BRCA1/2 Mutation Types Do Not Affect Prognosis in Ovarian Cancer Patients

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Cohort
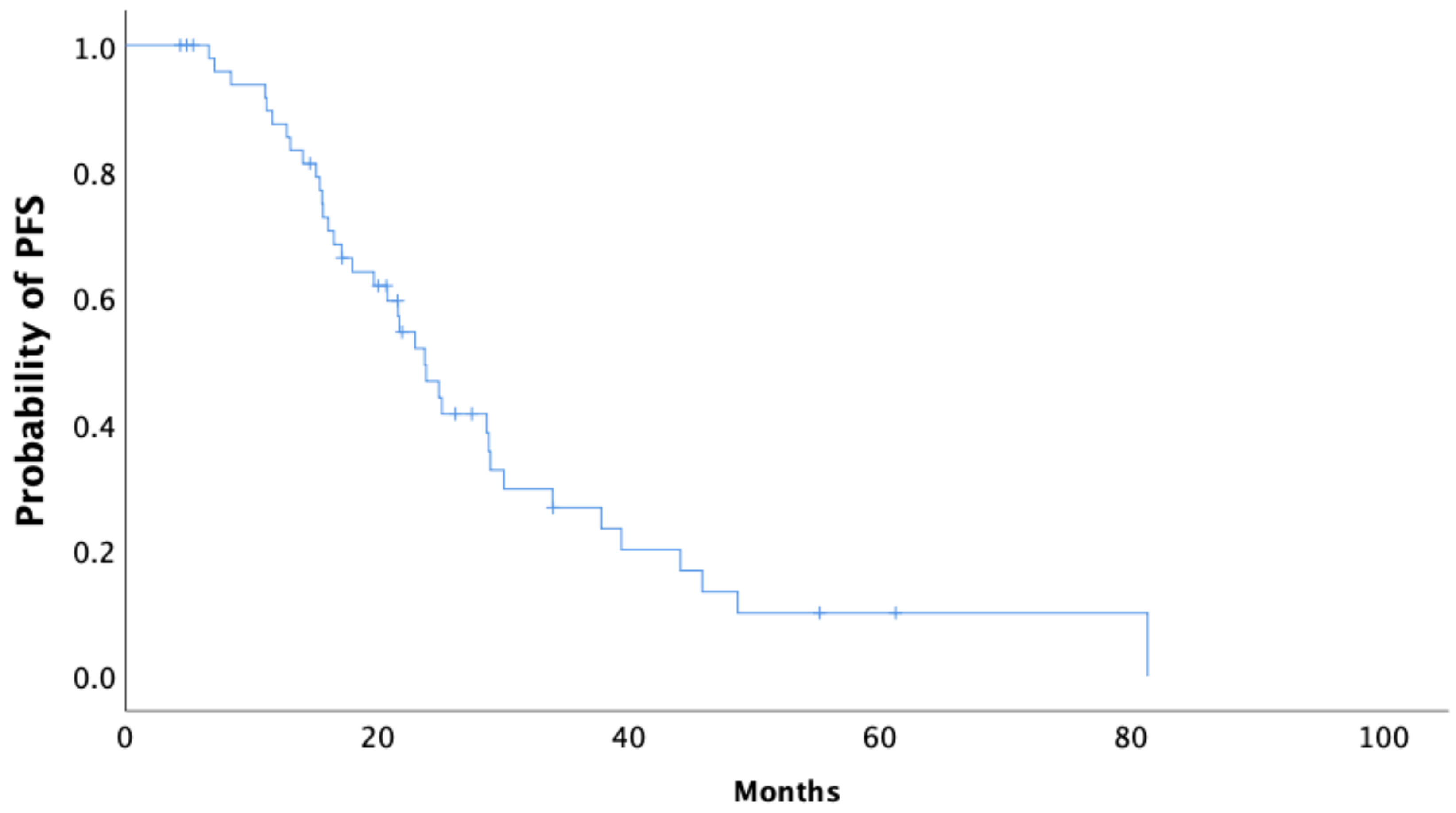
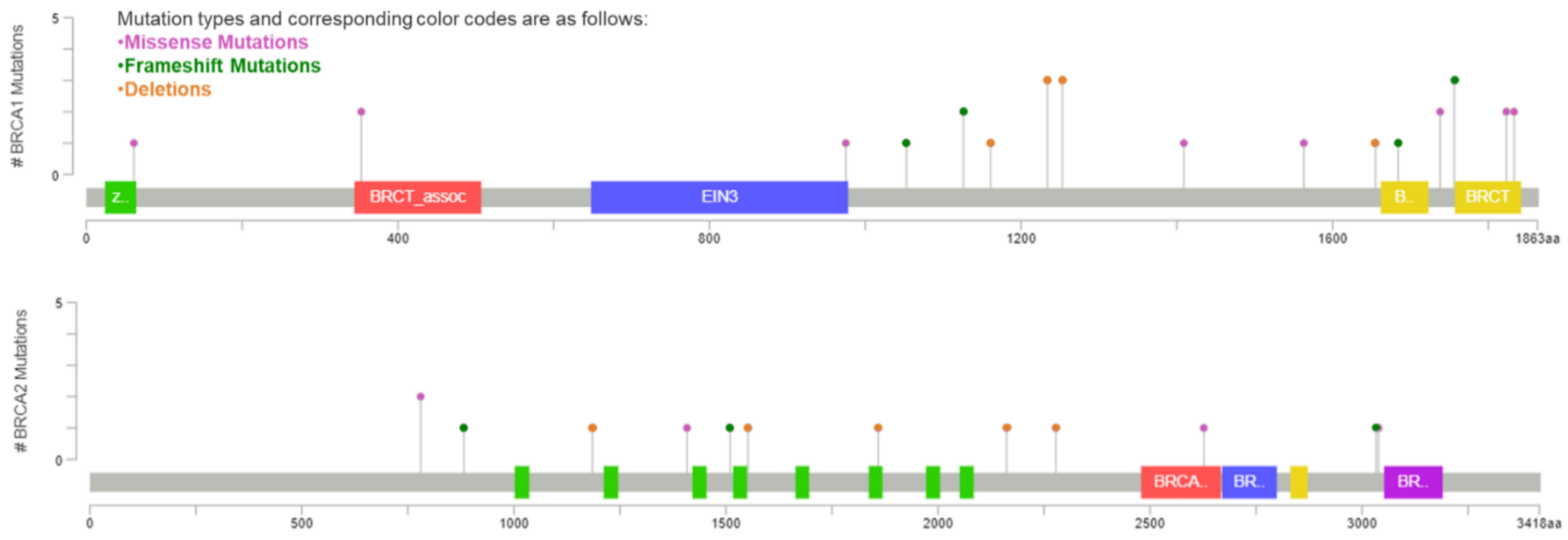
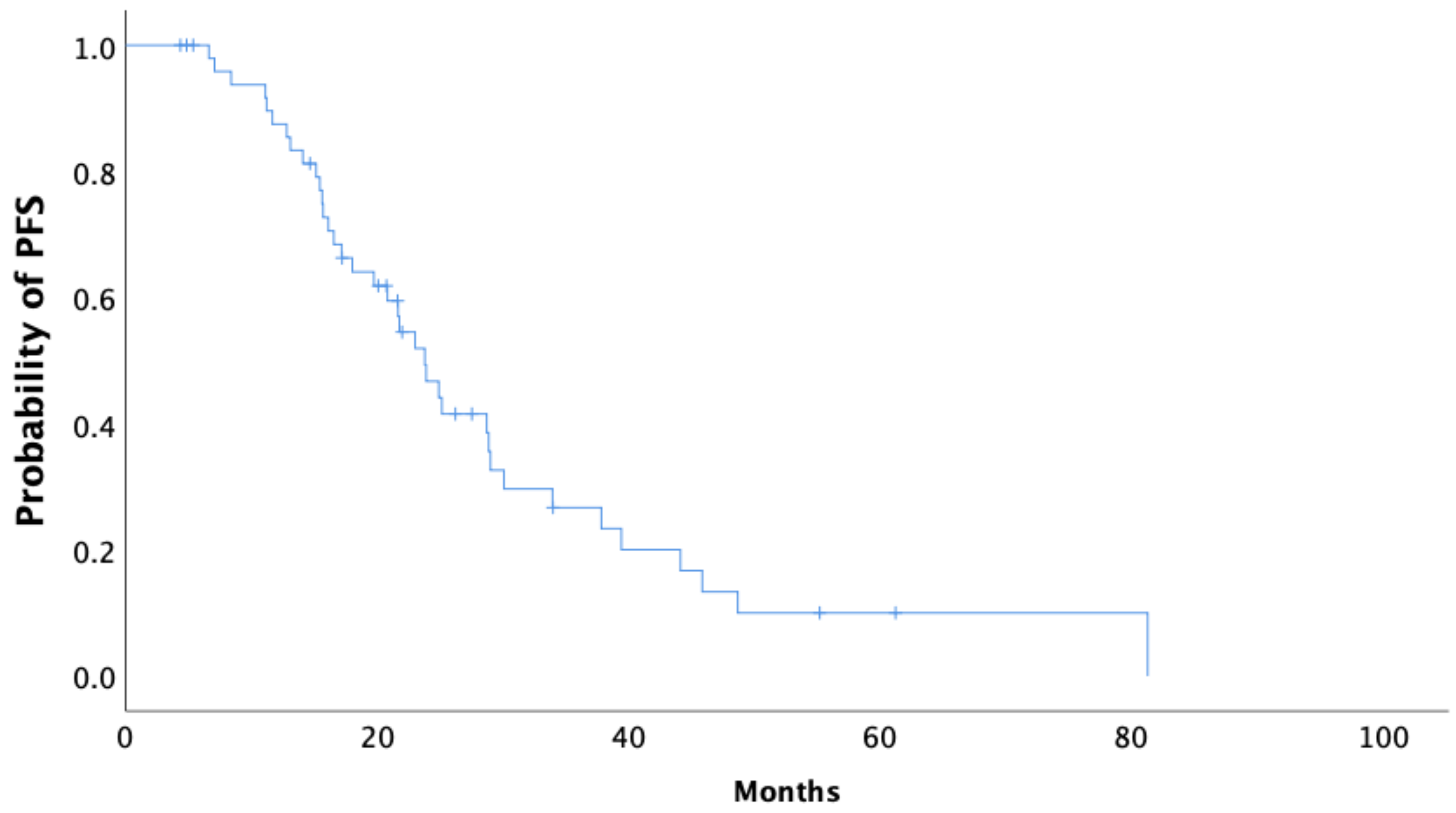
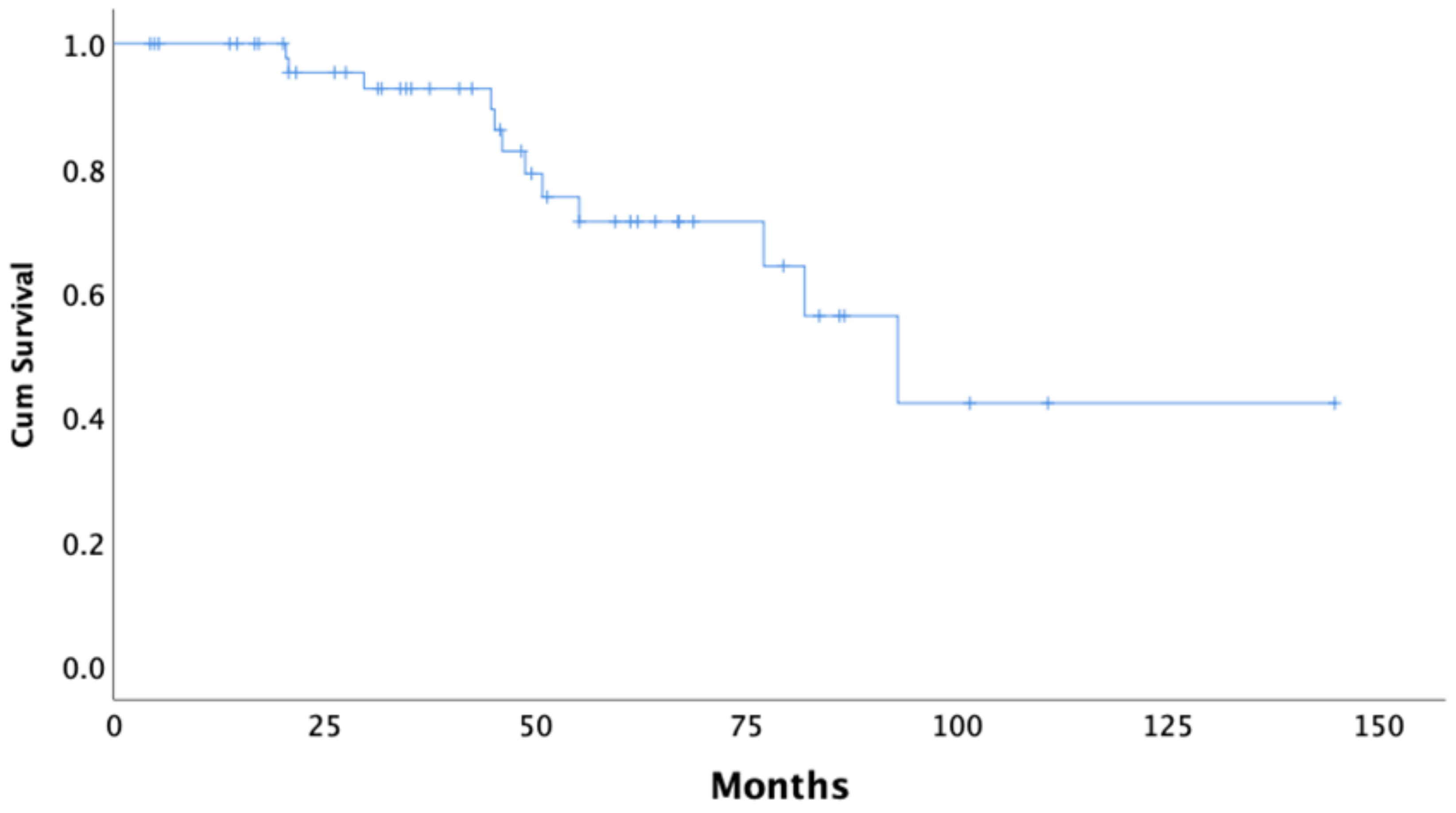
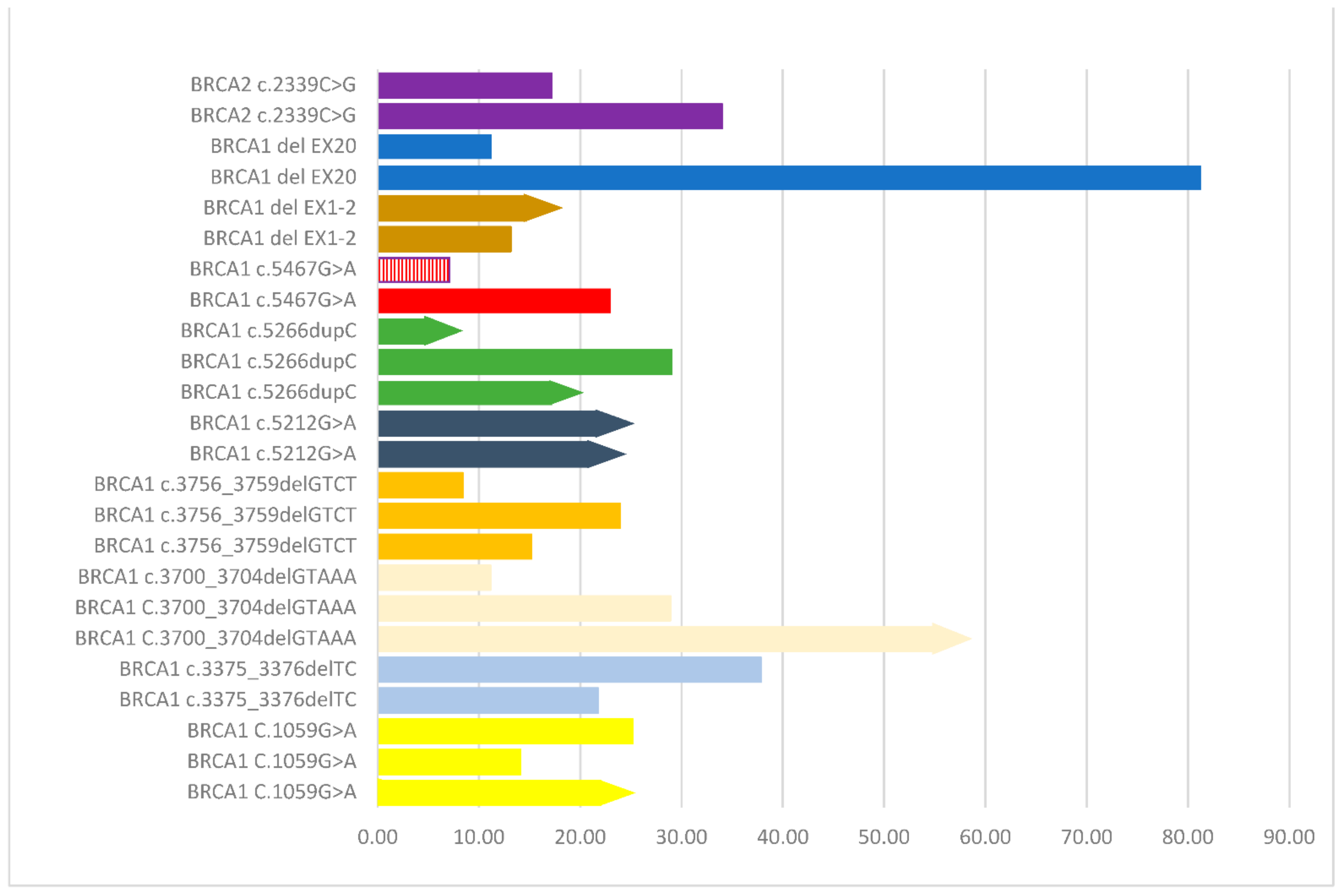
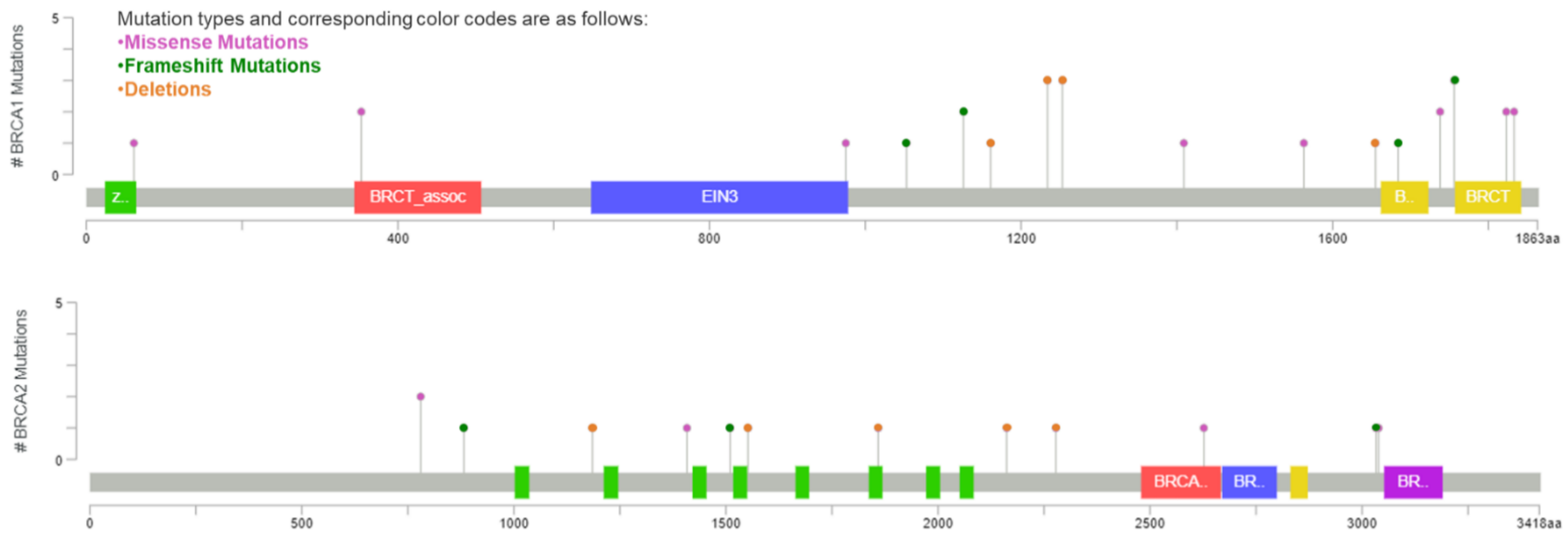
2.2. Location of Mutations in BRCA and Survival in the Study Cohort
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Genetic Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bell, D.; Berchuck, A.; Birrer, M.; Chien, J.; Cramer, D.W.; Dao, F.; Dhir, R.; Disaia, P.; Gabra, H.; Glenn, P.; et al. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Cohen, P.A.; Powell, A.; Böhm, S.; Gilks, C.B.; Stewart, C.J.; Meniawy, T.; Bulsara, M.; Avril, S.; Brockbank, E.C.; Bosse, T.; et al. Pathological chemotherapy response score is prognostic in tubo-ovarian high-grade serous carcinoma: A systematic review and meta-analysis of individual patient data. Gynecol. Oncol. 2019, 154, 441–448. [Google Scholar] [CrossRef] [Green Version]
- González-Martín, A.; Pothuri, B.; Vergote, I.; Christensen, R.D.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 1949–1961. [Google Scholar] [CrossRef] [Green Version]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.N.; Kachnic, L.A. Roles of BRCA1 and BRCA2 in homologous recombination, DNA replication fidelity and the cellular response to ionizing radiation. Oncogene 2003, 22, 5784–5791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkitaraman, A.R. Cancer Susceptibility and the Functions of BRCA1 and BRCA2. Cell 2002, 108, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Roy, R.; Chun, J.; Powell, S.N. BRCA1 and BRCA2: Different roles in a common pathway of genome protection. Nat. Rev. Cancer 2012, 12, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Moynahan, M.E.; Pierce, A.J.; Jasin, M. BRCA2 Is Required for Homology-Directed Repair of Chromosomal Breaks. Mol. Cell 2001, 7, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Khan, S.; Sun, Y.; Hess, K.; Shmulevich, I.; Sood, A.K.; Zhang, W. Association of BRCA1 and BRCA2 Mutations with Survival, Chemotherapy Sensitivity, and Gene Mutator Phenotype in Patients With Ovarian Cancer. JAMA 2011, 306, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Cristea, M.C.; Frankel, P.; Neuhausen, S.L.; Steele, L.; Engelstaedter, V.; Matulonis, U.; Sand, S.; Tung, N.; Garber, J.E.; et al. Clinical characteristics and outcomes of BRCA-associated ovarian cancer: Genotype and survival. Cancer Genet. 2012, 205, 34–41. [Google Scholar] [CrossRef] [Green Version]
- Van Der Groep, P.; Van Der Wall, E.; Van Diest, P.J. Pathology of hereditary breast cancer. Cell. Oncol. 2011, 34, 71–88. [Google Scholar] [CrossRef] [Green Version]
- Clark, S.L.; Rodriguez, A.M.; Snyder, R.R.; Hankins, G.D.; Boehning, D. Structure-Function of the Tumor Suppressor Brca1. Comput. Struct. Biotechnol. J. 2012, 1, e201204005. [Google Scholar] [CrossRef] [Green Version]
- Welcsh, P.L.; King, M.C. BRCA1 and BRCA2 and the genetics of breast and ovarian cancer. Hum. Mol. Genet. 2001, 10, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Gayther, S.A.; Warren, W.; Mazoyer, S.; Russell, P.A.; Harrington, P.A.; Chiano, M.; Seal, S.; Hamoudi, R.; Van Rensburg, E.J.; Dunning, A.M.; et al. Germline mutations of the BRCA1 gene in breast and ovarian cancer families provide evidence for a genotype—Phenotype correlation. Nat. Genet. 1995, 11, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Holt, J.T.; Thompson, M.E.; Szabo, C.; Robinson-Benion, C.; Arteaga, C.L.; King, M.-C.; Jensen, R.A. Growth retardation and tumour inhibition by BRCA1. Nat. Genet. 1996, 12, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Easton, D. Variation in BRCA1 cancer risks by mutation position. Cancer Epidemiol. Biomarks Prev. 2002, 11, 329–336. [Google Scholar]
- Gayther, S.A.; Mangion, J.; Russell, P.; Seal, S.; Barfoot, R.; Ponder, B.A.; Stratton, M.R.; Easton, D. Variation of risks of breast and ovarian cancer associated with different germline mutations of the BRCA2 gene. Nat. Genet. 1997, 15, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Easton, D. Variation in Cancer Risks, by Mutation Position, in BRCA2 Mutation Carriers. Am. J. Hum. Genet. 2001, 68, 410–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubinski, J.; Phelan, C.M.; Ghadirian, P.; Lynch, H.T.; Garber, J.; Weber, B.; Tung, N.; Horsman, D.; Isaacs, C.; Monteiro, A.N.A.; et al. Cancer variation associated with the position of the mutation in the BRCA2 gene. Fam. Cancer 2004, 3, 1–10. [Google Scholar] [CrossRef]
- Labidi-Galy, S.I.; Olivier, T.; Rodrigues, M.; Ferraioli, D.; Derbel, O.; Bodmer, A.; Petignat, P.; Rak, B.; Chopin, N.; Tredan, O.; et al. Location of Mutation in BRCA2 Gene and Survival in Patients with Ovarian Cancer. Clin. Cancer Res. 2018, 24, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Alsop, K.; Fereday, S.; Meldrum, C.; DeFazio, A.; Emmanuel, C.; George, J.; Dobrovic, A.; Birrer, M.J.; Webb, P.M.; Stewart, C.; et al. BRCA Mutation Frequency and Patterns of Treatment Response in BRCA Mutation–Positive Women with Ovarian Cancer: A Report From the Australian Ovarian Cancer Study Group. J. Clin. Oncol. 2012, 30, 2654–2663. [Google Scholar] [CrossRef] [Green Version]
- Bayraktar, S.; Jackson, M.; Gutierrez-Barrera, A.M.; Liu, D.; Meric-Bernstam, F.; Brandt, A.; Woodson, A.; Litton, J.; Lu, K.H.; Valero, V.; et al. Genotype-Phenotype Correlations by Ethnicity and Mutation Location in BRCA Mutation Carriers. Breast J. 2015, 21, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Ghezelayagh, T.S.; Pennington, K.P.; Norquist, B.M.; Khasnavis, N.; Radke, M.R.; Kilgore, M.R.; Garcia, R.L.; Lee, M.; Katz, R.; Leslie, K.K.; et al. Characterizing TP53 mutations in ovarian carcinomas with and without concurrent BRCA1 or BRCA2 mutations. Gynecol. Oncol. 2021, 160, 786–792. [Google Scholar] [CrossRef]
- DiSilvestro, P.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Efficacy of Maintenance Olaparib for Patients with Newly Diagnosed Advanced Ovarian Cancer with a BRCA Mutation: Subgroup Analysis Findings From the SOLO1 Trial. J. Clin. Oncol. 2020, 38, 3528–3537. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Ceccaldi, R.; Shapiro, G.I.; D’Andrea, A.D. Homologous Recombination Deficiency: Exploiting the Fundamental Vulnerability of Ovarian Cancer. Cancer Discov. 2015, 5, 1137–1154. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas Research Network. Undefined Integrated Genomic Analyses of Ovarian Carcinoma. 2011. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3163504/ (accessed on 12 September 2021).
- Coleman, R.L.; Monk, B.J.; Sood, A.K.; Herzog, T.J. Latest research and treatment of advanced-stage epithelial ovarian cancer. Nat. Rev. Clin. Oncol. 2013, 10, 211–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bookman, M.A.; Tyczynski, J.E.; Espirito, J.L.; Wilson, T.W.; Fernandes, A.W. Impact of primary platinum-free interval and BRCA1/2 mutation status on treatment and survival in patients with recurrent ovarian cancer. Gynecol. Oncol. 2017, 146, 58–63. [Google Scholar] [CrossRef]
- Gallotta, V.; Conte, C.; D’Indinosante, M.; Capoluongo, E.; Minucci, A.; De Rose, A.M.; Ardito, F.; Giuliante, F.; Di Giorgio, A.; Zannoni, G.F.; et al. Prognostic factors value of germline and somatic brca in patients undergoing surgery for recurrent ovarian cancer with liver metastases. Eur. J. Surg. Oncol. (EJSO) 2019, 45, 2096–2102. [Google Scholar] [CrossRef] [PubMed]
- Gallotta, V.; Bruno, M.; Conte, C.; Giudice, M.; Davià, F.; Moro, F.; Zannoni, G.; Fagotti, A.; De Bonis, M.; Capoluongo, E.; et al. Salvage lymphadenectomy in recurrent ovarian cancer patients: Analysis of clinical outcome and BRCA1/2 gene mutational status. Eur. J. Surg. Oncol. (EJSO) 2020, 46, 1327–1333. [Google Scholar] [CrossRef]
- Javle, M.; Curtin, N.J. The role of PARP in DNA repair and its therapeutic exploitation. Br. J. Cancer 2011, 105, 1114–1122. [Google Scholar] [CrossRef] [Green Version]
- Drost, R.; Bouwman, P.; Rottenberg, S.; Boon, U.; Schut, E.; Klarenbeek, S.; Klijn, C.; van der Heijden, I.; van der Gulden, H.; Wientjens, E.; et al. BRCA1 RING Function Is Essential for Tumor Suppression but Dispensable for Therapy Resistance. Cancer Cell 2011, 20, 797–809. [Google Scholar] [CrossRef] [Green Version]
- Jonsson, P.; Bandlamudi, C.; Cheng, M.L.; Srinivasan, P.; Chavan, S.S.; Friedman, N.D.; Rosen, E.Y.; Richards, A.L.; Bouvier, N.; Selcuklu, S.D.; et al. Tumour lineage shapes BRCA-mediated phenotypes. Nature 2019, 571, 576–579. [Google Scholar] [CrossRef]
- Eoh, K.J.; Kim, H.M.; Lee, J.-Y.; Kim, S.; Kim, S.W.; Kim, Y.T.; Nam, E.J. Mutation landscape of germline and somatic BRCA1/2 in patients with high-grade serous ovarian cancer. BMC Cancer 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Apostolou, P.; Fostira, F.; Kouroussis, C.; Kalfakakou, D.; Delimitsou, A.; Agelaki, S.; Androulakis, N.; Christodoulou, C.; Kalbakis, K.; Kalykaki, A.; et al. BRCA1 and BRCA2 germline testing in Cretan isolates reveals novel and strong founder effects. Int. J. Cancer 2020, 147, 1334–1342. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | ||
|---|---|---|
| Median (25th–75th Perc) | Missing (%) | |
| Age | 54.2 (45.8–62.1) | 0 (0) |
| n | (%) | |
| Stage | ||
| II | 8 | 15.7% |
| IIIA/IIIB | 4 | 7.9% |
| IIIC | 29 | 56.9% |
| IV | 10 | 19.6% |
| Debulking Surgery | ||
| Primary | 31 | 60.8% |
| Interval | 20 | 39.2% |
| Surgical Outcome | ||
| Complete | 45 | 88.2% |
| Optimal/Suboptimal | 6 | 11.8% |
| Mutated Gene | ||
| BRCA1 | 35 | 68.6% |
| BRCA2 | 16 | 31.4% |
| Type of mutation | ||
| Deletion | 26 | 51.0% |
| Frameshift | 4 | 7.8% |
| Insertion | 4 | 7.8% |
| Missense | 17 | 33.3% |
| Affected region | ||
| RING domain | 3 | 5.9% |
| BRCA1 exons 11–13 | 16 | 31.4% |
| BRCT domain | 16 | 31.4% |
| RAD51 binding domain | 11 | 21.6% |
| DNA binding domain | 5 | 9.8% |
| Bevacizumab administration | ||
| No | 31 | 60.8% |
| Yes | 20 | 39.2% |
| PARP inhibitor administration | ||
| No | 17 | 33.3% |
| Yes | 34 | 66.7% |
| PFS | OS | |||||
|---|---|---|---|---|---|---|
| Median | 95% CI | p-Value * | Median | 95% CI | p-Value | |
| Age | 0.867 | 0.467 | ||||
| ≤65 | 23.9 | 18.4–29.3 | 92.9 | 59.8–126.1 | ||
| >65 | 23.0 | 20.3–25.7 | NR | NR | ||
| Stage | 0.155 | 0.173 | ||||
| II/IIIA/IIIB | 45.8 | NR | NR | NR | ||
| IIIC/IV | 21.7 | 13.9–29.5 | 81.9 | 63.6–100.2 | ||
| Mutant gene | 0.828 | 0.405 | ||||
| BRCA1 | 23.0 | 19.1–26.9 | 81.9 | - | ||
| BRCA2 | 23.8 | 16.3–31.3 | 92.9 | 32.9–153.7 | ||
| Surgical outcome | <0.001 | 0.028 | ||||
| Complete | 24.9 | 18.4–31.4 | 92.9 | 69.3–116.7 | ||
| Optimal/Suboptimal | 11.1 | 2.5–19.8 | 45.2 | 17.4–72.8 | ||
| Surgical outcome | 0.459 | 0.178 | ||||
| Primary | 23.0 | 12.1–33.9 | NR | NR | ||
| Interval | 23.9 | 19.9–27.8 | 81.9 | 36.7–127.1 | ||
| Type of mutation | 0.369 | 0.187 | ||||
| Deletion | 19.7 | 13.4–26.1 | 92.9 | 40.8–145.2 | ||
| Frameshift | 30.1 | 21.1–39.1 | NR | NR | ||
| Missense | 23.0 | 18.1–27.9 | NR | NR | ||
| Affected domain | 0.339 | 0.882 | ||||
| RING domain | 15.6 | - | 77.1 | 10.9-NR | ||
| BRCA1 exons 11–13 | 21.8 | 18.1–25.5 | 81.9 | - | ||
| BRCT domain | 28.7 | 19.9–37.6 | NR | NR | ||
| DNA Binding domain | 19.7 | 12.9–26.6 | NR | NR | ||
| RAD51 binding domain | 33.9 | 16.0–51.9 | 92.9 | 25.9–160.1 | ||
| Bevacizumab | 0.707 | 0.214 | ||||
| No | 23.9 | 19.6–28.2 | NR | NR | ||
| Yes | 21.8 | 6.6–36.9 | 81.9 | 69.8–116.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liontos, M.; Zografos, E.; Zoumpourlis, P.; Andrikopoulou, A.; Svarna, A.; Fiste, O.; Kunadis, E.; Papatheodoridi, A.M.; Kaparelou, M.; Koutsoukos, K.; et al. BRCA1/2 Mutation Types Do Not Affect Prognosis in Ovarian Cancer Patients. Curr. Oncol. 2021, 28, 4446-4456. https://doi.org/10.3390/curroncol28060377
Liontos M, Zografos E, Zoumpourlis P, Andrikopoulou A, Svarna A, Fiste O, Kunadis E, Papatheodoridi AM, Kaparelou M, Koutsoukos K, et al. BRCA1/2 Mutation Types Do Not Affect Prognosis in Ovarian Cancer Patients. Current Oncology. 2021; 28(6):4446-4456. https://doi.org/10.3390/curroncol28060377
Chicago/Turabian StyleLiontos, Michalis, Eleni Zografos, Panagiotis Zoumpourlis, Angeliki Andrikopoulou, Anna Svarna, Oraianthi Fiste, Elena Kunadis, Alkistis Maria Papatheodoridi, Maria Kaparelou, Konstantinos Koutsoukos, and et al. 2021. "BRCA1/2 Mutation Types Do Not Affect Prognosis in Ovarian Cancer Patients" Current Oncology 28, no. 6: 4446-4456. https://doi.org/10.3390/curroncol28060377
APA StyleLiontos, M., Zografos, E., Zoumpourlis, P., Andrikopoulou, A., Svarna, A., Fiste, O., Kunadis, E., Papatheodoridi, A. M., Kaparelou, M., Koutsoukos, K., Thomakos, N., Haidopoulos, D., Rodolakis, A., Dimopoulos, M.-A., & Zagouri, F. (2021). BRCA1/2 Mutation Types Do Not Affect Prognosis in Ovarian Cancer Patients. Current Oncology, 28(6), 4446-4456. https://doi.org/10.3390/curroncol28060377