A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Survey Administration
2.2. Survey Measures and Definitions
2.2.1. Measuring a Negative and Positive Impact on Cancer Care Delivery
2.2.2. Measuring Sociodemographic-, Cancer-, and Other Health-Related Information
2.2.3. Province or Territory of Residence
2.3. Statistical Analysis
2.4. Qualitative Analysis
3. Results
3.1. Patient Demographics
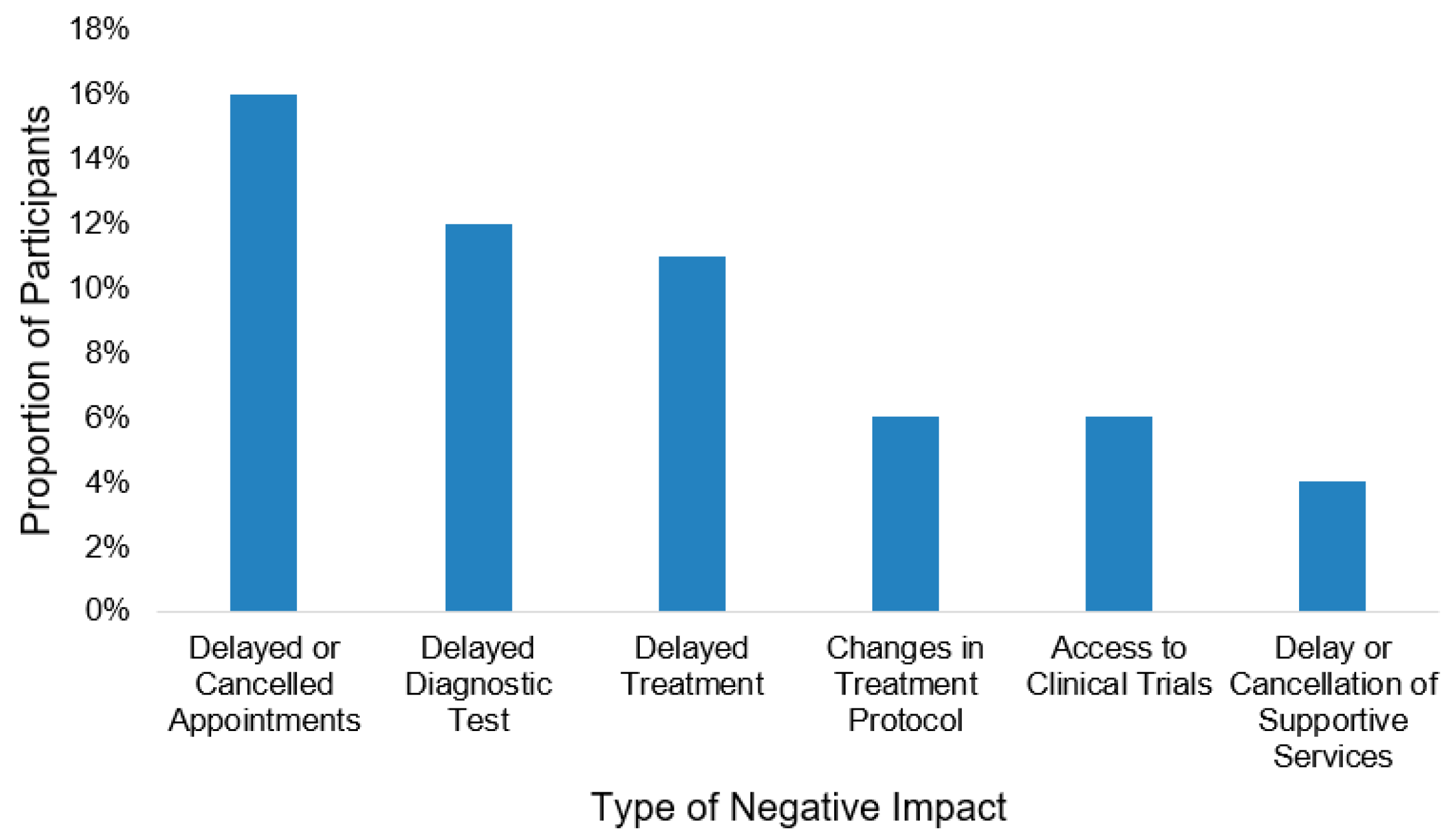
3.2. Impact of COVID-19 Pandemic on Cancer Care
3.3. Factors Associated with a Negative Impact of COVID-19 Pandemic on Cancer Care
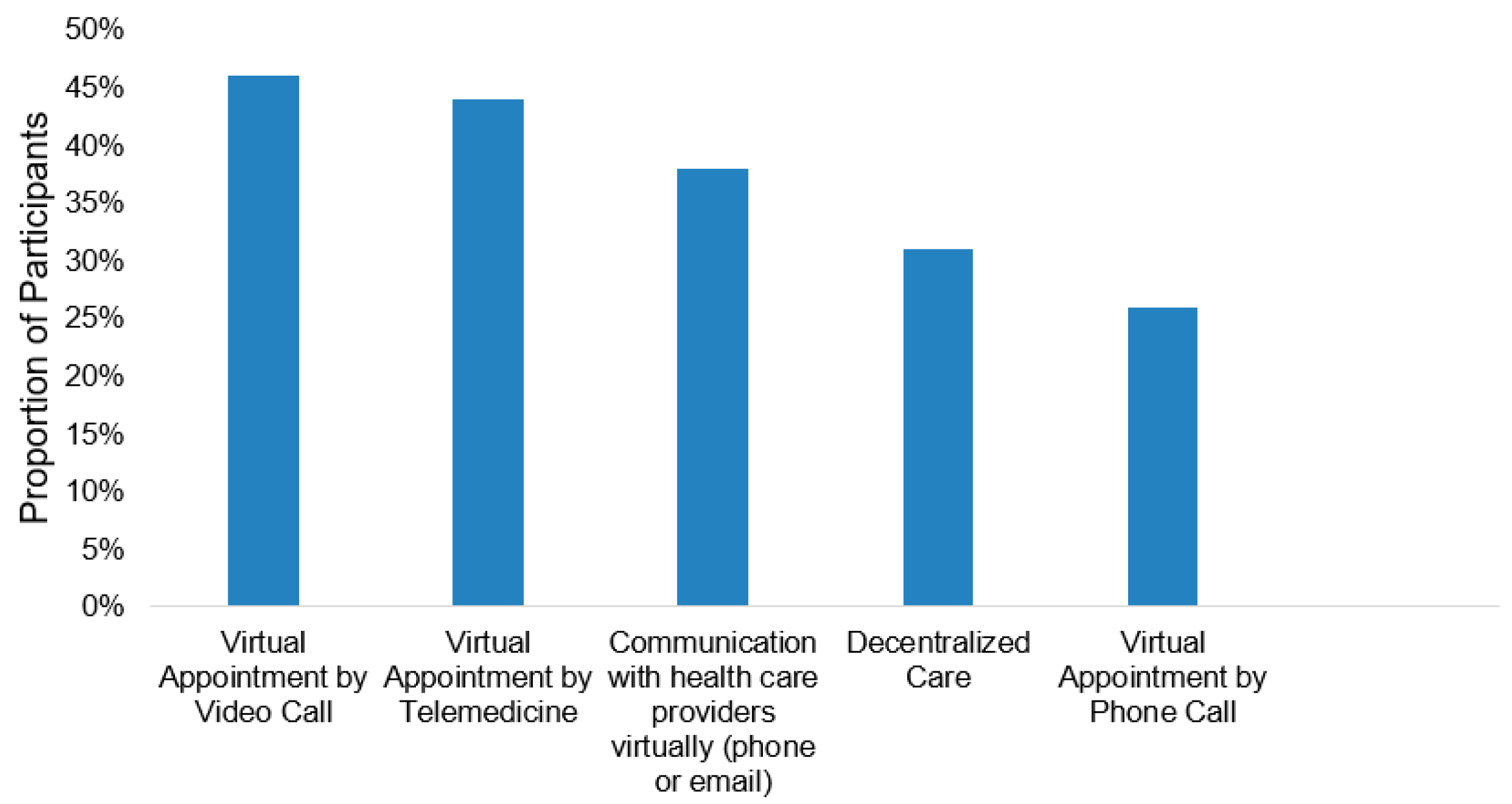
3.4. Optimization of Cancer Care
“Provide telephone and network consultation services to reduce the number of visits to the hospital and increase the function of making an appointment in advance.”
“Need more access electronically to supports (texts, email, etc.), would like access to test results, I think video chat is better than phone calls.”
“I think telephone and virtual appointments are only helpful for some people and should not be a catchall. I would prefer to see more in-person options for those that are struggling.”
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Graetz, D.; Agulnik, A.; Ranadive, R.; Vedaraju, Y.; Chen, Y.; Chantada, G.; Metzger, M.L.; Mukkada, S.; Force, L.M.; Friedrich, P.; et al. Global effect of the COVID-19 pandemic on paediatric cancer care: A cross-sectional study. Lancet Child Adolesc. Health 2021, 5, 332–340. [Google Scholar] [CrossRef]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A War on Two Fronts: Cancer Care in the Time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Jazieh, A.R.; Akbulut, H.; Curigliano, G.; Rogado, A.; Alsharm, A.A.; Razis, E.D.; Mula-Hussain, L.; Errihani, H.; Khattak, A.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob. Oncol. 2020, 6, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- Moraliyage, H.; De Silva, D.; Ranasinghe, W.; Adikari, A.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Cancer in Lockdown: Impact of the COVID-19 Pandemic on Patients with Cancer. Oncologist 2020, 26, 342–344. [Google Scholar] [CrossRef]
- Constantinou, C.; Kolokotroni, O.; Mosquera, M.; Heraclides, A.; Demetriou, C.; Karayiannis, P.; Quattrocchi, A.; Charalambous, A. Developing a holistic contingency plan: Challenges and dilemmas for cancer patients during the COVID-19. Cancer Med. 2020, 9, 6082–6092. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.; Babik, J.M. COVID-19 in Immunocompromised Hosts: What We Know So Far. Clin. Infect. Dis. 2020, 72, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.R.; Chan, S.L.; Curigliano, G.; Dickson, N.; Eaton, V.; Garcia-Foncillas, J.; Gilmore, T.; Horn, L.; Kerr, D.J.; Lee, J.; et al. Delivering Cancer Care during the COVID-19 Pandemic: Recommendations and Lessons Learned from ASCO Global Webinars. JCO Glob. Oncol. 2020, 6, 1461–1471. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, Z.; Ma, Z.; Mao, Y.; Li, X.; Wilson, A.; Qin, H.; Ou, J.; Peng, K.; Zhou, F.; et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl. Psychiatry 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.D.; Ferrari, A.; Ries, L.; Whelan, J.; Bleyer, W.A. Cancer in Adolescents and Young Adults. JAMA Pediatr. 2016, 170, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Košir, U.; Loades, M.; Wild, J.; Wiedemann, M.; Krajnc, A.; Roškar, S.; Bowes, L. The impact of COVID-19 on the cancer care of adolescents and young adults and their well-being: Results from an online survey conducted in the early stages of the pandemic. Cancer 2020, 126, 4414–4422. [Google Scholar] [CrossRef]
- YACPRIME: A Study to Incite Change; Young Adult Cancer Canada (YACC): 2019. Available online: https://youngadultcancer.ca/yacprime/ (accessed on 12 May 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Thompson, C.G.; Kim, R.S.; Aloe, A.M.; Becker, B.J. Extracting the Variance Inflation Factor and Other Multicollinearity Diagnostics from Typical Regression Results. Basic Appl. Soc. Psychol. 2017, 39, 81–90. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 13 May 2021).
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Dedoose Version 8.3.47, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data (2021). SocioCultural Research Consultants LLC: Los Angeles, CA, USA. Available online: www.dedoose.com (accessed on 13 May 2021).
- Kolb, S. Grounded Theory and the Constant Comparative Method: Valid Research Strategies for Educators. JETERAPS 2016, 3, 83–86. [Google Scholar]
- Lou, E.; Teoh, D.; Brown, K.; Blaes, A.; Holtan, S.G.; Jewett, P.; Parsons, H.; Mburu, E.W.; Thomaier, L.; Hui, J.Y.C.; et al. Perspectives of cancer patients and their health during the COVID-19 pandemic. PLoS ONE 2020, 15, e0241741. [Google Scholar] [CrossRef]
- Chen-See, S. Disruption of cancer care in Canada during COVID-19. Lancet Oncol. 2020, 21, e374. [Google Scholar] [CrossRef]
- Papautsky, E.L.; Hamlish, T. Patient-reported treatment delays in breast cancer care during the COVID-19 pandemic. Breast Cancer Res. Treat. 2020, 184, 249–254. [Google Scholar] [CrossRef]
- Holland, K.M.; Jones, C.; Vivolo-Kantor, A.M.; Idaikkadar, N.; Zwald, M.; Hoots, B.; Yard, E.; D’Inverno, A.; Swedo, E.; Chen, M.S.; et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes before and during the COVID-19 Pandemic. JAMA Psychiatry 2021, 78, 372. [Google Scholar] [CrossRef] [PubMed]
- Rains, L.S.; Johnson, S.; Barnett, P.; Steare, T.; Needle, J.J.; Carr, S.; Taylor, B.L.; Bentivegna, F.; Edbrooke-Childs, J.; Scott, H.R.; et al. Early impacts of the COVID-19 pandemic on mental health care and on people with mental health conditions: Framework synthesis of international experiences and responses. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 56, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Hendren, S.; Chin, N.; Fisher, S.; Winters, P.; Griggs, J.; Mohile, S.; Fiscella, K. Patients’ Barriers to Receipt of Cancer Care, and Factors Associated with Needing More Assistance from a Patient Navigator. J. Natl. Med. Assoc. 2011, 103, 701–710. [Google Scholar] [CrossRef]
- Kantamneni, N. The impact of the COVID-19 pandemic on marginalized populations in the United States: A research agenda. J. Vocat. Behav. 2020, 119, 103439. [Google Scholar] [CrossRef]
- Cameron-Blake, E.; Breton, C.; Sim, P.; Tatlow, H.; Hale, T.; Wood, A.; Smith, J.; Sawatsky, J.; Parsons, Z.; Tyson, K. Variation in the Canadian Provincial and Territorial Responses to COVID-19; University of Oxford: Oxford, UK, 2021; Available online: https://centre.irpp.org/wp-content/uploads/sites/3/2021/03/Variation-in-the-Canadian-provincial-and-territorial-responses-to-COVID-19.pdf (accessed on 23 May 2021).
- Hasson, S.P.; Waissengrin, B.; Shachar, E.; Hodruj, M.; Fayngor, R.; Brezis, M.; Nikolaevski-Berlin, A.; Pelles, S.; Safra, T.; Geva, R.; et al. Rapid Implementation of Telemedicine during the COVID-19 Pandemic: Perspectives and Preferences of Patients with Cancer. Oncologist 2021, 26, e679–e685. [Google Scholar] [CrossRef]
- Ramaswamy, A.; Yu, M.; Drangsholt, S.; Ng, E.; Culligan, P.J.; Schlegel, P.N.; Hu, J.C. Patient Satisfaction with Telemedicine during the COVID-19 Pandemic: Retrospective Cohort Study. J. Med. Internet Res. 2020, 22, e20786. [Google Scholar] [CrossRef]
- Mustafa, S.S.; Yang, L.; Mortezavi, M.; Vadamalai, K.; Ramsey, A. Patient satisfaction with telemedicine encounters in an allergy and immunology practice during the coronavirus disease 2019 pandemic. Ann. Allergy Asthma Immunol. 2020, 125, 478–479. [Google Scholar] [CrossRef]
- Shaverdian, N.; Gillespie, E.F.; Cha, E.; Kim, S.Y.; Benvengo, S.; Chino, F.; Kang, J.J.; Li, Y.; Atkinson, T.M.; Lee, N.; et al. Impact of Telemedicine on Patient Satisfaction and Perceptions of Care Quality in Radiation Oncology. J. Natl. Compr. Cancer Netw. 2021, 1, 1–7. [Google Scholar]
- Yoon, E.J.; Tong, D.; Anton, G.M.; Jasinski, J.M.; Claus, C.F.; Soo, T.M.; Kelkar, P.S. Patient Satisfaction with Neurosurgery Telemedicine Visits during the Coronavirus Disease 2019 Pandemic: A Prospective Cohort Study. World Neurosurg. 2021, 145, e184–e191. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Berlin, A.; Lovas, M.; Truong, T.; Melwani, S.; Liu, J.; Liu, Z.A.; Badzynski, A.; Carpenter, M.B.; Virtanen, C.; Morley, L.; et al. Implementation and Outcomes of Virtual Care Across a Tertiary Cancer Center during COVID-19. JAMA Oncol. 2021, 7, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Edwards, C.; Davey-Rothwell, M.A.; Tobin, K.E. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict. Behav. 2017, 73, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Tariq, S.; Woodman, J. Using mixed methods in health research. JRSM Short Rep. 2013, 4, 2042533313479197. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Mean ± SD, or n | % (Range) |
|---|---|---|
| Age (in years) | 30.27 ± 5.27 | (18–39) |
| Gender a | ||
| - Man | 445 | 55.50% |
| - Woman | 357 | 44.50% |
| - Non-Binary | 3 | 0.00% |
| Ethnicity (White) | 770 | 95.60% |
| Relationship Status (in a relationship) | 484 | 60.10% |
| Province/Territory | ||
| - Prairies e | 233 | 28.90% |
| - Central Canada f | 222 | 27.60% |
| - Atlantic g | 169 | 21.00% |
| - Territories h | 93 | 11.60% |
| - British Columbia | 88 | 10.90% |
| Geographic Location b | ||
| - Urban | 605 | 75.50% |
| - Rural | 179 | 22.30% |
| - Remote | 17 | 2.10% |
| Education Status c | ||
| - Part-time student | 24 | 3.00% |
| - Full-time student | 75 | 9.30% |
| Employment Status c | ||
| - Employed (part or full time) | 562 | 70.00% |
| - Unemployed | 103 | 12.80% |
| - Disability or unemployment benefits | 32 | 4.00% |
| - Other i | 51 | 6.30% |
| Personal Income in year 2020 j | ||
| - <$20,000 | 57 | 7.10% |
| - $20,000 to <$40,000 | 115 | 14.30% |
| - $40,000 to <$60,000 | 195 | 24.30% |
| - ≥$60,000 | 389 | 48.40% |
| Pre-pandemic mental health condition (yes) d | 118 | 14.80% |
| Type of pre-pandemic mental health condition d | ||
| - Anxiety disorder | 75 | 9.40% |
| - Mood disorder | 65 | 8.10% |
| - Other k | 4 | 0.50% |
| Presence of a chronic physical health condition (yes) | 192 | 23.90% |
| Type of chronic physical condition | ||
| - Hypertension or Diabetes | 89 | 11.00% |
| - Lung or Heart Disease | 59 | 7.30% |
| - Kidney or Liver Disease | 58 | 7.20% |
| - Other l | 22 | 2.70% |
| Cancer type | ||
| - Hematological malignancies | 155 | 19.30% |
| - Solid tumors (non-brain tumors) | 615 | 76.40% |
| - Brain tumors | 35 | 4.30% |
| Time since cancer diagnosis | ||
| - <2 years | 246 | 30.50% |
| - 2 years to <5 years | 421 | 52.20% |
| - ≥5 years | 138 | 17.10% |
| Currently receiving cancer treatment (yes) c | 265 | 33.00% |
| Negative impact of COVID-19 pandemic on cancer care | ||
| - Yes | 173 | 21.50% |
| - No | 632 | 78.50% |
| Univariable Analysis (n = 805) | Multivariable Analysis (n = 707) | |||||
|---|---|---|---|---|---|---|
| Adjusted Odds Ratio | 95% CI (Lower-Upper) | p-Value | Adjusted Odds Ratio | 95% CI (Lower, Upper) | p-Value | |
| Age | ||||||
| - >25 years | 0.72 | 0.49–1.07 | 0.102 | 0.98 | 0.94–1.03 | 0.431 |
| - <18–25 years | (ref) | (ref) | ||||
| Gender a | ||||||
| - Woman | 1.73 | 1.23–2.43 | 0.001 | 1.41 | 0.90–2.20 | 0.13 |
| - Man | (ref) | (ref) | ||||
| Ethnicity | ||||||
| - Non-White | 1.8 | 0.83–3.89 | 0.133 | 2.07 | 0.76–5.52 | 0.147 |
| - White | (ref) | (ref) | ||||
| Province/Territory | ||||||
| - Central Canada e | 9.41 | 3.32–26.69 | 8.43 | 2.90–32.03 | <0.001 | |
| - Prairies f | 7.37 | 2.59–20.96 | <0.001 | 4.52 | 1.54–17.13 | 0.012 |
| - British Columbia | 8.83 | 2.93–26.62 | 6.74 | 2.05–27.63 | 0.003 | |
| - Atlantic Canada g | 2.99 | 0.99–9.02 | 2.54 | 0.79–10.14 | 0.144 | |
| - Territories h | (ref) | (ref) | ||||
| Geographic Location b | ||||||
| - Rural | 1.4 | 0.95–2.06 | 1.06 | 0.63–1.76 | 0.815 | |
| - Remote | 0.52 | 0.12–2.32 | 0.146 | 0.69 | 0.09–3.12 | 0.661 |
| - Urban | (ref) | (ref) | ||||
| Income in year 2020 i | ||||||
| - <$20,000 | 4.34 | 2.41–7.80 | <0.001 | 4.21 | 2.03–8.75 | <0.001 |
| - $20,000 to <$40,000 | 1.51 | 0.90–2.53 | 0.89 | 0.45–1.72 | 0.732 | |
| - $40,000 to <$60,000 | 1.51 | 0.98–2.32 | 1.17 | 0.67–2.00 | 0.583 | |
| - $60,000+ | (ref) | (ref) | ||||
| Pre-pandemic mental health condition d | ||||||
| - Yes | 10.93 | 7.08–16.88 | <0.001 | 12.14 | 6.98– 21.66 | <0.001 |
| - No | (ref) | (ref) | ||||
| Presence of a chronic physical health condition d | ||||||
| - Yes | 2.71 | 1.88–3.92 | <0.001 | 2.22 | 1.34–3.67 | 0.002 |
| - No | (ref) | (ref) | ||||
| Time since cancer diagnosis | ||||||
| - <2 years | 0.9 | 0.53–1.53 | 0.32 | 1.08 | 0.53–2.24 | 0.84 |
| - 2 to <5 years | 1.21 | 0.75–1.94 | 1.23 | 0.65–2.39 | 0.529 | |
| - ≥5 years | (ref) | (ref) | ||||
| Cancer type | ||||||
| - Hematologic | 0.95 | 0.61–1.48 | 0.828 | 0.83 | 0.43–1.54 | 0.569 |
| - Non-hematologic j | (ref) | (ref) | ||||
| Currently receiving cancer treatment c | ||||||
| - Yes | 1.1 | 0.77–1.57 | 0.596 | 1.69 | 1.03–2.77 | 0.036 |
| - No | (ref) | (ref) | ||||
| Theme | Definition | Examples of Excerpts |
|---|---|---|
| Improving Healthcare Visits (37%) | ||
| Increased ability to make appointments in advance (flexible and responsible scheduling) | Descriptions of ways care could best be arranged or facilitated by healthcare providers | “Make it easier to contact doctors/nurses through email/video calls” |
| More virtual appointments | “Easier access to doctors regarding appointments and bookings so that calls don’t go weeks with no response” | |
| Providing care closer to home (decentralized care) | “Offers on-site therapy as well as telemedicine” | |
| Enhancing Personalized Care (18%) | ||
| Good communication from cancer organizations | Ideas about how their experience could be enhanced to support their wellbeing by healthcare teams | “Listen to us and do not ignore our symptoms” |
| Caring for and encouraging patients (compassion and validation) | “Continue to provide support services (as opposed to cancelling and closing most services during the pandemic)” | |
| Access to physical rehabilitation | ||
| Increased mental health supports | “Having access to support for mental health, coping, pain management” | |
| Improving Prevention of COVID-19 (15%) | ||
| Physical distancing | Suggestions on ways individuals and healthcare centers can prevent spreading or contracting COVID-19 | “We should not go to places where people gather. If we can not go out, we should not go out” “Reduce the number of visits to the hospital” |
| Use of protective equipment and practices | “Wash your hands frequently and wear a mask” | |
| Addressing Information Needs (13%) | ||
| COVID-19-specific information | Statements describing optimal ways to receive information related to cancer care, self-care, or how the COVID-19 pandemic affects them specifically as a population | “Reach out to cancer patients directly with information on how the pandemic affects our particular cases” |
| In-person and online mediums | “Provide digital resources or connections at home (e.g., how to stay healthy and active)” “Cancer organizations provide better care by including information on the site” | |
| Avoiding Diagnostic and Treatment Delays (11%) | ||
| Delay in diagnosis Delay in treatment | Statements highlighting the importance of not delaying diagnostic tests, appointments, and treatment protocols | “COVID should have NO impact on testing and treatment, and care providers should be very open about why appointments are being rescheduled” “Do not delay follow-up appointments, treatments, or exams” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Howden, K.; Glidden, C.; Romanescu, R.G.; Hatala, A.; Scott, I.; Deleemans, J.; Chalifour, K.; Eaton, G.; Gupta, A.A.; Bolton, J.M.; et al. A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults. Curr. Oncol. 2021, 28, 3201-3213. https://doi.org/10.3390/curroncol28040278
Howden K, Glidden C, Romanescu RG, Hatala A, Scott I, Deleemans J, Chalifour K, Eaton G, Gupta AA, Bolton JM, et al. A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults. Current Oncology. 2021; 28(4):3201-3213. https://doi.org/10.3390/curroncol28040278
Chicago/Turabian StyleHowden, Kaitlyn, Camille Glidden, Razvan G. Romanescu, Andrew Hatala, Ian Scott, Julie Deleemans, Karine Chalifour, Geoff Eaton, Abha A. Gupta, James M. Bolton, and et al. 2021. "A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults" Current Oncology 28, no. 4: 3201-3213. https://doi.org/10.3390/curroncol28040278
APA StyleHowden, K., Glidden, C., Romanescu, R. G., Hatala, A., Scott, I., Deleemans, J., Chalifour, K., Eaton, G., Gupta, A. A., Bolton, J. M., Mahar, A. L., Garland, S. N., & Oberoi, S. (2021). A Cross-Sectional Survey Exploring the Impact of the COVID-19 Pandemic on the Cancer Care of Adolescents and Young Adults. Current Oncology, 28(4), 3201-3213. https://doi.org/10.3390/curroncol28040278