

Fully Digital Workflow for the Fabrication of Three-Dimensionally Printed Surgical Splints for Preventing Postoperative Bleeding: A Case Report

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Ethical Considerations
2.2. Patient
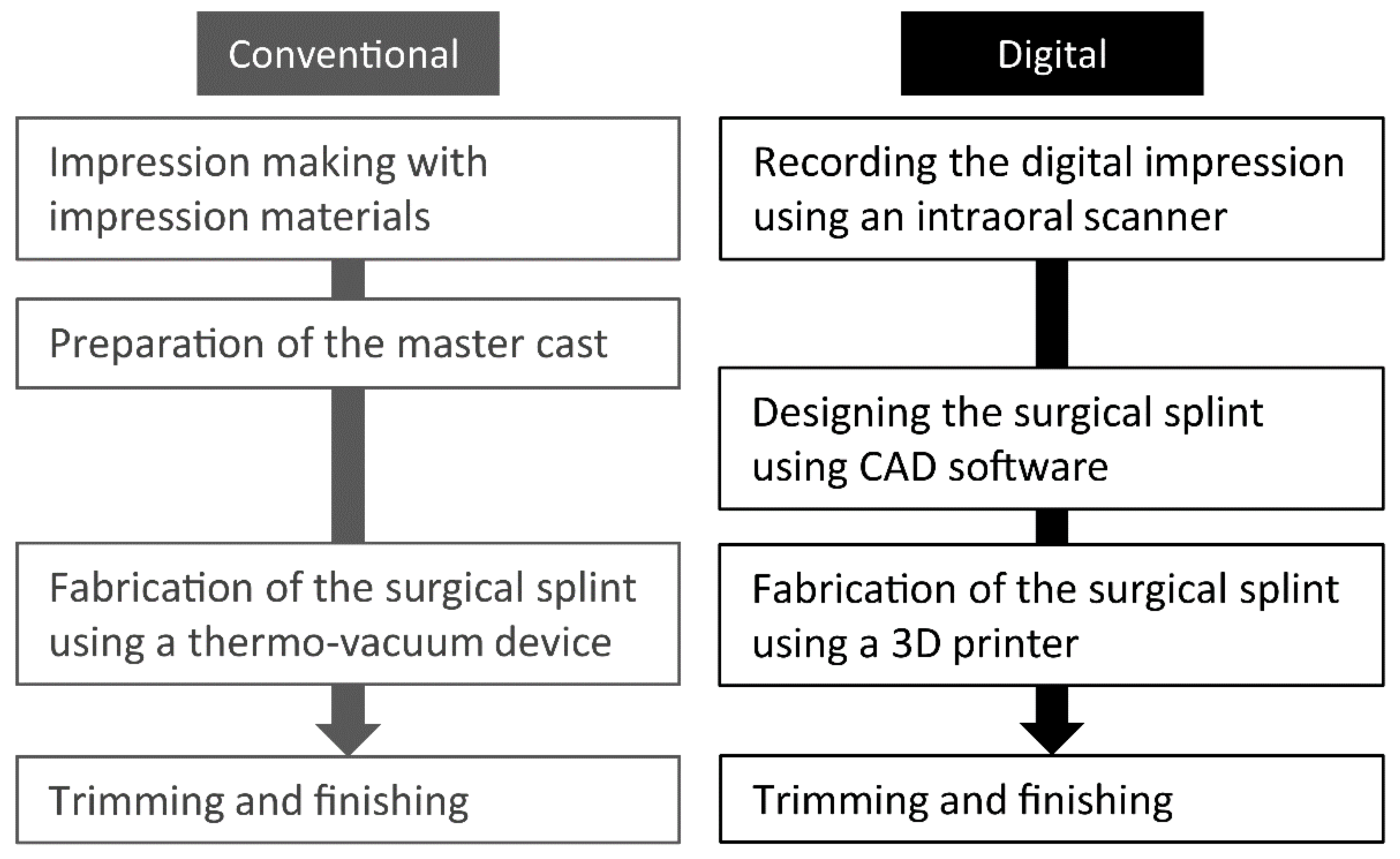
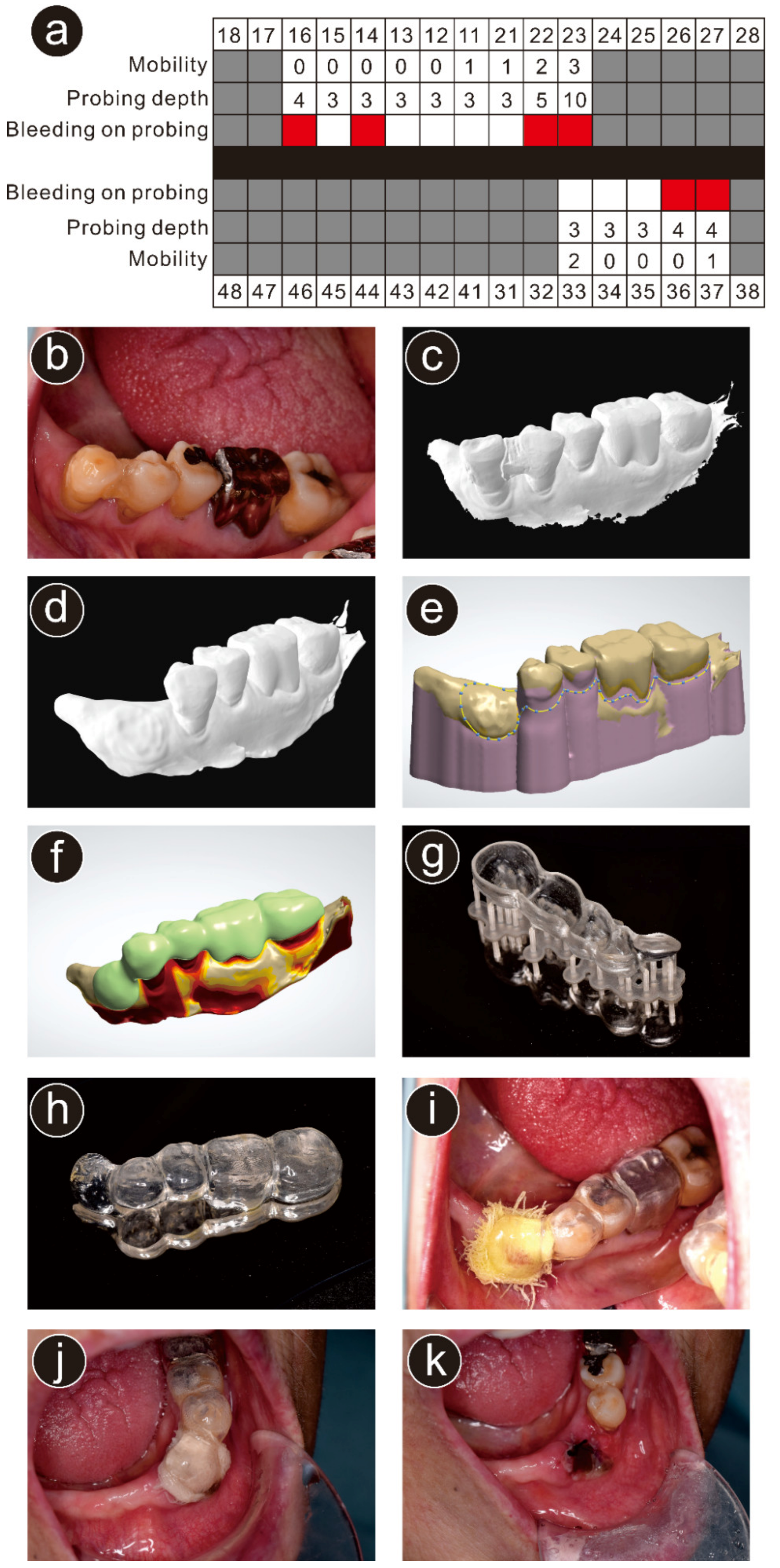
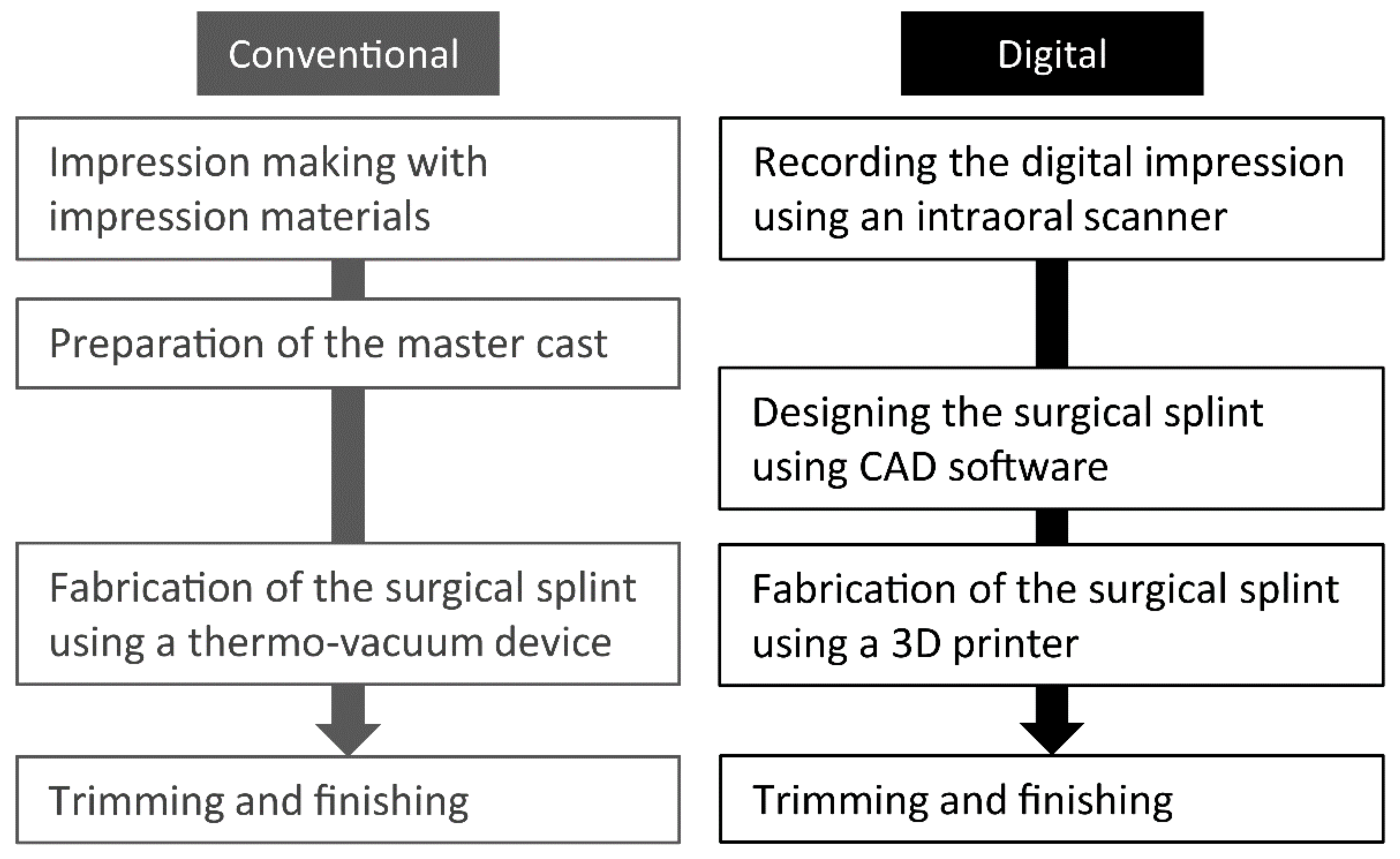
2.3. Treatment Procedure
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuzuya, M. Era of geriatric medical challenges: Multimorbidity among older patients. Geriatr. Gerontol. Int. 2019, 19, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Kwak, E.J.; Nam, S.; Park, K.M.; Kim, S.Y.; Huh, J.; Park, W. Bleeding related to dental treatment in patients taking novel oral anticoagulants (NOACs): A retrospective study. Clin. Oral Investig. 2019, 23, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Inokoshi, M.; Kubota, K.; Yamaga, E.; Ueda, K.; Minakuchi, S. Postoperative bleeding after dental extraction among elderly patients under anticoagulant therapy. Clin. Oral Investig. 2021, 25, 2363–2371. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Fischer, C.M.; Miller, S.E.; Al-Bitar, K.M.; Luepke, P.G. A fully digital workflow to achieve predictable esthetic and functional outcomes: A case series. Int. J. Periodont. Restorat. Dent. 2022, 42, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, H.; Taniguchi, A.; Tanaka, S.; Baba, K. Novel fully digital workflow for removable partial denture fabrication. J. Prosthodont. Res. 2020, 64, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Wahl, E.; Zander, A.T.; Huettig, F.; Spintzyk, S. Intraoral scanning to fabricate complete dentures with functional borders: A proof-of-concept case report. BMC Oral Health 2019, 19, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patzelt, S.B.M.; Krügel, M.; Wesemann, C.; Pieralli, S.; Nold, J.; Spies, B.C.; Vach, K.; Kohal, R.J. In vitro time efficiency, fit, and wear of conventionally- versus digitally-fabricated occlusal splints. Materials 2022, 15, 1085. [Google Scholar] [CrossRef] [PubMed]
- Waldecker, M.; Leckel, M.; Rammelsberg, P.; Bömicke, W. Fully digital fabrication of an occlusal device using an intraoral scanner and 3D printing: A dental technique. J. Prosthet. Dent. 2019, 121, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Dedem, P.; Türp, J.C. Digital Michigan splint—From intraoral scanning to plasterless manufacturing. Int. J. Comput. Dent. 2016, 19, 63–76. [Google Scholar] [PubMed]
- Salmi, M.; Paloheimo, K.S.; Tuomi, J.; Ingman, T.; Mäkitie, A. A digital process for additive manufacturing of occlusal splints: A clinical pilot study. J. R. Soc. Interface 2013, 10, 20130203. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.-J.; Kim, W.; Kim, J.-H.; Baik, U.-B. Stabilization splint fabrication using computer-aided design/computer-aided manufacturing and three-dimensional printing. J. Oral Med. Pain. 2019, 44, 74–76. [Google Scholar]
- Venezia, P.; Muzio, L.L.; De Furia, C.; Torsello, F. Digital manufacturing of occlusal splint: From intraoral scanning to 3D printing. J. Osseointegr. 2019, 11, 535–539. [Google Scholar]
- Joda, T.; Brägger, U. Complete digital workflow for the production of implant-supported single-unit monolithic crowns. Clin. Oral Implants Res. 2014, 25, 1304–1306. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y. A study of the usefulness of implant superstructure production methods using optical impression systems and CAD/CAM techniques. J. Interdiscipl. Clin. Dent. 2020, 1, 1–6. [Google Scholar]
- Yoshida, S.; Yamaguchi, K.; Taniguchi, Y.; Isshi, K.; Kido, H.; Tohara, H. Design of palatal and lingual augmentation prostheses by using an intraoral scanner for a patient after a glossectomy: A clinical report. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inokoshi, M.; Soeda, Y.; Akiyama, Y.; Ueda, K.; Kubota, K.; Minakuchi, S. Fully Digital Workflow for the Fabrication of Three-Dimensionally Printed Surgical Splints for Preventing Postoperative Bleeding: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 12773. https://doi.org/10.3390/ijerph191912773
Inokoshi M, Soeda Y, Akiyama Y, Ueda K, Kubota K, Minakuchi S. Fully Digital Workflow for the Fabrication of Three-Dimensionally Printed Surgical Splints for Preventing Postoperative Bleeding: A Case Report. International Journal of Environmental Research and Public Health. 2022; 19(19):12773. https://doi.org/10.3390/ijerph191912773
Chicago/Turabian StyleInokoshi, Masanao, Yumika Soeda, Yo Akiyama, Kaori Ueda, Kazumasa Kubota, and Shunsuke Minakuchi. 2022. "Fully Digital Workflow for the Fabrication of Three-Dimensionally Printed Surgical Splints for Preventing Postoperative Bleeding: A Case Report" International Journal of Environmental Research and Public Health 19, no. 19: 12773. https://doi.org/10.3390/ijerph191912773