
Impacts of Educational Interventions with Support of Mobile App versus Booklet for Patients with Hypertension and Metabolic Syndrome: A Secondary Data Analysis


 ,
,  ,
, 
Abstract
1. Introduction
Aims
2. Materials and Methods
2.1. Participants and Inclusion and Exclusion Criteria
2.2. Intervention Material
2.3. Data Collection
2.4. Outcvome Variables
2.5. Data Analysis
3. Results
3.1. Baseline Characteristics
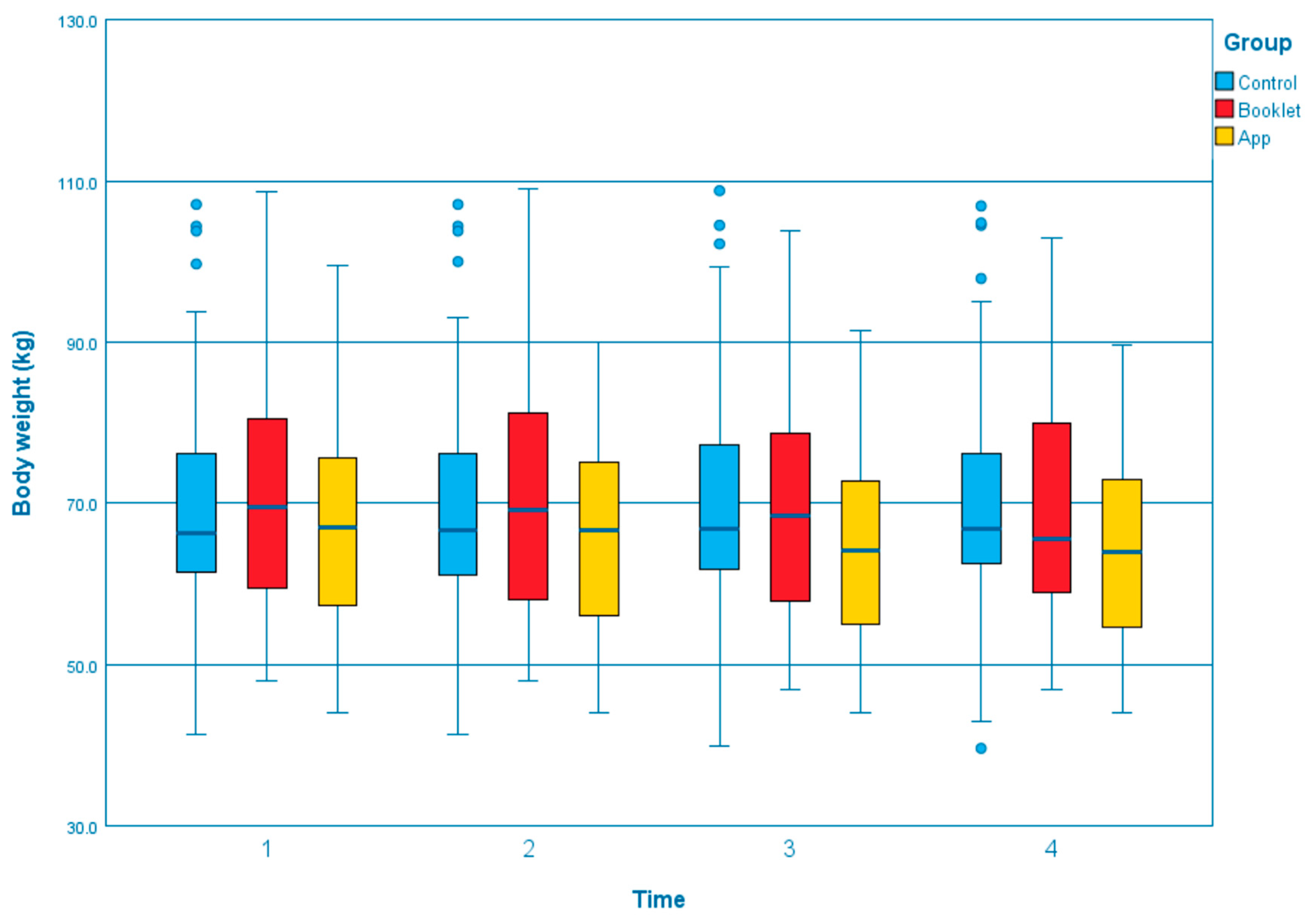
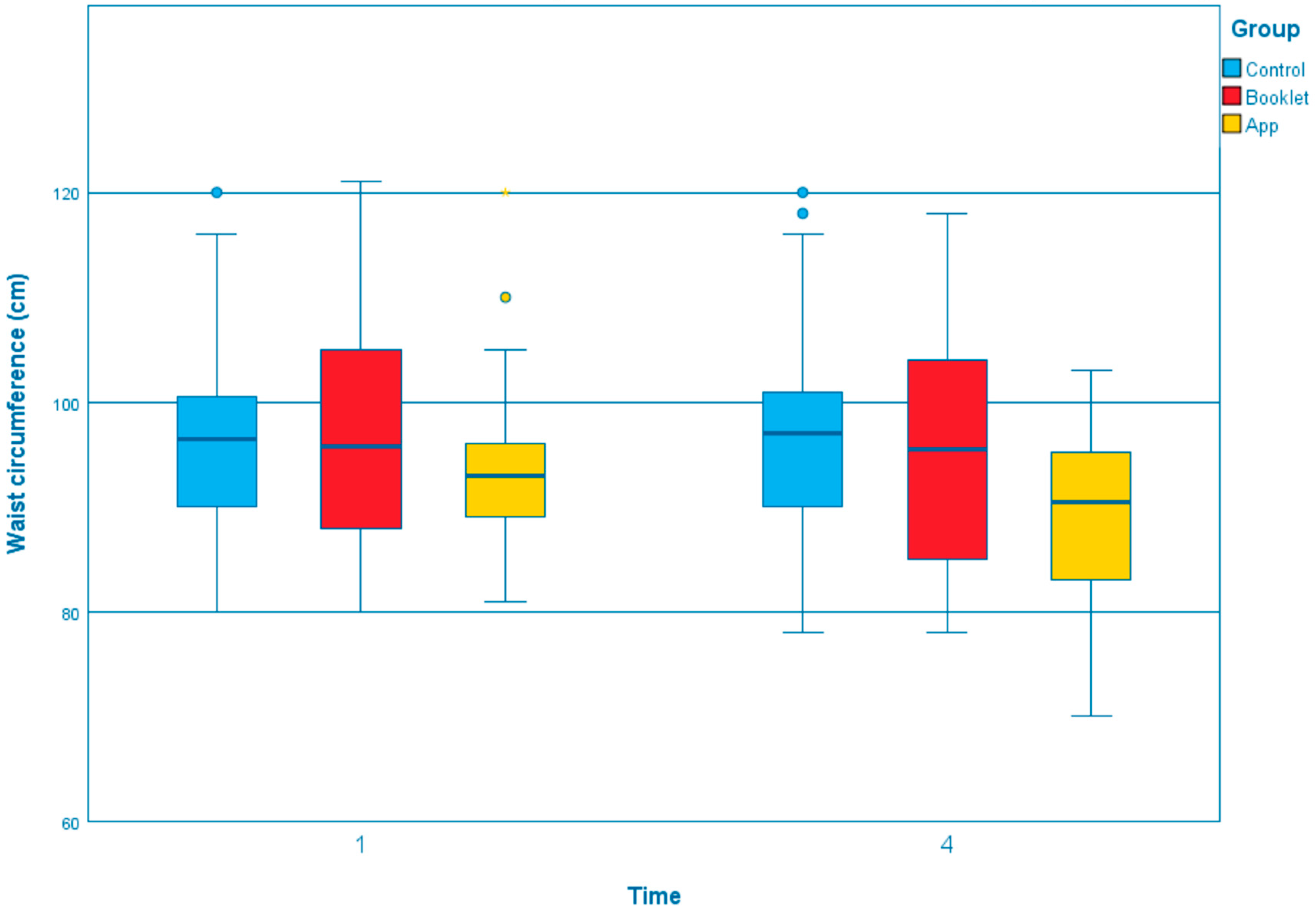
3.2. Efficacy of Different Interventions on Outcome Variables at Follow-Ups
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Consensus Worldwide Definition of the Metabolic Syndrome. Available online: https://www.idf.org/component/attachments/attachments.html?id=705&task=download (accessed on 18 July 2022).
- Leung, L.Y.L.; Chan, S.M.N.; Tam, H.L.; Wong, E.S.W. Astaxanthin Influence on Health Outcomes of Adults at Risk of Metabolic Syndrome: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2050. [Google Scholar] [CrossRef] [PubMed]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Lao, X.Q.; Ma, W.J.; Sobko, T.; Zhang, Y.H.; Xu, Y.J.; Xu, X.J.; Yu, D.M.; Nie, S.P.; Cai, Q.M.; Wei, X.L.; et al. Dramatic escalation in metabolic syndrome and cardiovascular risk in a Chinese population experiencing rapid economic development. BMC Public Health 2014, 14, 983. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.P.; Misra, A. Prevalence and trends of metabolic syndrome among adults in the asia-pacific region: A systematic review. BMC Public Health 2017, 17, 101. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- American Heart Association. What Is Metabolic Syndrome? Available online: https://www.heart.org/-/media/Files/Health-Topics/Answers-by-Heart/What-Is-Metabolic-Syndrome.pdf (accessed on 18 July 2022).
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar]
- Tam, H.L.; Wong, E.M.L.; Cheung, K. Effectiveness of Educational Interventions on Adherence to Lifestyle Modifications Among Hypertensive Patients: An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 2513. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chair, S.Y.; Wong, E.M.L. The effects of a lifestyle intervention program on physical outcomes, depression, and quality of life in adults with metabolic syndrome: A randomized clinical trial. Int. J. Cardiol. 2017, 230, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, K.; Tango, T. Effects of lifestyle modification on metabolic syndrome: A systematic review and meta-analysis. BMC Med. 2012, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Cheng, H.Y.; Cheng, L.; Sit, J.W.H. The effectiveness of electronic health interventions on blood pressure control, self-care behavioural outcomes and psychosocial well-being in patients with hypertension: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2019, 92, 27–46. [Google Scholar] [CrossRef]
- Wong, E.M.L.; Leung, D.Y.P.; Tam, H.L.; Wang, Q.; Yeung, K.W.; Leung, A.Y.M. The Effect of a Lifestyle Intervention Program Using a Mobile Application for Adults with Metabolic Syndrome, versus the Effect of a Program Using a Booklet: A Pilot Randomized Controlled Trial. Clin. Interv. Aging 2021, 16, 633–644. [Google Scholar] [CrossRef]
- Bassi, N.; Karagodin, I.; Wang, S.; Vassallo, P.; Priyanath, A.; Massaro, E.; Stone, N.J. Lifestyle modification for metabolic syndrome: A systematic review. Am. J. Med. 2014, 127, 1242.e1-10. [Google Scholar] [CrossRef]
- Jahangiry, L.; Montazeri, A.; Najafi, M.; Yaseri, M.; Farhangi, M. An interactive web-based intervention on nutritional status, physical activity and health-related quality of life in patients with metabolic syndrome: A randomized-controlled trial (The Red Ruby Study). Nutr. Diabetes 2017, 7, e240. [Google Scholar] [CrossRef]
- Wong, E.M.-L.; Leung, D.Y.P.; Chair, S.-Y.; Sit, J.W.H. Effects of a Web-Based Educational Support Intervention on Total Exercise and Cardiovascular Risk Markers in Adults With Coronary Heart Disease. Worldviews Evidence-Based Nurs. 2020, 17, 283–292. [Google Scholar] [CrossRef]
- Whitehead, L.; Seaton, P. The Effectiveness of Self-Management Mobile Phone and Tablet Apps in Long-term Condition Management: A Systematic Review. J. Med. Internet Res. 2016, 18, e97. [Google Scholar] [CrossRef]
- Wong, E.M.L.; Leung, D.Y.P.; Wang, Q.; Leung, A.Y.M. A nurse-led lifestyle intervention using mobile application versus booklet for adults with metabolic syndrome-Protocol for a randomized controlled trial. J. Adv. Nurs. 2020, 76, 364–372. [Google Scholar] [CrossRef]
- Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar]
- Leung, D.Y.P.; Lam, T.H.; Chan, S.S.C. Three versions of Perceived Stress Scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health 2010, 10, 513. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.L.; Perng, S.J.; Ho, C.C.; Hsu, H.M.; Lau, S.C.; Arthur, A. A preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adults. Int. J. Nurs. Stud. 2009, 46, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- LaPlante, C.; Peng, W. A Systematic Review of e-Health Interventions for Physical Activity: An Analysis of Study Design, Intervention Characteristics, and Outcomes. Telemed. e-Health 2011, 17, 509–523. [Google Scholar] [CrossRef]
- Korhonen, M.J.; Pentti, J.; Hartikainen, J.; Ilomaki, J.; Setoguchi, S.; Liew, D.; Kivimaki, M.; Vahtera, J. Lifestyle Changes in Relation to Initiation of Antihypertensive and Lipid-Lowering Medication: A Cohort Study. J. Am. Hear. Assoc. 2020, 9, e014168. [Google Scholar] [CrossRef]
- Tam, H.L.; Chung, S.F.; Wang, Q. Urban-rural disparities in hypertension management among middle-aged and older patients: Results of a 2018 Chinese national study. Chronic Illn. 2022. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf (accessed on 20 July 2022).
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef]
- Morrissey, E.C.; Casey, M.; Glynn, L.G.; Walsh, J.C.; Molloy, G.J. Smartphone apps for improving medication adherence in hypertension: Patients’ perspectives. Patient Prefer. Adher. 2018, 12, 813–822. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | App Group (n = 36) | Booklet Group (n = 42) | Control Group (n = 40) | p-Value |
|---|---|---|---|---|
| Age in years (SD) | 66.94 (10.51) | 64.07 (7.02) | 66.35 (10.04) | 0.344 |
| Sex | 0.156 | |||
| Male | 15 | 11 | 9 | |
| Female | 21 | 31 | 31 | |
| Education level | 0.09 | |||
| Primary school or below | 9 | 5 | 13 | |
| Secondary school | 16 | 29 | 20 | |
| Tertiary education | 11 | 8 | 7 | |
| Marital Status | 0.113 | |||
| Married | 25 | 26 | 21 | |
| Not married | 7 | 6 | 4 | |
| Separated/Divorced/Widow | 4 | 10 | 15 | |
| Employment status | 0.207 | |||
| Full-time job | 7 | 6 | 10 | |
| Part-time job | 3 | 6 | 1 | |
| Housewife | 3 | 10 | 6 | |
| Retired/Others | 23 | 20 | 23 | |
| Financial status | 0.118 | |||
| Good | 7 | 3 | 7 | |
| Average | 23 | 34 | 22 | |
| Poor | 6 | 5 | 11 | |
| Residential status | 0.106 | |||
| Live alone | 5 | 11 | 14 | |
| Live with family | 31 | 31 | 26 | |
| Smoking status | 0.607 | |||
| Current smoker | 0 | 0 | 1 | |
| Quitted | 3 | 6 | 4 | |
| Never smoked | 33 | 36 | 35 | |
| Outcome variables (SD) | ||||
| Body weight | 67.01 (12.76) | 71.06 (14.88) | 69.91 (15.41) | 0.455 |
| GSLTPAQ | 17.18 (11.14) | 18.07 (17.69) | 16.97 (18.72) | 0.949 |
| Waist circumference | 93.51 (8.30) | 96.99 (10.44) | 96.25 (9.41) | 0.247 |
| Systolic blood pressure | 136.83 (15.07) | 136.85 (14.51) | 132.70 (13.76) | 0.339 |
| Diastolic blood pressure | 83.42 (10.17) | 85.86 (6.77) | 79.05 (10.63) | 0.004 |
| Total cholesterol | 4.68 (1.11) | 4.91 (1.27) | 4.49 (0.93) | 0.233 |
| HDL cholesterol | 1.36 (0.33) | 1.35 (0.34) | 1.39 (0.31) | 0.846 |
| LDL cholesterol | 2.55 (0.98) | 2.70 (1.02) | 2.32 (0.91) | 0.213 |
| Triacylglycerols | 1.65 (0.77) | 1.85 (0.82) | 1.67 (0.72) | 0.443 |
| Fasting blood sugar | 5.97 (0.70) | 6.21 (1.43) | 6.39 (2.02) | 0.465 |
| 3-min step test | 4.19 (1.39) | 3.95 (1.28) | 4.45 (1.53) | 0.281 |
| Perceived stress scale | 13.58 (5.54) | 15.66 (4.54) | 15.77 (6.02) | 0.143 |
| Self-efficacy for exercise scale | 4.95 (1.81) | 4.24 (1.71) | 4.76 (2.04) | 0.21 |
| Variables | Cohen’s d | ||
|---|---|---|---|
| App vs. Control | Booklet vs. Control | App vs. Booklet | |
| Body weight | −0.673 | −0.294 | −0.360 |
| Godin-Shephard Leisure-Time Physical Activity Questionnaire | 0.495 | −0.074 | 0.910 |
| Waist circumference | −1.197 | −0.488 | −0.587 |
| Systolic blood pressure | −0.005 | 0.009 | −0.012 |
| Diastolic blood pressure | −0.156 | −0.296 | 0.111 |
| Total cholesterol | −0.349 | −0.421 | 0.038 |
| High density lipoprotein (HDL) cholesterol | 0.022 | −0.241 | 0.239 |
| Low density lipoprotein (LDL) cholesterol | −0.727 | −0.248 | −0.310 |
| Triacylglycerols | 0.301 | 0.090 | 0.160 |
| Fasting blood sugar | 0.177 | 0.151 | 0.056 |
| 3-min step test | 0.015 | 0.027 | −0.011 |
| Perceived stress scale | 0.038 | −0.344 | 0.600 |
| Self-efficacy for exercise scale | 0.256 | 0.118 | 0.173 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, E.M.L.; Tam, H.L.; Leung, A.Y.M.; Cheung, A.S.P.; Cheung, K.C.; Leung, D.Y.P. Impacts of Educational Interventions with Support of Mobile App versus Booklet for Patients with Hypertension and Metabolic Syndrome: A Secondary Data Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12591. https://doi.org/10.3390/ijerph191912591
Wong EML, Tam HL, Leung AYM, Cheung ASP, Cheung KC, Leung DYP. Impacts of Educational Interventions with Support of Mobile App versus Booklet for Patients with Hypertension and Metabolic Syndrome: A Secondary Data Analysis. International Journal of Environmental Research and Public Health. 2022; 19(19):12591. https://doi.org/10.3390/ijerph191912591
Chicago/Turabian StyleWong, Eliza Mi Ling, Hon Lon Tam, Angela Yee Man Leung, Alice Siu Ping Cheung, Ka Ching Cheung, and Doris Yin Ping Leung. 2022. "Impacts of Educational Interventions with Support of Mobile App versus Booklet for Patients with Hypertension and Metabolic Syndrome: A Secondary Data Analysis" International Journal of Environmental Research and Public Health 19, no. 19: 12591. https://doi.org/10.3390/ijerph191912591
APA StyleWong, E. M. L., Tam, H. L., Leung, A. Y. M., Cheung, A. S. P., Cheung, K. C., & Leung, D. Y. P. (2022). Impacts of Educational Interventions with Support of Mobile App versus Booklet for Patients with Hypertension and Metabolic Syndrome: A Secondary Data Analysis. International Journal of Environmental Research and Public Health, 19(19), 12591. https://doi.org/10.3390/ijerph191912591