Contribution of the IdyllaTM System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients from the ID-MUT Study and Paraffin-Embedded Specimens
2.2. EGFR Mutation Assay by Next-Generation Sequencing Panel CLv3 (Colon and Lung Cancer Panel v3)
2.3. EGFR Mutation Assay by the IdyllaTM System
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
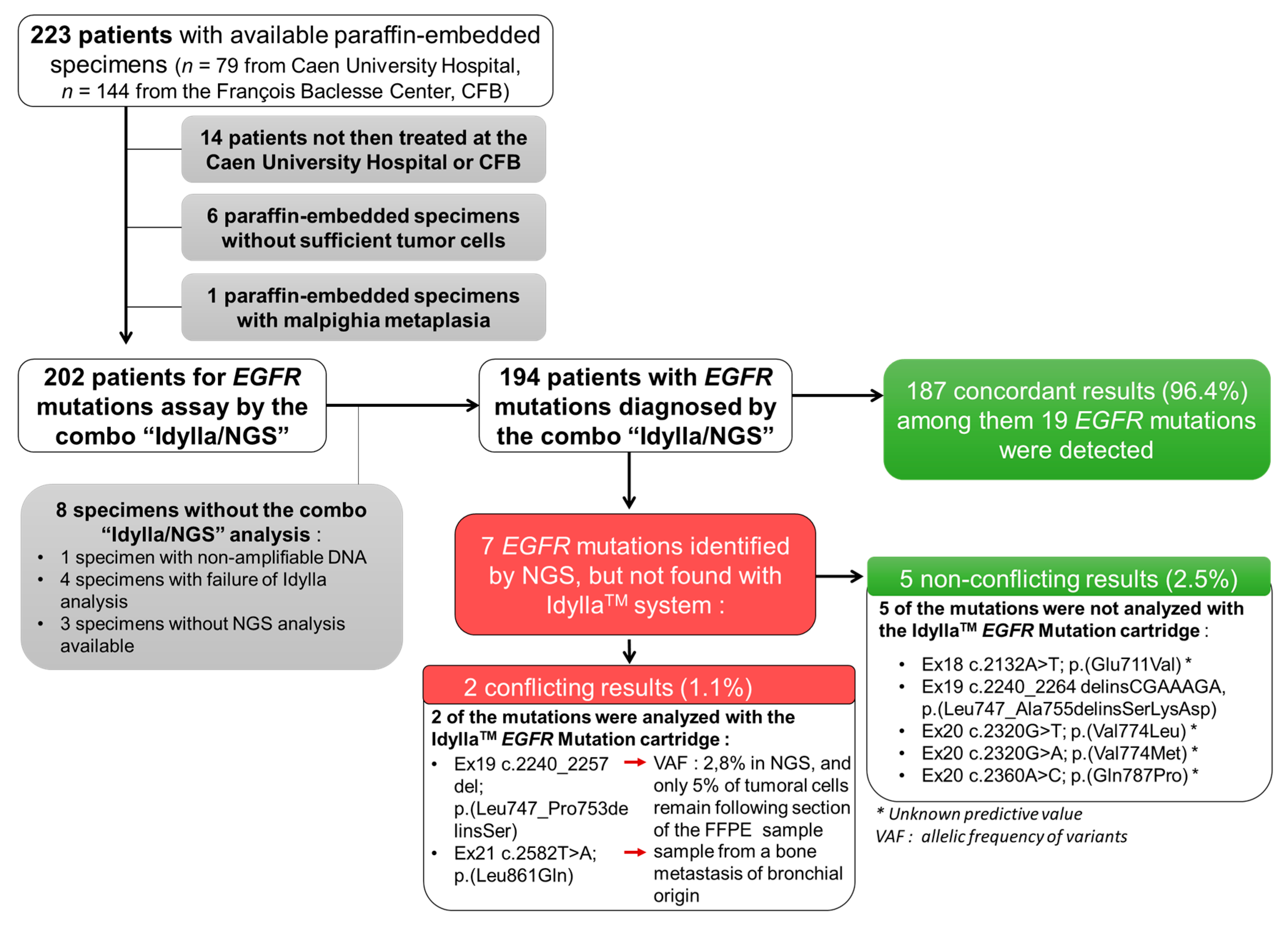
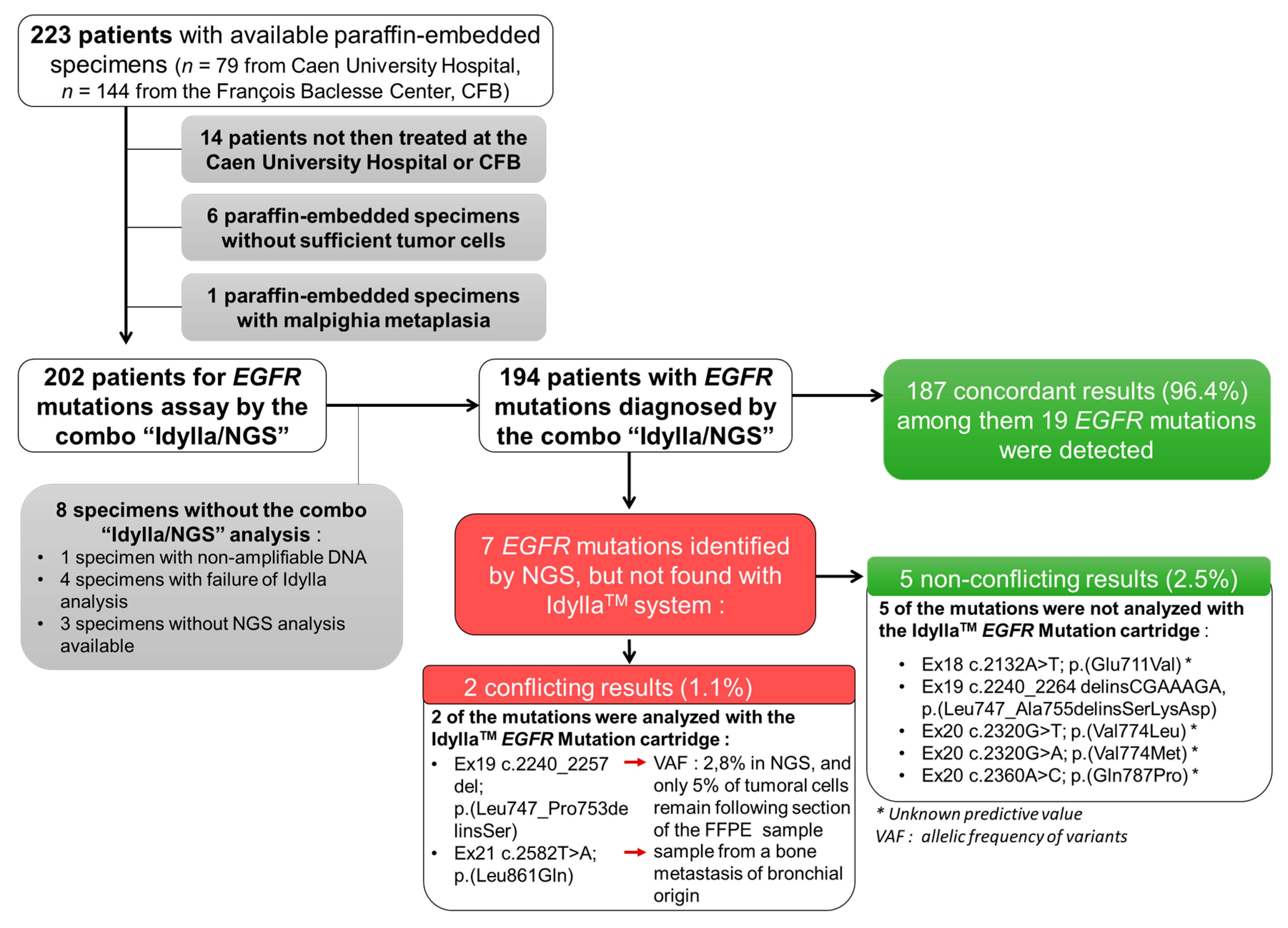
3.2. Concordance of EGFR Genotyping between the IdyllaTM and NGS Methods
3.3. Consideration of the EGFR Genotyping by the IdyllaTM Method in the Treatment Decision
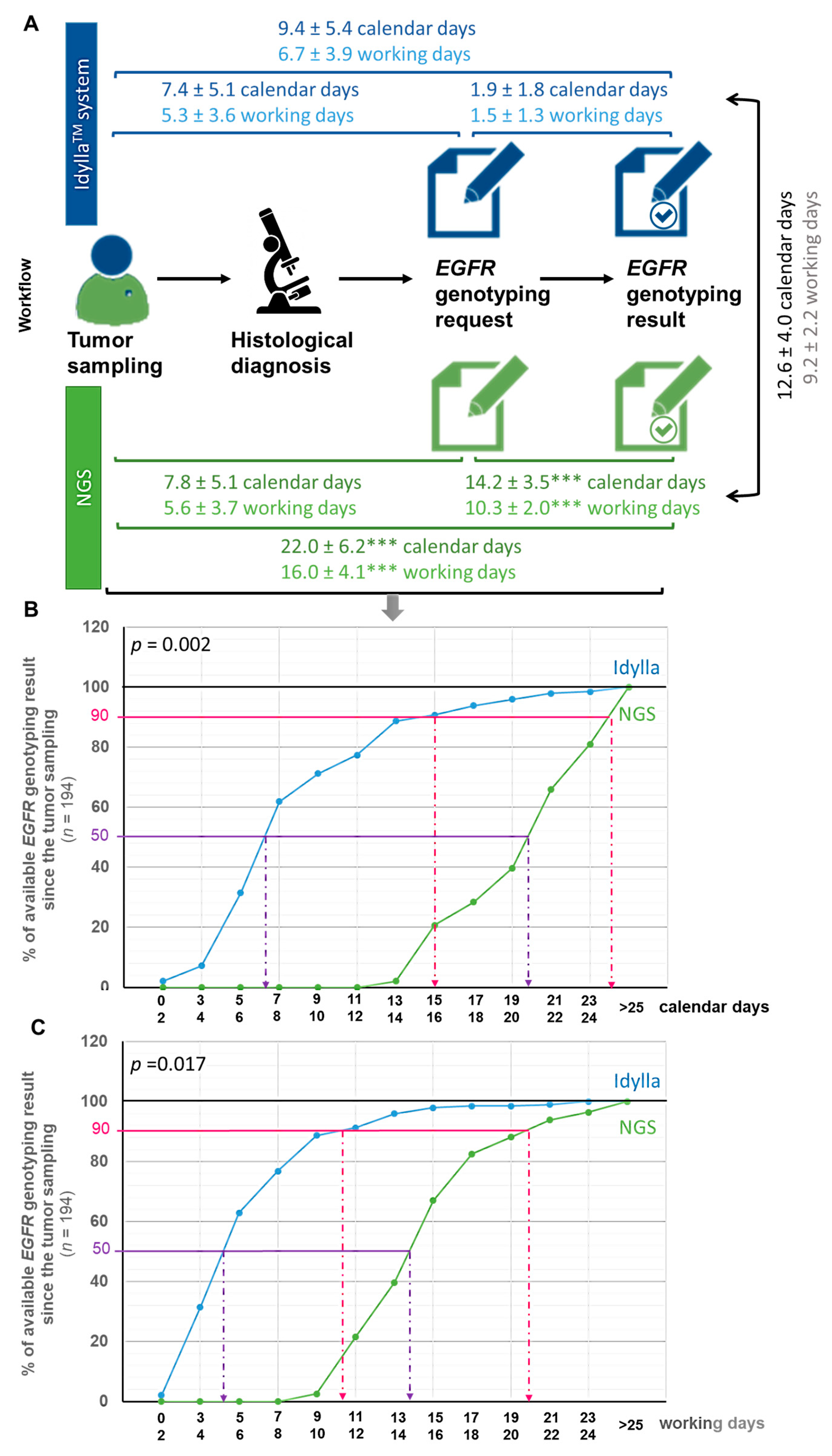
3.4. Turnaround Time (TAT)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hutchinson, B.; Shroff, G.S.; Truong, M.T.; Ko, J.P. Spectrum of lung adenocarcinoma. Semin. Ultrasound CT MRI 2019, 40, 255–264. [Google Scholar] [CrossRef]
- Riihimäki, M.; Hemminki, A.; Fallah, M.; Thomsen, H.; Sundquist, K. Metastatic sites and survival in lung cancer. Lung Cancer 2014, 86, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.M.; Doebele, R.C. Targeted therapies in non-small cell lung cancer: Emerging oncogene targets following the success of epidermal growth factor receptor. Semin. Oncol. 2014, 41, 110–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Recondo, G.; Facchinetti, F.; Olaussen, K.A.; Besse, B.; Friboulet, L. Making the first move in EGFR-driven or ALK-driven NSCLC: First-generation or next-generation TKI? Nat. Rev. Clin. Oncol. 2018, 15, 694–708. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- INCa (French National Cancer Institute). Accès Aux Tests Moléculaires EGFR, RAS et BRAF/Résultats D’une Enquête Dans 5 Régions Françaises. 2016. Available online: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Acces-aux-tests-moleculaires-EGFR-RAS-et-BRAF-Resultats-d-une-enquete-dans-5-regions-francaises (accessed on 1 January 2016).
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in resected EGFR-mutated non–small-cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Cooper, W.A.; Lam, D.C.L.; O’Toole, S.A.; Minna, J.D. Molecular biology of lung cancer. J. Thorac. Dis. 2013, 5, S479–S490. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Non-Small Cell Lung Cancer Version 4.2019; NCCN Guidelines: Plymouth Meeting, PA, USA, 2019. [Google Scholar]
- Lambros, L.; Caumont, C.; Guibourg, B.; Barel, F.; Quintin-Roué, I.; Marcorelles, P.; Merlio, J.P.; Uguen, A. Evaluation of a fast and fully automated platform to diagnose EGFR and KRAS mutations in formalin-fixed and paraffin-embedded non-small cell lung cancer samples in less than one day. J. Clin. Pathol. 2017, 70, 544–549. [Google Scholar] [CrossRef]
- Thomas De Montpréville, V.; Ghigna, M.R.; Lacroix, L.; Lemoine, A.; Besse, B.; Mercier, O.; Fadel, É.; Dorfmuller, P.; Le Chevalier, T. EGFR and KRAS molecular genotyping for pulmonary carcinomas: Feasibility of a simple and rapid technique implementable in any department of pathology. Pathol. Res. Pract. 2017, 213, 793–798. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.; Rappa, A.G.; Gragnano, G.; Malapelle, U.; Troncone, G.; Barberis, M. Idylla Assay and next generation sequencing: An integrated EGFR mutational testing algorithm. J. Clin. Pathol. 2018, 71, 745–750. [Google Scholar] [CrossRef]
- Evrard, S.M.; Taranchon-Clermont, E.; Rouquette, I.; Murray, S.; Dintner, S.; Nam-Apostolopoulos, Y.-C.; Bellosillo, B.; Varela, M.; Nadal, E.; Wiedorn, K.H.; et al. Multicenter evaluation of the fully automated PCR-based Idylla EGFR Mutation Assay on formalin-fixed, paraffin-embedded tissue of human lung cancer. J. Mol. Diagn. 2019, 21, 1010–1024. [Google Scholar] [CrossRef] [PubMed]
- Al-Turkmani, M.R.; Suriawinata, M.A.; Deharvengt, S.J.; Green, D.C.; Black, C.C.; Shirai, K.; Dragnev, K.H.; Tsongalis, G.J. Rapid EGFR mutation testing in lung cancer tissue samples using a fully automated system and single-use cartridge. Pract. Lab. Med. 2020, 20, e00156. [Google Scholar] [CrossRef] [PubMed]
- Colling, R.; Bancroft, H.; Langman, G.; Soilleux, E.J. Fully automated real-time PCR for EGFR testing in non-small cell lung carcinoma. Virchows Arch. 2019, 474, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chevalier, L.M.; Billaud, A.; Passot, C.; Renoult, A.; Bigot, F.; Verrièle, V.; Morel, A. EGFR molecular characterization in non-small cell bronchic cancer: Comparative prospective study by NGS and Idylla platform technologies. Ann. Pathol. 2020, 40, 389–400. [Google Scholar] [CrossRef]
- Bocciarelli, C.; Cohen, J.; Pelletier, R.; Tran Van Nhieu, J.; Derman, J.; Favre, L.; Bourgogne, A.; Monnet, I.; Chouaid, C.; Pujals, A. Evaluation of the Idylla system to detect the EGFRT790M mutation using extracted DNA. Pathol. Res. Pract. 2020, 216, 152773. [Google Scholar] [CrossRef]
- Van Haele, M.; Borght, S.V.; Ceulemans, A.; Wieërs, M.; Metsu, S.; Sagaert, X.; Weynand, B. Rapid clinical mutational testing of KRAS, BRAF and EGFR: A prospective comparative analysis of the Idylla technique with high-throughput next-generation sequencing. J. Clin. Pathol. 2019, 73, 35–41. [Google Scholar] [CrossRef]
- Haiduk, T.; Brockmann, M.; Tillmann, R.L.; Pieper, M.; Lüsebrink, J.; Schildgen, V.; Schildgen, O. Comparison of Biocartis IDYLLATM cartridge assay with Qiagen GeneReader NGS for detection of targetable mutations in EGFR, KRAS/NRAS, and BRAF genes. Exp. Mol. Pathol. 2021, 120, 104634. [Google Scholar] [CrossRef]
- Lee, E.; Jones, V.; Topkas, E.; Harraway, J. Reduced sensitivity for EGFR T790M mutations using the Idylla EGFR Mutation Test. J. Clin. Pathol. 2021, 74, 43–47. [Google Scholar] [CrossRef]
- Ilie, M.; Butori, C.; Lassalle, S.; Heeke, S.; Piton, N.; Sabourin, J.C.; Tanga, V.; Washetine, K.; Long-Mira, E.; Maitre, P.; et al. Optimization of EGFR mutation detection by the fully-automated qPCR-based Idylla system on tumor tissue from patients with non-small cell lung cancer. Oncotarget 2017, 8, 103055–103062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Garcia, M.; Weynand, B.; Gómez-Izquierdo, L.; Hernández, M.J.; Blanco, Á.M.; Varela, M.; Matias-Guiu, X.; Nadal, E.; Márquez-Lobo, B.; Alarcão, A.; et al. Clinical performance evaluation of the IdyllaTM EGFR Mutation Test on formalin-fixed paraffin-embedded tissue of non-small cell lung cancer. BMC Cancer 2020, 20, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaanane, H.; El Attar, H.; Louahabi, A.; Berradi, H.; Idrissi, H.H.; Khyatti, M.; Nadifi, S. Targeted methods for molecular characterization of EGFR mutational profile in lung cancer Moroccan cohort. Gene 2019, 705, 36–43. [Google Scholar] [CrossRef]
- De Luca, C.; Gragnano, G.; Pisapia, P.; Vigliar, E.; Malapelle, U.; Bellevicine, C.; Troncone, G. EGFR mutation detection on lung cancer cytological specimens by the novel fully automated PCR-based Idylla EGFR Mutation Assay. J. Clin. Pathol. 2017, 70, 295–300. [Google Scholar] [CrossRef]
- De Luca, C.; Conticelli, F.; Leone, A.; Gragnano, G.; Salatiello, M.; Galasso, P.; Pisapia, P.; Grillo, L.R.; Iaccarino, A.; Vigliar, E.; et al. Is the Idylla EGFR Mutation Assay feasible on archival stained cytological smears? A pilot study. J. Clin. Pathol. 2019, 72, 609–614. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Azzolli, C.G.; Fintelmann, F.; Mino-Kenudson, M.; Farago, A.F.; Gainor, J.F.; Jiang, G.; Piotrowska, Z.; Heist, R.S.; Lennes, I.T.; et al. Clinical utility of rapid EGFR genotyping in advanced lung cancer. JCO Precis. Oncol. 2018, 2, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.; Silveira, C.; Janeiro, A.; Malveiro, S.; Oliveira, A.R.; Felizardo, M.; Nogueira, F.; Teixeira, E.; Martins, J.; Carmo-Fonseca, M. Detection of rare and novel EGFR mutations in NSCLC patients: Implications for treatment-decision. Lung Cancer 2020, 139, 35–40. [Google Scholar] [CrossRef]
- Boureille, A.; Ferraro-Peyret, C.; Pontarollo, G.; Confavreux, C.; Pialat, J.-B.; Isaac, S.; Forest, F.; Yvorel, V.; Watkin, E.; Girard, N.; et al. Rapid detection of EGFR mutations in decalcified lung cancer bone metastasis. J. Bone Oncol. 2020, 21, 100277. [Google Scholar] [CrossRef]
- Lassalle, S.; Hofman, V.; Heeke, S.; Benzaquen, J.; Long, E.; Poudenx, M.; Lantéri, E.; Boutros, J.; Tanga, V.; Zahaf, K.; et al. Targeted assessment of the EGFR status as reflex testing in treatment-naive non-squamous cell lung carcinoma patients: A single laboratory experience (LPCE, Nice, France). Cancers 2020, 12, 955. [Google Scholar] [CrossRef] [Green Version]
- Momeni-Boroujeni, A.; Salazar, P.; Zheng, T.; Mensah, N.; Rijo, I.; Dogan, S.; Yao, J.; Moung, C.; Vanderbilt, C.; Benhamida, J.; et al. Rapid EGFR mutation detection using the Idylla platform: Single-institution experience of 1200 cases analyzed by an in-house developed pipeline and comparison with concurrent next-generation sequencing results. J. Mol. Diagn. 2021, 23, 310–322. [Google Scholar] [CrossRef]
- Heeke, S.; Hofman, P. EGFR mutation analysis in non-small cell lung carcinoma from tissue samples using the fully automated IdyllaTM qPCR system. Methods Mol. Biol. 2019, 2054, 147–155. [Google Scholar] [PubMed]
- Huang, H.; Springborn, S.; Haug, K.; Bartow, K.; Samra, H.; Menon, S.; Mackinnon, A.C. Evaluation, validation, and implementation of the Idylla system as rapid molecular testing for precision medicine. J. Mol. Diagn. 2019, 21, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, P.; Stevenson, T.; Powari, M. Use of the Idylla EGFR mutation test for variant detection in non–small cell lung cancer samples. Am. J. Clin. Pathol. 2021, 156, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Nunnari, J.; Graziano, P.; Muscarella, L.A.; Rossi, A.; Grillo, L.R.; Montrone, G.; Di Lorenzo, A.; Bronzini, M.; Leone, A. Rapid EGFR evaluation from used H&E, IHC and FISH diagnostic slides with the Idylla platform. J. Clin. Pathol. 2021. [Google Scholar] [CrossRef]
- Heeke, S.; Hofman, V.; Benzaquen, J.; Otto, J.; Tanga, V.; Zahaf, K.; Allegra, M.; Long-Mira, E.; Lassalle, S.; Marquette, C.-H.; et al. Detection of EGFR mutations from plasma of NSCLC patients using an automatic cartridge-based PCR system. Front. Pharmacol. 2021, 12, 657743. [Google Scholar] [CrossRef]
- Gilson, P.; Saurel, C.; Salleron, J.; Husson, M.; Demange, J.; Merlin, J.-L.; Harlé, A. Evaluation of the Idylla ctEGFR Mutation Assay to detect EGFR mutations in plasma from patients with non-small cell lung cancers. Sci. Rep. 2021, 11, 10470. [Google Scholar] [CrossRef]
- Grant, J.; Stanley, A.; Balbi, K.; Gerrard, G.; Bennett, P. Performance evaluation of the Biocartis Idylla EGFR Mutation Test using pre-extracted DNA from a cohort of highly characterised mutation positive samples. J. Clin. Pathol. 2021. [Google Scholar] [CrossRef]
- Arcila, M.E.; Yang, S.-R.; Momeni, A.; Mata, D.A.; Salazar, P.; Chan, R.; Elezovic, D.; Benayed, R.; Zehir, A.; Buonocore, D.J.; et al. Ultrarapid EGFR mutation screening followed by comprehensive next-generation sequencing: A feasible, informative approach for lung carcinoma cytology specimens with a high success rate. JTO Clin. Res. Rep. 2020, 1, 100077. [Google Scholar] [CrossRef]
- Wang, S.; Tsui, S.; Liu, C.; Song, Y.; Liu, D. EGFR C797S mutation mediates resistance to third-generation inhibitors in T790M-positive non-small cell lung cancer. J. Hematol. Oncol. 2016, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Lisberg, A.; Cummings, A.; Goldman, J.; Bornazyan, K.; Reese, N.; Wang, T.; Coluzzi, P.; Ledezma, B.; Mendenhall, M.; Hunt, J.; et al. A phase II study of pembrolizumab in EGFR-mutant, PD-L1+, tyrosine kinase inhibitor naïve patients with advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1138–1145. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.J.; Chin, E.; Yeap, B.Y.; Ferris, L.A.; Kamesan, V.; Lennes, I.T.; Sequist, L.V.; Heist, R.S.; Mino-Kenudson, M.; Gainor, J.F.; et al. Increased hepatotoxicity associated with sequential immune checkpoint inhibitor and crizotinib therapy in patients with non–small cell lung cancer. J. Thorac. Oncol. 2019, 14, 135–140. [Google Scholar] [CrossRef]
- Oshima, Y.; Tanimoto, T.; Yuji, K.; Tojo, A. EGFR–TKI-associated interstitial pneumonitis in nivolumab-treated patients with non–small cell lung cancer. JAMA Oncol. 2018, 4, 1112–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc-Durand, F.; Florescu, M.; Tehfe, M.; Routy, B.; Alameddine, R.; Tran-Thanh, D.; Blais, N. Improvement of EGFR Testing over the last decade and impact of delaying TKI initiation. Curr. Oncol. 2021, 28, 1045–1055. [Google Scholar] [CrossRef] [PubMed]
- Le Flahec, G.; Guibourg, B.; Marcorelles, P.; Uguen, A. Financial implications of Idylla testing in colorectal cancer, lung cancer and melanoma: A French laboratory point of view. J. Clin. Pathol. 2017, 70, 906–907. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Total (n = 223) | CHU (n = 79) | CFB (n = 144) | Patients with EGFR Mutation (n = 25) | |
|---|---|---|---|---|
| Population | ||||
| Male | 126 (56.5%) | 47 (59.5%) | 79 (54.8%) | 8 (32.0%) |
| Female | 97 (43.5%) | 32 (40.5%) | 65 (45.2%) | 17 (68.0%) |
| Age (mean ± SD) years old (range) years old | 65.4 ± 9.8 [36.5–89.8] | 64.0 ± 9.2 [39.6–83.2] | 66.2 ± 10.1 [36.5–89.8] | 68.5 ± 10.1 [47.3–81.1] |
| Smoker status 1 | ||||
| Never-smokers Smokers ≤ 10 pack-years Smokers > 10 pack-years | 39 (17.5%) 9 (4.1%) 167 (74.8%) | 10 (14.1%) 2 (2.8%) 59 (83.1%) | 29 (20.1%) 7 (4.9%) 108 (75.0%) | 15 (60.0%) 4 (16.0%) 6 (24.0%) |
| Stage | ||||
| I (A/B) | 7 (4/3) (3.1%) | 4 (2/2) (5%) | 3 (2/1) (20.1%) | 1 (1/0) (4%) |
| II (A/B) | 6 (2/4) (2.7%) | 3 (1/2) (3.8%) | 3 (1/2) (20.1%) | 1 (1/0) (4%) |
| III (A/B/C) | 31 (18/10/3) (13.9%) | 8 (4/4/0) (10%) | 23 (14/6/3) (15.9%) | 2 (2/0/0) (8%) |
| IV (A/B) | 164 (47/117) (73.5%) | 52 (10/42) (65.8%) | 112 (37/75) (77.8%) | 21 (7/14) (84%) |
| Histology according to the WHO 2015 4th edition | ||||
Adenocarcinoma (ADC)
| 164 (73.6%)
| 57 (72.1%)
| 107 (74.3%)
| 22 (88.0%)
|
| NSCLC 2 NOS 3 | 30 (13.4%) | 12 (15.2%) | 18 (12.5%) | 0 |
| NSCLC in favor of an ADC | 21 (9.4%) | 10 (12.6%) | 11 (7.5%) | 3 (12.0%) |
| Squamous cell carcinoma | 6 (2.7%) | 0 | 6 (4.1%) | 0 |
| Carcinoid tumor | 1 (0.4%) | 0 | 1 (0.7%) | 0 |
| Small cell carcinoma and compound ADC | 1 (0.4%) | 0 | 1 (0.7%) | 0 |
| Nature of tumoral sample | ||||
| Fibroendoscopy biopsy | 87 (39.0%) | 42 (53.2%) | 45 (31.2%) | 9 (36.0%) |
| Fine needle aspiration | 57 (25.6%) | 30 (38.0%) | 27 (18.8%) | 6 (24.0%) |
| Biopsy by scanner | 42 (18.8%) | 0 | 42 (29.2%) | 6 (24.0%) |
| Ultrasound biopsy | 30 (13.5%) | 2 (2.5%) | 28 (19.4%) | 3 (12.0%) |
| Surgical biopsy | 7 (3.1%) | 5 (6.3%) | 2 (1.4%) | 1 (4.0%) |
| Localization | ||||
| Lung | 112 (50.2%) | 47 (59.5%) | 65 (45.2%) | 12 (48.0%) |
| Lymphadenopathy | 61 (27.3%) | 27 (34.2%) | 34 (23.7%) | 6 (24.0%) |
| Bone metastasis | 20 (8.9%) | 1 (1.3%) | 19 (13.0%) | 5 (20.0%) |
| Pleural metastasis | 5 (2.3%) | 1 (1.3%) | 4 (2.8%) | 0 |
| Metastasis in other locations | 21 (9.4%) | 0 | 21 (14.6%) | 1 (4.0%) |
| Brain | 2 (0.9%) | 2 (2.5%) | 0 | 0 |
| Pleural fluid | 2 (0.9%) | 1 (1.3%) | 1 (0.7%) | 1 (4.0%) |
| Time for: | ||||||
|---|---|---|---|---|---|---|
| Patient | Gender | Smoker Status Histology p. Stage | EGFR Mutation | EGFR Genotyping by IdyllaTM * | EGFR Genotyping by NGS * | EGFR-TKI Initiation * |
| 18 | F | Never-smoker NSCLC in favor of an ADC, IVB | ex19 c.2240_2257del; p (Leu747_Pro753delinsSer) | 5 cd | 15 cd | 12 cd on IdyllaTM |
| 32 | F | Never-smoker ADC, IVB | ex21 c.2573T > G p. (Leu858Arg) | 11 cd | 20 cd | 18 cd on IdyllaTM |
| 40 | F | ≤10 pack-years ADC, IVB | ex19 c.2235_2249del; p. (Glu746_Ala750del) | 5 cd | 15 cd | 8 cd on IdyllaTM |
| 81 | F | Never-smoker ADC, IVB | ex21 c.2573T > G; p. (Leu858Arg) | 9 cd | 23 cd | 9 cd on IdyllaTM |
| 96 | F | Never-smoker ADC, IVB | ex19 c2239_2248delinsC; p. (Leu747_Ala750delinsPro) | 7 cd | 17 cd | 14 cd on IdyllaTM |
| 171 | F | >10 pack-years ADC, IVA | ex19 c2240_2254del; p. (Leu747_Thr751del) | 6 cd | 21 cd | 12 cd on IdyllaTM |
| 183 | F | Never-smoker ADC, IIIA | ex19 c2235_2249del; p. (Glu746_Ala750del) | 7 cd | 23 cd | 10 cd on IdyllaTM |
| 187 | F | ≤10 Pack-years ADC, IVB | ex21 c.2573T > G; p. (Leu858Arg) | 13 cd | 21 cd | 9 cd on IdyllaTM |
| 193 | F | Never-smoker ADC, IVA | ex21 c.2573_2579delinsGGGCCAT; p. (Leu858_Lys860delinsArgAlaIle) | 5 cd | 13 cd | 11 cd on IdyllaTM(1) |
| Mean in EGFR-TKI Initiation on IdyllaTM ± SD: 11.4 ± 3.1 cd (7.7 ± 1.2 wd) | ||||||
| 16 | F | Never-smoker ADC, IVB | ex19 c.2235_2249del; p. (Glu746_Ala750del) | 12 cd | 23 cd | 28 cd on NGS |
| 20 | F | Never-smoker ADC, IVB | ex21 c.2573T > G; p. (Leu858Arg) | 16 cd | 23 cd | 45 cd on NGS |
| 62 | M | Never-smoker ADC, IVB | ex19 c2240_2254del p. (Leu747_Thr751del) | 13 cd | 26 cd | 31 cd on NGS |
| 84 | M | >10 pack-years ADC, IVB | ex19 c2240_2254del; p. (Leu747_Thr751del), eX20 c.2305G > A; p (Val769MET) | 3 cd | 16 cd | 25 cd on NGS |
| 85 | M | Never-smoker ADC, IVA | ex19 c2236_2250del; p. (Glu746_Ala750del) | 7 cd | 19 cd | 25 cd on NGS |
| 97 | F | Never-smoker ADC, IIIA | ex19 c.2235_2249del; p. (Glu746_Ala750del) | 7 cd | 16 cd | 20 cd on NGS |
| 105 | F | Never-smoker ADC, IVB | ex21 c.2582T > A p. (Leu861Gln) | 12 cd | 22 cd | 28 cd on NGS |
| 110 | F | Never-smoker ADC, IVA | ex18 c.2132A > T; p. (Glu711Val) | 5 cd | 15 cd | 15 cd on NGS |
| 134 | M | ≤10 pack-years ADC, IVB | ex20 c.2319_2320insTAC; p. (His773_Val774insTyr) | 8 cd | 22 cd | 29 cd on NGS |
| 162 | F | ≤10 pack-years NSCLC in favor of an ADC, IVB | ex 19 c.2240_2257del; p. (Leu747_Pro753delinsSer) | 7 cd | 16 cd | 20 cd on NGS |
| 194 | M | >10 pack-years ADC, IVB | ex20 c.2320G > A; p. (Val774Met) | 4 cd | 11 cd | 14 cd on NGS |
| 211 | F | Never-smoker ADC, IIA | ex21 c.2573T > G; p. (Leu858Arg) | 13 cd | 16 cd | 27 cd on NGS |
| Mean in EGFR-TKI Initiation on NGS ± SD: 27.2 ± 8.3 cd (20.3 ± 6.7 wd) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petiteau, C.; Robinet-Zimmermann, G.; Riot, A.; Dorbeau, M.; Richard, N.; Blanc-Fournier, C.; Bibeau, F.; Deshayes, S.; Bergot, E.; Gervais, R.; et al. Contribution of the IdyllaTM System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations. Curr. Oncol. 2021, 28, 4432-4445. https://doi.org/10.3390/curroncol28060376
Petiteau C, Robinet-Zimmermann G, Riot A, Dorbeau M, Richard N, Blanc-Fournier C, Bibeau F, Deshayes S, Bergot E, Gervais R, et al. Contribution of the IdyllaTM System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations. Current Oncology. 2021; 28(6):4432-4445. https://doi.org/10.3390/curroncol28060376
Chicago/Turabian StylePetiteau, Constance, Gwladys Robinet-Zimmermann, Adèle Riot, Marine Dorbeau, Nicolas Richard, Cécile Blanc-Fournier, Frédéric Bibeau, Simon Deshayes, Emmanuel Bergot, Radj Gervais, and et al. 2021. "Contribution of the IdyllaTM System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations" Current Oncology 28, no. 6: 4432-4445. https://doi.org/10.3390/curroncol28060376
APA StylePetiteau, C., Robinet-Zimmermann, G., Riot, A., Dorbeau, M., Richard, N., Blanc-Fournier, C., Bibeau, F., Deshayes, S., Bergot, E., Gervais, R., & Levallet, G. (2021). Contribution of the IdyllaTM System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations. Current Oncology, 28(6), 4432-4445. https://doi.org/10.3390/curroncol28060376