Multitumor Case Series of Germline BRCA1, BRCA2 and CHEK2-Mutated Patients Responding Favorably on Immune Checkpoint Inhibitors

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Genetic Testing
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Included Patients
3.2. Genetic Testing and Outcome on ICPI Treatment
4. Case Descriptions
4.1. Patient 1: BRCA1 (c.212+3A>G, p.?): Renal Cell Carcinoma
4.2. Patient 2: BRCA2 (c.6644_6647del, p.Ty2215Serfs*13): Squamous Cell Carcinoma of Unknown Origin
4.3. Patient 3: CHEK2 (c. 1100del, p.Thr367Metfs*15): Malignant Melanoma
4.4. Patient 4: BRCA2 (c.516+1G>A, p.?): Malignant Melanoma
4.5. Patient 5: BRCA1 (c.5186T>A, p.Leu1729Gln): Malignant Melanoma
4.6. Patient 6: BRCA2 (c.4936_4939del, p.Glu1646Glnfs*23): Transitional Cell Carcinoma
4.7. Patient 7: BRCA1 (c.212+3A>G, p.?): Transitional Cell Carcinoma
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Forschner, A.; Battke, F.; Hadaschik, D.; Schulze, M.; Weißgraeber, S.; Han, C.T.; Kopp, M.; Frick, M.; Klumpp, B.; Tietze, N.; et al. Tumor mutation burden and circulating tumor DNA in combined CTLA-4 and PD-1 antibody therapy in metastatic melanoma—Results of a prospective biomarker study. J. Immunother. Cancer 2019, 7, 180. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef]
- Strickland, K.C.; Howitt, B.E.; Shukla, S.A.; Rodig, S.; Ritterhouse, L.L.; Liu, J.F.; Garber, J.E.; Chowdhury, D.; Wu, C.J.; D’Andrea, A.D.; et al. Association and prognostic significance of BRCA1/2-mutation status with neoantigen load, number of tumor-infiltrating lymphocytes and expression of PD-1/PD-L1 in high grade serous ovarian cancer. Oncotarget 2016, 7, 13587–13598. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Lu, L.Y.; Yu, X. The role of BRCA1 in DNA damage response. Protein Cell 2010, 1, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.; Makarov, V.; Merghoub, T.; Yuan, J.; Zaretsky, J.M.; Desrichard, A.; Walsh, L.A.; Postow, M.A.; Wong, P.; Ho, T.S.; et al. Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma. N. Engl. J. Med. 2014, 371, 2189–2199. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Wang, Z.; Zhao, J.; Wang, G.; Zhang, F.; Zhang, Z.; Zhang, F.; Zhang, Y.; Dong, H.; Zhao, X.; Duan, J.; et al. Comutations in DNA damage response pathways serve as potential biomarkers for immune checkpoint blockade. Cancer Res. 2018, 78, 6486–6496. [Google Scholar] [CrossRef] [Green Version]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- Mei, P.; Freitag, C.E.; Wei, L.; Zhang, Y.; Parwani, A.V.; Li, Z. High tumor mutation burden is associated with DNA damage repair gene mutation in breast carcinomas. Diagn. Pathol. 2020, 15, 50. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.R.; He, Y.; Hong, T.S.; Corcoran, R.B.; Clark, J.W.; Ryan, D.P.; Zou, L.; Ting, D.T.; Catenacci, D.V.; Chao, J.; et al. Analysis of DNA Damage Response Gene Alterations and Tumor Mutational Burden Across 17,486 Tubular Gastrointestinal Carcinomas: Implications for Therapy. Oncologist 2019, 24, 1340–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, Y.K.; Anker, J.F.; Bais, P.; Namburi, S.; Giles, F.J.; Chuang, J.H. Mutations in DNA repair genes are associated with increased neo-antigen load and activated T cell infiltration in lung adenocarcinoma. Oncotarget 2018, 9, 7949–7960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatzinikolaou, G.; Karakasilioti, I.; Garinis, G.A. DNA damage and innate immunity: Links and trade-offs. Trends Immunol. 2014, 35, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Barber, G.N. STING: Infection, inflammation and cancer. Nat. Rev. Immunol. 2015, 15, 760–770. [Google Scholar] [CrossRef] [Green Version]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; de Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/ mismatch repair–deficient cancer: Results from the phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef] [Green Version]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [Green Version]
- Cupp, M.A.; Cariolou, M.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A.J. Neutrophil to lymphocyte ratio and cancer prognosis: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18. [Google Scholar] [CrossRef]
- Roussel, E.; Kinget, L.; Verbiest, A.; Debruyne, P.R.; Baldewijns, M.; Van Poppel, H.; Albersen, M.; Beuselinck, B. C-reactive protein and neutrophil-lymphocyte ratio are prognostic in metastatic clear-cell renal cell carcinoma patients treated with nivolumab. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 239.e17–239.e25. [Google Scholar] [CrossRef]
- Cohen, J.T.; Miner, T.J.; Vezeridis, M.P. Is the neutrophil-to-lymphocyte ratio a useful prognostic indicator in melanoma patients? Melanoma Manag. 2020, 7, MMT47. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Beulque, Y.; Deleu, A.L.; Punie, K.; De Wever, L.; Baldewijns, M.; Caruso, S.; Couchy, G.; Zucman-Rossi, J.; Beuselinck, B. Immunogenomics of Metastatic Clear-Cell Renal Cell Carcinoma: Remarkable Response to Nivolumab in a Patient With a Pathogenic Germ Line BRCA1 Mutation. Clin. Genitourin. Cancer 2019, 17, e909–e912. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Van der Heijden, M.S.; Loriot, Y.; Durán, I.; Ravaud, A.; Retz, M.; Vogelzang, N.J.; Nelson, B.; Wang, J.; Shen, X.; Powles, T. Atezolizumab Versus Chemotherapy in Patients with Platinum-treated Locally Advanced or Metastatic Urothelial Carcinoma: A Long-term Overall Survival and Safety Update from the Phase 3 IMvigor211 Clinical Trial. Eur. Urol. 2021, 80, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Csőszi, T.; Özgüroğlu, M.; Matsubara, N.; Géczi, L.; Cheng, S.Y.S.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Morales Barrera, R.; et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef]
- Corrales, L.; Gajewski, T.F. Molecular pathways: Targeting the Stimulator of Interferon Genes (STING) in the immunotherapy of cancer. Clin. Cancer Res. 2015, 21, 4774–4779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, W.; Zhang, Q.; Wang, R.; Li, Y.; Sun, Y.; Yang, L. Targeting DNA Damage Repair for Immune Checkpoint Inhibition: Mechanisms and Potential Clinical Applications. Front. Oncol. 2021, 11, 648687. [Google Scholar] [CrossRef] [PubMed]
- Samstein, R.M.; Lee, C.H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Li, M. Evaluation of BRCA1 and BRCA2 as Indicators of Response to Immune Checkpoint Inhibitors. JAMA Netw. Open 2021, 4. [Google Scholar] [CrossRef] [PubMed]
- Teo, M.Y.; Seier, K.; Ostrovnaya, I.; Regazzi, A.M.; Kania, B.E.; Moran, M.M.; Cipolla, C.K.; Bluth, M.J.; Chaim, J.; Al-Ahmadie, H.; et al. Alterations in DNA Damage Response and Repair Genes as Potential Marker of Clinical Benefit From PD-1/PD-L1 Blockade in Advanced Urothelial Cancers. J. Clin. Oncol. 2018, 36, 1685–1694. [Google Scholar] [CrossRef]
- Joshi, M.; Grivas, P.; Mortazavi, A.; Monk, P.; Clinton, S.K.; Sue-Ann Woo, M.; Holder, S.L.; Drabick, J.J.; Yin, M. Alterations of DNA damage response genes correlate with response and overall survival in anti-PD-1/PD-L1-treated advanced urothelial cancer. Cancer Med. 2020, 9, 9365–9372. [Google Scholar] [CrossRef]
- Powles, T.B.; Loriot, Y.; Bellmunt, J.; Sternberg, C.N.; Sridhar, S.; Petrylak, D.P.; Tambaro, R.; Dourthe, L.M.; Alvarez-Fernandez, C.; Aarts, M.; et al. 699O Avelumab first-line (1L) maintenance + best supportive care (BSC) vs BSC alone for advanced urothelial carcinoma (UC): Association between clinical outcomes and exploratory biomarkers. Ann. Oncol. 2020, 31, S552–S553. [Google Scholar] [CrossRef]
- Labriola, M.K.; Zhu, J.; Gupta, R.; McCall, S.; Jackson, J.; Kong, E.F.; White, J.R.; Cerqueira, G.; Gerding, K.; Simmons, J.K.; et al. Characterization of tumor mutation burden, PD-L1 and DNA repair genes to assess relationship to immune checkpoint inhibitors response in metastatic renal cell carcinoma. J. Immunother. Cancer 2020, 8, 319. [Google Scholar] [CrossRef] [Green Version]
- Ged, Y.; Chaim, J.L.; DInatale, R.G.; Knezevic, A.; Kotecha, R.R.; Carlo, M.I.; Lee, C.H.; Foster, A.; Feldman, D.R.; Teo, M.Y.; et al. DNA damage repair pathway alterations in metastatic clear cell renal cell carcinoma and implications on systemic therapy. J. Immunother. Cancer 2020, 8, 230. [Google Scholar] [CrossRef] [PubMed]
- Hugo, W.; Zaretsky, J.M.; Sun, L.; Song, C.; Moreno, B.H.; Hu-Lieskovan, S.; Berent-Maoz, B.; Pang, J.; Chmielowski, B.; Cherry, G.; et al. Genomic and Transcriptomic Features of Response to Anti-PD-1 Therapy in Metastatic Melanoma. Cell 2016, 165, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Amaral, T.; Schulze, M.; Sinnberg, T.; Nieser, M.; Martus, P.; Battke, F.; Garbe, C.; Biskup, S.; Forschner, A. Are pathogenic germline variants in metastatic melanoma associated with resistance to combined immunotherapy? Cancers 2020, 12, 1101. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Spragg, S.E.; Ciccone, M.A.; Blake, E.A.; Ricker, C.; Pham, H.Q.; Roman, L.D. Nivolumab use for BRCA gene mutation carriers with recurrent epithelial ovarian cancer: A case series. Gynecol. Oncol. Rep. 2018, 25, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.L.; Selenica, P.; Zhou, Q.; Iasonos, A.; Callahan, M.; Feit, N.Z.; Boland, J.; Vazquez-Garcia, I.; Mandelker, D.; Zehir, A.; et al. BRCA Mutations, Homologous DNA Repair Deficiency, Tumor Mutational Burden, and Response to Immune Checkpoint Inhibition in Recurrent Ovarian Cancer. JCO Precis. Oncol. 2020, 4, 665–679. [Google Scholar] [CrossRef]
- Boudadi, K.; Suzman, D.L.; Anagnostou, V.; Fu, W.; Luber, B.; Wang, H.; Niknafs, N.; White, J.R.; Silberstein, J.L.; Sullivan, R.; et al. Ipilimumab plus nivolumab and DNA-repair defects in AR-V7-expressing metastatic prostate cancer. Oncotarget 2018, 9, 28561–28571. [Google Scholar] [CrossRef] [Green Version]
- Markowski, M.C.; Shenderov, E.; Eisenberger, M.A.; Kachhap, S.; Pardoll, D.M.; Denmeade, S.R.; Antonarakis, E.S. Extreme responses to immune checkpoint blockade following bipolar androgen therapy and enzalutamide in patients with metastatic castration resistant prostate cancer. Prostate 2020, 80, 407–411. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Piulats, J.M.; Gross-Goupil, M.; Goh, J.; Ojamaa, K.; Hoimes, C.J.; Vaishampayan, U.; Berger, R.; Sezer, A.; Alanko, T.; et al. Pembrolizumab for treatment-refractory metastatic castration-resistant prostate cancer: Multicohort, open-label phase II KEYNOTE-199 study. J. Clin. Oncol. 2020, 38, 395–405. [Google Scholar] [CrossRef]
- Pang, X.; Qian, J.; Jin, H.; Zhang, L.; Lin, L.; Wang, Y.; Lei, Y.; Zhou, Z.; Li, M.; Zhang, H. Durable benefit from immunotherapy and accompanied lupus erythematosus in pancreatic adenocarcinoma with DNA repair deficiency. J. Immunother. Cancer 2020, 8, e000463. [Google Scholar] [CrossRef]
- Boeck, S.; Mehraein, Y.; Ormanns, S.; Kruger, S.; Westphalen, C.B.; Haas, M.; Jung, A.; Kirchner, T.; Heinemann, V. Mismatch-repair-deficient metastatic pancreatic ductal adenocarcinoma with a germline PALB2 mutation: Unusual genetics, unusual clinical course. Ann. Oncol. 2017, 28, 438–439. [Google Scholar] [CrossRef]
- Dizon, D.S.; Dias-Santagata, D.; Bregar, A.; Sullivan, L.; Filipi, J.; DiTavi, E.; Miller, L.; Ellisen, L.; Birrer, M.; DelCarmen, M. Complete Remission Following Pembrolizumab in a Woman with Mismatch Repair-Deficient Endometrial Cancer and a Germline BRCA1 Mutation. Oncologist 2018, 23, 650–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santin, A.D.; Bellone, S.; Buza, N.; Choi, J.; Schwartz, P.E.; Schlessinger, J.; Lifton, R.P. Regression of chemotherapy-resistant polymerase ϵ (POLE) ultra-mutated and MSH6 hyper-mutated endometrial tumors with nivolumab. Clin. Cancer Res. 2016, 22, 5682–5687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momen, S.; Fassihi, H.; Davies, H.R.; Nikolaou, C.; Degasperi, A.; Stefanato, C.M.; Dias, J.M.L.; Dasgupta, D.; Craythorne, E.; Sarkany, R.; et al. Dramatic response of metastatic cutaneous angiosarcoma to an immune checkpoint inhibitor in a patient with xeroderma pigmentosum: Whole-genome sequencing aids treatment decision in end-stage disease. Cold Spring Harb. Mol. Case Stud. 2019, 5, a004408. [Google Scholar] [CrossRef] [PubMed]
- Johanns, T.M.; Miller, C.A.; Dorward, I.G.; Tsien, C.; Chang, E.; Perry, A.; Uppaluri, R.; Ferguson, C.; Schmidt, R.E.; Dahiya, S.; et al. Immunogenomics of hypermutated glioblastoma: A patient with germline POLE deficiency treated with checkpoint blockade immunotherapy. Cancer Discov. 2016, 6, 1230–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Germline DDR Variant Present (n = 7) | Germline DDR Variant Absent (n = 13) | |
|---|---|---|
| Age at diagnosis (median, range) | 59 (31–73) | 57 (43–71) |
| Gender | 5 males—2 females | 7 males—6 females |
| Tumor Type (n) | ||
| Malignant melanoma | 3 | 2 |
| Squamous cell carcinoma of unknown origin | 1 | 0 |
| Renal cell carcinoma | 1 | 11 |
| Transitional cell carcinoma | 2 | 0 |
| Second Tumor (n) | ||
| Prostate adenocarcinoma | 2 | 2 |
| Colorectal adenocarcinoma | 1 | 2 |
| Transitional cell carcinoma | 0 | 1 |
| Breast cancer | 0 | 5 |
| Malignant melanoma | 0 | 2 |
| Basocellular carcinoma (skin) | 0 | 2 |
| Squamous cell carcinoma (skin) | 0 | 1 |
| Endometrial cancer | 0 | 1 |
| Clinical and Biochemical Characteristics | ||
| Number of metastatic sites (mean, SD) | 3.57 ± 1.8 | 2.23 ± 1.0 |
| CRP (mg/L) (mean, SD) | 28.5 ± 63.0 | 51.2 ± 77.9 |
| Albumin (g/L) (mean, SD) | 40.9 ± 5.34 | 39.3 ± 3.9 |
| NLR (mean, SD) | 5.85 ± 7.1 | 3.54 ± 2.6 |
| LDH (U/l) (mean, SD) | 237.9 ± 87.2 | 207.2 ± 65.2 |
| ECOG Performance Status | ||
| ECOG 0 (n, %) | 5 (71.4%) | 8 (61.5%) |
| ECOG 1 (n, %) | 2 (28.6%) | 5 (38.5%) |
| Type of ICPI | ||
| Nivolumab | 3 (42.9%) | 8 (61.5%) |
| Ipilimumab and nivolumab | 1 (14.3%) | 4 (30.8%) |
| Pembrolizumab | 2 (28.6%) | 1 (7.7%) |
| Atezolizumab | 1 (14.3%) | 0 (0%) |
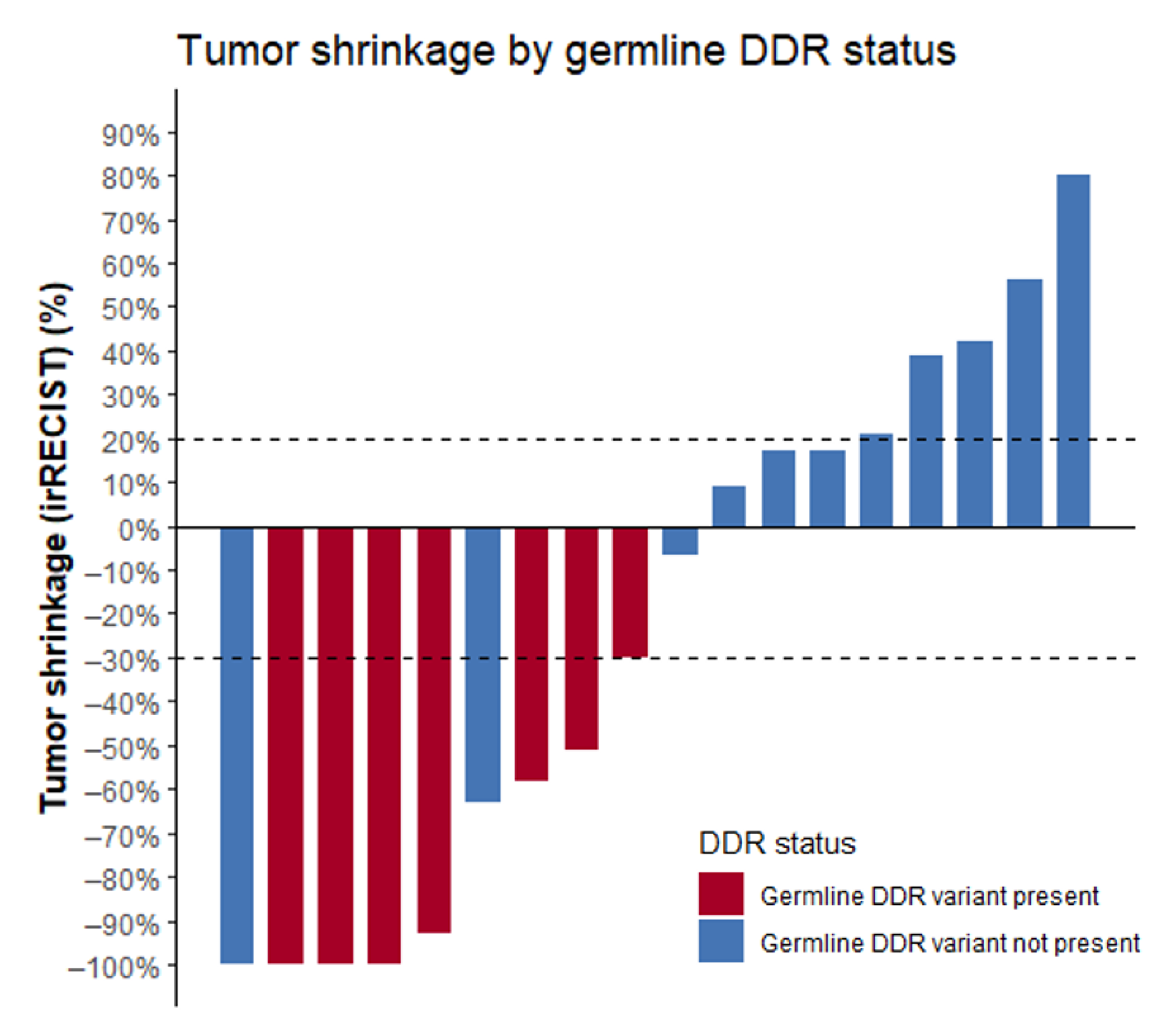
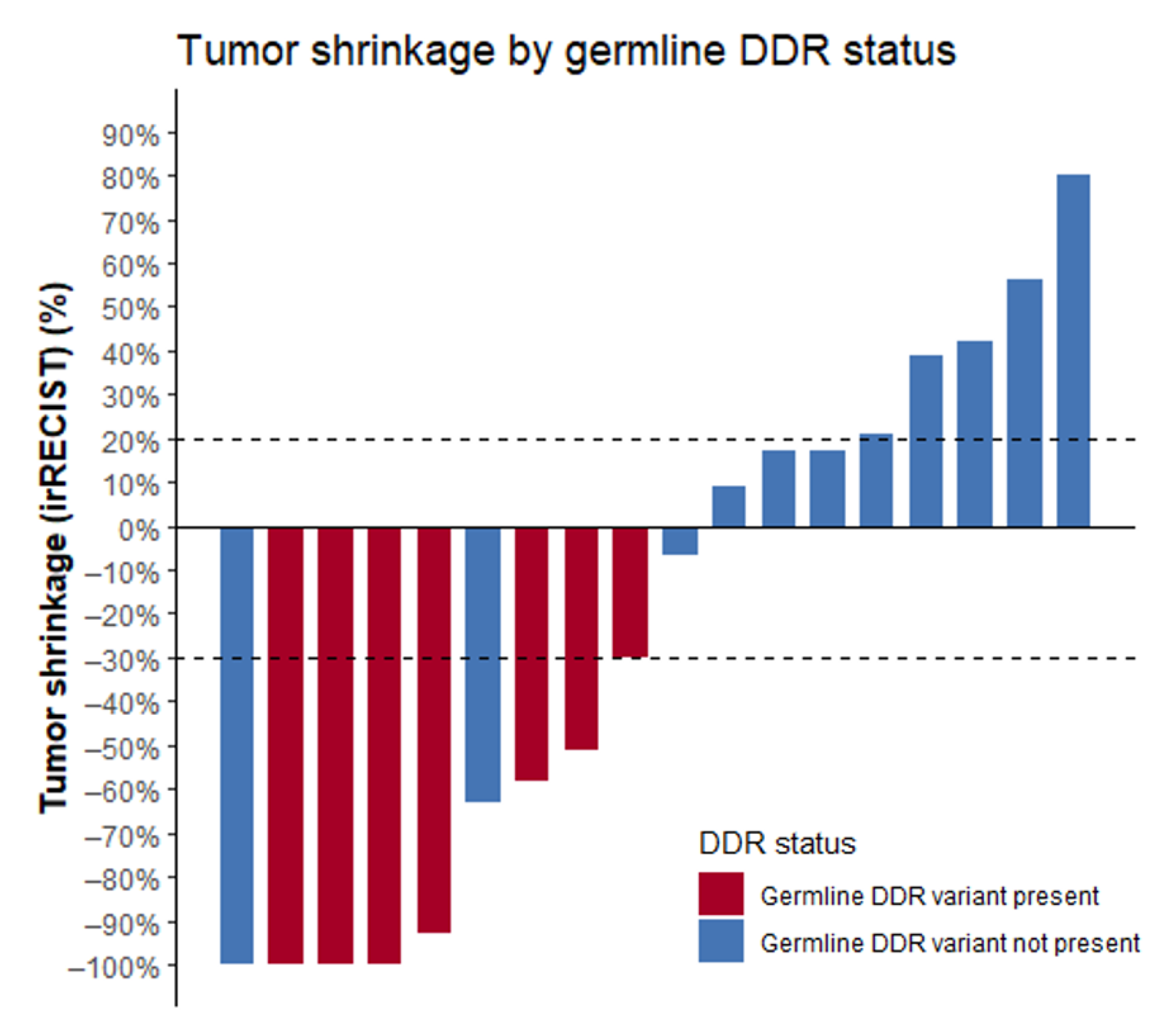
| Germline DDR Status | Partial Response | Stable Disease | Progressive Disease | Clinical Benefit | p-Value (Chi-Square Test) |
|---|---|---|---|---|---|
| Germline DDR variant present | 6/7 (86%) | 1/7 (14%) | 0/7 (0%) | 0/7 (0%) | 0.02 |
| Germline DDR variant absent | 2/13 (15.4%) | 4/13 (30.8%) | 5/13 (38.5%) | 2/13 (15.4%) |
| Patient | Genetic Variant Identified | Genetic Screening Performed |
| 1 | BRCA1 (c.212+3A>G, p.?) | Analysis of known family variant |
| 2 | BRCA2 (c.6644_6647del, p.Ty2215Serfs*13) | Analysis of known family variant |
| 3 | CHEK2 (c.1100del, p.Thr367Metfs*15) | Analysis of known family variant |
| 4 | BRCA2 (c.516+1G>A, p.?) | Analysis of known family variant |
| 5 | BRCA1 (c.5186T>A, p.Leu1729Gln) | ATM, BRIP1, CDH1, CHEK2, MLH1, MSH2, MSH6, NBN (only c.657_661del), PALB2, PTEN, RAD51C, RAD51D, TP53 Additional testing: NGS sequencing of tumor tissue |
| 6 | BRCA2 (c.4936_4939del, p.Glu1646Glnfs*23) | Analysis of known family variant |
| 7 | BRCA1 (c.212+3A>G, p.?) | Analysis of known family variant |
| 8 | No class 4 or 5 variant found | HaloPlex panel |
| 9 | No class 4 or 5 variant found | HaloPlex panel |
| 10 | No class 4 or 5 variant found | HaloPlex panel |
| 11 | No class 4 or 5 variant found | HaloPlex panel |
| 12 | No class 4 or 5 variant found | HaloPlex panel |
| 13 | No class 4 or 5 variant found | HaloPlex panel |
| 14 | No class 4 or 5 variant found | HaloPlex panel |
| 15 | No class 4 or 5 variant found | HaloPlex panel |
| 16 | No class 4 or 5 variant found | BRCA hereditary cancer MASTR plus kit |
| 17 | No class 4 or 5 variant found | BRCA hereditary cancer MASTR plus kit |
| 18 | No class 4 or 5 variant found | BRCA hereditary cancer MASTR plus kit |
| 19 | No class 4 or 5 variant found | FamCanc + Precision 2 trial (BMSO) |
| 20 | No class 4 or 5 variant found | HaloPlex panel |
| Authors | n | Somatic or Germline | ICPI | Concordant with DDR Hypothesis | Findings |
|---|---|---|---|---|---|
| Pan-cancer | |||||
| Zhou et al. [36] | 141 | Somatic | ICPI in monotherapy or combination | Yes | Patients with somatic BRCA2 alterations had improved OS (median OS 31 vs. 18 months, p = 0.02). Patients with BRCA2 altered tumors with low TMB had comparable OS with patients with high TMB tumors (median OS 44 vs. 41 months; p < 0.001). |
| Metastatic urothelial carcinoma | |||||
| Teo et al. [37] | 60 | Somatic | Anti-PD(L)1 antibodies in monotherapy | Yes | Response rate of 80% in patients with deleterious DDR alteration (n = 18), 54% in patients with DDR VUS (n = 15) and 19% in wild type tumors (n = 17) (p < 0.001). Median PFS not reached, 15.8 and 2.9 months, respectively, and median OS not reached, 23.0 and 9.3 months, respectively. |
| Joshi et al. [38] | 53 | Somatic | Anti-PD(L)1 antibodies | Yes | DDR alterations, somatic or germline, were associated with trend towards longer OS. Increased number of DDR alterations were associated with trend for higher ORR. |
| Powles et al. [39] | 559 | Somatic | Avelumab versus BSC | Yes | DDR alterations were associated with improved OS when treated with ICPI (HR 0.65; 95%CI 0.504–0.847) compared to BSC. Association was not observed in DDR wild type tumors (HR 0.89; 95%CI 0.489–1.612). |
| Metastatic renal cell carcinoma | |||||
| Labriola et al. [40] | 34 | Somatic | Nivolumab, ipilimumab—nivolumab or pembrolizumab | Yes | 68.8% of patients with disease control (n = 16) had enrichment in somatic DDR alterations vs. 38.9% of patients with PD (n = 18) (p = 0.03). |
| Ged et al. [41] | 107 | Germline (27%) Somatic (73%) | Anti-PD1 monotherapy (68%) and combination ICPIs (32%) | Yes | 19 patients had deleterious DDR alterations and 88 patients wild type/VUS DDR. Deleterious DDR was associated with improved OS on ICPI (p = 0.049). This effect was not seen in control group of 118 patients treated with angiogenesis inhibitors. |
| Metastatic malignant melanoma | |||||
| Hugo et al. [42] | 469 | Somatic | Nivolumab and pembrolizumab | Yes | 28 patients had somatic BRCA2 mutation. BRCA2 mutations were significantly more frequent in responders compared to nonresponders (OR 6.2, p = 0.002). |
| Amaral et al. [43] | 4 | Germline | Combination ICPIs | No | None of the patients (two with BRCA2, one with BAP1 and one with PALB2 germline alteration) responded well. |
| Metastatic ovarian carcinoma | |||||
| Matsuo et al. [44] | 6 | Germline | Nivolumab | Yes | In these six heavily pretreated patients with germline BRCA1/2 mutations, ORR was 67%. |
| Liu et al. [45] | 134 | Somatic of germline | ICPIs | No | 31 patients had deleterious somatic or germline BRCA1/2 mutations. No association was found between mutation status and response to ICPIs. |
| Metastatic castration resistant prostate carcinoma | |||||
| Boudadi et al. [46] | 15 | Somatic | Ipilimumab—nivolumab | Yes | Six out of these 15 patients with an aggressive subtype of AR-V7 expressing prostate carcinoma carried a somatic DDR mutation (three BRCA2, two in ATM and one in ERCC4) and showed improved PFS (HR 0.31, p = 0.01) compared to the nine patients without DDR mutations. |
| Markowski et al. [47] | 3 | One germline, two somatic | PD-1 inhibitors | Yes | Three patients with inactivating BRCA2 or ATM mutations showed profound and durable response to ICPI. |
| Antonarakis et al. [48] | 153 | Somatic | Pembrolizumab | No | 29 patients with somatic DDR mutations, response to ICPI was not associated with mutational status. |
| Case reports in other tumors | |||||
| Pang et al. [49] | 1 | Germline | Pembrolizumab | Yes | Patient with metastatic PDAC with germline and somatic PALB2 mutation, had a durable PR. |
| Boeck et al. [50] | 1 | Germline | Pembrolizumab | No | Patient with metastatic PDAC, with a germline PALB2 mutation, had PD as best response. |
| Dizon et al. [51] | 1 | Germline and somatic | Pembrolizumab | Yes | Patient with high grade Mullerian adenocarcinoma, with germline BRCA1 and somatic BRCA2 mutation, had a CR. |
| Santin et al. [52] | 1 | Somatic | Nivolumab | Yes | Patient with hypermutated endometrial tumor with a POLE mutation had a profound PR. |
| Momen et al. [53] | 1 | Germline | Pembrolizumab | Yes | Patient with xeroderma pigmentosum (germline XPC mutation) and metastatic angiosarcoma (somatic POLE mutation and high TMB) achieved PR. |
| Johanns et al. [54] | 1 | Germline | Pembrolizumab | Yes | Patient with a hypermutated glioblastoma and germline POLE mutation showed evidence of clinical and immunological response to ICPI. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinget, L.; Bechter, O.; Punie, K.; Debruyne, P.R.; Brems, H.; Clement, P.; Roussel, E.; Van Herck, Y.; Albersen, M.; Baldewijns, M.; et al. Multitumor Case Series of Germline BRCA1, BRCA2 and CHEK2-Mutated Patients Responding Favorably on Immune Checkpoint Inhibitors. Curr. Oncol. 2021, 28, 3227-3239. https://doi.org/10.3390/curroncol28050280
Kinget L, Bechter O, Punie K, Debruyne PR, Brems H, Clement P, Roussel E, Van Herck Y, Albersen M, Baldewijns M, et al. Multitumor Case Series of Germline BRCA1, BRCA2 and CHEK2-Mutated Patients Responding Favorably on Immune Checkpoint Inhibitors. Current Oncology. 2021; 28(5):3227-3239. https://doi.org/10.3390/curroncol28050280
Chicago/Turabian StyleKinget, Lisa, Oliver Bechter, Kevin Punie, Philip R. Debruyne, Hilde Brems, Paul Clement, Eduard Roussel, Yannick Van Herck, Maarten Albersen, Marcella Baldewijns, and et al. 2021. "Multitumor Case Series of Germline BRCA1, BRCA2 and CHEK2-Mutated Patients Responding Favorably on Immune Checkpoint Inhibitors" Current Oncology 28, no. 5: 3227-3239. https://doi.org/10.3390/curroncol28050280
APA StyleKinget, L., Bechter, O., Punie, K., Debruyne, P. R., Brems, H., Clement, P., Roussel, E., Van Herck, Y., Albersen, M., Baldewijns, M., Schöffski, P., & Beuselinck, B. (2021). Multitumor Case Series of Germline BRCA1, BRCA2 and CHEK2-Mutated Patients Responding Favorably on Immune Checkpoint Inhibitors. Current Oncology, 28(5), 3227-3239. https://doi.org/10.3390/curroncol28050280