Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2+ Breast Cancer in Both the Early and Metastatic Setting

 ,
,  ,
,  , ,
, ,  , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Consensus Recommendation Process
2.2. Guiding Principles
3. Systemic Therapy in HER2+ Breast Cancer
3.1. Early Breast Cancer

{kind=link}
{kind=link}
| Neoadjuvant Regimen * | Adjuvant Regimen | Primary Outcome | Secondary Outcomes | |
|---|---|---|---|---|
| NeoSphere [29,30] | DHP (Q3W × 4) DH (Q3W × 4) | FEC (Q3W × 3) | pCR: 45.8% vs. 29.0% | 5-year PFS: 86% vs. 81% (HR 0.69, 95% CI 0.34–1.40) 5-year DFS: 84% vs. 81% (HR 0.60, 95% CI 0.28–1.27) |
| PEONY [31,32] | DHP (Q3W × 4) DH (Q3W × 4) | FEC (Q3W × 3) followed by HP (13 cycles) FEC (Q3W × 3) followed by H (13 cycles) | pCR: 39.3% vs. 21.8% (Δ = 17.5%, 95% CI 6.9–28.0%, p = 0.001) | 5-year EFS: 84.8% vs. 73.7% (HR 0.53, 95% CI 0.32–0.89) 5-year DFS: 86.0% vs. 75.0% (HR 0.52, 95% CI 0.30–0.88) 5-year OS: 93.9% vs. 90.0%(HR 0.53, 95% CI 0.23–1.19) |
| BERENICE [33] | ddAC (Q2W × 4) followed by T (QW × 12) + HP (Q3W × 4) FEC (Q3W × 4) followed by DHP (Q3W × 4) | HP (Q3W × 13) | NYHA class III/IV heart failure (patients): 3 (1.5%) vs. 0 Confirmed LVEF decline †: 2 (1.0%) vs. 1 (0.5%) | 5-year EFS: 90.8% vs. 89.2% 4-year iDFs: 92.6% vs. 91.1% 5-year OS: 96.1% vs. 93.8% pCR: 61.8% vs. 60.7% |
| TRYPHAENA [36,39] | FEC + HP (Q3W × 3) followed by DHP (Q3W × 3) FEC (Q3W × 3) followed by DHP (Q3W × 3) TCHP (Q3W x 6) | H (up to 1 year) | Symptomatic LVSD: 0 vs. 2 (2.7%) vs. 0 LVEF decline ‡: 4 (5.6%) vs. 4 (5.3%) vs. 3 (3.9%) | 3-year DFS: 87% vs. 88% vs. 90% 3-year PFS: 89% vs. 89% vs. 87% 3-year OS: 94% vs. 94% vs. 93% |
| TRAIN-2 [37,38] | HP + FEC (Q3W × 3) followed by HP + TC (Q3W × 6) HP + TC (Q3W × 9) | N/A | pCR: 67% vs. 68% (Δ= −1.5%, 95% CI −11 to 8, p = 0.95) | 3-year EFS: 92.7% vs. 93.6% (HR 0.90, 95% CI 0.50–1.63) 3-year OS: 97.7% vs. 98.2% (HR 0.91, 95% CI 0.35–2.36) |
3.2. Metastatic Breast Cancer
| Study Population | Key Outcomes (Intervention vs. Comparator Arm), HR (95% CI) | Key Safety Observations | |
|---|---|---|---|
| DESTINY-Breast01 [54] Phase 2 T-DXd | HER2+ unresectable or mBC with prior T-DM1 (N = 184) | Median PFS: 19.4 months (14.1–25.0) Median OS: 29.1 months (24.6–36.1) | Grade ≥3 TEAE occurred in 53.8% of patients Most common TEAEs GI or hematologic Drug-related ILD/pneumonitis in 15.8% |
| NALA [60] Phase 3 Neratinib + capecitabine (+loperamide prophylaxis) vs. lapatinib + capecitabine | HER2+ mBC and ≥ 2 previous HER2-directed mBC therapies (N = 621) | PFS: 0.76 (0.63–0.93) OS: 0.88 (0.72–1.07) | Diarrhea, nausea, PPES, vomiting most common AEs of any grade overall More grade 3 diarrhea with neratinib No new cardiac safety concerns |
| Subgroup with ≥3 previous HER2-targeted regimens: 30% | PFS: 0.71 (0.50–1.00) OS: 0.71 (0.50–1.02) | ||
| NCT00078572 [61] Phase 3 Lapatinib + capecitabine vs. capecitabine alone | HER2+ locally advanced or mBC and progression after anthracycline, taxane, and H (N = 324) Prior H for mBC: 91% | PFS: 0.49 (0.34–0.71) OS: 0.92 (0.58–1.46) | Diarrhea, dyspepsia, rash, asymptomatic cardia events more common with lapatinib |
| SOPHIA [62] Phase 3 Margetuximab vs. H, each in combination with chemotherapy (1 of capecitabine, eribulin, gemcitabine, or vinorelbine) | HER2+ mBC, ≥2 previous HER2-directed therapies, and 1–3 nonhormonal mBC therapy (N = 536) | PFS: 0.76 (0.59–0.98) OS: 0.89 (0.69–1.13) | Grade ≥3 AEs (≥5%): neutropenia, anemia (both groups); fatigue (margetuximab); febrile neutropenia (H) ↑IRRs with margetuximab; no increase in cardiac toxicity |
| Subgroup with ≥3 previous mBC regimens: 34% | PFS: 0.72 (0.48–1.08) OS: 0.70 (0.47–1.05) |
3.3. Brain Metastases
3.4. Special Considerations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Society Breast Cancer Statistics. Available online: https://cancer.ca/en/cancer-information/cancer-types/breast/statistics (accessed on 2 August 2024).
- Wolff, A.C.; Somerfield, M.R.; Dowsett, M.; Hammond, M.E.H.; Hayes, D.F.; McShane, L.M.; Saphner, T.J.; Spears, P.A.; Allison, K.H. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer. Arch. Pathol. Lab. Med. 2023, 147, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Mercogliano, M.F.; Bruni, S.; Mauro, F.L.; Schillaci, R. Emerging Targeted Therapies for HER2-Positive Breast Cancer. Cancers 2023, 15, 1987. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Cronin, K.A.; Kurian, A.W.; Andridge, R. Differences in Breast Cancer Survival by Molecular Subtypes in the United States. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2018, 27, 619–626. [Google Scholar] [CrossRef]
- Seung, S.J.; Traore, A.N.; Pourmirza, B.; Fathers, K.E.; Coombes, M.; Jerzak, K.J. A Population-Based Analysis of Breast Cancer Incidence and Survival by Subtype in Ontario Women. Curr. Oncol. 2020, 27, e191–e198. [Google Scholar] [CrossRef]
- Bezerra, C.T.; Grande, A.J.; Galvão, V.K.; Santos, D.H.M.D.; Atallah, Á.N.; Silva, V. Assessment of the Strength of Recommendation and Quality of Evidence: GRADE Checklist. A Descriptive Study. Sao Paulo Med. J. 2022, 140, 829–836. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Connolly, J.L.; D’Orsi, C.J.; Edge, S.B.; Mittendorf, E.A.; Rugo, H.S.; Solin, L.J.; Weaver, D.L.; Winchester, D.J.; Giuliano, A. Chapter in AJCC Cancer Staging Manual, 8th ed.; The American College of Surgeons (ACS): Chicago, IL, USA, 2017; Available online: http://www.breastsurgeonsweb.com/wp-content/uploads/downloads/2020/10/AJCC-Breast-Cancer-Staging-System.pdf (accessed on 19 October 2024).
- Female Breast Cancer Subtypes—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/breast-subtypes.html (accessed on 6 August 2024).
- Yau, C.; Osdoit, M.; van der Noordaa, M.; Shad, S.; Wei, J.; de Croze, D.; Hamy, A.-S.; Laé, M.; Reyal, F.; Sonke, G.S.; et al. Residual Cancer Burden after Neoadjuvant Chemotherapy and Long-Term Survival Outcomes in Breast Cancer: A Multicentre Pooled Analysis of 5161 Patients. Lancet Oncol. 2022, 23, 149–160. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Rayson, D.; Gandhi, S.; Joy, A.A.; Brezden-Masley, C.; Gelmon, K.A.; Sehdev, S.; Cescon, D.; Chia, S. Access to Neoadjuvant Pertuzumab for HER2 Positive Breast Cancer in Canada: A Dilemma Increasingly Difficult to Explain. Curr. Oncol. 2022, 29, 9891–9895. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhao, W.; Liu, C.; Gao, Y.; Chen, D.; Wu, M.; Li, C.; Wang, X.; Song, X.; Yu, J.; et al. The Residual Cancer Burden Index as a Valid Prognostic Indicator in Breast Cancer after Neoadjuvant Chemotherapy. BMC Cancer 2024, 24, 13. [Google Scholar] [CrossRef]
- Loibl, S.; André, F.; Bachelot, T.; Barrios, C.H.; Bergh, J.; Burstein, H.J.; Cardoso, M.J.; Carey, L.A.; Dawood, S.; Del Mastro, L.; et al. Early Breast Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2024, 35, 159–182. [Google Scholar] [CrossRef]
- Gradishar, W. NCCN Breast Cancer Guidelines V4.2024. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419 (accessed on 10 July 2024).
- Tolaney, S.M.; Barry, W.T.; Dang, C.T.; Yardley, D.A.; Beverly, M.; Kelly, M.P.; Albain, K.S.; Rugo, H.S.; Matthew, E.; Shapira, I.; et al. Adjuvant Paclitaxel and Trastuzumab for Node-Negative, HER2-Positive Breast Cancer. N. Engl. J. Med. 2015, 372, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Tolaney, S.M.; Tarantino, P.; Graham, N.; Tayob, N.; Parè, L.; Villacampa, G.; Dang, C.T.; Yardley, D.A.; Moy, B.; Marcom, P.K.; et al. Adjuvant Paclitaxel and Trastuzumab for Node-Negative, HER2-Positive Breast Cancer: Final 10-Year Analysis of the Open-Label, Single-Arm, Phase 2 APT Trial. Lancet Oncol. 2023, 24, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Faleh, S.; Prakash, I.; Eisenberg, E.; Basik, M.; Boileau, J.F.; Tejera, D.; Panet, F.; Buhlaiga, N.; Meterissian, S.; Wong, S.M. Predictors of Nodal Metastases in Early Stage HER2+ Breast Cancer: Deciding on Treatment Approach with Neoadjuvant Chemotherapy vs. Upfront Surgery. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2023, 49, 1411–1416. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Huang, C.-S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Untch, M.; Mano, M.S.; Huang, C.-S.; Geyer, C.E., Jr.; von Minckwitz, G.; Wolmark, N.; Pivot, X.; Kuemmel, S.; DiGiovanna, M.P.; et al. Adjuvant T-DM1 versus Trastuzumab in Patients with Residual Invasive Disease after Neoadjuvant Therapy for HER2-Positive Breast Cancer: Subgroup Analyses from KATHERINE. Ann. Oncol. 2021, 32, 1005–1014. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef]
- Jones, S.E.; Collea, R.; Paul, D.; Sedlacek, S.; Favret, A.M.; Gore, I.; Lindquist, D.L.; Holmes, F.A.; Allison, M.A.K.; Brooks, B.D.; et al. Adjuvant Docetaxel and Cyclophosphamide plus Trastuzumab in Patients with HER2-Amplified Early Stage Breast Cancer: A Single-Group, Open-Label, Phase 2 Study. Lancet Oncol. 2013, 14, 1121–1128. [Google Scholar] [CrossRef]
- Romond, E.H.; Suman, V.J.; Tan-Chiu, E.; Kaufman, P.A.; Fehrenbacher, L.; Vogel, V.G.; Jenkins, R.B.; Mamounas, E.P.; Klein, P.M. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.-H.; Sledge, G.; Geyer, C.E.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.M.; et al. Trastuzumab Plus Adjuvant Chemotherapy for Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: Planned Joint Analysis of Overall Survival From NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 Years’ Follow-up of Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer: Final Analysis of the HERceptin Adjuvant (HERA) Trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Patel, T.A.; Dave, B.; Rodriguez, A.A.; Chang, J.C.; Perez, E.A.; Colon-Otero, G. Dual HER2 Blockade: Preclinical and Clinical Data. Breast Cancer Res. 2014, 16, 419. [Google Scholar] [CrossRef] [PubMed]
- Nami, B.; Maadi, H.; Wang, Z. Mechanisms Underlying the Action and Synergism of Trastuzumab and Pertuzumab in Targeting HER2-Positive Breast Cancer. Cancers 2018, 10, 342. [Google Scholar] [CrossRef] [PubMed]
- Samiei, S.; Simons, J.M.; Engelen, S.M.E.; Beets-Tan, R.G.H.; Classe, J.-M.; Smidt, M.L. EUBREAST Group Axillary Pathologic Complete Response After Neoadjuvant Systemic Therapy by Breast Cancer Subtype in Patients with Initially Clinically Node-Positive Disease: A Systematic Review and Meta-Analysis. JAMA Surg. 2021, 156, e210891. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and Safety of Neoadjuvant Pertuzumab and Trastuzumab in Women with Locally Advanced, Inflammatory, or Early HER2-Positive Breast Cancer (NeoSphere): A Randomised Multicentre, Open-Label, Phase 2 Trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Starosławska, E.; de la Haba-Rodriguez, J.; Im, S.-A.; Pedrini, J.L.; et al. 5-Year Analysis of Neoadjuvant Pertuzumab and Trastuzumab in Patients with Locally Advanced, Inflammatory, or Early-Stage HER2-Positive Breast Cancer (NeoSphere): A Multicentre, Open-Label, Phase 2 Randomised Trial. Lancet Oncol. 2016, 17, 791–800. [Google Scholar] [CrossRef]
- Shao, Z.; Pang, D.; Yang, H.; Li, W.; Wang, S.; Cui, S.; Liao, N.; Wang, Y.; Wang, C.; Chang, Y.-C.; et al. Efficacy, Safety, and Tolerability of Pertuzumab, Trastuzumab, and Docetaxel for Patients with Early or Locally Advanced ERBB2-Positive Breast Cancer in Asia: The PEONY Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e193692. [Google Scholar] [CrossRef]
- Huang, L.; Pang, D.; Yang, H.; Li, W.; Wang, S.; Cui, S.; Liao, N.; Wang, Y.; Wang, C.; Chang, Y.-C.; et al. Neoadjuvant–Adjuvant Pertuzumab in HER2-Positive Early Breast Cancer: Final Analysis of the Randomized Phase III PEONY Trial. Nat. Commun. 2024, 15, 2153. [Google Scholar] [CrossRef]
- Swain, S.M.; Ewer, M.S.; Viale, G.; Delaloge, S.; Ferrero, J.-M.; Verrill, M.; Colomer, R.; Vieira, C.; Werner, T.L.; Douthwaite, H.; et al. Pertuzumab, Trastuzumab, and Standard Anthracycline- and Taxane-Based Chemotherapy for the Neoadjuvant Treatment of Patients with HER2-Positive Localized Breast Cancer (BERENICE): A Phase II, Open-Label, Multicenter, Multinational Cardiac Safety Study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 646–653. [Google Scholar] [CrossRef]
- Dang, C.; Ewer, M.S.; Delaloge, S.; Ferrero, J.-M.; Colomer, R.; de la Cruz-Merino, L.; Werner, T.L.; Dadswell, K.; Verrill, M.; Eiger, D.; et al. BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer. Cancers 2022, 14, 2596. [Google Scholar] [CrossRef]
- Panet, F.; Young, M.; Wong, S.; Dragomir, A.; Rose, A.A.N.; Panasci, L. Abstract P2-01-06: Real-World Outcome and Cost Analysis of the Addition of Pertuzumab to Neoadjuvant Therapy in Localized HER2 Positive Breast Cancer: A Single Center Experience. Cancer Res. 2023, 83, P2-01–P2-06. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Waldron-Lynch, M.; Eng-Wong, J.; Kirk, S.; Cortés, J. Long-Term Efficacy Analysis of the Randomised, Phase II TRYPHAENA Cardiac Safety Study: Evaluating Pertuzumab and Trastuzumab plus Standard Neoadjuvant Anthracycline-Containing and Anthracycline-Free Chemotherapy Regimens in Patients with HER2-Positive Early Breast Cancer. Eur. J. Cancer Oxf. Engl. 2018, 89, 27–35. [Google Scholar] [CrossRef]
- van Ramshorst, M.S.; van der Voort, A.; van Werkhoven, E.D.; Mandjes, I.A.; Kemper, I.; Dezentjé, V.O.; Oving, I.M.; Honkoop, A.H.; Tick, L.W.; van de Wouw, A.J.; et al. Neoadjuvant Chemotherapy with or without Anthracyclines in the Presence of Dual HER2 Blockade for HER2-Positive Breast Cancer (TRAIN-2): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2018, 19, 1630–1640. [Google Scholar] [CrossRef]
- van der Voort, A.; van Ramshorst, M.S.; van Werkhoven, E.D.; Mandjes, I.A.; Kemper, I.; Vulink, A.J.; Oving, I.M.; Honkoop, A.H.; Tick, L.W.; van de Wouw, A.J.; et al. Three-Year Follow-up of Neoadjuvant Chemotherapy With or Without Anthracyclines in the Presence of Dual ERBB2 Blockade in Patients with ERBB2-Positive Breast Cancer: A Secondary Analysis of the TRAIN-2 Randomized, Phase 3 Trial. JAMA Oncol. 2021, 7, 978–984. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.F.; Ratnayake, J.; et al. Pertuzumab plus Trastuzumab in Combination with Standard Neoadjuvant Anthracycline-Containing and Anthracycline-Free Chemotherapy Regimens in Patients with HER2-Positive Early Breast Cancer: A Randomized Phase II Cardiac Safety Study (TRYPHAENA). Ann. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E.; et al. Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer. N. Engl. J. Med. 2017, 377, 122–131. [Google Scholar] [CrossRef]
- Piccart, M.; Procter, M.; Fumagalli, D.; de Azambuja, E.; Clark, E.; Ewer, M.S.; Restuccia, E.; Jerusalem, G.; Dent, S.; Reaby, L.; et al. Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer in the APHINITY Trial: 6 Years’ Follow-Up. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Holmes, F.A.; Ejlertsen, B.; Delaloge, S.; Moy, B.; Iwata, H.; von Minckwitz, G.; Chia, S.K.L.; Mansi, J.; Barrios, C.H.; et al. Neratinib after Trastuzumab-Based Adjuvant Therapy in HER2-Positive Breast Cancer (ExteNET): 5-Year Analysis of a Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2017, 18, 1688–1700. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Moy, B.; Mansi, J.; Ejlertsen, B.; Holmes, F.A.; Chia, S.; Iwata, H.; Gnant, M.; Loibl, S.; Barrios, C.H.; et al. Final Efficacy Results of Neratinib in HER2-Positive Hormone Receptor-Positive Early-Stage Breast Cancer From the Phase III ExteNET Trial. Clin. Breast Cancer 2021, 21, 80–91.e7. [Google Scholar] [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.-B.; Im, Y.-H.; Im, S.-A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, Trastuzumab, and Docetaxel for HER2-Positive Metastatic Breast Cancer (CLEOPATRA): End-of-Study Results from a Double-Blind, Randomised, Placebo-Controlled, Phase 3 Study. Lancet Oncol. 2020, 21, 519–530. [Google Scholar] [CrossRef]
- Baselga, J.; Cortés, J.; Kim, S.-B.; Im, S.-A.; Hegg, R.; Im, Y.-H.; Roman, L.; Pedrini, J.L.; Pienkowski, T.; Knott, A.; et al. Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer. N. Engl. J. Med. 2012, 366, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.; Ciruelos, E.; Schneeweiss, A.; Puglisi, F.; Peretz-Yablonski, T.; Campone, M.; Bondarenko, I.; Nowecki, Z.; Errihani, H.; Paluch-Shimon, S.; et al. Final Results from the PERUSE Study of First-Line Pertuzumab plus Trastuzumab plus a Taxane for HER2-Positive Locally Recurrent or Metastatic Breast Cancer, with a Multivariable Approach to Guide Prognostication. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Rimawi, M.; Ferrero, J.-M.; De La Haba-Rodriguez, J.; Poole, C.; De Placido, S.; Osborne, C.K.; Hegg, R.; Easton, V.; Wohlfarth, C.; Arpino, G.; et al. First-Line Trastuzumab Plus an Aromatase Inhibitor, With or Without Pertuzumab, in Human Epidermal Growth Factor Receptor 2–Positive and Hormone Receptor–Positive Metastatic or Locally Advanced Breast Cancer (PERTAIN): A Randomized, Open-Label Phase II Trial. J. Clin. Oncol. 2018, 36, 2826–2835. [Google Scholar] [CrossRef] [PubMed]
- Nicolò, E.; Zagami, P.; Curigliano, G. Antibody-Drug Conjugates in Breast Cancer: The Chemotherapy of the Future? Curr. Opin. Oncol. 2020, 32, 494–502. [Google Scholar] [CrossRef]
- Hurvitz, S.A.; Hegg, R.; Chung, W.-P.; Im, S.-A.; Jacot, W.; Ganju, V.; Chiu, J.W.Y.; Xu, B.; Hamilton, E.; Madhusudan, S.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine in Patients with HER2-Positive Metastatic Breast Cancer: Updated Results from DESTINY-Breast03, a Randomised, Open-Label, Phase 3 Trial. Lancet 2023, 401, 105–117. [Google Scholar] [CrossRef]
- Cortés, J.; Hurvitz, S.A.; Im, S.-A.; Iwata, H.; Curigliano, G.; Kim, S.-B.; Chiu, J.W.Y.; Pedrini, J.L.; Li, W.; Yonemori, K.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine in HER2-Positive Metastatic Breast Cancer: Long-Term Survival Analysis of the DESTINY-Breast03 Trial. Nat. Med. 2024, 30, 2208–2215. [Google Scholar] [CrossRef]
- Powell, C.A.; Modi, S.; Iwata, H.; Takahashi, S.; Smit, E.F.; Siena, S.; Chang, D.-Y.; Macpherson, E.; Qin, A.; Singh, J.; et al. Pooled Analysis of Drug-Related Interstitial Lung Disease and/or Pneumonitis in Nine Trastuzumab Deruxtecan Monotherapy Studies. ESMO Open 2022, 7, 100554. [Google Scholar] [CrossRef]
- Henning, J.-W.; Brezden-Masley, C.; Gelmon, K.; Chia, S.; Shapera, S.; McInnis, M.; Rayson, D.; Asselah, J. Managing the Risk of Lung Toxicity with Trastuzumab Deruxtecan (T-DXd): A Canadian Perspective. Curr. Oncol. 2023, 30, 8019–8038. [Google Scholar] [CrossRef] [PubMed]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef]
- André, F.; Park, Y.H.; Kim, S.-B.; Takano, T.; Im, S.-A.; Borges, G.; Lima, J.P.; Aksoy, S.; Gregori, J.G.; Laurentiis, M.D.; et al. Trastuzumab Deruxtecan versus Treatment of Physician’s Choice in Patients with HER2-Positive Metastatic Breast Cancer (DESTINY-Breast02): A Randomised, Open-Label, Multicentre, Phase 3 Trial. Lancet 2023, 401, 1773–1785. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Modi, S.; Krop, I.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Iwata, H.; Tsurutani, J.; Sohn, J.; Mathias, E.; et al. Trastuzumab Deruxtecan in Previously Treated Patients with HER2-Positive Metastatic Breast Cancer: Updated Survival Results from a Phase II Trial (DESTINY-Breast01). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2024, 35, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Krop, I.E.; Kim, S.-B.; Martin, A.G.; LoRusso, P.M.; Ferrero, J.-M.; Badovinac-Crnjevic, T.; Hoersch, S.; Smitt, M.; Wildiers, H. Trastuzumab Emtansine versus Treatment of Physician’s Choice in Patients with Previously Treated HER2-Positive Metastatic Breast Cancer (TH3RESA): Final Overall Survival Results from a Randomised Open-Label Phase 3 Trial. Lancet Oncol. 2017, 18, 743–754. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Tolaney, S.M.; Wardley, A.M.; Zambelli, S.; Hilton, J.F.; Troso-Sandoval, T.A.; Ricci, F.; Im, S.-A.; Kim, S.-B.; Johnston, S.R.; Chan, A.; et al. Abemaciclib plus Trastuzumab with or without Fulvestrant versus Trastuzumab plus Standard-of-Care Chemotherapy in Women with Hormone Receptor-Positive, HER2-Positive Advanced Breast Cancer (monarcHER): A Randomised, Open-Label, Phase 2 Trial. Lancet Oncol. 2020, 21, 763–775. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Oliveira, M.; Feng, Y.-H.; Dai, M.-S.; Chen, S.-W.; Hurvitz, S.A.; Kim, S.-B.; Moy, B.; Delaloge, S.; Gradishar, W.; et al. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated with ≥ 2 HER2-Directed Regimens: Phase III NALA Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 3138–3149. [Google Scholar] [CrossRef]
- Geyer, C.E.; Forster, J.; Lindquist, D.; Chan, S.; Romieu, C.G.; Pienkowski, T.; Jagiello-Gruszfeld, A.; Crown, J.; Chan, A.; Kaufman, B.; et al. Lapatinib plus Capecitabine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2006, 355, 2733–2743. [Google Scholar] [CrossRef]
- Rugo, H.S.; Im, S.-A.; Cardoso, F.; Cortés, J.; Curigliano, G.; Musolino, A.; Pegram, M.D.; Wright, G.S.; Saura, C.; Escrivá-de-Romaní, S.; et al. Efficacy of Margetuximab vs. Trastuzumab in Patients with Pretreated ERBB2-Positive Advanced Breast Cancer: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 573–584. [Google Scholar] [CrossRef]
- Gabos, Z.; Sinha, R.; Hanson, J.; Chauhan, N.; Hugh, J.; Mackey, J.R.; Abdulkarim, B. Prognostic Significance of Human Epidermal Growth Factor Receptor Positivity for the Development of Brain Metastasis After Newly Diagnosed Breast Cancer. J. Clin. Oncol. 2006, 24, 5658–5663. [Google Scholar] [CrossRef]
- Darlix, A.; Louvel, G.; Fraisse, J.; Jacot, W.; Brain, E.; Debled, M.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; Delaloge, S.; et al. Impact of Breast Cancer Molecular Subtypes on the Incidence, Kinetics and Prognosis of Central Nervous System Metastases in a Large Multicentre Real-Life Cohort. Br. J. Cancer 2019, 121, 991–1000. [Google Scholar] [CrossRef]
- Kuksis, M.; Gao, Y.; Tran, W.; Hoey, C.; Kiss, A.; Komorowski, A.S.; Dhaliwal, A.J.; Sahgal, A.; Das, S.; Chan, K.K.; et al. The Incidence of Brain Metastases among Patients with Metastatic Breast Cancer: A Systematic Review and Meta-Analysis. Neuro-Oncology 2021, 23, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Rosen, M.N.; Chehade, R.; Sahgal, A.; Das, S.; Warner, E.; Saskin, R.; Zhang, B.; Soliman, H.; Chan, K.K.W.; et al. Analysis of Rates of Brain Metastases and Association with Breast Cancer Subtypes in Ontario, Canada. JAMA Netw. Open 2022, 5, e2225424. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S. Phase III Study of Adjuvant Ado-Trastuzumab Emtansine vs. Trastuzumab for Residual Invasive HER2-Positive Early Breast Cancer after Neoadjuvant Chemotherapy and HER2-Targeted Therapy: KATHERINE Final IDFS and Updated OS Analysis. In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 5–9 December 2023. [Google Scholar]
- Brufsky, A.M.; Mayer, M.; Rugo, H.S.; Kaufman, P.A.; Tan-Chiu, E.; Tripathy, D.; Tudor, I.C.; Wang, L.I.; Brammer, M.G.; Shing, M.; et al. Central Nervous System Metastases in Patients with HER2-Positive Metastatic Breast Cancer: Incidence, Treatment, and Survival in Patients from registHER. Clin. Cancer Res. 2011, 17, 4834–4843. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, D.; Darlix, A.; Louvel, G.; Fraisse, J.; Jacot, W.; Brain, E.; Petit, A.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; et al. Treatment and Outcomes in Patients with Central Nervous System Metastases from Breast Cancer in the Real-Life ESME MBC Cohort. Eur. J. Cancer Oxf. Engl. 2020, 125, 22–30. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Cancer Clinical Trial Eligibility Criteria: Brain Metastases Guidance for Industry; U.S. Department of Health and Human Services: Washington, DC, USA, 2020.
- Achrol, A.S.; Rennert, R.C.; Anders, C.; Soffietti, R.; Ahluwalia, M.S.; Nayak, L.; Peters, S.; Arvold, N.D.; Harsh, G.R.; Steeg, P.S.; et al. Brain Metastases. Nat. Rev. Dis. Primer 2019, 5, 5. [Google Scholar] [CrossRef]
- Murthy, R.K.; O’Brien, B.; Berry, D.A.; Singareeka-Raghavendra, A.; Monroe, M.G.; Johnson, J.; White, J.; Childress, J.; Sanford, J.; Schwartz-Gomez, J.; et al. Abstract PD4-02: Safety and Efficacy of a Tucatinib-Trastuzumab-Capecitabine Regimen for Treatment of Leptomeningeal Metastasis (LM) in HER2-Positive Breast Cancer: Results from TBCRC049, a Phase 2 Non-Randomized Study. Cancer Res. 2022, 82, PD4-02. [Google Scholar] [CrossRef]
- Yang, T.J.; Wijetunga, N.A.; Yamada, J.; Wolden, S.; Mehallow, M.; Goldman, D.A.; Zhang, Z.; Young, R.J.; Kris, M.G.; Yu, H.A.; et al. Clinical Trial of Proton Craniospinal Irradiation for Leptomeningeal Metastases. Neuro-Oncology 2021, 23, 134–143. [Google Scholar] [CrossRef]
- Ramakrishna, N.; Anders, C.K.; Lin, N.U.; Morikawa, A.; Temin, S.; Chandarlapaty, S.; Crews, J.R.; Davidson, N.E.; Franzoi, M.A.B.; Kirshner, J.J.; et al. Management of Advanced Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer and Brain Metastases: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 2636–2655. [Google Scholar] [CrossRef]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef]
- Kim, G.M.; Sohn, J.H.; Kim, M.H.; Kim, S.-G.; Park, H.S.; Jang, J.H.; Kim, Y.B.; Lee, S. Clinical Impact of Routine MRI Screening for Brain Metastases in Patients with HER2 Positive or Triple Negative Metastatic Breast Cancer. Cancer Res. 2024, 84, PO2-27-09. [Google Scholar] [CrossRef]
- Soon, Y.Y.; Tham, I.W.K.; Lim, K.H.; Koh, W.Y.; Lu, J.J. Surgery or Radiosurgery plus Whole Brain Radiotherapy versus Surgery or Radiosurgery Alone for Brain Metastases. Cochrane Database Syst. Rev. 2014, 2016, CD009454. [Google Scholar] [CrossRef] [PubMed]
- Fleege, N.M.G.; Pierce-Gjeldum, D.; Swartz, L.K.; Verbal, K.; Merajver, S.; Friese, C.R.; Kiyota, A.; Heth, J.; Leung, D.; Smith, S.R.; et al. IMPACT the Brain: A Team-Based Approach to Management of Metastatic Breast Cancer with CNS Metastases. JCO Oncol. Pract. 2023, 19, e67–e77. [Google Scholar] [CrossRef] [PubMed]
- Lievens, Y.; Guckenberger, M.; Gomez, D.; Hoyer, M.; Iyengar, P.; Kindts, I.; Méndez Romero, A.; Nevens, D.; Palma, D.; Park, C.; et al. Defining Oligometastatic Disease from a Radiation Oncology Perspective: An ESTRO-ASTRO Consensus Document. Radiother. Oncol. 2020, 148, 157–166. [Google Scholar] [CrossRef]
- Merloni, F.; Palleschi, M.; Casadei, C.; Romeo, A.; Curcio, A.; Casadei, R.; Stella, F.; Ercolani, G.; Gianni, C.; Sirico, M.; et al. Oligometastatic Breast Cancer and Metastasis-Directed Treatment: An Aggressive Multimodal Approach to Reach the Cure. Ther. Adv. Med. Oncol. 2023, 15, 175883592311614. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, R.; Berghoff, A.S.; Furtner, J.; Marhold, M.; Bergen, E.S.; Roider-Schur, S.; Mair, M.J.; Starzer, A.M.; Forstner, H.; Rottenmanner, B.; et al. Final Outcome Analysis from the Phase II TUXEDO-1 Trial of Trastuzumab-Deruxtecan in HER2-Positive Breast Cancer Patients with Active Brain Metastases. Neuro-Oncology 2024, 2024, noae123. [Google Scholar] [CrossRef]
- Lebow, E.S.; Pike, L.R.G.; Seidman, A.D.; Moss, N.; Beal, K.; Yu, Y. Symptomatic Necrosis with Antibody-Drug Conjugates and Concurrent Stereotactic Radiotherapy for Brain Metastases. JAMA Oncol. 2023, 9, 1729. [Google Scholar] [CrossRef]
- AstraZeneca Canada Inc. ENHERTU (Trastuzumab Deruxtecan) Product Monograph; AstraZeneca Canada Inc.: Mississauga, ON, Canada, 2024. [Google Scholar]
- Hoffmann-La Roche Ltd. KADCYLA (Trastuzumab Emtansine) Product Monograph; Hoffmann-La Roche Ltd.: Basel, Switzerland, 2022. [Google Scholar]
- Swain, S.M.; Baselga, J.; Miles, D.; Im, Y.-H.; Quah, C.; Lee, L.F.; Cortés, J. Incidence of Central Nervous System Metastases in Patients with HER2-Positive Metastatic Breast Cancer Treated with Pertuzumab, Trastuzumab, and Docetaxel: Results from the Randomized Phase III Study CLEOPATRA. Ann. Oncol. 2014, 25, 1116–1121. [Google Scholar] [CrossRef]
- Bachelot, T.; Ciruelos, E.; Schneeweiss, A.; Puglisi, F.; Peretz-Yablonski, T.; Bondarenko, I.; Paluch-Shimon, S.; Wardley, A.; Merot, J.-L.; du Toit, Y.; et al. Preliminary Safety and Efficacy of First-Line Pertuzumab Combined with Trastuzumab and Taxane Therapy for HER2-Positive Locally Recurrent or Metastatic Breast Cancer (PERUSE). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 766–773. [Google Scholar] [CrossRef]
- Harbeck, N.; Ciruelos, E.; Jerusalem, G.; Müller, V.; Niikura, N.; Viale, G.; Bartsch, R.; Kurzeder, C.; Higgins, M.J.; Connolly, R.M.; et al. Trastuzumab Deruxtecan in HER2-Positive Advanced Breast Cancer with or without Brain Metastases: A Phase 3b/4 Trial. Nat. Med. 2024. [Google Scholar] [CrossRef]
- Niikura, N.; Yamanaka, T.; Nomura, H.; Shiraishi, K.; Kusama, H.; Yamamoto, M.; Matsuura, K.; Inoue, K.; Takahara, S.; Kita, S.; et al. Treatment with Trastuzumab Deruxtecan in Patients with HER2-Positive Breast Cancer and Brain Metastases and/or Leptomeningeal Disease (ROSET-BM). NPJ Breast Cancer 2023, 9, 82. [Google Scholar] [CrossRef]
- Yan, F.; Rinn, K.J.; Kullnat, J.A.; Wu, A.Y.; Ennett, M.D.; Scott, E.L.; Kaplan, H.G. Response of Leptomeningeal Metastasis of Breast Cancer with a HER2/Neu Activating Variant to Tucatinib: A Case Report. J. Natl. Compr. Cancer Netw. 2022, 20, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.U.; Borges, V.; Anders, C.; Murthy, R.K.; Paplomata, E.; Hamilton, E.; Hurvitz, S.; Loi, S.; Okines, A.; Abramson, V.; et al. Intracranial Efficacy and Survival with Tucatinib Plus Trastuzumab and Capecitabine for Previously Treated HER2-Positive Breast Cancer with Brain Metastases in the HER2CLIMB Trial. J. Clin. Oncol. 2020, 38, 2610–2619. [Google Scholar] [CrossRef] [PubMed]
- Mudgway, R.; Chavez de Paz Villanueva, C.; Lin, A.C.; Senthil, M.; Garberoglio, C.A.; Lum, S.S. The Impact of Primary Tumor Surgery on Survival in HER2 Positive Stage IV Breast Cancer Patients in the Current Era of Targeted Therapy. Ann. Surg. Oncol. 2020, 27, 2711–2720. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Jia, L.; Yang, R.; Liu, Y.; Lv, Z.; Cui, J. Primary Site Surgery of de Novo Stage IV HER2-Positive Breast Cancer in the Era of New Drug Treatments. Front. Oncol. 2024, 13, 1308854. [Google Scholar] [CrossRef] [PubMed]
- Soran, A.; Ozmen, V.; Ozbas, S.; Karanlik, H.; Muslumanoglu, M.; Igci, A.; Canturk, N.Z.; Utkan, Z.; Evrensel, T.; Sezgin, E. Primary Surgery with Systemic Therapy in Patients with de Novo Stage IV Breast Cancer: 10-Year Follow-up; Protocol MF07-01 Randomized Clinical Trial. J. Am. Coll. Surg. 2021, 233, 742–751.e5. [Google Scholar] [CrossRef]
- Badwe, R.; Hawaldar, R.; Nair, N.; Kaushik, R.; Parmar, V.; Siddique, S. Locoregional Treatment versus No Treatment of the Primary Tumour in Metastatic Breast Cancer: An Open-Label Randomised Controlled Trial. Lancet Oncol. 2015, 16, 1380–1388. [Google Scholar] [CrossRef]
- Patel, G.; Kishore Reddy, B.V.; Patil, P. Is Surgical Management of Primary Beneficial in Metastatic Breast Cancer? Indian J. Surg. Oncol. 2021, 12, 421–427. [Google Scholar] [CrossRef]

| Recommendations for Early Breast Cancer | REAL | ESMO | ASCO | |
|---|---|---|---|---|
| 1 | cT1a and b, cN0 For patients with HER2+ early breast cancer cT1a and b (i.e., ≤1 cm) without evidence of nodal disease (cN0), the standard of care is timely surgery followed by adjuvant treatment depending on the pathologic staging of disease (see Recommendations 3–5). | Strong recommendation ●● |  cT1 cN0 | |
| 2 | cT1c, cN0 For patients with HER2+ early breast cancer cT1c (i.e., >1 to ≤2 cm) without evidence of nodal disease (cN0), the standard of care is surgery followed by adjuvant treatment. However, due to current global practices, consideration can be given to neoadjuvant treatment followed by surgery and adjuvant treatment. | Strong recommendation ●● Strong consideration ○○ | NC No specific guideline for cT1c | For high-risk node-negative disease, pertuzumab may be used with trastuzumab |
| 3 | pT1, pN0 For patients with HER2+ early breast cancer with pT1 without evidence of nodal disease (pN0), the standard of care adjuvant systemic treatment is paclitaxel + trastuzumab for 12 weeks followed by trastuzumab monotherapy for 9 months. | Strong recommendation ●● | | |
| 4 | ≥pT2, pN0 Although neoadjuvant treatment is preferred, for those patients who are treated with upfront surgery and are then found to have ≥pT2 pN0 disease, the standard of care is adjuvant chemotherapy + trastuzumab. | Strong recommendation ●● | | |
| 5 | ≥cT2 or cN+ For patients with HER2+ early breast cancer with ≥cT2 or those with nodal disease (cN+), the standard of care is neoadjuvant therapy with trastuzumab + pertuzumab + chemotherapy. | Strong recommendation ●● | | |
| 6 | pN+ Although neoadjuvant treatment is preferred, for those patients who are treated with upfront surgery and are then found to have nodal disease in the pathological specimen (pN+), the standard of care is adjuvant chemotherapy + trastuzumab with consideration given to the addition of pertuzumab. | Strong consideration ○○ | Chemo + HP followed by HP to complete the year | |
| 7 | Pathologic complete response For patients with HER2+ early breast cancer in whom a pathologic complete response is determined in the surgical specimen after completion of neoadjuvant trastuzumab + pertuzumab + chemotherapy, the standard of care is trastuzumab for a total of 1 year. | Strong recommendation ●● | If cN0 at initial diagnosis If cN+ at initial diagnosis, then HP | |
| 8 | Residual invasive disease For patients with HER2+ early breast cancer in whom residual invasive disease is detected pathologically in the surgical specimen of the breast or axillary lymph nodes after completion of neoadjuvant trastuzumab + pertuzumab + chemotherapy, the standard of care is to treat with trastuzumab emtansine (T-DM1) for 14 cycles in the adjuvant setting. | Strong recommendation ●● | | |
| 9 | Hormone receptor-positive disease Although there is not a survival benefit, for patients with HER2+ HR+ and N+ disease who have completed (neo)adjuvant chemotherapy + trastuzumab, extended adjuvant treatment with neratinib for 1 year after completion of trastuzumab-based adjuvant therapy can be considered to decrease recurrence. | Moderate recommendation ● | | |
 , alignment; NC, not covered. Pink text describes the tumour and nodal status, and bolded text describes the patient. ASCO, American Society of Medical Oncology; ESMO, European Society of Medical Oncology; HP, trastuzumab + pertuzumab; HR, hormone receptor.
, alignment; NC, not covered. Pink text describes the tumour and nodal status, and bolded text describes the patient. ASCO, American Society of Medical Oncology; ESMO, European Society of Medical Oncology; HP, trastuzumab + pertuzumab; HR, hormone receptor.| Recommendations for Metastatic Breast Cancer | Strength of Recommendation | ESMO | ASCO | |
|---|---|---|---|---|
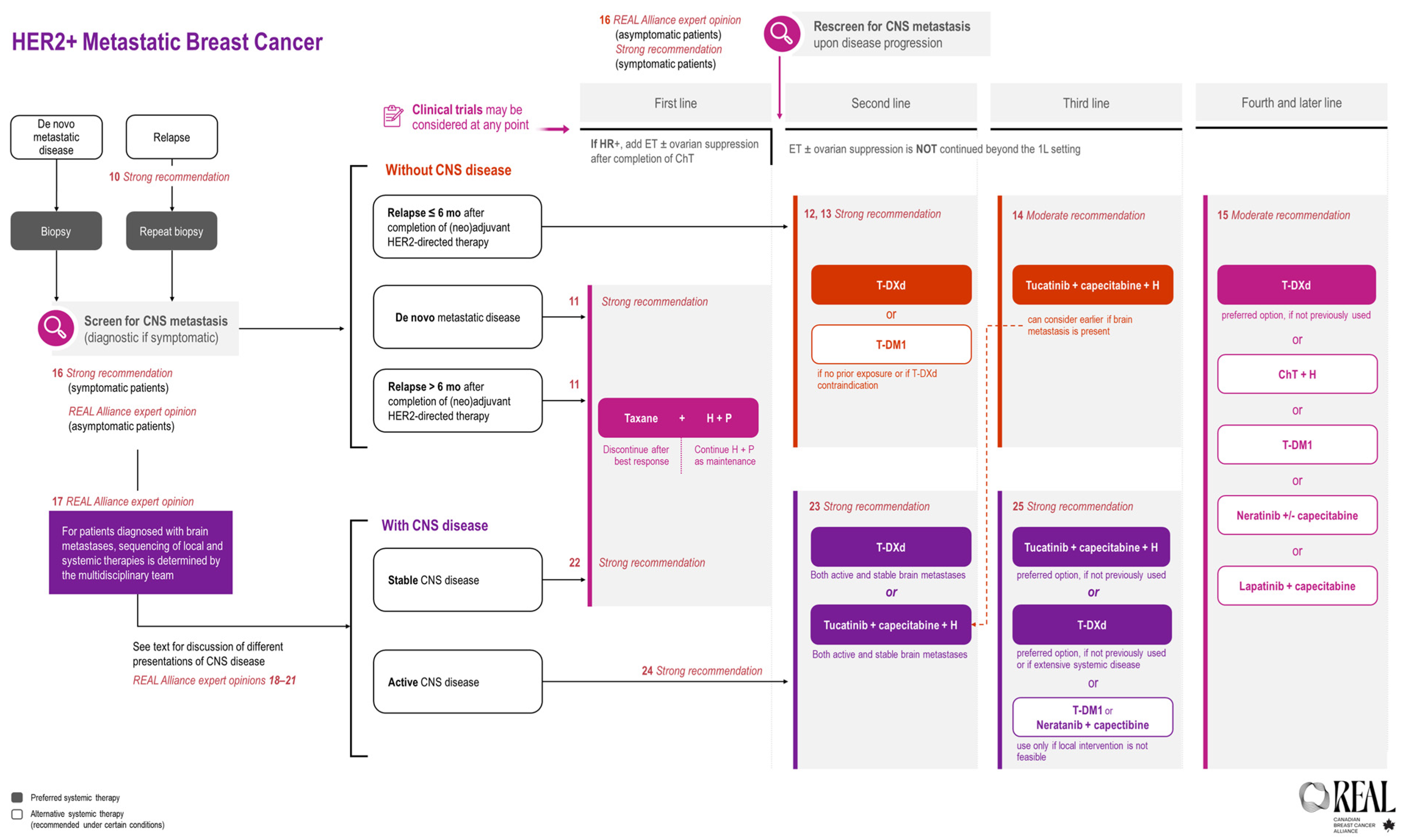
| 10 | Repeat biopsy When safe and feasible, repeat biopsy should be performed in all patients whose disease relapses on or after adjuvant treatment. | Strong recommendation ●● | | |
| 11 | 1L treatment late relapse For patients with de novo HER2+ (HR±) metastatic breast cancer who have not received prior HER2-directed therapy or chemotherapy for metastatic disease or with disease that relapses >6 months after completion of (neo)adjuvant chemotherapy + HER2-directed therapy, the standard of care is trastuzumab + pertuzumab + taxane chemotherapy followed by trastuzumab + pertuzumab +/− ET maintenance therapy. | Strong recommendation ●● | | |
| 12 | 1L treatment early relapse For patients with HER2-positive (HR±) metastatic breast cancer whose disease relapses ≤6 months after completion of (neo)adjuvant chemotherapy + HER2-directed therapy, the recommended treatment is as per the second-line recommendation (see Recommendation 13). | Strong recommendation ●● | (relapse ≤ 12 mos) | |
| 13 | 2L treatment For patients with HER2-positive metastatic breast cancer whose disease has progressed on first-line HER2-directed therapy, the standard of care is trastuzumab deruxtecan (T-DXd) in the absence of contraindications. | Strong recommendation ●● | | |
| 14 | 3L treatment For patients with HER2+ metastatic breast cancer whose disease has progressed after at least 2 HER2-directed therapies the recommendation for treatment is tucatinib + capecitabine + trastuzumab (can be considered earlier if brain metastasis is present). | Moderate recommendation ● | | |
| 15 | 4L and later treatment For patients with HER2+ metastatic breast cancer whose disease has progressed after at least 3 HER2-directed therapies, the recommendation based on evidence is to continue HER2-directed therapy. Options include T-DXd (preferred option, if not previously used); chemotherapy + trastuzumab or another monoclonal antibody; trastuzumab emtansine (T-DM1); neratinib +/- capecitabine; and lapatinib + capecitabine. | Moderate recommendation ● | | |
, alignment; NC, not covered. Pink text describes the tumour and nodal status, and bolded text describes the patient. 1L, first-line; 2L, second-line; 3L, third-line; 4L, fourth-line; ASCO, American Society of Medical Oncology; ESMO, European Society of Medical Oncology.| Recommendations for Brain Metastases | Strength of Recommendation | ESMO | ASCO | |
|---|---|---|---|---|
| 16 | CNS screening For patients with HER2+ metastatic breast cancer who have symptoms suggestive of CNS metastases, appropriate diagnostic investigations for CNS metastases are essential. | Strong recommendation ●● REAL Alliance expert opinion ○ | If detection of CNS metastases will alter the choice of systemic therapy |  |
| For patients with HER2+ metastatic breast cancer, screening for CNS metastases should be considered in asymptomatic patients at baseline in the metastatic setting and at disease progression. | ||||
| 17 | Multidisciplinary care For patients with a history of HER2+ metastatic breast cancer who are diagnosed with brain metastases, multidisciplinary care with representation from radiology, radiation oncology, neurosurgery, medical oncology, and supportive care is the standard of care, with the multidisciplinary team providing recommendations on sequencing of local and systemic therapies. | REAL Alliance expert opinion ○ | NC | NC |
| 18 | Characteristics of CNS disease at screening For patients with a history of HER2+ metastatic breast cancer but without other extracranial systemic disease who present with oligometastatic brain disease amenable to local therapy, there is insufficient evidence to make a recommendation for a change in systemic therapy. Multidisciplinary care is the standard of care, and the multidisciplinary team is to make recommendations on sequencing of local and systemic therapies in such patients. | REAL Alliance expert opinion ○ | NC | NC |
| 19 | Characteristics of CNS disease at screening For patients with a history of HER2+ metastatic disease who present with asymptomatic, low volume, newly diagnosed brain metastases, treatment should be discussed by MDT incorporating patient values with treatment options including initial HER2-directed systemic therapy versus upfront local therapy. | REAL Alliance expert opinion ○ | NC | NC |
| 20 | Characteristics of CNS disease at screening For patients with a history of HER2+ metastatic disease who present with symptomatic, newly diagnosed brain metastases, upfront stereotactic radiosurgery is a reasonable approach when technically feasible (and often preferred over whole brain radiotherapy). | REAL Alliance expert opinion ○ | NC | NC |
| 21 | Characteristics of CNS disease at screening For patients with HER2+ metastatic breast cancer with parenchymal CNS disease, the decision to offer systemic therapy prior to local therapies should be individualized for each patient and ideally discussed at multi-disciplinary rounds. Key considerations include tumour burden and clinical symptoms. A multidisciplinary approach should be conducted to confirm if and when systemic therapy should be held during local CNS therapy to reduce the risk of toxicities and tumour necrosis. | REAL Alliance expert opinion ○ | NC | NC |
| 22 | 1L treatment stable brain metastases For patients with HER+ metastatic breast cancer with active or progressive systemic disease in the presence of treated brain metastases, the standard of care in the first line setting is trastuzumab + pertuzumab + taxane. | Strong recommendation ●● | | |
| 23 | 2L treatment stable brain metastases For patients with HER2+ metastatic breast cancer with stable brain metastases whose disease has progressed on first line therapy, the standard of care options are trastuzumab deruxtecan (T-DXd [preferred]), or tucatinib + capecitabine + trastuzumab. | Strong recommendation ●● | | |
| 24 | 2L treatment active brain metastases For patients with HER2+ metastatic breast cancer and asymptomatic active (i.e., untreated) or stable brain metastases where local therapy is not indicated and whose disease has progressed on first-line therapy, options include tucatinib + capecitabine + trastuzumab or T-DXd. Such cases should be reviewed by the multidisciplinary team to determine sequencing of local and systemic therapies. | Strong recommendation ●● | | |
| 25 | 3L treatment For patients with HER2+ metastatic breast cancer and active brain metastases whose disease has progressed on second-line systemic therapy, the standard of care is tucatinib + capecitabine + trastuzumab (preferred if not used in second line) or T-DXd (preferred if not used in second line or if there are signs of extensive systemic disease) | Strong recommendation ●● | NC | |
, alignment;  , some variation; NC, not covered. Pink text describes the tumour and nodal status, and bolded text describes the patient. 1L, first-line; 2L, second-line; 3L, third-line; ASCO, American Society of Medical Oncology; ESMO, European Society of Medical Oncology.
, some variation; NC, not covered. Pink text describes the tumour and nodal status, and bolded text describes the patient. 1L, first-line; 2L, second-line; 3L, third-line; ASCO, American Society of Medical Oncology; ESMO, European Society of Medical Oncology.| Antibody–Drug Conjugate | Trastuzumab Deruxtecan [83] | Trastuzumab Emtansine [84] |
|---|---|---|
| Half life | 5.6 days | 3.1 to 4.5 days |
| Recommendations for Other Areas of Interest | Strength of Recommendation | ESMO | ASCO | |
|---|---|---|---|---|
| 26 | Drug holiday In patients with HER2+ metastatic breast cancer, a drug holiday can be considered in cases where there is stable disease based on imaging. | REAL Alliance expert opinion ○ | NC | NC |
| 27 | Multidisciplinary care In patients with HER2+ de novo metastatic breast cancer, who have a clinical complete response in the metastatic sites from chemotherapy + HER2-directed therapy and whose PET scan is negative, but who have breast-only residual disease, surgery can be considered at the site of the primary tumour to obtain no evidence of disease. | REAL Alliance expert opinion ○ | NC | NC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manna, M.; Gelmon, K.A.; Boileau, J.-F.; Brezden-Masley, C.; Cao, J.Q.; Jerzak, K.J.; Prakash, I.; Sehdev, S.; Simmons, C.; Bouganim, N.; et al. Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2+ Breast Cancer in Both the Early and Metastatic Setting. Curr. Oncol. 2024, 31, 6536-6567. https://doi.org/10.3390/curroncol31110484
Manna M, Gelmon KA, Boileau J-F, Brezden-Masley C, Cao JQ, Jerzak KJ, Prakash I, Sehdev S, Simmons C, Bouganim N, et al. Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2+ Breast Cancer in Both the Early and Metastatic Setting. Current Oncology. 2024; 31(11):6536-6567. https://doi.org/10.3390/curroncol31110484
Chicago/Turabian StyleManna, Mita, Karen A. Gelmon, Jean-François Boileau, Christine Brezden-Masley, Jeffrey Q. Cao, Katarzyna J. Jerzak, Ipshita Prakash, Sandeep Sehdev, Christine Simmons, Nathaniel Bouganim, and et al. 2024. "Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2+ Breast Cancer in Both the Early and Metastatic Setting" Current Oncology 31, no. 11: 6536-6567. https://doi.org/10.3390/curroncol31110484
APA StyleManna, M., Gelmon, K. A., Boileau, J.-F., Brezden-Masley, C., Cao, J. Q., Jerzak, K. J., Prakash, I., Sehdev, S., Simmons, C., Bouganim, N., Brackstone, M., Cescon, D. W., Chia, S., Dayes, I. S., Edwards, S., Hilton, J., Joy, A. A., Laing, K., Webster, M., & Henning, J.-W. (2024). Guidance for Canadian Breast Cancer Practice: National Consensus Recommendations for the Systemic Treatment of Patients with HER2+ Breast Cancer in Both the Early and Metastatic Setting. Current Oncology, 31(11), 6536-6567. https://doi.org/10.3390/curroncol31110484