Gynecologic Cancer Risk and Genetics: Informing an Ideal Model of Gynecologic Cancer Prevention

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
1.1. Current System of Hereditary Cancer Prevention
1.2. Combined Epidemiological Risk Factors, Pathogenic Variants, and Polygenic Risk Scores
1.3. Evidence from Population-Based Genetic Testing Trials
1.4. Problem
2. Methodology
3. Results of Panel Discussion
3.1. Preparing the Path from Patient-Driven Genetic Testing to Population-Based Genetic Testing. Why Do We Need to Wait for a Cancer to Happen to Identify People in Whom We Can Prevent Cancer?
3.1.1. Paradigm Shift: Family History Based to Population-Based Testing
3.1.2. Clinical Utility and Clinical Risk Management
3.1.3. Psychological Impacts on Patients and Public Acceptability of Population-Based Testing
3.2. Establishing the Social and Economic Context in Which Increased Genetic Testing Will Be Feasible and Acceptable. How Can the Canadian Model of Gynecologic Cancer Prevention Better Utilise Genetic and Genomics at a Population Level?
3.2.1. Developing the Infrastructure to Support Increased Genetic Testing
3.2.2. Ensuring Equitable Access to Genetic Testing
3.2.3. Economic Feasibility and Sustainability
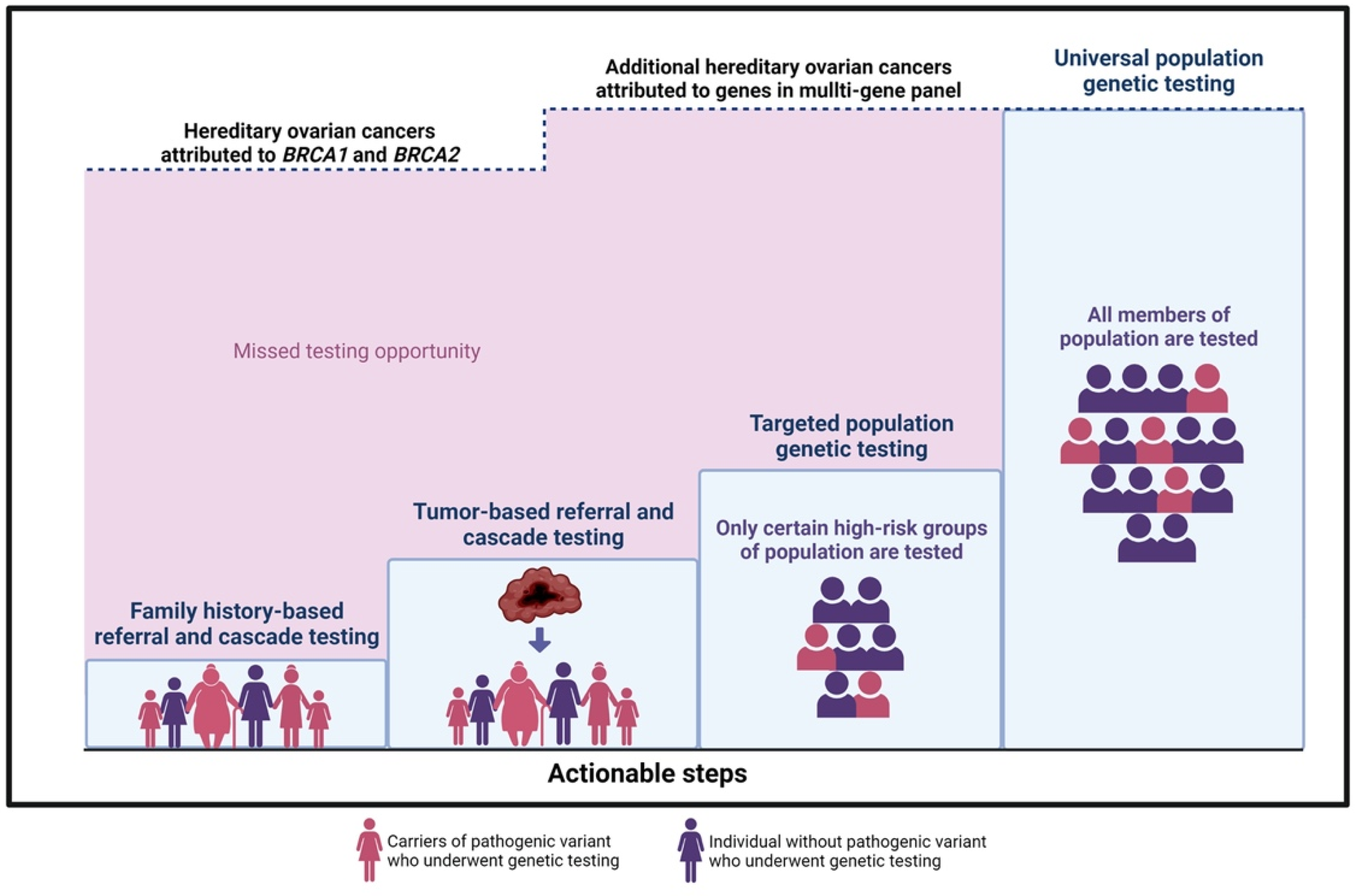
3.3. Actionable Steps towards Adopting Population-Based Genetic Cancer Testing
3.4. Recommended First Steps
- (1)
- Family history-based referral and cascade testing: Strategies to increase detection of high-risk individuals would improve the uptake of testing in relatives of HCS carriers. i.e., a sister of a confirmed BRCA carrier is at 50% risk of having the familial mutation. In the current model, an index patient is responsible for communication with family members. This strategy has low uptake, with fewer than 50% of high-risk relatives accessing care. Direct relative communication via health professionals increases the uptake of cascade testing [65]. Studies in a UK model evaluating the effectiveness of registries in the facilitation of family contact confirm that registries provide long-term follow-up and proactive genetic counselling to relatives at risk, potentially an effective initiative in the Canadian context. The shift towards a formal provider-initiated, registry-based cascade testing is optimal, but important considerations must balance the concept of “duty to warn” with individual confidentiality and privacy [66].
- (2)
- Tumor-based referral and cascade testing: A tumor-first approach can be employed where samples from surgical specimens are sequenced, triggering a stepwise process whereby tumor genomic results are reported routinely and then patients with possible HCS are counselled regarding germline testing. This strategy would be delivered universally, without barriers, and would allow more equitable care across race or socioeconomic status. Patients may directly benefit from information about potential targeted therapies [67,68]. This approach could also offer the option of improving family risk assessment via tumor sequencing from deceased patients for the benefit of relatives and could be delivered in a way to respect individual preferences of patients about germline testing.
- (3)
- Targeted population-based genetic testing: A strategic step toward increased detection of HCS carriers in a population would expand testing to specific groups or population subsets with higher mutation prevalence; this approach is now standard care for all ovarian cancer patients and has been successfully implemented across Canada. By removing the requirement of a family cancer history for testing eligibility, the process of offering testing to all patients in a category, i.e., breast cancer [69] or pancreatic cancer [70], irrespective of family history could meaningfully reduce barriers to care [71]. Testing all women with breast cancer for HCS genes has been shown to be cost-effective for UK and USA health systems [72]. Testing all individuals with Ashkenazi Jewish descent will identify BRCA mutations in 2–3% of unselected cases and has been proven (1) acceptable to patients, (2) clinically effective, and (3) cost saving for health systems [42,73,74]. A logical first step in any planned expansion of prevention would begin with publicly funded testing for Ashkenazi Jewish Canadians [75,76] and broader eligibility testing criteria for patients with specific cancers. Populations experiencing reduced access, care, and family history assessment, i.e., Indigenous communities, would be prioritized. These higher risk groups could be approached first for population-based testing initiatives [77,78,79,80,81].
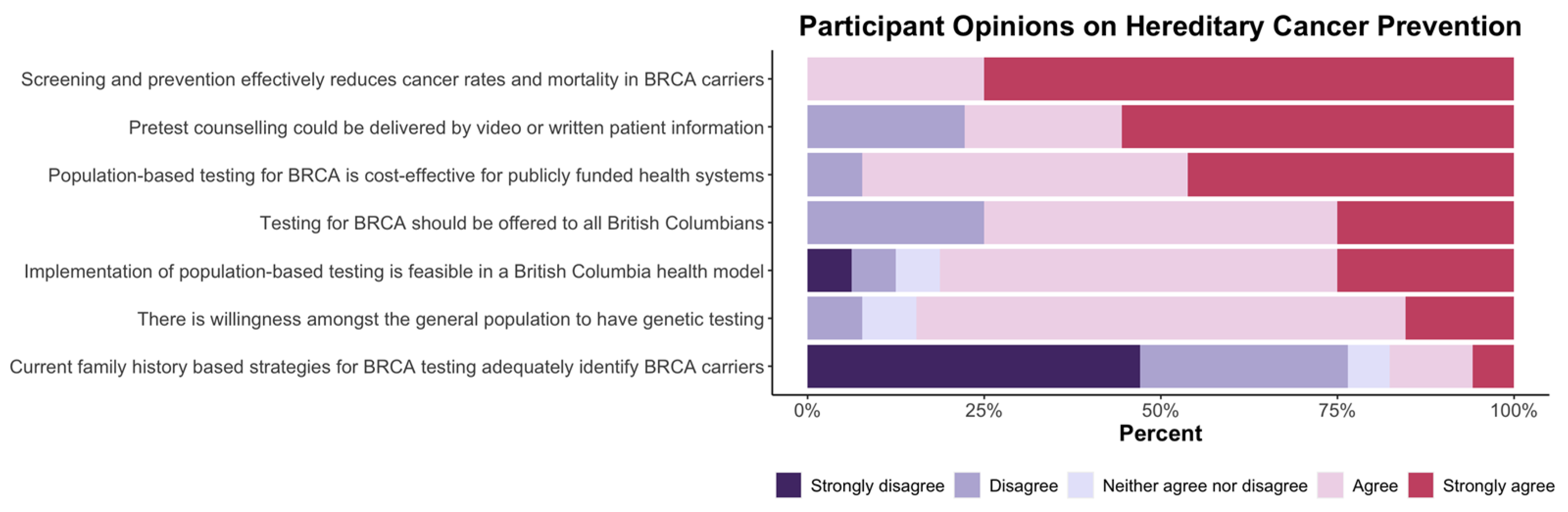
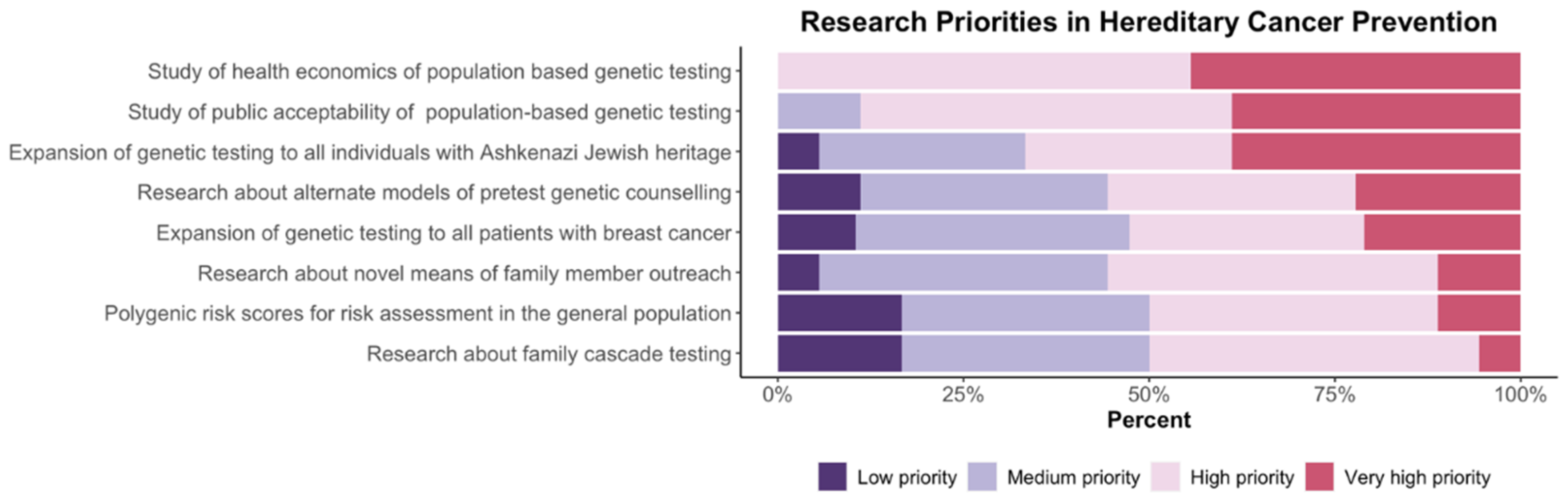
3.5. Cancer Prevention Summit Participant Survey Results
4. Discussion
- (1)
- Implementation of new technologies and prevention strategies must be developed in a way that is equitable to all individuals in a population, regardless of ethnicity, socio-economic status, or geography. Every effort to remove elements of institutional racism in the delivery of new systems is essential. In communities where family-history-based requirements for testing are a barrier, those populations, specifically Indigenous peoples, should be provided first offer to engage in the development of broad population-based testing initiatives.
- (2)
- Population-based testing for genetic risk should become the standard of care for effective cancer prevention and could be cost-effective for the long-term sustainability of health systems. Before population-based testing is implemented, incremental improvements in the identification of high-risk individuals will deliver more effective cancer prevention. This will include testing for all individuals with Ashkenazi Jewish heritage, relatives of women with ovarian cancer, and expanded access to testing for patients with breast, prostate, and pancreatic cancer.
- (3)
- Hereditary cancer registries providing high-risk patients with supportive navigation of preventative screening/surgery and access to research will be a key element in effective prevention programs.
- (4)
- Successful population-based testing strategies will require infrastructure, well-developed public education models and must be guided by public preferences.
- (5)
- There is need for improved patient access and more efficient delivery of germline testing within current hereditary cancer systems. This will require broader use of group pre-test counselling, testing embedded in cancer clinics, and use of digital patient-facing education and counselling tools.
- (6)
- Cascade testing of family members is critical for success of prevention programs. Strategies to improve rates of testing in high-risk family members will include facilitated family communication, use of digital education/outreach tools, and broader public education.
- (7)
- Polygenic risk scores and epidemiological risk assessment models have value in the delivery of personalized preventative interventions. These models may be implemented in parallel with germline testing at both a population level and in the context of proven BRCA mutations. This will become feasible as better validation data emerge and implementation studies follow.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Toss, A.; Tomasello, C.; Razzaboni, E.; Contu, G.; Grandi, G.; Cagnacci, A.; Schilder, R.J.; Cortesi, L. Hereditary Ovarian Cancer: Not Only BRCA 1 and 2 Genes. BioMed Res. Int. 2015, 2015, 341723. [Google Scholar] [CrossRef]
- Chen, X.; Jiang, J.; Shen, H.; Hu, Z. Genetic Susceptibility of Cervical Cancer. J. Biomed. Res. 2011, 25, 155. [Google Scholar] [CrossRef]
- Trietsch, M.D.; Nooij, L.S.; Gaarenstroom, K.N.; Van Poelgeest, M.I.E. Genetic and Epigenetic Changes in Vulvar Squamous Cell Carcinoma and Its Precursor Lesions: A Review of the Current Literature. Gynecol. Oncol. 2015, 136, 143–157. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.-A.; Mooij, T.M.; Roos-Blom, M.-J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef]
- Li, J.; Wen, W.X.; Eklund, M.; Kvist, A.; Eriksson, M.; Christensen, H.N.; Torstensson, A.; Bajalica-Lagercrantz, S.; Dunning, A.M.; Decker, B.; et al. Prevalence of BRCA1 and BRCA2 Pathogenic Variants in a Large, Unselected Breast Cancer Cohort. Int. J. Cancer 2019, 144, 1195–1204. [Google Scholar] [CrossRef]
- Wen, W.X.; Allen, J.; Lai, K.N.; Mariapun, S.; Hasan, S.N.; Ng, P.S.; Lee, D.S.C.; Lee, S.Y.; Yoon, S.Y.; Lim, J.; et al. Inherited Mutations in BRCA1 and BRCA2 in an Unselected Multiethnic Cohort of Asian Patients with Breast Cancer and Healthy Controls from Malaysia. J. Med. Genet. 2018, 55, 97–103. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Poll, A.; Royer, R.; Llacuachaqui, M.; Tulman, A.; Sun, P.; Narod, S.A. Screening for Founder Mutations in BRCA1 and BRCA2 in Unselected Jewish Women. J. Clin. Oncol. 2010, 28, 387–391. [Google Scholar] [CrossRef]
- Grzymski, J.J.; Elhanan, G.; Morales Rosado, J.A.; Smith, E.; Schlauch, K.A.; Read, R.; Rowan, C.; Slotnick, N.; Dabe, S.; Metcalf, W.J.; et al. Population Genetic Screening Efficiently Identifies Carriers of Autosomal Dominant Diseases. Nat. Med. 2020, 26, 1235–1239. [Google Scholar] [CrossRef]
- Rowley, S.M.; Mascarenhas, L.; Devereux, L.; Li, N.; Amarasinghe, K.C.; Zethoven, M.; Lee, J.E.A.; Lewis, A.; Morgan, J.A.; Limb, S.; et al. Population-Based Genetic Testing of Asymptomatic Women for Breast and Ovarian Cancer Susceptibility. Genet. Med. 2019, 21, 913–922. [Google Scholar] [CrossRef]
- Manchanda, R.; Blyuss, O.; Gaba, F.; Gordeev, V.S.; Jacobs, C.; Burnell, M.; Gan, C.; Taylor, R.; Turnbull, C.; Legood, R.; et al. Current Detection Rates and Time-to-Detection of All Identifiable BRCA Carriers in the Greater London Population. J. Med. Genet. 2018, 55, 538–545. [Google Scholar] [CrossRef]
- Richardson, M.; Min, H.J.; Hong, Q.; Compton, K.; Mung, S.W.; Lohn, Z.; Nuk, J.; McCullum, M.; Portigal-Todd, C.; Karsan, A.; et al. Oncology Clinic-Based Hereditary Cancer Genetic Testing in a Population-Based Health Care System. Cancers 2020, 12, 338. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, K.D.; Obeid, E.; Daly, M.B.; Hall, M.J. Cascade Genetic Testing for Hereditary Cancer Risk: An Underutilized Tool for Cancer Prevention. JCO Precis. Oncol. 2021, 5, 1387–1396. [Google Scholar] [CrossRef] [PubMed]
- Hagoel, L.; Dishon, S.; Almog, R.; Bisland-Becktell, S.; Rennert, G. Proband Family Uptake of Familial-Genetic Counselling. Psychooncology 2000, 9, 522–527. [Google Scholar] [CrossRef]
- Julian-Reynier, C.; Sobol, H.; Sevilla, C.; Nogues, C.; Bourret, P. French Cancer Genetic Network Uptake of Hereditary Breast/Ovarian Cancer Genetic Testing in a French National Sample of BRCA1 Families. Psychooncology 2000, 9, 504–510. [Google Scholar] [CrossRef]
- Holloway, S.M.; Bernhard, B.; Campbell, H.; Lam, W.W.K. Uptake of Testing for BRCA1/2 Mutations in South East Scotland. Eur. J. Hum. Genet. 2008, 16, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Finlay, E.; Stopfer, J.E.; Burlingame, E.; Evans, K.G.; Nathanson, K.L.; Weber, B.L.; Armstrong, K.; Rebbeck, T.R.; Domchek, S.M. Factors Determining Dissemination of Results and Uptake of Genetic Testing in Families with Known BRCA1/2 Mutations. Genet. Test. 2008, 12, 81–91. [Google Scholar] [CrossRef]
- Blandy, C.; Chabal, F.; Stoppa-Lyonnet, D.; Julian-Reynier, C. Testing Participation in BRCA1/2-Positive Families: Initiator Role of Index Cases. Genet. Test. 2004, 7, 225–233. [Google Scholar] [CrossRef]
- Sharaf, R.N.; Myer, P.; Stave, C.D.; Diamond, L.C.; Ladabaum, U. Uptake of Genetic Testing by Relatives of Lynch Syndrome Probands: A Systematic Review. Clin. Gastroenterol. Hepatol. 2013, 11, 1093–1100. [Google Scholar] [CrossRef]
- Braley, E.F.; Bedard, A.C.; Nuk, J.; Hong, Q.; Bedard, J.E.J.; Sun, S.; Schrader, K.A. Patient Ethnicity and Cascade Genetic Testing: A Descriptive Study of a Publicly Funded Hereditary Cancer Program. Fam. Cancer 2022, 21, 369–374. [Google Scholar] [CrossRef]
- Sutton, S.; Saidi, G.; Bickler, G.; Hunter, J. Does Routine Screening for Breast Cancer Raise Anxiety? Results from a Three Wave Prospective Study in England. J. Epidemiol. Community Health 1995, 49, 413–418. [Google Scholar] [CrossRef]
- Puliti, D.; Miccinesi, G.; Paci, E. Overdiagnosis in Breast Cancer: Design and Methods of Estimation in Observational Studies. Prev. Med. 2011, 53, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Duffy, S.W.; Chowdhury, S.; Dent, T.; Burton, H.; Neal, D.E.; Easton, D.F.; Eeles, R.; Pharoah, P. Polygenic Susceptibility to Prostate and Breast Cancer: Implications for Personalised Screening. Br. J. Cancer 2011, 104, 1656–1663. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Blyuss, O.; Liu, X.; Goyal, S.; Lahoti, N.; Chandrasekaran, D.; Kurzer, M.; Kalsi, J.; Sanderson, S.; Lanceley, A.; et al. Population Study of Ovarian Cancer Risk Prediction for Targeted Screening and Prevention. Cancers 2020, 12, 1241. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.; Waller, J.; Manchanda, R.; Jacobs, I.; Sanderson, S. Women’s Intentions to Engage in Risk-Reducing Behaviours after Receiving Personal Ovarian Cancer Risk Information: An Experimental Survey Study. Cancers 2020, 12, 3543. [Google Scholar] [CrossRef] [PubMed]
- Mbuya-Bienge, C.; Pashayan, N.; Brooks, J.D.; Dorval, M.; Chiquette, J.; Eloy, L.; Turgeon, A.; Lambert-Côté, L.; Paquette, J.S.; Lévesque, E.; et al. Women’s Views on Multifactorial Breast Cancer Risk Assessment and Risk-Stratified Screening: A Population-Based Survey from Four Provinces in Canada. J. Pers. Med. 2021, 11, 95. [Google Scholar] [CrossRef]
- Manchanda, R.; Legood, R.; Antoniou, A.C.; Gordeev, V.S.; Menon, U. Specifying the Ovarian Cancer Risk Threshold of “premenopausal Risk-Reducing Salpingo-Oophorectomy” for Ovarian Cancer Prevention: A Cost-Effectiveness Analysis. J. Med. Genet. 2016, 53, 591–599. [Google Scholar] [CrossRef]
- Manchanda, R.; Gaba, F.; Talaulikar, V.; Pundir, J.; Gessler, S.; Davies, M.; Menon, U. Risk-Reducing Salpingo-Oophorectomy and the Use of Hormone Replacement Therapy Below the Age of Natural Menopause: Scientific Impact Paper No. 66 October 2021: Scientific Impact Paper No. 66. BJOG 2022, 129, e16–e34. [Google Scholar] [CrossRef]
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Lee, A.; Yang, X.; Tyrer, J.; Gentry-Maharaj, A.; Ryan, A.; Mavaddat, N.; Cunningham, A.P.; Carver, T.; Archer, S.; Leslie, G.; et al. Comprehensive Epithelial Tubo-Ovarian Cancer Risk Prediction Model Incorporating Genetic and Epidemiological Risk Factors. J. Med. Genet. 2021, 59, jmedgenet-2021-107904. [Google Scholar] [CrossRef]
- Usset, J.L.; Raghavan, R.; Tyrer, J.P.; McGuire, V.; Sieh, W.; Webb, P.; Chang-Claude, J.; Rudolph, A.; Anton-Culver, H.; Berchuck, A.; et al. Assessment of Multifactor Gene?Environment Interactions and Ovarian Cancer Risk: Candidate Genes, Obesity, and Hormone-Related Risk Factors. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 780–790. [Google Scholar] [CrossRef]
- Hanley, G.E.; Pearce, C.L.; Talhouk, A.; Kwon, J.S.; Finlayson, S.J.; Mcalpine, J.N.; Huntsman, D.G.; Miller, D. Outcomes from Opportunistic Salpingectomy for Ovarian Cancer Prevention. JAMA Netw. Open 2022, 5, e2147343. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Goyal, S.; Marks, D.; Chandrasekaran, D.; Evans, O.; Robbani, S.; Tyson, C.; Legood, R.; Saridogan, E.; McCluggage, W.G.; et al. Surgical Decision Making in Premenopausal BRCA Carriers Considering Risk-Reducing Early Salpingectomy or Salpingo-Oophorectomy: A Qualitative Study. J. Med. Genet. 2022, 59, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Robbani, S.; Singh, N.; McCluggage, W.G.; Wilkinson, N.; Ganesan, R.; Bryson, G.; Rowlands, G.; Tyson, C.; Arora, R.; et al. Preventing Ovarian Cancer through Early Excision of Tubes and Late Ovarian Removal (PROTECTOR): Protocol for a Prospective Non-Randomised Multi-Center Trial. Int. J. Gynecol. Cancer 2021, 31, 286–291. [Google Scholar] [CrossRef]
- Chung, C.C.; Magalhaes, W.C.S.; Gonzalez-Bosquet, J.; Chanock, S.J. Genome-Wide Association Studies in Cancer—Current and Future Directions. Carcinogenesis 2010, 31, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Easton, D.F.; Pharoah, P.D.P.; Antoniou, A.C.; Tischkowitz, M.; Tavtigian, S.V.; Nathanson, K.L.; Devilee, P.; Meindl, A.; Couch, F.J.; Southey, M.; et al. Gene-Panel Sequencing and the Prediction of Breast-Cancer Risk. N. Engl. J. Med. 2015, 372, 2243–2257. [Google Scholar] [CrossRef]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21. [Google Scholar] [CrossRef] [PubMed]
- Dareng, E.O.; Tyrer, J.P.; Barnes, D.R.; Jones, M.R.; Yang, X.; Aben, K.K.H.; Adank, M.A.; Agata, S.; Andrulis, I.L.; Anton-Culver, H.; et al. Polygenic Risk Modeling for Prediction of Epithelial Ovarian Cancer Risk. Eur. J. Hum. Genet. 2022, 30, 349–362. [Google Scholar] [CrossRef]
- Rudolph, A.; Milne, R.L.; Truong, T.; Knight, J.A.; Seibold, P.; Flesch-Janys, D.; Behrens, S.; Eilber, U.; Bolla, M.K.; Wang, Q.; et al. Investigation of Gene-Environment Interactions between 47 Newly Identified Breast Cancer Susceptibility Loci and Environmental Risk Factors. Int. J. Cancer 2015, 136, E685–E696. [Google Scholar] [CrossRef]
- Dorling, L.; Carvalho, S.; Allen, J.; González-Neira, A.; Luccarini, C.; Wahlström, C.; Pooley, K.A.; Parsons, M.T.; Fortuno, C.; Wang, Q.; et al. Breast Cancer Risk Genes—Association Analysis in More than 113,000 Women. N. Engl. J. Med. 2021, 384, 428–439. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Poll, A.; Royer, R.; Nanda, S.; Llacuachaqui, M.; Sun, P.; Narod, S.A. A Comparison of the Detection of BRCA Mutation Carriers through the Provision of Jewish Population-Based Genetic Testing Compared with Clinic-Based Genetic Testing. Br. J. Cancer 2013, 109, 777–779. [Google Scholar] [CrossRef][Green Version]
- Manchanda, R.; Loggenberg, K.; Sanderson, S.; Burnell, M.; Wardle, J.; Gessler, S.; Side, L.; Balogun, N.; Desai, R.; Kumar, A.; et al. Population Testing for Cancer Predisposing BRCA1/BRCA2 Mutations in the Ashkenazi-Jewish Community: A Randomized Controlled Trial. JNCI J. Natl. Cancer Inst. 2015, 107, dju379. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, R.; Burnell, M.; Gaba, F.; Desai, R.; Wardle, J.; Gessler, S.; Side, L.; Sanderson, S.; Loggenberg, K.; Brady, A.F.; et al. Randomised Trial of Population-Based BRCA Testing in Ashkenazi Jews: Long-Term Outcomes. BJOG 2020, 127, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Narod, S.A.; Gojska, N.; Sun, P.; Tryon, A.; Kotsopoulos, J.; Metcalfe, K.; Akbari, M.R. The Screen Project: Guided Direct-To-Consumer Genetic Testing for Breast Cancer Susceptibility in Canada. Cancers 2021, 13, 1894. [Google Scholar] [CrossRef] [PubMed]
- Gabai-Kapara, E.; Lahad, A.; Kaufman, B.; Friedman, E.; Segev, S.; Renbaum, P.; Beeri, R.; Gal, M.; Grinshpun-Cohen, J.; Djemal, K.; et al. Population-Based Screening for Breast and Ovarian Cancer Risk Due to BRCA1 and BRCA2. Proc. Natl. Acad. Sci. USA 2014, 111, 14205–14210. [Google Scholar] [CrossRef]
- Manchanda, R.; Sun, L.; Patel, S.; Evans, O.; Wilschut, J.; Lopes, A.C.D.F.; Gaba, F.; Brentnall, A.; Duffy, S.; Cui, B.; et al. Economic Evaluation of Population-Based BRCA1/BRCA2 Mutation Testing across Multiple Countries and Health Systems. Cancers 2020, 12, 1929. [Google Scholar] [CrossRef]
- Chandrasekaran, D.; Sobocan, M.; Blyuss, O.; Miller, R.E.; Evans, O.; Crusz, S.M.; Mills-Baldock, T.; Sun, L.; Hammond, R.F.L.; Gaba, F.; et al. Implementation of Multigene Germline and Parallel Somatic Genetic Testing in Epithelial Ovarian Cancer: SIGNPOST Study. Cancers 2021, 13, 4344. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Knoppers, B.M.; Turnbull, C. Population Genetic Testing for Cancer Susceptibility: Founder Mutations to Genomes. Nat. Rev. Clin. Oncol. 2016, 13, 41–54. [Google Scholar] [CrossRef]
- World Health Organization. WHO Handbook for Standardized Cancer Registries; World Health Organization: Geneva, Switzerland, 1976. [Google Scholar]
- Rothenmund, H.; Singh, H.; Candas, B.; Chodirker, B.N.; Serfas, K.; Aronson, M.; Holter, S.; Volenik, A.; Green, J.; Dicks, E.; et al. Hereditary Colorectal Cancer Registries in Canada: Report from the Colorectal Cancer Association of Canada Consensus Meeting; Montreal, Quebec; October 28, 2011. Curr. Oncol. 2013, 20, 273. [Google Scholar] [CrossRef]
- Wright, C.; Kerzin-Storrar, L.; Williamson, P.R.; Fryer, A.; Njindou, A.; Quarrell, O.; Donnai, D.; Craufurd, D. Comparison of Genetic Services with and without Genetic Registers: Knowledge, Adjustment, and Attitudes about Genetic Counselling among Probands Referred to Three Genetic Clinics. J. Med. Genet. 2002, 39, e84. [Google Scholar] [CrossRef]
- Ueda, M.; Tsubamoto, H.; Kashima-Morii, M.; Torii, Y.; Kamihigashi, M.; Wakimoto, Y.; Nakagomi, N.; Hashimoto-Tamaoki, T.; Sawai, H.; Shibahara, H. Challenges in Managing Patients with Hereditary Cancer at Gynecological Services. Obstet. Gynecol. Int. 2019, 2019, 4365754. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.; Langlois, S.; Lynd, L.D.; Austin, J.C.; Elliott, A.M.; Dragojlovic, N.; Knoppers, B.; Dey, A.; Adam, S.; Bansback, N.; et al. Out-of-Pocket and Private Pay in Clinical Genetic Testing: A Scoping Review. Clin. Genet. 2021, 100, 504–521. [Google Scholar] [CrossRef] [PubMed]
- Hynes, J.; MacMillan, A.; Fernandez, S.; Jacob, K.; Carter, S.; Predham, S.; Etchegary, H.; Dawson, L. Group plus “Mini” Individual Pre-Test Genetic Counselling Sessions for Hereditary Cancer Shorten Provider Time and Improve Patient Satisfaction. Hered. Cancer Clin. Pract. 2020, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.C.; Hamilton, J.G.; Conley, C.C.; Peshkin, B.N.; Sacca, R.; McDonnell, G.A.; Isaacs, C.; Robson, M.E.; Tercyak, K.P. Improving Our Model of Cascade Testing for Hereditary Cancer Risk by Leveraging Patient Peer Support: A Concept Report. Hered. Cancer Clin. Pract. 2021, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Lohn, Z.; Fok, A.; Richardson, M.; Derocher, H.; Mung, S.W.; Nuk, J.; Yuson, J.; Jevon, M.; A. Schrader, K.; Sun, S. Large-Scale Group Genetic Counseling: Evaluation of a Novel Service Delivery Model in a Canadian Hereditary Cancer Clinic. J. Genet. Couns. 2022, 31, 459–469. [Google Scholar] [CrossRef]
- Calzone, K.A.; Prindiville, S.A.; Jourkiv, O.; Jenkins, J.; DeCarvalho, M.; Wallerstedt, D.B.; Liewehr, D.J.; Steinberg, S.M.; Soballe, P.W.; Lipkowitz, S.; et al. Randomized Comparison of Group versus Individual Genetic Education and Counseling for Familial Breast and/or Ovarian Cancer. J. Clin. Oncol. 2005, 23, 3455–3464. [Google Scholar] [CrossRef]
- Adeyemo, A.; Balaconis, M.K.; Darnes, D.R.; Fatumo, S.; Granados Moreno, P.; Hodonsky, C.J.; Inouye, M.; Kanai, M.; Kato, K.; Knoppers, B.M.; et al. Responsible Use of Polygenic Risk Scores in the Clinic: Potential Benefits, Risks and Gaps. Nat. Med. 2021, 27, 1876–1884. [Google Scholar] [CrossRef]
- Knoppers, B.M.; Bernier, A.; Moreno, P.G.; Pashayan, N. Of Screening, Stratification, and Scores. J. Pers. Med. 2021, 11, 736. [Google Scholar] [CrossRef]
- Silent Genomes Project | BC Children’s Hospital Research Institute. Available online: https://www.bcchr.ca/silent-genomes-project (accessed on 20 December 2021).
- Centers for Disease Control and Prevention Health and Economic Costs of Chronic Diseases. Available online: https://www.cdc.gov/chronicdisease/about/costs/index.htm (accessed on 11 January 2022).
- Harter, P.; Hauke, J.; Heitz, F.; Reuss, A.; Kommoss, S.; Marmé, F.; Heimbach, A.; Prieske, K.; Richters, L.; Burges, A.; et al. Prevalence of Deleterious Germline Variants in Risk Genes including BRCA1/2 in Consecutive Ovarian Cancer Patients (AGO-TR-1). PLoS ONE 2017, 12, e0186043. [Google Scholar] [CrossRef]
- Buys, S.S.; Sandbach, J.F.; Gammon, A.; Patel, G.; Kidd, J.; Brown, K.L.; Sharma, L.; Saam, J.; Lancaster, J.; Daly, M.B. A Study of over 35,000 Women with Breast Cancer Tested with a 25-Gene Panel of Hereditary Cancer Genes. Cancer 2017, 123, 1721–1730. [Google Scholar] [CrossRef]
- Manchanda, R.; Patel, S.; Gordeev, V.S.; Antoniou, A.C.; Smith, S.; Lee, A.; Hopper, J.L.; MacInnis, R.J.; Turnbull, C.; Ramus, S.J.; et al. Cost-Effectiveness of Population-Based BRCA1, BRCA2, RAD51C, RAD51D, BRIP1, PALB2 Mutation Testing in Unselected General Population Women. J. Natl. Cancer Inst. 2018, 110, 714–725. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Dotson, W.D.; DeVore, C.S.; Bednar, E.M.; Bowen, D.J.; Ganiats, T.G.; Green, R.F.; Hurst, G.M.; Philp, A.R.; Ricker, C.N.; et al. Delivery of Cascade Screening for Hereditary Conditions: A Scoping Review of the Literature. Health Aff. 2018, 37, 801–808. [Google Scholar] [CrossRef]
- Wang, Y.; Golesworthy, B.; Cuggia, A.; Domecq, C.; Chaudhury, P.; Barkun, J.; Metrakos, P.; Asselah, J.; Bouganim, N.; Gao, Z.-H.; et al. Oncology Clinic-Based Germline Genetic Testing for Exocrine Pancreatic Cancer Enables Timely Return of Results and Unveils Low Uptake of Cascade Testing. J. Med. Genet. 2021, jmedgenet-2021-108054. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.S.J.; Lee, S.C. BRCA Sequencing of Tumors: Understanding Its Implications in the Oncology Community. Chin. Clin. Oncol. 2020, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Offit, K.; Tkachuk, K.A.; Stadler, Z.K.; Walsh, M.F.; Diaz-Zabala, H.; Levin, J.D.; Steinsnyder, Z.; Ravichandran, V.; Sharaf, R.N.; Frey, M.K.; et al. Cascading after Peridiagnostic Cancer Genetic Testing: An Alternative to Population-Based Screening. J. Clin. Oncol. 2020, 38, 1398–1408. [Google Scholar] [CrossRef]
- Manahan, E.R.; Kuerer, H.M.; Sebastian, M.; Hughes, K.S.; Boughey, J.C.; Euhus, D.M.; Boolbol, S.K.; Taylor, W.A. Consensus Guidelines on Genetictesting for Hereditary Breast Cancer from the American Society of Breast Surgeons. Ann. Surg. Oncol. 2019, 26, 3025. [Google Scholar] [CrossRef]
- Cremin, C.; Lee, M.K.C.; Hong, Q.; Hoeschen, C.; Mackenzie, A.; Dixon, K.; McCullum, M.; Nuk, J.; Kalloger, S.; Karasinska, J.; et al. Burden of Hereditary Cancer Susceptibility in Unselected Patients with Pancreatic Ductal Adenocarcinoma Referred for Germline Screening. Cancer Med. 2020, 9, 4004–4013. [Google Scholar] [CrossRef]
- Armstrong, N.; Ryder, S.; Forbes, C.; Ross, J.; Quek, R.G.W. A Systematic Review of the International Prevalence of BRCA Mutation in Breast Cancer. Clin. Epidemiol. 2019, 11, 543. [Google Scholar] [CrossRef]
- Sun, L.; Brentnall, A.; Patel, S.; Buist, D.S.M.; Bowles, E.J.A.; Evans, D.G.R.; Eccles, D.; Hopper, J.; Li, S.; Southey, M.; et al. A Cost-Effectiveness Analysis of Multigene Testing for All Patients with Breast Cancer. JAMA Oncol. 2019, 5, 1718–1730. [Google Scholar] [CrossRef]
- Manchanda, R.; Patel, S.; Antoniou, A.C.; Levy-Lahad, E.; Turnbull, C.; Evans, D.G.; Hopper, J.L.; Macinnis, R.J.; Menon, U.; Jacobs, I.; et al. Cost-Effectiveness of Population Based BRCA Testing with Varying Ashkenazi Jewish Ancestry. Am. J. Obstet. Gynecol. 2017, 217, 578.e1–578.e12. [Google Scholar] [CrossRef]
- Lehmann, L.S.; Weeks, J.C.; Klar, N.; Garber, J.E. A Population-Based Study of Ashkenazi Jewish Women’s Attitudes toward Genetic Discrimination and BRCA1/2 Testing. Genet. Med. 2002, 4, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Hartge, P.; Struewing, J.P.; Wacholder, S.; Brody, L.C.; Tucker, M.A. The Prevalence of Common BRCA1 and BRCA2 Mutations among Ashkenazi Jews. Am. J. Hum. Genet. 1999, 64, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Frey, M.K.; Kopparam, R.V.; Ni Zhou, Z.; Fields, J.C.; Buskwofie, A.; Carlson, A.D.; Caputo, T.; Holcomb, K.; Chapman-Davis, E. Prevalence of Nonfounder BRCA1/2 Mutations in Ashkenazi Jewish Patients Presenting for Genetic Testing at a Hereditary Breast and Ovarian Cancer Center. Cancer 2019, 125, 690–697. [Google Scholar] [CrossRef] [PubMed]
- John, E.M.; Miron, A.; Gong, G.; Phipps, A.I.; Felberg, A.; Li, F.P.; West, D.W.; Whittemore, A.S. Prevalence of Pathogenic BRCA1 Mutation Carriers in 5 US Racial/Ethnic Groups. JAMA 2007, 298, 2869–2876. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.J.; Reid, J.E.; Burbidge, L.A.; Pruss, D.; Deffenbaugh, A.M.; Frye, C.; Wenstrup, R.J.; Ward, B.E.; Scholl, T.A.; Noll, W.W. BRCA1 and BRCA2 Mutations in Women of Different Ethnicities Undergoing Testing for Hereditary Breast-Ovarian Cancer. Cancer 2009, 115, 2222–2233. [Google Scholar] [CrossRef]
- Kolnsberg, L.; Riffelmann, M.; Friedrich, M. Comparison of Serum 25-HydroxyVitamin D Levels in Patients with Malignant and Benign Gynaecological Disease. Anticancer Res. 2020, 40, 545–550. [Google Scholar] [CrossRef]
- Abul-Husn, N.S.; Soper, E.R.; Odgis, J.A.; Cullina, S.; Bobo, D.; Moscati, A.; Rodriguez, J.E.; Loos, R.J.F.; Cho, J.H.; Belbin, G.M.; et al. Exome Sequencing Reveals a High Prevalence of BRCA1 and BRCA2 Founder Variants in a Diverse Population-Based Biobank. Genome Med. 2020, 12, 2. [Google Scholar] [CrossRef]
- Abdulrashid, K.; Alhussaini, N.; Ahmed, W.; Thalib, L. Prevalence of BRCA Mutations among Hereditary Breast and/or Ovarian Cancer Patients in Arab Countries: Systematic Review and Meta-Analysis. BMC Cancer 2019, 19, 256. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Population | Genetic Testing | Main Findings |
|---|---|---|---|
| Metcalfe 2010 [7] Metcalfe 2013 [40] | AJ * women 25–80 y Ontario, Canada (n = 2082) | Three BRCA1/2 AJ founder mutations |
|
| Manchada 2015 [41] Manchada 2020 [42] | Randomized controlled trial of AJ women/men (n = 1034) >18 y in Northern London | Three BRCA1/2 AJ founder mutations |
|
| Narod 2021 [44] The Screen Project | Canadians >18 y, open recruitment (n = 1269) | BRCA1/2 mutations |
|
| Grzymski 2020 [8] Healthy Nevada Project | Population-based cohort <18 y (n = 26,906) | BRCA1/2, MLH1, MSH2, MSH6, PMS2 |
|
| Rowley 2019 [9] Lifepool Australia | Women without cancer 50–74 y (n = 5908) | BRCA1/2, PALB2, ATM, CDH1, PTEN, STK11, TP53, BRIP1, RAD51C/D |
|
| Hu 2021 [43] | Breast cancer (n = 32,247) Controls (n = 32,544) | ATM, BARD1, BRCA1/2, CDH1, CHEK2, NF1, PALB2, PTEN, RAD51C/D, TP53 |
|
| Gabai-kapara 2014 [45] | Population-based cohort of AJ men (n = 8195) | BRCA1/2 |
|
| Dorling 2021 [39] | Breast cancer (n = 66,466) Controls (n = 53,461) | 35 gene panel |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tindale, L.C.; Zhantuyakova, A.; Lam, S.; Woo, M.; Kwon, J.S.; Hanley, G.E.; Knoppers, B.; Schrader, K.A.; Peacock, S.J.; Talhouk, A.; et al. Gynecologic Cancer Risk and Genetics: Informing an Ideal Model of Gynecologic Cancer Prevention. Curr. Oncol. 2022, 29, 4632-4646. https://doi.org/10.3390/curroncol29070368
Tindale LC, Zhantuyakova A, Lam S, Woo M, Kwon JS, Hanley GE, Knoppers B, Schrader KA, Peacock SJ, Talhouk A, et al. Gynecologic Cancer Risk and Genetics: Informing an Ideal Model of Gynecologic Cancer Prevention. Current Oncology. 2022; 29(7):4632-4646. https://doi.org/10.3390/curroncol29070368
Chicago/Turabian StyleTindale, Lauren C., Almira Zhantuyakova, Stephanie Lam, Michelle Woo, Janice S. Kwon, Gillian E. Hanley, Bartha Knoppers, Kasmintan A. Schrader, Stuart J. Peacock, Aline Talhouk, and et al. 2022. "Gynecologic Cancer Risk and Genetics: Informing an Ideal Model of Gynecologic Cancer Prevention" Current Oncology 29, no. 7: 4632-4646. https://doi.org/10.3390/curroncol29070368
APA StyleTindale, L. C., Zhantuyakova, A., Lam, S., Woo, M., Kwon, J. S., Hanley, G. E., Knoppers, B., Schrader, K. A., Peacock, S. J., Talhouk, A., Dummer, T., Metcalfe, K., Pashayan, N., Foulkes, W. D., Manchanda, R., Huntsman, D., Stuart, G., Simard, J., & Dawson, L. (2022). Gynecologic Cancer Risk and Genetics: Informing an Ideal Model of Gynecologic Cancer Prevention. Current Oncology, 29(7), 4632-4646. https://doi.org/10.3390/curroncol29070368