL Medical intervention indicated |
| 3 | Severely altered eating/swallowing Tube feeding, TPN, or hospitalization indicated | Severe symptoms; limiting self-care ADL Oxygen indicated |
| 4 | Life-threatening consequences Urgent operative intervention indicated | Life-threatening respiratory compromise Urgent intervention indicated (e.g., tracheotomy or intubation) |
| 5 | Death | |
| Target Population | Patients with stage III unresectable NSCLC treated with cCRT ± durvalumab consolidation therapy | |
| Target Audience | Radiation oncologists; medical oncologists; oncology nurses, nurse practitioners, and physician assistants; respirologists; pulmonologists; radiologists; family physician/community primary care team members; geriatric oncologists; pharmacists; patients | |
| Clinical Question | Recommendations and Level of Agreement | Key Considerations |
| E1. How should patients be evaluated to ascertain the risk of developing esophagitis during or after cCRT? | Recommendation E1.1: Before cCRT, all patients should be assessed for risk of developing esophagitis to inform a risk-adapted treatment approach. (Level of agreement: 8 agree, 1 abstains) Recommendation E1.2: Radiation exposure to the esophagus is the most critical risk factor contributing to esophagitis during and/or after cCRT. (Level of agreement: unanimous) |
|
| E2. What measures should be undertaken to prevent or mitigate the risk of esophagitis during or after cCRT? | Recommendation E2.1: Early education of patients and caregivers/family members is critical to provide information on potential signs and symptoms of esophagitis, hydration requirements, dietary management, and when to seek care. (Level of agreement: unanimous) Recommendation E2.2: Appropriate planning techniques should be used to minimize exposure to RT. (Level of agreement: unanimous) Recommendation E2.3: Dietitian consultation is recommended early in the course of cCRT for patients with high or moderate esophagitis risk. (Level of agreement: unanimous) Recommendation E2.4: Proton pump inhibitor therapy should be considered for patients with symptoms suggestive of GERD. (Level of agreement: unanimous) |
|
| E3. What treatments are effective for management of esophagitis? | Recommendation E3.1: For symptomatic esophagitis, provide analgesics and consider dietitian support and PPI therapy if not already initiated; outpatient IV hydration can be initiated if patient is clinically dehydrated. Consider temporarily holding cCRT if initial measures prove ineffective. (Level of agreement: unanimous) Recommendation E3.2: For esophagitis requiring hospitalization, consider holding or discontinuing cCRT (if ongoing), provide continuous IV hydration, optimize pain management, and increase dietitian support. (Level of agreement: unanimous) |
|
| E4. Which HCPs should be involved in the care of patients who experience esophagitis? | Recommendation E4.1: Multidisciplinary team care is essential for optimizing management of esophagitis and must involve shared responsibilities, clear communication, and collaboration. (Level of agreement: 8 agree, 1 disagree) Recommendation E4.2: Patient follow-up frequency and HCP responsibility should be determined by esophagitis severity and timing of presentation. (Level of agreement: unanimous) Recommendation E4.3: Healthcare providers should share clear follow-up care instructions, including point-of-care contact(s) at the cancer center, during cCRT and consolidation treatment phases. (Level of agreement: unanimous) |
|
| Target Population | Patients with stage III unresectable NSCLC treated with cCRT ± durvalumab consolidation therapy | |
| Target Audience | Radiation oncologists; medical oncologists; oncology nurses, nurse practitioners, and physician assistants; respirologists; pulmonologists; radiologists; family physician/community primary care team members; geriatric oncologists; pharmacists; patients | |
| Clinical Question | Recommendation and Level of Agreement | Key Considerations |
| P1. How should patients be evaluated to ascertain the risk of developing pneumonitis after cCRT ± durvalumab consolidation? | Recommendation P1.1: Before initiating cCRT ± durvalumab, all patients should be assessed for risk of developing pneumonitis to inform a risk-adapted treatment approach. (Level of agreement: unanimous) Recommendation P1.2: Key factors identified to increase the risk of symptomatic pneumonitis include large radiation volume (V20, MLD) and poor lung function or presence of ILD at baseline. (Level of agreement: unanimous) |
|
| P2. What measures should be undertaken to prevent or mitigate the risk of pneumonitis after cCRT ± durvalumab consolidation? | Recommendation P2.1: Strategies should be implemented to reduce the volume of radiation delivered to normal structures and to address other modifiable risk factors. (Level of agreement: 8 agree, 1 abstains) Recommendation P2.2: For patients at very high risk of pneumonitis, determine whether definitive cCRT ± durvalumab consolidation is appropriate and safe to deliver on a case-by-case basis. (Level of agreement: unanimous) |
|
| P3. What approach is recommended to determine the etiology of symptomatic pneumonitis? | Recommendation P3.1: Presentation of pneumonitis during durvalumab consolidation therapy may reflect RP or IO-related pneumonitis. Patients should be assessed by the treating RO to help determine underlying etiology. (Level of agreement: 8 agree, 1 disagree) Recommendation P3.2: The RO should compare the radiation plan with changes on CT imaging. In RP, lung parenchymal changes generally conform to the radiation treatment field, while IO-related pneumonitis is more likely to present with bilateral or diffuse lung changes. (Level of agreement: unanimous) |
|
| P4. What treatments are effective for management of RP? | Recommendation P4.1: Asymptomatic (grade 1) RP is common after cCRT and does not warrant investigation or treatment; however, increased monitoring may be warranted for patients presenting with new radiological changes after initiation of durvalumab consolidation therapy. (Level of agreement: unanimous) Recommendation P4.2: Patients with confirmed grade 2 RP should be followed under close observation. Prompt initiation of corticosteroid therapy should be considered in the event of worsening symptoms, as well as supplemental oxygen as clinically appropriate. Consider holding durvalumab if patient has initiated consolidation therapy. (Level of agreement: unanimous) Recommendation P4.3: Patients with confirmed grade 3/4 RP should promptly receive corticosteroid therapy and supplemental oxygen as clinically appropriate. Consider whether referral to respirology and/or hospitalization are warranted. Hold durvalumab if patient has initiated consolidation therapy. (Level of agreement: unanimous) Recommendation P4.4: Recommended corticosteroid therapy is oral prednisone 1 mg/kg/day up to 60 mg/day; treatment should be tapered slowly over a duration of at least 6 weeks once RP has clinically improved. Simultaneous initiation of PPI therapy is also recommended, as well as consideration of prophylaxis for PJP. (Level of agreement: unanimous) |
|
| P5. What treatments are effective for management of IO-related pneumonitis? | Recommendation P5.1: Patients with asymptomatic (grade 1) IO-related pneumonitis should receive more frequent follow-up with oxygen saturation and chest X-ray. Consider holding durvalumab on a case-by-case basis. (Level of agreement: 8 agree, 1 abstains) Recommendation P5.2: Patients with confirmed grade 2 IO-related pneumonitis should have durvalumab suspended, corticosteroid therapy promptly initiated, and supplemental oxygen provided as clinically appropriate. Monitor closely; if pneumonitis persists or worsens after 48 to 72 h, treat as grade 3 or 4. (Level of agreement: unanimous) Recommendation P5.3: Patients with confirmed grade 3 or 4 IO-related pneumonitis should have durvalumab suspended or discontinued and corticosteroid therapy promptly initiated. Supplemental oxygen, hospitalization, and respirology referral are warranted. If pneumonitis persists or worsens after 48 h, consider initiating a non-steroidal immunosuppressive agent. (Level of agreement: unanimous) Recommendation P5.4: Recommended outpatient corticosteroid therapy is oral prednisone 1–2 mg/kg/day; treatment should be tapered slowly over a duration of at least 6 weeks once pneumonitis has improved clinically. Simultaneous initiation of PPI therapy is recommended, as well as consideration of prophylaxis for PJP. (Level of agreement: 8 agree, 1 abstains) |
|
| P6. Which patients with RP are suitable for initiation of durvalumab consolidation? | Recommendation P6.1: Consider initiating durvalumab for patients with asymptomatic RP after cCRT; more frequent follow-up with chest X-ray may be warranted. (Level of agreement: unanimous) |
|
| P7. Which patients are suitable for durvalumab re-initiation after resolution of pneumonitis? | Recommendation P7.1: For patients with confirmed RP who have resolution of symptoms and corticosteroids tapered to ≤10 mg/day, consider re-initiating durvalumab. (Level of agreement: unanimous) Recommendation P7.2: For patients with IO-related pneumonitis who have symptom resolution and corticosteroids tapered to ≤10 mg/day, the decision to re-initiate durvalumab should be individualized on the basis of patient characteristics and shared decision-making. (Level of agreement: 8 agree, 1 disagree) |
|
| P8. Which HCPs should be involved in the care of patients who experience pneumonitis? | Recommendation P8.1: Multidisciplinary team care is essential for optimizing follow-up of pneumonitis and must involve shared responsibilities, clear communication, and collaboration. (Level of agreement: 8 agree, 1 disagree) Recommendation P8.2: Radiation and medical oncologists should communicate regarding patient status and classification of pneumonitis etiology. If RP, the RO should be responsible for management and follow-up until resolution; if IO-related, the MO should be responsible. (Level of agreement: unanimous) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brade, A.M.; Bahig, H.; Bezjak, A.; Juergens, R.A.; Lynden, C.; Marcoux, N.; Melosky, B.; Schellenberg, D.; Snow, S. Esophagitis and Pneumonitis Related to Concurrent Chemoradiation ± Durvalumab Consolidation in Unresectable Stage III Non-Small-Cell Lung Cancer: Risk Assessment and Management Recommendations Based on a Modified Delphi Process. Curr. Oncol. 2024, 31, 6512-6535. https://doi.org/10.3390/curroncol31110483
Brade AM, Bahig H, Bezjak A, Juergens RA, Lynden C, Marcoux N, Melosky B, Schellenberg D, Snow S. Esophagitis and Pneumonitis Related to Concurrent Chemoradiation ± Durvalumab Consolidation in Unresectable Stage III Non-Small-Cell Lung Cancer: Risk Assessment and Management Recommendations Based on a Modified Delphi Process. Current Oncology. 2024; 31(11):6512-6535. https://doi.org/10.3390/curroncol31110483
Chicago/Turabian StyleBrade, Anthony M., Houda Bahig, Andrea Bezjak, Rosalyn A. Juergens, Charmaine Lynden, Nicolas Marcoux, Barbara Melosky, Devin Schellenberg, and Stephanie Snow. 2024. "Esophagitis and Pneumonitis Related to Concurrent Chemoradiation ± Durvalumab Consolidation in Unresectable Stage III Non-Small-Cell Lung Cancer: Risk Assessment and Management Recommendations Based on a Modified Delphi Process" Current Oncology 31, no. 11: 6512-6535. https://doi.org/10.3390/curroncol31110483
APA StyleBrade, A. M., Bahig, H., Bezjak, A., Juergens, R. A., Lynden, C., Marcoux, N., Melosky, B., Schellenberg, D., & Snow, S. (2024). Esophagitis and Pneumonitis Related to Concurrent Chemoradiation ± Durvalumab Consolidation in Unresectable Stage III Non-Small-Cell Lung Cancer: Risk Assessment and Management Recommendations Based on a Modified Delphi Process. Current Oncology, 31(11), 6512-6535. https://doi.org/10.3390/curroncol31110483