Efficacy of Different Interventions to Reduce Pre- or Perioperative Blood Transfusion Rate in Patients with Colorectal Cancer: A Network Meta-Analysis of Randomized Controlled Trials


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. General Guidelines Applied in This Study
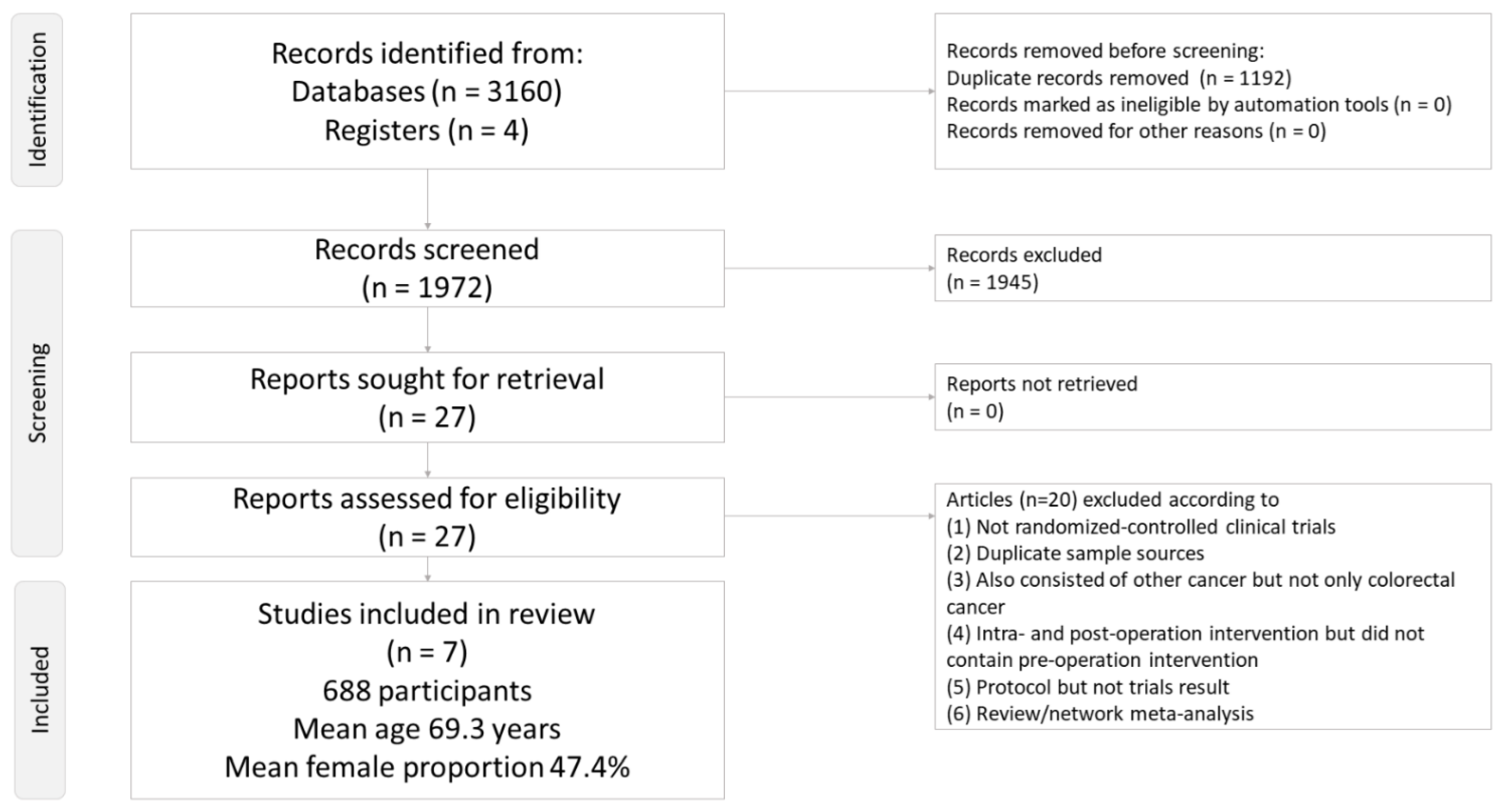
2.2. Search Strategy and Selection Criteria
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Primary Outcome
2.6. Secondary Outcomes
2.7. Acceptability
2.8. Cochrane Risk of Bias Tool and Quality of Evidence Evaluation
2.9. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
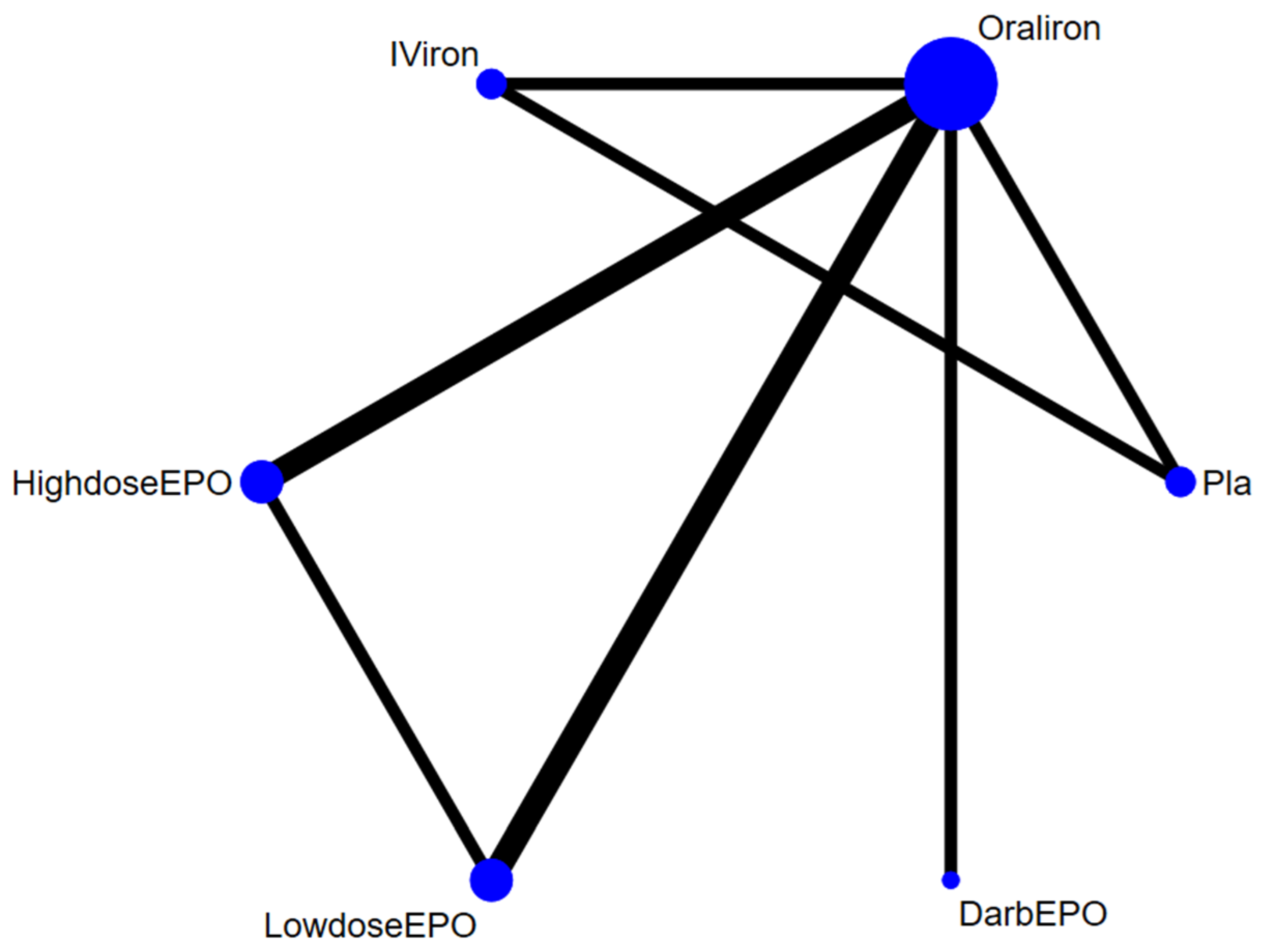
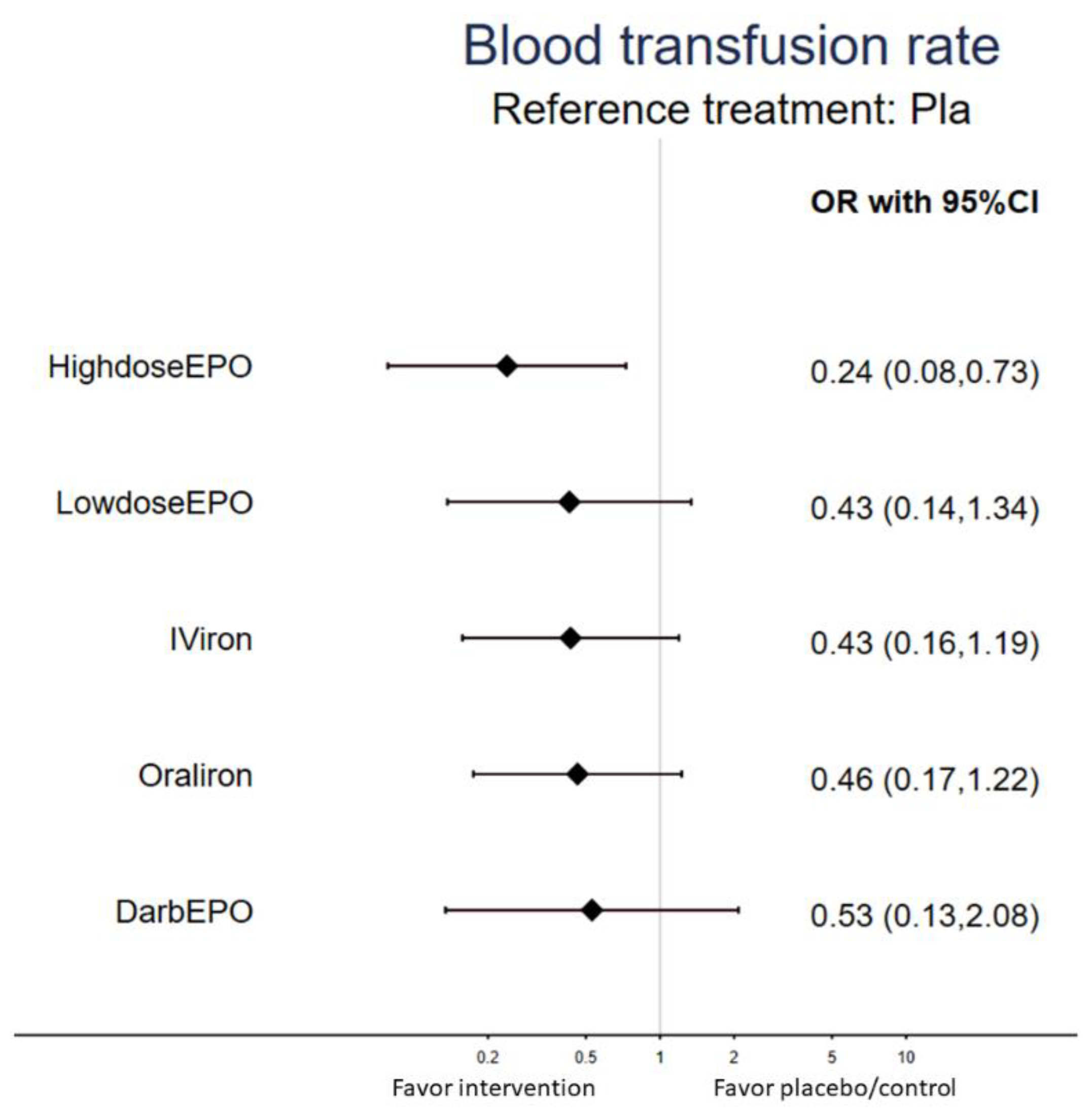
3.2. Primary Outcome: Rate of Blood Transfusion
3.3. Secondary Outcome: Changes in Hemoglobin Level
3.4. Secondary Outcome: Changes in Ferritin Level
3.5. Secondary Outcome: Changes in the Amount of Blood Transfused
3.6. Association between Individual Interventions and Acceptability with Respect to Dropout Rates
3.7. Risk of Bias, Publication Bias, Inconsistency, and GRADE Ratings
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Dickson, E.A.; Keeler, B.D.; Ng, O.; Kumar, A.; Brookes, M.J.; Acheson, A.G.; IVICA Trial Group. Preoperative intravenous iron therapy and survival after colorectal cancer surgery: Long-term results from the IVICA randomised controlled trial. Colorectal Dis. 2020, 22, 2018–2027. [Google Scholar] [CrossRef]
- Leichtle, S.W.; Mouawad, N.J.; Lampman, R.; Singal, B.; Cleary, R.K. Does preoperative anemia adversely affect colon and rectal surgery outcomes? J. Am. Coll. Surg. 2011, 212, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Vamvakas, E.C.; Blajchman, M.A. Deleterious clinical effects of transfusion-associated immunomodulation: Fact or fiction? Blood 2001, 97, 1180–1195. [Google Scholar] [CrossRef]
- Acheson, A.G.; Brookes, M.J.; Spahn, D.R. Effects of allogeneic red blood cell transfusions on clinical outcomes in patients undergoing colorectal cancer surgery: A systematic review and meta-analysis. Ann. Surg. 2012, 256, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Pescatori, M. Perioperative blood transfusions for the recurrence of colorectal cancer. Cochrane Database Syst. Rev. 2006, CD005033. [Google Scholar] [CrossRef] [PubMed]
- Christodoulakis, M.; Tsiftsis, D.D.; Hellenic Surgical Oncology Perioperative, EPO Study Group. Preoperative epoetin alfa in colorectal surgery: A randomized, controlled study. Ann. Surg. Oncol. 2005, 12, 718–725. [Google Scholar] [CrossRef]
- Heiss, M.M.; Mempel, W.; Jauch, K.W.; Delanoff, C.; Mayer, G.; Mempel, M.; Eissner, H.J.; Schildberg, F.W. Beneficial effect of autologous blood transfusion on infectious complications after colorectal cancer surgery. Lancet 1993, 342, 1328–1333. [Google Scholar] [CrossRef]
- Van Papendrecht, M.A.H.; Hop, W.; Langenhorst, B.L.; Kothe, F.C.; Marquet, R.L.; Jeekel, J. Feasibility of a predeposit autologous blood donation program in colorectal cancer patients: Results from a randomized clinical study. Vox Sang. 1992, 62, 102–107. [Google Scholar] [CrossRef]
- Lidder, P.G.; Sanders, G.; Whitehead, E.; Douie, W.J.; Mellor, N.; Lewis, S.J.; Hosie, K.B. Pre-operative oral iron supplementation reduces blood transfusion in colorectal surgery—A prospective, randomised, controlled trial. Ann. R. Coll. Surg. Engl. 2007, 89, 418–421. [Google Scholar] [CrossRef]
- Edwards, T.J.; Noble, E.J.; Durran, A.; Mellor, N.; Hosie, K.B. Randomized clinical trial of preoperative intravenous iron sucrose to reduce blood transfusion in anaemic patients after colorectal cancer surgery. Br. J. Surg. 2009, 96, 1122–1128. [Google Scholar] [CrossRef]
- Ng, O.; Keeler, B.D.; Mishra, A.; Simpson, A.; Neal, K.; Brookes, M.J.; Acheson, A.G. Iron therapy for pre-operative anaemia. Cochrane Database Syst. Rev. 2015, CD011588. [Google Scholar] [CrossRef]
- Borstlap, W.A.; Stellingwerf, M.E.; Moolla, Z.; Musters, G.D.; Buskens, C.J.; Tanis, P.J.; Bemelman, W.A. Iron therapy for the treatment of preoperative anaemia in patients with colorectal carcinoma: A systematic review. Colorectal Dis. 2015, 17, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Goodnough, L.T.; Skikne, B.; Brugnara, C. Erythropoietin, iron, and erythropoiesis. Blood 2000, 96, 823–833. [Google Scholar] [CrossRef]
- Devon, K.M.; McLeod, R.S. Pre and peri-operative erythropoietin for reducing allogeneic blood transfusions in colorectal cancer surgery. Cochrane Database Syst. Rev. 2009, CD007148. [Google Scholar] [CrossRef]
- Heiss, M.M.; Tarabichi, A.; Delanoff, C.; Allgayer, H.; Jauch, K.W.; Hernandez-Richter, T.; Mempel, W.; Beck, K.G.; Schildberg, F.W.; Messmer, K. Perisurgical erythropoietin application in anemic patients with colorectal cancer: A double-blind randomized study. Surgery 1996, 119, 523–527. [Google Scholar] [CrossRef]
- Norager, C.B.; Jensen, M.B.; Madsen, M.R.; Qvist, N.; Laurberg, S. Effect of darbepoetin alfa on physical function in patients undergoing surgery for colorectal cancer. A randomized, double-blind, placebo-controlled study. Oncology 2006, 71, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Qvist, N.; Boesby, S.; Wolff, B.; Hansen, C.P. Recombinant human erythropoietin and hemoglobin concentration at operation and during the postoperative period: Reduced need for blood transfusions in patients undergoing colorectal surgery–prospective double-blind placebo-controlled study. World J. Surg. 1999, 23, 30–35. [Google Scholar] [CrossRef]
- Higgins, J.P.; Welton, N.J. Network meta-analysis: A norm for comparative effectiveness? Lancet 2015, 386, 628–630. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Chiu, Y.H.; Chang, K.V.; Chen, I.J.; Wu, W.T.; Ozcakar, L. Utility of sonoelastography for the evaluation of rotator cuff tendon and pertinent disorders: A systematic review and meta-analysis. Eur. Radiol. 2020, 30, 6663–6672. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.P.; Chang, K.V.; Huang, Y.K.; Wu, W.T.; Ozcakar, L. Regenerative Injections Including 5% Dextrose and Platelet-Rich Plasma for the Treatment of Carpal Tunnel Syndrome: A Systematic Review and Network Meta-Analysis. Pharmaceuticals 2020, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.J.; Chang, K.V.; Lou, Y.M.; Wu, W.T.; Ozcakar, L. Can ultrasound imaging be used for the diagnosis of carpal tunnel syndrome in diabetic patients? A systemic review and network meta-analysis. J. Neurol. 2020, 267, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. Lancet 2018, 16, 420–429. [Google Scholar] [CrossRef]
- Huhn, M.; Nikolakopoulou, A.; Schneider-Thoma, J.; Krause, M.; Samara, M.; Peter, N.; Arndt, T.; Backers, L.; Rothe, P.; Cipriani, A.; et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: A systematic review and network meta-analysis. Lancet 2019, 394, 939–951. [Google Scholar] [CrossRef]
- Hallet, J.; Hanif, A.; Callum, J.; Pronina, I.; Wallace, D.; Yohanathan, L.; McLeod, R.; Coburn, N. The impact of perioperative iron on the use of red blood cell transfusions in gastrointestinal surgery: A systematic review and meta-analysis. Transfus. Med. Rev. 2014, 28, 205–211. [Google Scholar] [CrossRef]
- Zhou, X.; Teng, T.; Zhang, Y.; Del Giovane, C.; Furukawa, T.A.; Weisz, J.R.; Li, X.; Cuijpers, P.; Coghill, D.; Xiang, Y.; et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: A systematic review and network meta-analysis. Lancet Psychiatry 2020, 7, 581–601. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. 2009. Available online: https://training.cochrane.org/handbook/archive/v5.0.2/ (accessed on 30 September 2009).
- Brockhaus, A.C.; Bender, R.; Skipka, G. The Peto odds ratio viewed as a new effect measure. Stat. Med. 2014, 33, 4861–4874. [Google Scholar] [CrossRef]
- Cheng, J.; Pullenayegum, E.; Marshall, J.K.; Iorio, A.; Thabane, L. Impact of including or excluding both-armed zero-event studies on using standard meta-analysis methods for rare event outcome: A simulation study. BMJ Open 2016, 6, e010983. [Google Scholar] [CrossRef] [PubMed]
- White, I.R. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar] [CrossRef]
- Lu, G.; Ades, A.E. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef]
- Higgins, J.P.; Del Giovane, C.; Chaimani, A.; Caldwell, D.M.; Salanti, G. Evaluating the Quality of Evidence from a Network Meta-Analysis. Value Health 2014, 17, A324. [Google Scholar] [CrossRef]
- Puhan, M.A.; Schunemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef]
- Keeler, B.D.; Dickson, E.A.; Simpson, J.A.; Ng, O.; Padmanabhan, H.; Brookes, M.J.; Acheson, A.G.; Group, I.T. The impact of pre-operative intravenous iron on quality of life after colorectal cancer surgery: Outcomes from the intravenous iron in colorectal cancer-associated anaemia (IVICA) trial. Anaesthesia 2019, 74, 714–725. [Google Scholar] [CrossRef]
- Keeler, B.D.; Simpson, J.A.; Ng, O.; Padmanabhan, H.; Brookes, M.J.; Acheson, A.G.; Group, I.T. Randomized clinical trial of preoperative oral versus intravenous iron in anaemic patients with colorectal cancer. Br. J. Surg. 2017, 104, 214–221. [Google Scholar] [CrossRef]
- Qvist, N.; Boesby, S.; Wolff, B.; Hansen, C.P. Perioperative administration of recombinant human erythropoietin in colorectal cancer surgery. A prospective, randomized, double-blind placebo controlled study. Ugeskr. Laeger 2000, 162, 355–358. [Google Scholar]
- Kettelhack, C.; Hones, C.; Messinger, D.; Schlag, P.M. Randomized multicentre trial of the influence of recombinant human erythropoietin on intraoperative and postoperative transfusion need in anaemic patients undergoing right hemicolectomy for carcinoma. Br. J. Surg. 1998, 85, 63–67. [Google Scholar] [CrossRef]
- Ludwig, H.; Muldur, E.; Endler, G.; Hubl, W. Prevalence of iron deficiency across different tumors and its association with poor performance status, disease status and anemia. Ann. Oncol. 2013, 24, 1886–1892. [Google Scholar] [CrossRef]
- Braga, M.; Gianotti, L.; Vignali, A.; Gentilini, O.; Servida, P.; Bordignon, C.; Di Carlo, V. Evaluation of recombinant human erythropoietin to facilitate autologous blood donation before surgery in anaemic patients with cancer of the gastrointestinal tract. Br. J. Surg. 1995, 82, 1637–1640. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, K.A.; Qvist, N.; Winther, K.; Boesby, S. Haemostatic aspects of recombinant human erythropoietin in colorectal surgery. Eur. J. Surg. 1998, 164, 211–215. [Google Scholar] [CrossRef]
- Sowade, B.; Sowade, O.; Mocks, J.; Franke, W.; Warnke, H. The safety of treatment with recombinant human erythropoietin in clinical use: A review of controlled studies. Int. J. Mol. Med. 1998, 1, 303–314. [Google Scholar] [CrossRef]
- Rupertus, K.; Sperling, J.; Corsten, M.; Scheuer, C.; Nickels, R.M.; Schilling, M.K.; Menger, M.D.; Kollmar, O. Darbepoetin-alpha enhances hepatectomy-associated stimulation of colorectal liver metastatic growth. Ann. Surg. 2010, 252, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Henke, M.; Laszig, R.; Rube, C.; Schafer, U.; Haase, K.D.; Schilcher, B.; Mose, S.; Beer, K.T.; Burger, U.; Dougherty, C.; et al. Erythropoietin to treat head and neck cancer patients with anaemia undergoing radiotherapy: Randomised, double-blind, placebo-controlled trial. Lancet 2003, 362, 1255–1260. [Google Scholar] [CrossRef]
- Rocha, J.; Eduardo-Figueira, M.; Barateiro, A.; Fernandes, A.; Brites, D.; Pinto, R.; Freitas, M.; Fernandes, E.; Mota-Filipe, H.; Sepodes, B. Erythropoietin reduces acute lung injury and multiple organ failure/dysfunction associated to a scald-burn inflammatory injury in the rat. Inflammation 2015, 38, 312–326. [Google Scholar] [CrossRef]
- Jungers, P.; Choukroun, G.; Oualim, Z.; Robino, C.; Nguyen, A.T.; Man, N.K. Beneficial influence of recombinant human erythropoietin therapy on the rate of progression of chronic renal failure in predialysis patients. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2001, 16, 307–312. [Google Scholar] [CrossRef][Green Version]
- Iconomou, G.; Koutras, A.; Rigopoulos, A.; Vagenakis, A.G.; Kalofonos, H.P. Effect of recombinant human erythropoietin on quality of life in cancer patients receiving chemotherapy: Results of a randomized, controlled trial. J. Pain Symptom Manag. 2003, 25, 512–518. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| HighdoseEPO | 0.61 (0.31, 1.22) | * 0.50 (0.29, 0.86) | |||
| 0.56 (0.30, 1.05) | LowdoseEPO | 0.96 (0.52, 1.77) | |||
| 0.55 (0.21, 1.46) | 0.99 (0.36, 2.70) | IViron | 0.75 (0.30, 1.85) | 0.72 (0.19, 2.82) | |
| * 0.52 (0.30, 0.89) | 0.93 (0.51, 1.68) | 0.94 (0.42, 2.11) | Oraliron | 0.87 (0.33, 2.29) | 0.31 (0.09, 1.03) |
| 0.45 (0.15, 1.36) | 0.81 (0.26, 2.51) | 0.82 (0.23, 2.89) | 0.87 (0.33, 2.29) | DarbEPO | |
| * 0.24 (0.08, 0.73) | 0.43 (0.14, 1.34) | 0.43 (0.16, 1.19) | 0.46 (0.17, 1.22) | 0.53 (0.13, 2.08) | Pla |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, C.-M.; Chen, J.-J.; Zeng, B.-Y.; Zeng, B.-S.; Chen, Y.-W.; Suen, M.-W.; Wu, M.-K.; Tseng, P.-T. Efficacy of Different Interventions to Reduce Pre- or Perioperative Blood Transfusion Rate in Patients with Colorectal Cancer: A Network Meta-Analysis of Randomized Controlled Trials. Curr. Oncol. 2021, 28, 3214-3226. https://doi.org/10.3390/curroncol28040279
Hung C-M, Chen J-J, Zeng B-Y, Zeng B-S, Chen Y-W, Suen M-W, Wu M-K, Tseng P-T. Efficacy of Different Interventions to Reduce Pre- or Perioperative Blood Transfusion Rate in Patients with Colorectal Cancer: A Network Meta-Analysis of Randomized Controlled Trials. Current Oncology. 2021; 28(4):3214-3226. https://doi.org/10.3390/curroncol28040279
Chicago/Turabian StyleHung, Chao-Ming, Jiann-Jy Chen, Bing-Yan Zeng, Bing-Syuan Zeng, Yen-Wen Chen, Mein-Woei Suen, Ming-Kung Wu, and Ping-Tao Tseng. 2021. "Efficacy of Different Interventions to Reduce Pre- or Perioperative Blood Transfusion Rate in Patients with Colorectal Cancer: A Network Meta-Analysis of Randomized Controlled Trials" Current Oncology 28, no. 4: 3214-3226. https://doi.org/10.3390/curroncol28040279
APA StyleHung, C.-M., Chen, J.-J., Zeng, B.-Y., Zeng, B.-S., Chen, Y.-W., Suen, M.-W., Wu, M.-K., & Tseng, P.-T. (2021). Efficacy of Different Interventions to Reduce Pre- or Perioperative Blood Transfusion Rate in Patients with Colorectal Cancer: A Network Meta-Analysis of Randomized Controlled Trials. Current Oncology, 28(4), 3214-3226. https://doi.org/10.3390/curroncol28040279