Counselling Framework for Germline BRCA1/2 and PALB2 Carriers Considering Risk-Reducing Mastectomy

Abstract
1. Introduction
2. Risk Reduction with Mastectomy
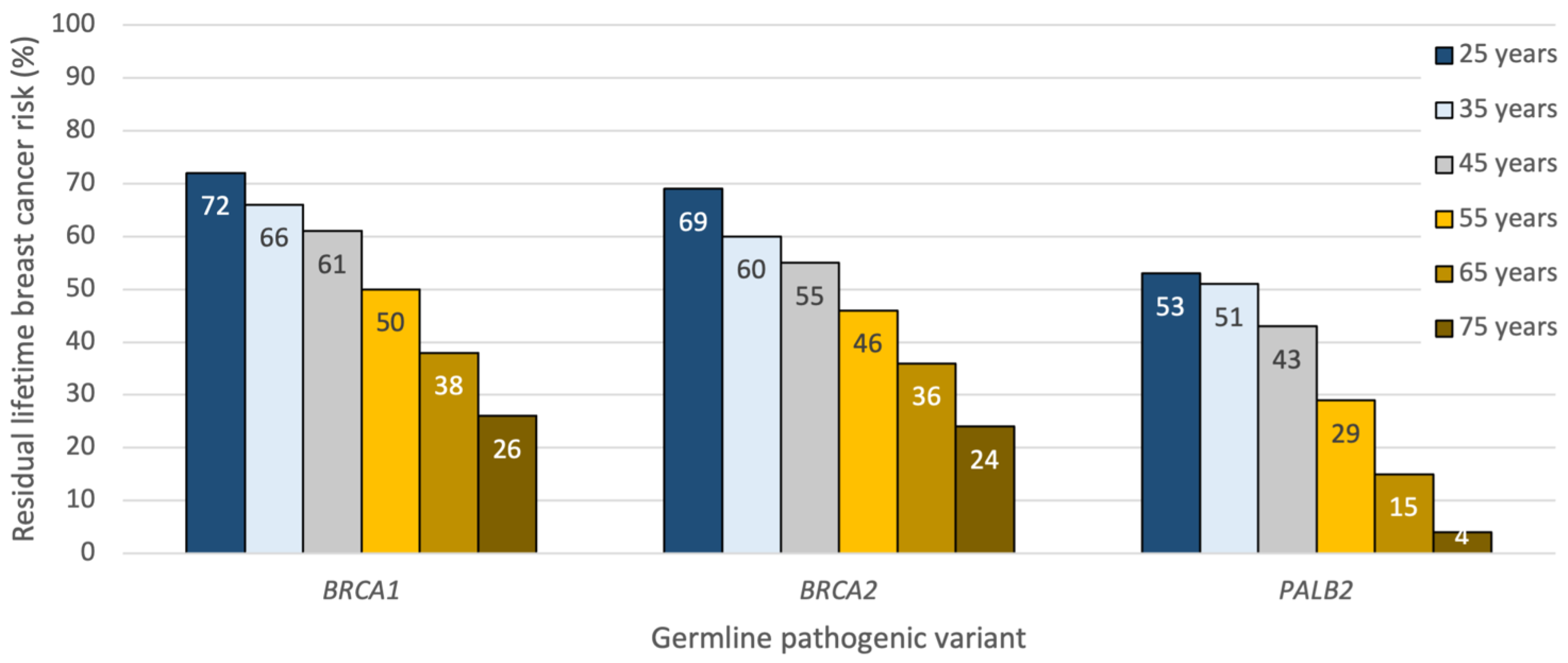
2.1. Residual Lifetime Risk and Risk Reduction following Bilateral Mastectomy in Unaffected Carriers
2.2. Ipsilateral and Contralateral Breast Cancer Risk in Affected Carriers with a History of Breast Cancer
2.3. Breast Cancer Risk in Affected Carriers with a History of Ovarian Cancer
3. Survival following Mastectomy
4. Uptake of Risk-Reducing Mastectomy
5. Skin- versus Nipple-Sparing Mastectomy
6. Axillary Staging and Occult Breast Cancer at the Time of RRM
7. Reconstructive Options
8. Supplemental Surgery after Risk-Reducing Mastectomy
9. Sensation after Mastectomy
10. Psychological Outcomes following Risk-Reducing Mastectomy
11. Postmastectomy Surveillance
12. Nipple Discharge and Pregnancy-Related Changes following Risk-Reducing Mastectomy
13. Future Directions: Sensation-Sparing and Robotic Nipple-Sparing Mastectomy
14. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Leslie, G.; Doroszuk, A.; Schneider, S.; Allen, J.; Decker, B.; Dunning, A.M.; Redman, J.; Scarth, J.; Plaskocinska, I.; et al. Cancer Risks Associated With Germline PALB2 Pathogenic Variants: An International Study of 524 Families. J. Clin. Oncol. 2020, 38, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, L.C.; Lindor, N.M. The Role of Risk-Reducing Surgery in Hereditary Breast and Ovarian Cancer. N. Engl. J. Med. 2016, 374, 454–468. [Google Scholar] [CrossRef] [PubMed]
- Braun, D.; Yang, J.; Griffin, M.; Parmigiani, G.; Hughes, K.S. A Clinical Decision Support Tool to Predict Cancer Risk for Commonly Tested Cancer-Related Germline Mutations. J. Genet. Couns. 2018, 27, 1187–1199. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, L.C.; Sellers, T.A.; Schaid, D.J.; Frank, T.S.; Soderberg, C.L.; Sitta, D.L.; Frost, M.H.; Grant, C.S.; Donohue, J.H.; Woods, J.E.; et al. Efficacy of bilateral prophylactic mastectomy in BRCA1 and BRCA2 gene mutation carriers. J. Natl. Cancer Inst. 2001, 93, 1633–1637. [Google Scholar] [CrossRef] [PubMed]
- Meijers-Heijboer, H.; van Geel, B.; van Putten, W.L.; Henzen-Logmans, S.C.; Seynaeve, C.; Menke-Pluymers, M.B.; Bartels, C.C.; Verhoog, L.C.; van den Ouweland, A.M.; Niermeijer, M.F.; et al. Breast cancer after prophylactic bilateral mastectomy in women with a BRCA1 or BRCA2 mutation. N. Engl. J. Med. 2001, 345, 159–164. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Friebel, T.; Lynch, H.T.; Neuhausen, S.L.; van ‘t Veer, L.; Garber, J.E.; Evans, G.R.; Narod, S.A.; Isaacs, C.; Matloff, E.; et al. Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: The PROSE Study Group. J. Clin. Oncol. 2004, 22, 1055–1062. [Google Scholar] [CrossRef]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef]
- Skytte, A.B.; Cruger, D.; Gerster, M.; Laenkholm, A.V.; Lang, C.; Brondum-Nielsen, K.; Andersen, M.K.; Sunde, L.; Kolvraa, S.; Gerdes, A.M. Breast cancer after bilateral risk-reducing mastectomy. Clin. Genet. 2011, 79, 431–437. [Google Scholar] [CrossRef]
- Carbine, N.E.; Lostumbo, L.; Wallace, J.; Ko, H. Risk-reducing mastectomy for the prevention of primary breast cancer. Cochrane Database Syst. Rev. 2018, 4, CD002748. [Google Scholar] [CrossRef] [PubMed]
- Heemskerk-Gerritsen, B.A.; Brekelmans, C.T.; Menke-Pluymers, M.B.; van Geel, A.N.; Tilanus-Linthorst, M.M.; Bartels, C.C.; Tan, M.; Meijers-Heijboer, H.E.; Klijn, J.G.; Seynaeve, C. Prophylactic mastectomy in BRCA1/2 mutation carriers and women at risk of hereditary breast cancer: Long-term experiences at the Rotterdam Family Cancer Clinic. Ann. Surg. Oncol. 2007, 14, 3335–3344. [Google Scholar] [CrossRef] [PubMed]
- Kaidar-Person, O.; Boersma, L.J.; Poortmans, P.; Sklair-Levy, M.; Offersen, B.V.; Cardoso, M.J.; de Ruysscher, D. Residual Glandular Breast Tissue After Mastectomy: A Systematic Review. Ann. Surg. Oncol. 2020, 27, 2288–2296. [Google Scholar] [CrossRef]
- Papassotiropoulos, B.; Guth, U.; Chiesa, F.; Rageth, C.; Amann, E.; Baege, A.; Elfgen, C.; Varga, Z.; Moskovszky, L.; Endhardt, K.; et al. Prospective Evaluation of Residual Breast Tissue After Skin- or Nipple-Sparing Mastectomy: Results of the SKINI-Trial. Ann. Surg. Oncol. 2019, 26, 1254–1262. [Google Scholar] [CrossRef]
- Heemskerk-Gerritsen, B.A.M.; Jager, A.; Koppert, L.B.; Obdeijn, A.I.; Collee, M.; Meijers-Heijboer, H.E.J.; Jenner, D.J.; Oldenburg, H.S.A.; van Engelen, K.; de Vries, J.; et al. Survival after bilateral risk-reducing mastectomy in healthy BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2019, 177, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Tung, N.; Lin, N.U.; Kidd, J.; Allen, B.A.; Singh, N.; Wenstrup, R.J.; Hartman, A.R.; Winer, E.P.; Garber, J.E. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients With Breast Cancer. J. Clin. Oncol. 2016, 34, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Couch, F.J.; Shimelis, H.; Hu, C.; Hart, S.N.; Polley, E.C.; Na, J.; Hallberg, E.; Moore, R.; Thomas, A.; Lilyquist, J.; et al. Associations Between Cancer Predisposition Testing Panel Genes and Breast Cancer. JAMA Oncol. 2017, 3, 1190–1196. [Google Scholar] [CrossRef]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef]
- Webster, A.J.; Shanno, J.N.; Santa Cruz, H.S.; Kelly, B.N.; Garstka, M.; Henriquez, A.; Specht, M.C.; Gadd, M.A.; Verdial, F.C.; Nguyen, A.; et al. Oncologic Safety of Nipple-Sparing Mastectomy for Breast Cancer in BRCA Gene Mutation Carriers: Outcomes at 70 Months Median Follow-Up. Ann. Surg. Oncol. 2023, 30, 3215–3222. [Google Scholar] [CrossRef]
- Shubeck, S.; Sevilimedu, V.; Berger, E.; Robson, M.; Heerdt, A.S.; Pilewskie, M.L. Comparison of Outcomes Between BRCA Pathogenic Variant Carriers Undergoing Breast-Conserving Surgery Versus Mastectomy. Ann. Surg. Oncol. 2022, 29, 4706–4713. [Google Scholar] [CrossRef]
- Taghian, A.; Jeong, J.H.; Mamounas, E.; Anderson, S.; Bryant, J.; Deutsch, M.; Wolmark, N. Patterns of locoregional failure in patients with operable breast cancer treated by mastectomy and adjuvant chemotherapy with or without tamoxifen and without radiotherapy: Results from five National Surgical Adjuvant Breast and Bowel Project randomized clinical trials. J. Clin. Oncol. 2004, 22, 4247–4254. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P.; Anderson, S.J.; Dignam, J.J.; Bear, H.D.; Julian, T.B.; Geyer, C.E., Jr.; Taghian, A.; Wickerham, D.L.; Wolmark, N. Predictors of locoregional recurrence after neoadjuvant chemotherapy: Results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J. Clin. Oncol. 2012, 30, 3960–3966. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Boddicker, N.J.; Na, J.; Polley, E.C.; Hu, C.; Hart, S.N.; Gnanaolivu, R.D.; Larson, N.; Holtegaard, S.; Huang, H.; et al. Contralateral Breast Cancer Risk Among Carriers of Germline Pathogenic Variants in ATM, BRCA1, BRCA2, CHEK2, and PALB2. J. Clin. Oncol. 2023, 41, 1703–1713. [Google Scholar] [CrossRef] [PubMed]
- Gangi, A.; Cass, I.; Paik, D.; Barmparas, G.; Karlan, B.; Dang, C.; Li, A.; Walsh, C.; Rimel, B.J.; Amersi, F.F. Breast cancer following ovarian cancer in BRCA mutation carriers. JAMA Surg. 2014, 149, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Nanez, A.; Stram, D.A.; Bethan Powell, C.; Garcia, C. Breast cancer risk in BRCA mutation carriers after diagnosis of epithelial ovarian cancer is lower than in carriers without ovarian cancer. Gynecol. Oncol. Rep. 2022, 39, 100899. [Google Scholar] [CrossRef] [PubMed]
- Domchek, S.M.; Jhaveri, K.; Patil, S.; Stopfer, J.E.; Hudis, C.; Powers, J.; Stadler, Z.; Goldstein, L.; Kauff, N.; Khasraw, M.; et al. Risk of metachronous breast cancer after BRCA mutation-associated ovarian cancer. Cancer 2013, 119, 1344–1348. [Google Scholar] [CrossRef] [PubMed]
- Vencken, P.M.; Kriege, M.; Hooning, M.; Menke-Pluymers, M.B.; Heemskerk-Gerritsen, B.A.; van Doorn, L.C.; Collee, M.M.; Jager, A.; van Montfort, C.; Burger, C.W.; et al. The risk of primary and contralateral breast cancer after ovarian cancer in BRCA1/BRCA2 mutation carriers: Implications for counseling. Cancer 2013, 119, 955–962. [Google Scholar] [CrossRef]
- McGee, J.; Giannakeas, V.; Karlan, B.; Lubinski, J.; Gronwald, J.; Rosen, B.; McLaughlin, J.; Risch, H.; Sun, P.; Foulkes, W.D.; et al. Risk of breast cancer after a diagnosis of ovarian cancer in BRCA mutation carriers: Is preventive mastectomy warranted? Gynecol. Oncol. 2017, 145, 346–351. [Google Scholar] [CrossRef]
- John, C.S.; Fong, A.; Alban, R.; Gillen, J.; Moore, K.M.; Walsh, C.S.; Li, A.J.; Rimel, B.J.; Amersi, F.; Cass, I. Breast cancer surveillance following ovarian cancer in BRCA mutation carriers. Gynecol. Oncol. 2022, 164, 202–207. [Google Scholar] [CrossRef]
- Candido-dos-Reis, F.J.; Song, H.; Goode, E.L.; Cunningham, J.M.; Fridley, B.L.; Larson, M.C.; Alsop, K.; Dicks, E.; Harrington, P.; Ramus, S.J.; et al. Germline mutation in BRCA1 or BRCA2 and ten-year survival for women diagnosed with epithelial ovarian cancer. Clin. Cancer Res. 2015, 21, 652–657. [Google Scholar] [CrossRef]
- Banerjee, S.; Moore, K.N.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; et al. Maintenance olaparib for patients with newly diagnosed advanced ovarian cancer and a BRCA mutation (SOLO1/GOG 3004): 5-year follow-up of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Heemskerk-Gerritsen, B.A.; Menke-Pluijmers, M.B.; Jager, A.; Tilanus-Linthorst, M.M.; Koppert, L.B.; Obdeijn, I.M.; van Deurzen, C.H.; Collee, J.M.; Seynaeve, C.; Hooning, M.J. Substantial breast cancer risk reduction and potential survival benefit after bilateral mastectomy when compared with surveillance in healthy BRCA1 and BRCA2 mutation carriers: A prospective analysis. Ann. Oncol. 2013, 24, 2029–2035. [Google Scholar] [CrossRef] [PubMed]
- Ingham, S.L.; Sperrin, M.; Baildam, A.; Ross, G.L.; Clayton, R.; Lalloo, F.; Buchan, I.; Howell, A.; Evans, D.G. Risk-reducing surgery increases survival in BRCA1/2 mutation carriers unaffected at time of family referral. Breast Cancer Res. Treat. 2013, 142, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Sigal, B.M.; Plevritis, S.K. Survival analysis of cancer risk reduction strategies for BRCA1/2 mutation carriers. J. Clin. Oncol. 2010, 28, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Giannakeas, V.; Narod, S.A. The expected benefit of preventive mastectomy on breast cancer incidence and mortality in BRCA mutation carriers, by age at mastectomy. Breast Cancer Res. Treat. 2018, 167, 263–267. [Google Scholar] [CrossRef]
- Grann, V.R.; Jacobson, J.S.; Thomason, D.; Hershman, D.; Heitjan, D.F.; Neugut, A.I. Effect of prevention strategies on survival and quality-adjusted survival of women with BRCA1/2 mutations: An updated decision analysis. J. Clin. Oncol. 2002, 20, 2520–2529. [Google Scholar] [CrossRef]
- Neven, P.; Punie, K.; Wildiers, H.; Willers, N.; Van Ongeval, C.; Van Buggenhout, G.; Legius, E. Risk-reducing mastectomy in BRCA carriers: Survival is not the issue. Breast Cancer Res. Treat. 2020, 179, 251–252. [Google Scholar] [CrossRef]
- Mavaddat, N.; Barrowdale, D.; Andrulis, I.L.; Domchek, S.M.; Eccles, D.; Nevanlinna, H.; Ramus, S.J.; Spurdle, A.; Robson, M.; Sherman, M.; et al. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: Results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol. Biomark. Prev. 2012, 21, 134–147. [Google Scholar] [CrossRef]
- Metcalfe, K.; Gershman, S.; Ghadirian, P.; Lynch, H.T.; Snyder, C.; Tung, N.; Kim-Sing, C.; Eisen, A.; Foulkes, W.D.; Rosen, B.; et al. Contralateral mastectomy and survival after breast cancer in carriers of BRCA1 and BRCA2 mutations: Retrospective analysis. BMJ 2014, 348, g226. [Google Scholar] [CrossRef]
- Antill, Y.; Reynolds, J.; Young, M.A.; Kirk, J.; Tucker, K.; Bogtstra, T.; Wong, S.; Dudding, T.; Di Iulio, J.; Phillips, K.A. Risk-reducing surgery in women with familial susceptibility for breast and/or ovarian cancer. Eur. J. Cancer 2006, 42, 621–628. [Google Scholar] [CrossRef]
- Haroun, I.; Graham, T.; Poll, A.; Sun, P.; Hill, K.; Weitzner, E.; Narod, S.; Warner, E. Reasons for risk-reducing mastectomy versus MRI-screening in a cohort of women at high hereditary risk of breast cancer. Breast 2011, 20, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, E.; Zabor, E.C.; Stempel, M.; Mangino, D.; Heerdt, A.; Pilewskie, M. Differences Among a Modern Cohort of BRCA Mutation Carriers Choosing Bilateral Prophylactic Mastectomies Compared to Breast Surveillance. Ann. Surg. Oncol. 2017, 24, 3048–3054. [Google Scholar] [CrossRef] [PubMed]
- Galmor, L.; Bernstein-Molho, R.; Sklair-Levy, M.; Madoursky-Feldman, D.; Zippel, D.; Laitman, Y.; Friedman, E. Time trends in uptake rates of risk-reducing mastectomy in Israeli asymptomatic BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2021, 185, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Lalloo, F.; Ashcroft, L.; Shenton, A.; Clancy, T.; Baildam, A.D.; Brain, A.; Hopwood, P.; Howell, A. Uptake of risk-reducing surgery in unaffected women at high risk of breast and ovarian cancer is risk, age, and time dependent. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2318–2324. [Google Scholar] [CrossRef] [PubMed]
- Marcinkute, R.; Woodward, E.R.; Gandhi, A.; Howell, S.; Crosbie, E.J.; Wissely, J.; Harvey, J.; Highton, L.; Murphy, J.; Holland, C.; et al. Uptake and efficacy of bilateral risk reducing surgery in unaffected female BRCA1 and BRCA2 carriers. J. Med. Genet. 2022, 59, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Eisen, A.; Senter, L.; Armel, S.; Bordeleau, L.; Meschino, W.S.; Pal, T.; Lynch, H.T.; Tung, N.M.; Kwong, A.; et al. International trends in the uptake of cancer risk reduction strategies in women with a BRCA1 or BRCA2 mutation. Br. J. Cancer 2019, 121, 15–21. [Google Scholar] [CrossRef]
- Flippo-Morton, T.; Walsh, K.; Chambers, K.; Amacker-North, L.; White, B.; Sarantou, T.; Boselli, D.M.; White, R.L., Jr. Surgical Decision Making in the BRCA-Positive Population: Institutional Experience and Comparison with Recent Literature. Breast J. 2016, 22, 35–44. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Birenbaum-Carmeli, D.; Lubinski, J.; Gronwald, J.; Lynch, H.; Moller, P.; Ghadirian, P.; Foulkes, W.D.; Klijn, J.; Friedman, E.; et al. International variation in rates of uptake of preventive options in BRCA1 and BRCA2 mutation carriers. Int. J. Cancer 2008, 122, 2017–2022. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.M.; Ryu, J.M.; Park, H.S.; Park, J.S.; Kang, E.; Lee, S.; Lee, H.B.; Youn, H.J.; Yoo, T.K.; Kim, J.; et al. Trends in Risk-Reducing Mastectomy and Risk-Reducing Salpingo-Oophorectomy in Korean Carriers of the BRCA1/2 Mutation. J. Breast Cancer 2020, 23, 647–655. [Google Scholar] [CrossRef]
- Skytte, A.B.; Gerdes, A.M.; Andersen, M.K.; Sunde, L.; Brondum-Nielsen, K.; Waldstrom, M.; Kolvraa, S.; Cruger, D. Risk-reducing mastectomy and salpingo-oophorectomy in unaffected BRCA mutation carriers: Uptake and timing. Clin. Genet. 2010, 77, 342–349. [Google Scholar] [CrossRef]
- Petelin, L.; Hossack, L.; Mitchell, G.; Liew, D.; Trainer, A.H.; James, P.A. A Microsimulation Model for Evaluating the Effectiveness of Cancer Risk Management for BRCA Pathogenic Variant Carriers: miBRovaCAre. Value Health 2019, 22, 854–862. [Google Scholar] [CrossRef]
- Singer, C.F.; Muhr, D.; Rappaport, C.; Tea, M.K.; Gschwantler-Kaulich, D.; Fink-Retter, A.; Pfeiler, G.; Berger, A.; Sun, P.; Narod, S.A. Clinical implications of genetic testing for BRCA1 and BRCA2 mutations in Austria. Clin. Genet. 2014, 85, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Evans, T.G.; Bailey, D.; Lewis, M.H.; Gower-Thomas, K.; Murray, A. Uptake of risk-reducing surgery in BRCA gene carriers in Wales, UK. Breast J. 2018, 24, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Peled, A.W.; Irwin, C.S.; Hwang, E.S.; Ewing, C.A.; Alvarado, M.; Esserman, L.J. Total skin-sparing mastectomy in BRCA mutation carriers. Ann. Surg. Oncol. 2014, 21, 37–41. [Google Scholar] [CrossRef] [PubMed]
- de Alcantara Filho, P.; Capko, D.; Barry, J.M.; Morrow, M.; Pusic, A.; Sacchini, V.S. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: The Memorial Sloan-Kettering Cancer Center experience. Ann. Surg. Oncol. 2011, 18, 3117–3122. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.; Davidson, J.A.; Lindor, N.M.; Glazebrook, K.N.; Jakub, J.W.; Degnim, A.C.; Sandhu, N.P.; Walsh, M.F.; Hartmann, L.C.; Boughey, J.C. Prophylactic and therapeutic mastectomy in BRCA mutation carriers: Can the nipple be preserved? Ann. Surg. Oncol. 2011, 18, 3102–3109. [Google Scholar] [CrossRef]
- Yao, K.; Liederbach, E.; Tang, R.; Lei, L.; Czechura, T.; Sisco, M.; Howard, M.; Hulick, P.J.; Weissman, S.; Winchester, D.J.; et al. Nipple-sparing mastectomy in BRCA1/2 mutation carriers: An interim analysis and review of the literature. Ann. Surg. Oncol. 2015, 22, 370–376. [Google Scholar] [CrossRef]
- Valero, M.G.; Moo, T.A.; Muhsen, S.; Zabor, E.C.; Stempel, M.; Pusic, A.; Gemignani, M.L.; Morrow, M.; Sacchini, V. Use of bilateral prophylactic nipple-sparing mastectomy in patients with high risk of breast cancer. Br. J. Surg. 2020, 107, 1307–1312. [Google Scholar] [CrossRef]
- Wei, C.H.; Scott, A.M.; Price, A.N.; Miller, H.C.; Klassen, A.F.; Jhanwar, S.M.; Mehrara, B.J.; Disa, J.J.; McCarthy, C.; Matros, E.; et al. Psychosocial and Sexual Well-Being Following Nipple-Sparing Mastectomy and Reconstruction. Breast J. 2016, 22, 10–17. [Google Scholar] [CrossRef]
- Didier, F.; Radice, D.; Gandini, S.; Bedolis, R.; Rotmensz, N.; Maldifassi, A.; Santillo, B.; Luini, A.; Galimberti, V.; Scaffidi, E.; et al. Does nipple preservation in mastectomy improve satisfaction with cosmetic results, psychological adjustment, body image and sexuality? Breast Cancer Res. Treat. 2009, 118, 623–633. [Google Scholar] [CrossRef]
- Hartmann, L.C.; Schaid, D.J.; Woods, J.E.; Crotty, T.P.; Myers, J.L.; Arnold, P.G.; Petty, P.M.; Sellers, T.A.; Johnson, J.L.; McDonnell, S.K.; et al. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N. Engl. J. Med. 1999, 340, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Rusby, J.E.; Brachtel, E.F.; Michaelson, J.S.; Koerner, F.C.; Smith, B.L. Breast duct anatomy in the human nipple: Three-dimensional patterns and clinical implications. Breast Cancer Res. Treat. 2007, 106, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Rusby, J.E.; Kirstein, L.J.; Brachtel, E.F.; Michaelson, J.S.; Koerner, F.C.; Smith, B.L. Nipple-sparing mastectomy: Lessons from ex vivo procedures. Breast J. 2008, 14, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Grinstein, O.; Krug, B.; Hellmic, M.; Siedek, F.; Malter, W.; Burke, C.; Schmutzler, R.; Maintz, D.; Rhiem, K. Residual glandular tissue (RGT) in BRCA1/2 germline mutation carriers with unilateral and bilateral prophylactic mastectomies. Surg. Oncol. 2019, 29, 126–133. [Google Scholar] [CrossRef]
- Baltzer, H.L.; Alonzo-Proulx, O.; Mainprize, J.G.; Yaffe, M.J.; Metcalfe, K.A.; Narod, S.A.; Warner, E.; Semple, J.L. MRI volumetric analysis of breast fibroglandular tissue to assess risk of the spared nipple in BRCA1 and BRCA2 mutation carriers. Ann. Surg. Oncol. 2014, 21, 1583–1588. [Google Scholar] [CrossRef]
- Garstka, M.; Henriquez, A.; Kelly, B.N.; Webster, A.; Khubchandani, J.A.; Hughes, K.; Nguyen, A.; Oseni, T.; Specht, M.; Coopey, S.B.; et al. How Protective are Nipple-Sparing Prophylactic Mastectomies in BRCA1 and BRCA2 Mutation Carriers? Ann. Surg. Oncol. 2021, 28, 5657–5662. [Google Scholar] [CrossRef]
- Jakub, J.W.; Peled, A.W.; Gray, R.J.; Greenup, R.A.; Kiluk, J.V.; Sacchini, V.; McLaughlin, S.A.; Tchou, J.C.; Vierkant, R.A.; Degnim, A.C.; et al. Oncologic Safety of Prophylactic Nipple-Sparing Mastectomy in a Population With BRCA Mutations: A Multi-institutional Study. JAMA Surg. 2018, 153, 123–129. [Google Scholar] [CrossRef]
- Kaas, R.; Verhoef, S.; Wesseling, J.; Rookus, M.A.; Oldenburg, H.S.; Peeters, M.J.; Rutgers, E.J. Prophylactic mastectomy in BRCA1 and BRCA2 mutation carriers: Very low risk for subsequent breast cancer. Ann. Surg. 2010, 251, 488–492. [Google Scholar] [CrossRef]
- Wong, S.M.; Ferroum, A.; Apostolova, C.; Alhassan, B.; Prakash, I.; Basik, M.; Boileau, J.F.; Meterissian, S.; Aleynikova, O.; Wong, N.; et al. Incidence of Occult Breast Cancer in Carriers of BRCA1/2 or Other High-Penetrance Pathogenic Variants Undergoing Prophylactic Mastectomy: When is Sentinel Lymph Node Biopsy Indicated? Ann. Surg. Oncol. 2022, 29, 6660–6668. [Google Scholar] [CrossRef]
- Karakatsanis, A.; Hersi, A.F.; Pistiolis, L.; Olofsson Bagge, R.; Lykoudis, P.M.; Eriksson, S.; Warnberg, F.; SentiNot Trialists, G. Effect of preoperative injection of superparamagnetic iron oxide particles on rates of sentinel lymph node dissection in women undergoing surgery for ductal carcinoma in situ (SentiNot study). Br. J. Surg. 2019, 106, 720–728. [Google Scholar] [CrossRef]
- Jazrawi, A.; Warnberg, M.; Hersi, A.F.; Obondo, C.; Pistioli, L.; Eriksson, S.; Karakatsanis, A.; Warnberg, F. A Comparison of Skin Staining after Sentinel Lymph Node Biopsy in Women Undergoing Breast Cancer Surgery Using Blue Dye and Superparamagnetic Iron Oxide Nanoparticle (SPIO) Tracers. Cancers 2022, 14, 6017. [Google Scholar] [CrossRef] [PubMed]
- Sigalove, S.; Maxwell, G.P.; Sigalove, N.M.; Storm-Dickerson, T.L.; Pope, N.; Rice, J.; Gabriel, A. Prepectoral Implant-Based Breast Reconstruction: Rationale, Indications, and Preliminary Results. Plast. Reconstr. Surg. 2017, 139, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Cammarata, E.; Toia, F.; Rossi, M.; Cipolla, C.; Vieni, S.; Speciale, A.; Cordova, A. Implant-Based Breast Reconstruction after Risk-Reducing Mastectomy in BRCA Mutation Carriers: A Single-Center Retrospective Study. Healthcare 2023, 11, 1741. [Google Scholar] [CrossRef] [PubMed]
- Antony, A.K.; Poirier, J.; Madrigrano, A.; Kopkash, K.A.; Robinson, E.C. Evolution of the Surgical Technique for “Breast in a Day” Direct-to-Implant Breast Reconstruction: Transitioning from Dual-Plane to Prepectoral Implant Placement. Plast. Reconstr. Surg. 2019, 143, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Caputo, G.G.; Zingaretti, N.; Kiprianidis, I.; Zanfisi, C.; Domenici, L.; Parodi, P.C.; Governa, M. Quality of Life and Early Functional Evaluation in Direct-to-Implant Breast Reconstruction After Mastectomy: A Comparative Study Between Prepectoral Versus Dual-Plane Reconstruction. Clin. Breast Cancer 2021, 21, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Holland, M.; Su, P.; Piper, M.; Withers, J.; Harbell, M.W.; Bokoch, M.P.; Sbitany, H. Prepectoral Breast Reconstruction Reduces Opioid Consumption and Pain After Mastectomy: A Head-to-Head Comparison With Submuscular Reconstruction. Ann. Plast. Surg. 2022, 89, 492–499. [Google Scholar] [CrossRef]
- Spear, S.L.; Coles, C.N.; Leung, B.K.; Gitlin, M.; Parekh, M.; Macarios, D. The Safety, Effectiveness, and Efficiency of Autologous Fat Grafting in Breast Surgery. Plast. Reconstr. Surg. Glob. Open 2016, 4, e827. [Google Scholar] [CrossRef]
- Arver, B.; Isaksson, K.; Atterhem, H.; Baan, A.; Bergkvist, L.; Brandberg, Y.; Ehrencrona, H.; Emanuelsson, M.; Hellborg, H.; Henriksson, K.; et al. Bilateral prophylactic mastectomy in Swedish women at high risk of breast cancer: A national survey. Ann. Surg. 2011, 253, 1147–1154. [Google Scholar] [CrossRef]
- Fijany, A.J.; Friedlich, N.; Olsson, S.E.; Bishay, A.E.; Pekarev, M. Current Trends in Autologous Breast Reconstruction and the Implications of Impending Changes to Insurance Reimbursement. Cureus 2023, 15, e43855. [Google Scholar] [CrossRef]
- Santosa, K.B.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Long-term Patient-Reported Outcomes in Postmastectomy Breast Reconstruction. JAMA Surg. 2018, 153, 891–899. [Google Scholar] [CrossRef]
- Domchek, S.M. Risk-Reducing Mastectomy in BRCA1 and BRCA2 Mutation Carriers: A Complex Discussion. JAMA 2019, 321, 27. [Google Scholar] [CrossRef] [PubMed]
- Richardson, H.; Ma, G. The Goldilocks mastectomy. Int. J. Surg. 2012, 10, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Richardson, H.; Aronowitz, J.A. Goldilocks Mastectomy with Bilateral In Situ Nipple Preservation Via Dermal Pedicle. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1748. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, A.; Oliver, J.D.; Vyas, K.S.; Alsubaie, S.A.; Manrique, O.J.; Martinez-Jorge, J. Outcomes analysis of Goldilocks mastectomy and breast reconstruction: A single institution experience of 96 cases. J. Surg. Oncol. 2019, 119, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.D.; Skowronksi, P.P. Extending the Indications for Autologous Breast Reconstruction Using a Two-Stage Modified Goldilocks Procedure: A Case Report. Breast J. 2017, 23, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Nurudeen, S.; Guo, H.; Chun, Y.; Coopey, S.; Barry, W.; Garber, J.; Dominici, L.S. Patient experience with breast reconstruction process following bilateral mastectomy in BRCA mutation carriers. Am. J. Surg. 2017, 214, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Moberg, I.O.; Schou Bredal, I.; Schneider, M.R.; Tonseth, K.A.; Schlichting, E. Complications, risk factors, and patients-reported outcomes after skin-sparing mastectomy followed by breast reconstruction in women with BRCA mutations. J. Plast. Surg. Hand Surg. 2018, 52, 234–239. [Google Scholar] [CrossRef]
- Zion, S.M.; Slezak, J.M.; Sellers, T.A.; Woods, J.E.; Arnold, P.G.; Petty, P.M.; Donohue, J.H.; Frost, M.H.; Schaid, D.J.; Hartmann, L.C. Reoperations after prophylactic mastectomy with or without implant reconstruction. Cancer 2003, 98, 2152–2160. [Google Scholar] [CrossRef]
- Apostolova, C.; Ferroum, A.; Alhassan, B.; Prakash, I.; Viezel-Mathieu, A.; Basik, M.; Boileau, J.F.; Meterissian, S.; Wong, N.; Foulkes, W.D.; et al. Surgical Decision Making in Genetically High-Risk Women: Quantifying Postoperative Complications and Long-Term Risks of Supplemental Surgery After Risk-Reducing Mastectomy. Ann. Surg. Oncol. 2023, 31, 356–364. [Google Scholar] [CrossRef]
- Schlenz, I.; Kuzbari, R.; Gruber, H.; Holle, J. The sensitivity of the nipple-areola complex: An anatomic study. Plast. Reconstr. Surg. 2000, 105, 905–909. [Google Scholar] [CrossRef]
- Hammond, J.B.; Kandi, L.A.; Armstrong, V.L.; Kosiorek, H.E.; Rebecca, A.M.; Casey, W.J., 3rd; Kruger, E.A.; Cronin, P.A.; Pockaj, B.A.; Teven, C.M. Long-term breast and nipple sensation after nipple-sparing mastectomy with implant reconstruction: Relevance to physical, psychosocial, and sexual well-being. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 2914–2919. [Google Scholar] [CrossRef]
- Dossett, L.A.; Lowe, J.; Sun, W.; Lee, M.C.; Smith, P.D.; Jacobsen, P.B.; Laronga, C. Prospective evaluation of skin and nipple-areola sensation and patient satisfaction after nipple-sparing mastectomy. J. Surg. Oncol. 2016, 114, 11–16. [Google Scholar] [CrossRef]
- Yueh, J.H.; Houlihan, M.J.; Slavin, S.A.; Lee, B.T.; Pories, S.E.; Morris, D.J. Nipple-sparing mastectomy: Evaluation of patient satisfaction, aesthetic results, and sensation. Ann. Plast. Surg. 2009, 62, 586–590. [Google Scholar] [CrossRef]
- Djohan, R.; Gage, E.; Gatherwright, J.; Pavri, S.; Firouz, J.; Bernard, S.; Yetman, R. Patient satisfaction following nipple-sparing mastectomy and immediate breast reconstruction: An 8-year outcome study. Plast. Reconstr. Surg. 2010, 125, 818–829. [Google Scholar] [CrossRef]
- Gahm, J.; Jurell, G.; Wickman, M.; Hansson, P. Sensitivity after bilateral prophylactic mastectomy and immediate reconstruction. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2007, 41, 178–183. [Google Scholar] [CrossRef]
- van Verschuer, V.M.; Mureau, M.A.; Gopie, J.P.; Vos, E.L.; Verhoef, C.; Menke-Pluijmers, M.B.; Koppert, L.B. Patient Satisfaction and Nipple-Areola Sensitivity After Bilateral Prophylactic Mastectomy and Immediate Implant Breast Reconstruction in a High Breast Cancer Risk Population: Nipple-Sparing Mastectomy Versus Skin-Sparing Mastectomy. Ann. Plast. Surg. 2016, 77, 145–152. [Google Scholar] [CrossRef]
- Petit, J.Y.; Veronesi, U.; Orecchia, R.; Rey, P.; Martella, S.; Didier, F.; Viale, G.; Veronesi, P.; Luini, A.; Galimberti, V.; et al. Nipple sparing mastectomy with nipple areola intraoperative radiotherapy: One thousand and one cases of a five years experience at the European institute of oncology of Milan (EIO). Breast Cancer Res. Treat. 2009, 117, 333–338. [Google Scholar] [CrossRef]
- Gahm, J.; Hansson, P.; Brandberg, Y.; Wickman, M. Breast sensibility after bilateral risk-reducing mastectomy and immediate breast reconstruction: A prospective study. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1521–1527. [Google Scholar] [CrossRef]
- Bresser, P.J.; Seynaeve, C.; Van Gool, A.R.; Niermeijer, M.F.; Duivenvoorden, H.J.; van Dooren, S.; van Geel, A.N.; Menke-Pluijmers, M.B.; Klijn, J.G.; Tibben, A. The course of distress in women at increased risk of breast and ovarian cancer due to an (identified) genetic susceptibility who opt for prophylactic mastectomy and/or salpingo-oophorectomy. Eur. J. Cancer 2007, 43, 95–103. [Google Scholar] [CrossRef]
- Heiniger, L.; Butow, P.N.; Coll, J.; Bullen, T.; Wilson, J.; Baylock, B.; Meiser, B.; Price, M.A. Long-term outcomes of risk-reducing surgery in unaffected women at increased familial risk of breast and/or ovarian cancer. Fam. Cancer 2015, 14, 105–115. [Google Scholar] [CrossRef]
- Frost, M.H.; Schaid, D.J.; Sellers, T.A.; Slezak, J.M.; Arnold, P.G.; Woods, J.E.; Petty, P.M.; Johnson, J.L.; Sitta, D.L.; McDonnell, S.K.; et al. Long-term satisfaction and psychological and social function following bilateral prophylactic mastectomy. JAMA 2000, 284, 319–324. [Google Scholar] [CrossRef]
- Dick, J.; Tuchler, A.; Bredart, A.; Vitinius, F.; Wassermann, K.; Rhiem, K.; Schmutzler, R.K. Psychological factors and the uptake of preventative measures in BRCA1/2 pathogenic variant carriers: Results of a prospective cohort study. Hered. Cancer Clin. Pract. 2022, 20, 38. [Google Scholar] [CrossRef]
- van Egdom, L.S.E.; de Kock, M.A.; Apon, I.; Mureau, M.A.M.; Verhoef, C.; Hazelzet, J.A.; Koppert, L.B. Patient-Reported Outcome Measures may optimize shared decision-making for cancer risk management in BRCA mutation carriers. Breast Cancer 2020, 27, 426–434. [Google Scholar] [CrossRef]
- Keller, K.; Meisel, C.; Grubling, N.; Petzold, A.; Wimberger, P.; Kast, K. Patient-Reported Satisfaction after Prophylactic Operations of the Breast. Breast Care 2019, 14, 217–223. [Google Scholar] [CrossRef]
- Glassey, R.; Ives, A.; Saunders, C.; Musiello, T. Decision making, psychological wellbeing and psychosocial outcomes for high risk women who choose to undergo bilateral prophylactic mastectomy—A review of the literature. Breast 2016, 28, 130–135. [Google Scholar] [CrossRef]
- Patenaude, A.F.; Orozco, S.; Li, X.; Kaelin, C.M.; Gadd, M.; Matory, Y.; Mayzel, K.; Roche, C.A.; Smith, B.L.; Farkas, W.; et al. Support needs and acceptability of psychological and peer consultation: Attitudes of 108 women who had undergone or were considering prophylactic mastectomy. Psychooncology 2008, 17, 831–843. [Google Scholar] [CrossRef]
- Payne, D.K.; Biggs, C.; Tran, K.N.; Borgen, P.I.; Massie, M.J. Women’s regrets after bilateral prophylactic mastectomy. Ann. Surg. Oncol. 2000, 7, 150–154. [Google Scholar] [CrossRef]
- Rolnick, S.J.; Altschuler, A.; Nekhlyudov, L.; Elmore, J.G.; Greene, S.M.; Harris, E.L.; Herrinton, L.J.; Barton, M.B.; Geiger, A.M.; Fletcher, S.W. What women wish they knew before prophylactic mastectomy. Cancer Nurs. 2007, 30, 285–291; quiz 292–293. [Google Scholar] [CrossRef]
- Herold, N.; Hellmich, M.; Lichtenheldt, F.; Ataseven, B.; Hillebrand, V.; Wappenschmidt, B.; Schmutzler, R.K.; Rhiem, K. Satisfaction and Quality of Life of Healthy and Unilateral Diseased BRCA1/2 Pathogenic Variant Carriers after Risk-Reducing Mastectomy and Reconstruction Using the BREAST-Q Questionnaire. Genes 2022, 13, 1357. [Google Scholar] [CrossRef]
- Kanana, N.; Ben David, M.A.; Nissan, N.; Yagil, Y.; Shalmon, A.; Halshtok, O.; Gotlieb, M.; Faermann, R.; Klang, E.; Samoocha, D.; et al. Post-mastectomy surveillance of BRCA1/BRCA2 mutation carriers: Outcomes from a specialized clinic for high-risk breast cancer patients. Breast J. 2021, 27, 441–447. [Google Scholar] [CrossRef]
- Weed, C.; Wang, T.; Fat, S.C.; Chung, A.; Boyle, M.K.; Giuliano, A.; Amersi, F. Surveillance Strategies Following Prophylactic Nipple-Sparing Mastectomy in BRCA Mutation Carriers. Ann. Surg. Oncol. 2023, 30, 5335–5336. [Google Scholar] [CrossRef]
- Aschen, S.Z.; Paik, K.C.; Swistel, A.S.; Talmor, M. Pregnancy-Associated Breast Changes after Nipple-Sparing Mastectomy. Plast. Reconstr. Surg. 2023, 152, 492–500. [Google Scholar] [CrossRef]
- Tang, R.; Kelly, B.N.; Smith, B.L.; Lanahan, C.R.; Brown, C.L.; Gadd, M.A.; Hughes, K.S.; Oseni, T.O.; McGugin, C.; Specht, M.C.; et al. Nipple Discharge After Nipple-Sparing Mastectomy With and Without Associated Pregnancy. Clin. Breast Cancer 2019, 19, e534–e539. [Google Scholar] [CrossRef]
- Djohan, R.; Knackstedt, R.; Scomacao, I.; Cakmakoglu, C.; Downs, E.K.; Grobmyer, S.R. A novel approach to sensory re-innervation to the nipple areolar complex after mastectomy with implant-based reconstruction: Anatomic and technical considerations. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 983–1007. [Google Scholar] [CrossRef] [PubMed]
- Blondeel, P.N.; Demuynck, M.; Mete, D.; Monstrey, S.J.; Van Landuyt, K.; Matton, G.; Vanderstraeten, G.G. Sensory nerve repair in perforator flaps for autologous breast reconstruction: Sensational or senseless? Br. J. Plast. Surg. 1999, 52, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Temple, C.L.; Tse, R.; Bettger-Hahn, M.; MacDermid, J.; Gan, B.S.; Ross, D.C. Sensibility following innervated free TRAM flap for breast reconstruction. Plast. Reconstr. Surg. 2006, 117, 2119–2127; discussion 2128–2130. [Google Scholar] [CrossRef]
- Temple, C.L.F.; Ross, D.C.; Kim, S.; Tse, R.; Bettger-Hahn, M.; Gan, B.S.; MacDermid, J. Sensibility following innervated free TRAM flap for breast reconstruction: Part II. Innervation improves patient-rated quality of life. Plast. Reconstr. Surg. 2009, 124, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Djohan, R.; Scomacao, I.; Duraes, E.F.R.; Knackstedt, R.; Mangan, R.; Schwarz, G. Sensory Restoration in Abdominally Based Free Flaps for Breast Reconstruction Using Nerve Allograft. Plast. Reconstr. Surg. 2023, 151, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Momeni, A.; Meyer, S.; Shefren, K.; Januszyk, M. Flap Neurotization in Breast Reconstruction with Nerve Allografts: 1-year Clinical Outcomes. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3328. [Google Scholar] [CrossRef] [PubMed]
- Djohan, R.; Scomacao, I.; Knackstedt, R.; Cakmakoglu, C.; Grobmyer, S.R. Neurotization of the Nipple-Areola Complex during Implant-Based Reconstruction: Evaluation of Early Sensation Recovery. Plast. Reconstr. Surg. 2020, 146, 250–254. [Google Scholar] [CrossRef]
- Peled, A.W.; Peled, Z.M. Nerve Preservation and Allografting for Sensory Innervation Following Immediate Implant Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2332. [Google Scholar] [CrossRef] [PubMed]
- Abbas, F.; Klomparens, K.; Simman, R. Functional and Psychosocial Outcomes following Innervated Breast Reconstruction: A Systematic Review. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4559. [Google Scholar] [CrossRef] [PubMed]
- Shiah, E.; Laikhter, E.; Comer, C.D.; Manstein, S.M.; Bustos, V.P.; Bain, P.A.; Lee, B.T.; Lin, S.J. Neurotization in Innervated Breast Reconstruction: A Systematic Review of Techniques and Outcomes. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 2890–2913. [Google Scholar] [CrossRef] [PubMed]
- Gfrerer, L.; Sager, J.E.; Ford, O.A.; Carty, M.J.; Verdial, F.C.; Gadd, M.A.; Specht, M.C.; Winograd, J.M.; Valerio, I.L. Targeted Nipple Areola Complex Reinnervation: Technical Considerations and Surgical Efficiency in Implant-based Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4420. [Google Scholar] [CrossRef]
- Toesca, A.; Peradze, N.; Manconi, A.; Galimberti, V.; Intra, M.; Colleoni, M.; Bonanni, B.; Curigliano, G.; Rietjens, M.; Viale, G.; et al. Robotic nipple-sparing mastectomy for the treatment of breast cancer: Feasibility and safety study. Breast 2017, 31, 51–56. [Google Scholar] [CrossRef]
- Huang, J.J.; Chuang, E.Y.; Cheong, D.C.; Kim, B.S.; Chang, F.C.; Kuo, W.L. Robotic-assisted nipple-sparing mastectomy followed by immediate microsurgical free flap reconstruction: Feasibility and aesthetic results—Case series. Int. J. Surg. 2021, 95, 106143. [Google Scholar] [CrossRef]
- Ryu, J.M.; Kim, J.Y.; Choi, H.J.; Ko, B.; Kim, J.; Cho, J.; Lee, M.H.; Choi, J.E.; Kim, J.H.; Lee, J.; et al. Robot-assisted Nipple-sparing Mastectomy With Immediate Breast Reconstruction: An initial Experience of the Korea Robot-endoscopy Minimal Access Breast Surgery Study Group (KoREa-BSG). Ann. Surg. 2022, 275, 985–991. [Google Scholar] [CrossRef]
- Toesca, A.; Sangalli, C.; Maisonneuve, P.; Massari, G.; Girardi, A.; Baker, J.L.; Lissidini, G.; Invento, A.; Farante, G.; Corso, G.; et al. A Randomized Trial of Robotic Mastectomy Versus Open Surgery in Women With Breast Cancer or BrCA Mutation. Ann. Surg. 2022, 276, 11–19. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Country | No. | Overall % BRRM | BRCA1 (% BRRM) | BRCA2 (% BRRM) |
|---|---|---|---|---|---|
| Metcalfe et al. (2019) [46] | USA | 774 | 49.9% | - | - |
| Heemskirk et al. (2019) [15] | Netherlands | 2857 | 39.5% | 42% | 35% |
| Metcalfe et al. (2019) [46] | Canada | 1005 | 38.0% | - | - |
| Marcinkute et al. (2022) [45] | UK (Manchester) | 887 | 34.5% | 37% | 32% |
| Long et al. (2018) [50] | UK (Wales) | 280 | 34.0% | - | - |
| Skytte et al. (2010) [50] | Denmark | 206 | 30.0% | 33% | 25% |
| Petelin et al. (2019) [51] | Australia | 493 | 27.6% | 31% | 25% |
| Singer et al. (2014) [51] | Austria | 246 | 21.4% | - | - |
| Galmor et al. (2021) [43] | Israel | 427 | 9.6% | 12% | 7% |
| Jung et al. (2020) [49] | South Korea | 514 | 1.2% | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, S.M.; Apostolova, C.; Eisenberg, E.; Foulkes, W.D. Counselling Framework for Germline BRCA1/2 and PALB2 Carriers Considering Risk-Reducing Mastectomy. Curr. Oncol. 2024, 31, 350-365. https://doi.org/10.3390/curroncol31010023
Wong SM, Apostolova C, Eisenberg E, Foulkes WD. Counselling Framework for Germline BRCA1/2 and PALB2 Carriers Considering Risk-Reducing Mastectomy. Current Oncology. 2024; 31(1):350-365. https://doi.org/10.3390/curroncol31010023
Chicago/Turabian StyleWong, Stephanie M., Carla Apostolova, Elisheva Eisenberg, and William D. Foulkes. 2024. "Counselling Framework for Germline BRCA1/2 and PALB2 Carriers Considering Risk-Reducing Mastectomy" Current Oncology 31, no. 1: 350-365. https://doi.org/10.3390/curroncol31010023
APA StyleWong, S. M., Apostolova, C., Eisenberg, E., & Foulkes, W. D. (2024). Counselling Framework for Germline BRCA1/2 and PALB2 Carriers Considering Risk-Reducing Mastectomy. Current Oncology, 31(1), 350-365. https://doi.org/10.3390/curroncol31010023