
The Effectiveness of Interventions to Increase Participation and Physical Activities in Parks: A Systematic Review of the Literature


Abstract
:1. Introduction
2. Methods
2.1. Peer-Reviewed Literature
- (a)
- In English;
- (b)
- A peer-reviewed and published journal article;
- (c)
- Full text available for review;
- (d)
- Relevant to park visitation or physical activities in parks.
2.2. Evidence Grading
3. Results
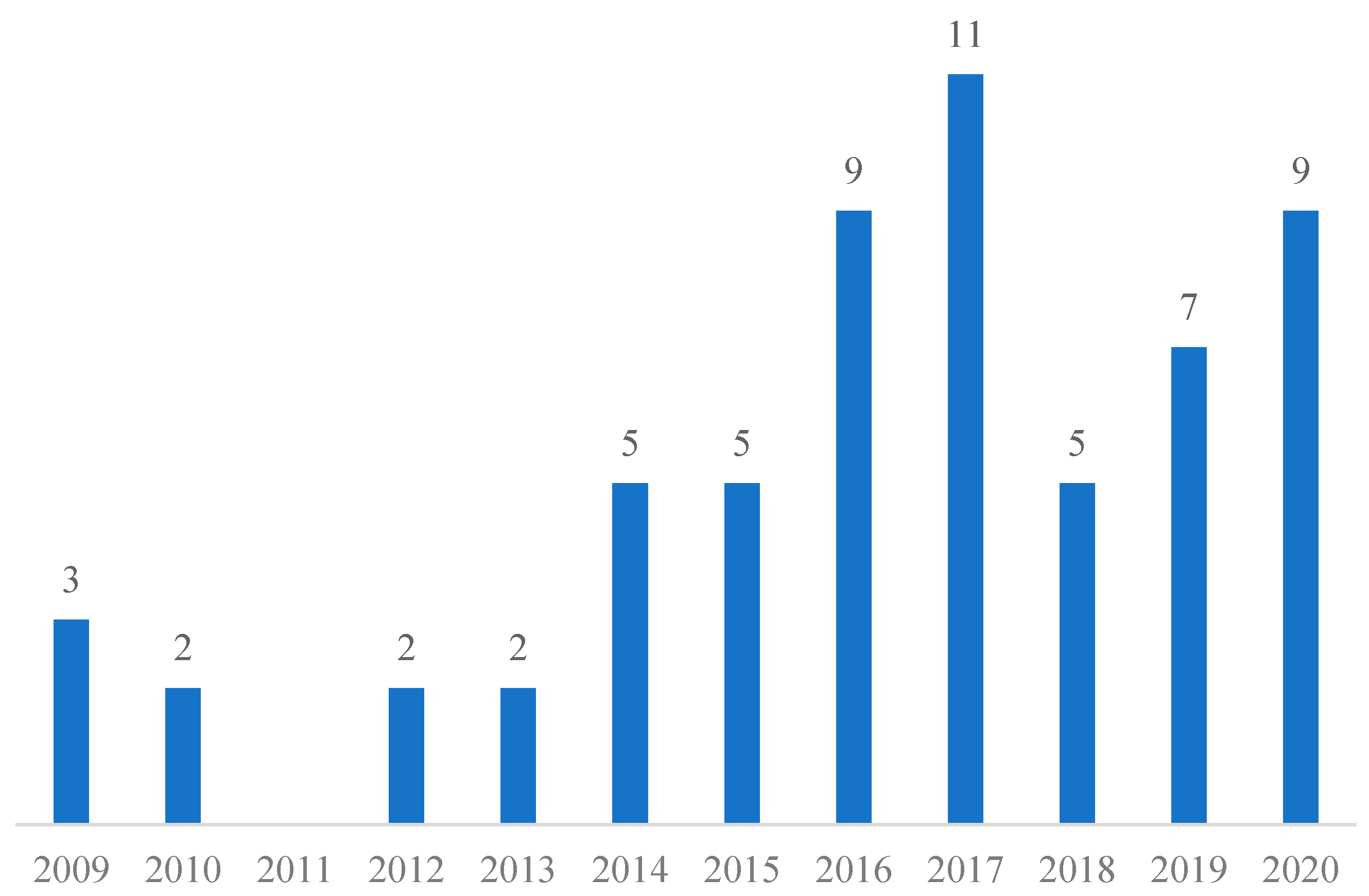
3.1. An Overview of Systematic Review Publications
3.2. Study Design
3.3. Population of Interest
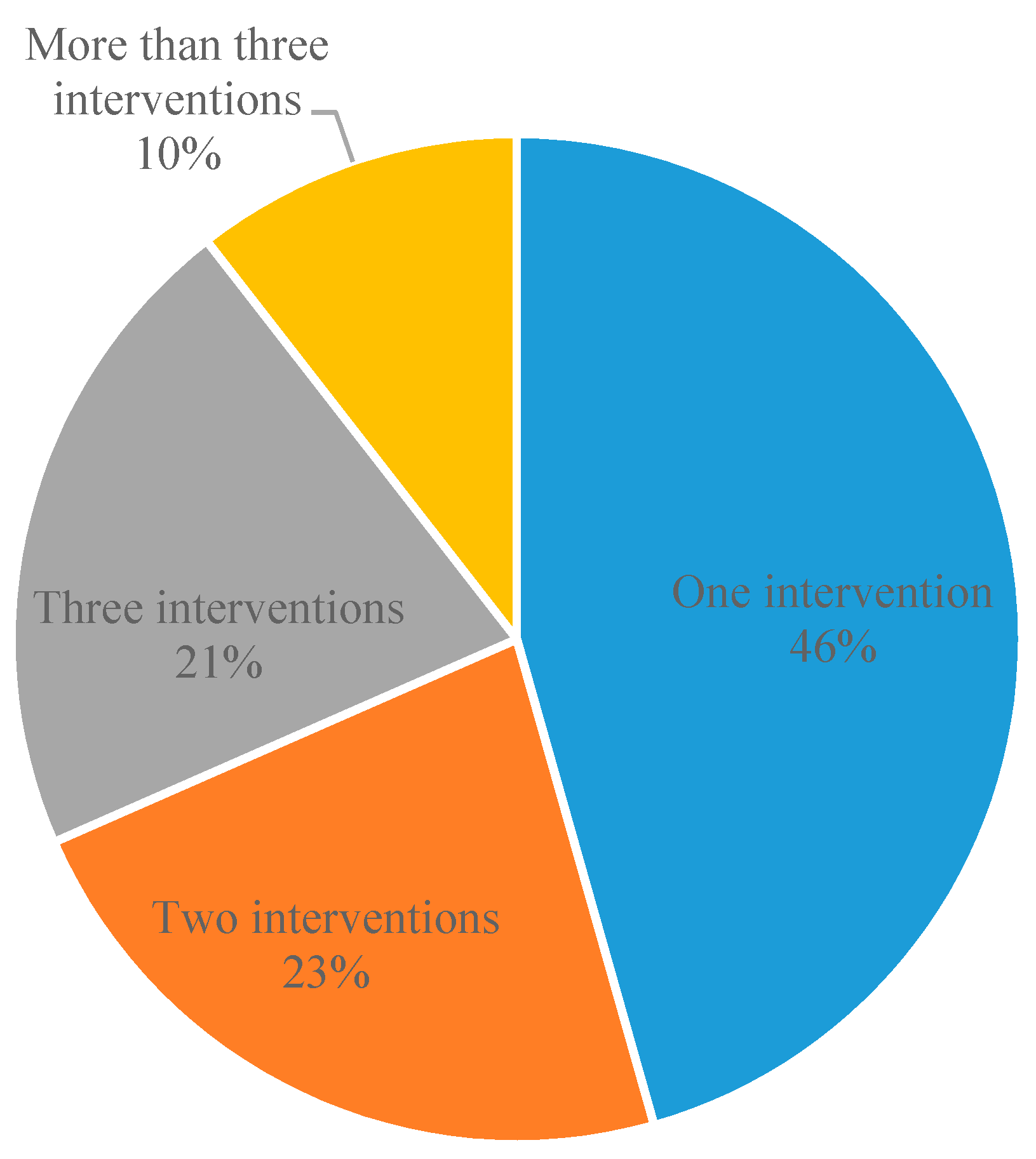
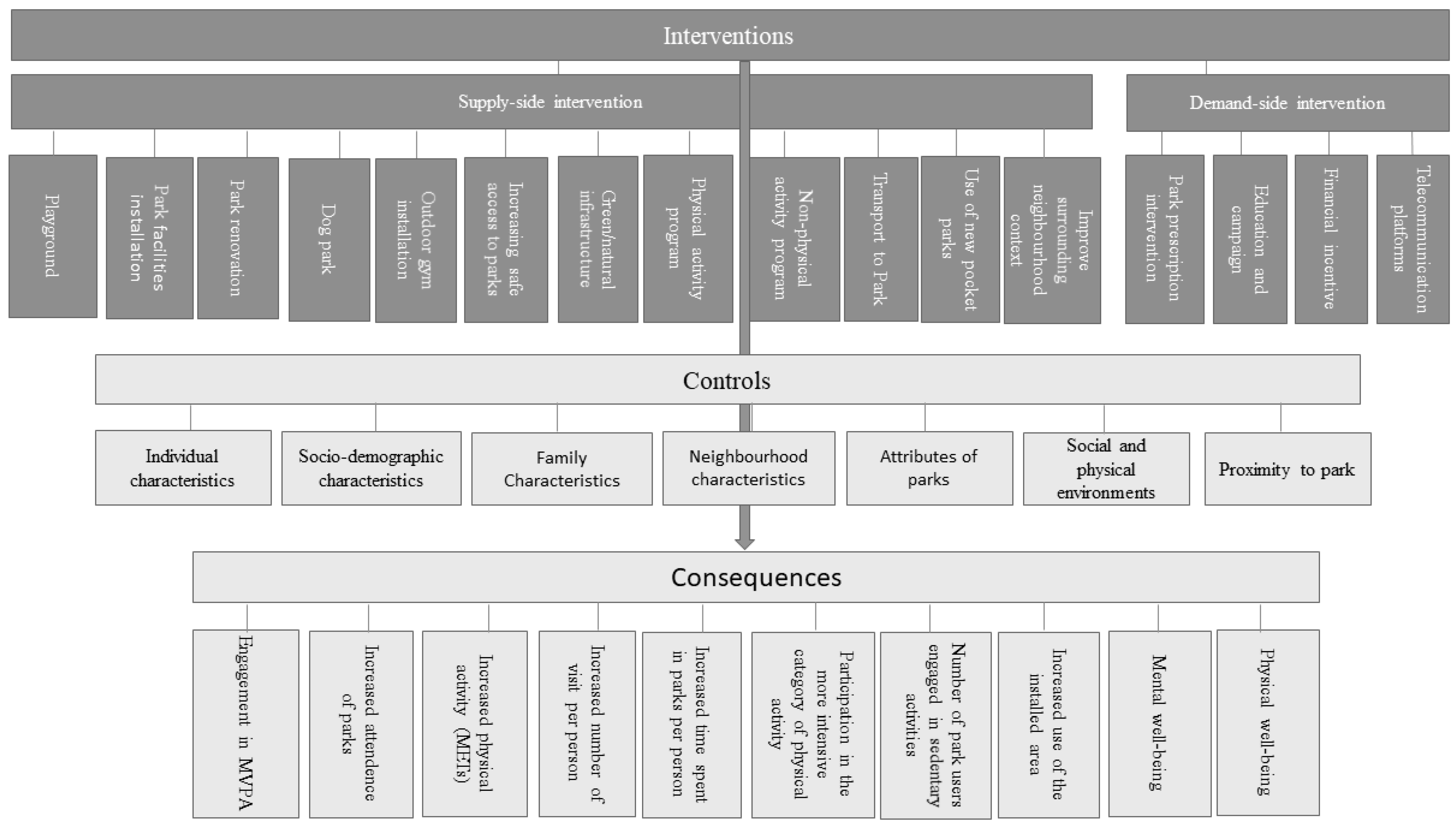
3.4. Type of Interventions
3.5. Outcome Measures and Impacts of Interventions
3.6. Risk of Bias
3.7. GRADE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sallis, J.A. Proportional public health response to physical inactivity. J. Public Health Manag. Pract. 2012, 18, 399–401. [Google Scholar] [CrossRef]
- Hallal, P.; Bauman, A.; Heath, G.; Kohl, H.; Lee, I.; Pratt, M. Physical activity: More of the same is not enough. Lancet 2012, 380, 190–191. [Google Scholar] [CrossRef]
- Renalds, A.; Smith, T.H.; Hale, P.J. A Systematic Review of Built Environment and Health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Sturm, R.; Cohen, D. Proximity to urban parks and mental health. J. Ment. Health Policy Econ. 2014, 17, 19. [Google Scholar] [PubMed]
- Wood, L.; Hooper, P.; Foster, S.; Bull, F. Public green spaces and positive mental health—Investigating the relationship between access, quantity and types of parks and mental wellbeing. Health Place 2017, 48, 63–71. [Google Scholar] [CrossRef]
- Orstad, S.L.; Szuhany, K.; Tamura, K.; Thorpe, L.E.; Jay, M. Park Proximity and Use for Physical Activity among Urban Residents: Associations with Mental Health. Int. J. Environ. Res. Public Heal. 2020, 17, 4885. [Google Scholar] [CrossRef]
- Aliyas, Z. Does social environment mediate the association between perceived safety and physical activity among adults living in low socioeconomic neighborhoods? J. Transp. Health 2019, 14, 100578. [Google Scholar] [CrossRef]
- Stanis, S.A.W.; Schneider, I.E.; Pereira, M.A. Parks and Health: Differences in Constraints and Negotiation Strategies for Park-Based Leisure Time Physical Activity by Stage of Change. J. Phys. Act. Health 2010, 7, 273–284. [Google Scholar] [CrossRef]
- Veitch, J.; Carver, A.; Abbott, G.; Giles-Corti, B.; Timperio, A.; Salmon, J. How active are people in metropolitan parks? An observational study of park visitation in Australia. BMC Public Health 2015, 15, 610. [Google Scholar] [CrossRef] [Green Version]
- Chow, B.C.; McKenzie, T.L.; Sit, C.H.P. Public Parks in Hong Kong: Characteristics of Physical Activity Areas and Their Users. Int. J. Environ. Res. Public Health 2016, 13, 639. [Google Scholar] [CrossRef]
- Farías-Torbidoni, E.; Barić, D.; Mas-Alòs, S. Assessing the Influence of Visitors’ Sociodemographic and Trip Characteristics on Physical Activity Intensities in Alt Pirineu Natural Park, Spain. J. Phys. Act. Health 2018, 15, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Veitch, J.; Salmon, J.; Crawford, D.; Abbott, G.; Giles-Corti, B.; Carver, A.; Timperio, A. The REVAMP natural experiment study: The impact of a play-scape installation on park visitation and park-based physical activity. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.; French, S.A.; Das, K.V. Family Structure and Park Use Among Parents. Am. J. Prev. Med. 2012, 43, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Van Nes, A.; López, M. Spatio-socio classification of deprived neighbourhouds in the Netherlands. Strategies for neighbourhood revitalization. In Proceedings of the Ninth International Space Syntax Symposium, Seoul, Korea, 31 October–3 November 2013. [Google Scholar]
- Babey, S.H.; Tan, D.; Wolstein, J.; Diamant, A.L. Neighborhood, family and individual characteristics related to adolescent park-based physical activity. Prev. Med. 2015, 76, 31–36. [Google Scholar] [CrossRef]
- Huang, J.; Hipp, J.; Marquet, O.; Alberico, C.; Fry, D.; Mazak, E.; Lovasi, G.S.; Robinson, W.R.; Floyd, M.F. Neighborhood characteristics associated with park use and park-based physical activity among children in low-income diverse neighborhoods in New York City. Prev. Med. 2020, 131, 105948. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Park, M.; Wallace, J.P. The impact of perceived social support, loneliness, and physical activity on quality of life in South Korean older adults. J. Sport Heal. Sci. 2016, 7, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Crespo-Cebada, E.; Díaz-Caro, C.; Robina-Ramírez, R.; Sánchez-Hernández, M.I. Is Biodiversity a Relevant Attribute for Assessing Natural Parks? Evidence from Cornalvo Natural Park in Spain. Forests 2020, 11, 410. [Google Scholar] [CrossRef] [Green Version]
- Dias, A.; Gaya, A.; Brand, C.; Pizarro, A.I.; Fochesatto, C.F.; Mendes, T.M.; Mota, J.; Santos, M.M.; Gaya, A.C.A. Distance from home to the nearest park and the use of the parks for physical activity: The mediator role of road safety perception in adolescents. Public Health 2019, 168, 9–16. [Google Scholar] [CrossRef]
- McCormack, G.R.; Rock, M.; Toohey, A.M.; Hignell, D. Characteristics of urban parks associated with park use and physical activity: A review of qualitative research. Health Place 2010, 16, 712–726. [Google Scholar] [CrossRef]
- Floyd, M.F.; Taylor, W.C.; Whitt-Glover, M. Measurement of Park and Recreation Environments That Support Physical Activity in Low-Income Communities of Color: Highlights of Challenges and Recommendations. Am. J. Prev. Med. 2009, 36, S156–S160. [Google Scholar] [CrossRef]
- Park, C.; Song, H. Visitors’ Perceived Place Value and the Willingness to Pay in an Urban Lake Park. Int. J. Environ. Res. Public Health 2018, 15, 2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan-Basri, B.; Karim, M.Z.A. Can Benefits in Recreational Parks in Malaysia Be Transferred? A Choice Experiment (CE) Technique. Int. J. Tour. Res. 2014, 18, 19–26. [Google Scholar] [CrossRef]
- Parra, D.C.; Van Zandt, A.; Wang, P.; Goodman, M.; Abhishek, J.; Haire-Joshu, D.; Brownson, R.C. Evaluating Park Use and Satisfaction: The Case of Trojan Park in St. Louis Missouri. Int. J. Environ. Res. Public Health 2019, 16, 2798. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.A.; Ashwood, J.S.; Scott, M.M.; Overton, A.; Evenson, K.R.; Staten, L.K.; Porter, D.; McKenzie, T.L.; Catellier, D. Public Parks and Physical Activity among Adolescent Girls. Pediatrics 2006, 118, e1381–e1389. [Google Scholar] [CrossRef] [Green Version]
- Ou, J.Y.; Levy, J.I.; Peters, J.L.; Bongiovanni, R.; Garcia-Soto, J.; Medina, R.; Scammell, M.K. A Walk in the Park: The Influence of Urban Parks and Community Violence on Physical Activity in Chelsea, MA. Int. J. Environ. Res. Public Health 2016, 13, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burrows, E.; O’Mahony, M.; Geraghty, D. How Urban Parks Offer Opportunities for Physical Activity in Dublin, Ireland. Int. J. Environ. Res. Public Health 2018, 15, 815. [Google Scholar] [CrossRef] [Green Version]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health: A conceptual model. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef]
- Wallace, D.D.; Derose, K.P.; Han, B.; Cohen, D.A. The effects of park-based interventions on health: A systematic review protocol. Syst. Rev. 2020, 9, 135. [Google Scholar] [CrossRef]
- Roberts, H.; McEachan, R.; Margary, T.; Conner, M.; Kellar, I. Identifying Effective Behavior Change Techniques in Built Environment Interventions to Increase Use of Green Space: A Systematic Review. Environ. Behav. 2016, 50, 28–55. [Google Scholar] [CrossRef]
- Zhang, R.; Wulff, H.; Duan, Y.; Wagner, P. Associations between the physical environment and park-based physical activity: A systematic review. J. Sport Health Sci. 2019, 8, 412–421. [Google Scholar] [CrossRef]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; Macmillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.F.; Christian, H.; Veitch, J.; Astell-Burt, T.; Hipp, J.; Schipperijn, J. The impact of interventions to promote physical activity in urban green space: A systematic review and recommendations for future research. Soc. Sci. Med. 2015, 124, 246–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, R.; Cleland, C.; Cleary, A.; Droomers, M.; Wheeler, B.W.; Sinnett, D.; Nieuwenhuijsen, M.J.; Braubach, M. Environmental, health, wellbeing, social and equity effects of urban green space interventions: A meta-narrative evidence synthesis. Environ. Int. 2019, 130, 104923. [Google Scholar] [CrossRef]
- Audrey, S.; Batista-Ferrer, H. Healthy urban environments for children and young people: A systematic review of intervention studies. Health Place 2015, 36, 97–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derose, K.P.; Wallace, D.D.; Han, B.; Cohen, D.A. Effects of park-based interventions on health-related outcomes: A systematic review. Prev. Med. 2021, 147, 106528. [Google Scholar] [CrossRef]
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Sterne, J.; Higgins, J.; Reeves, B.; On behalf of the development group for ACROBAT-NRSI. A Cochrane RISK of Bias Assessment Tool: For Non-Randomized Studies of Interventions (ACROBAT-NRSI). version 1.0; Available online: https://www.bristol.ac.uk/media-library/sites/social-community-medicine/images/centres/cresyda/ACROBAT-NRSI%20Version%201_0_0.pdf (accessed on 30 September 2022).
- Bohn-Goldbaum, E.E.; Phongsavan, P.; Merom, D.; Rogers, K.; Kamalesh, V.; Bauman, A.E. Does Playground Improvement Increase Physical Activity among Children? A Quasi-Experimental Study of a Natural Experiment. J. Environ. Public Health 2013, 2013, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.A.; Golinelli, D.; Williamson, S.; Sehgal, A.; Marsh, T.; McKenzie, T.L. Effects of Park Improvements on Park Use and Physical Activity: Policy and Programming Implications. Am. J. Prev. Med. 2009, 37, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Pawlowski, C.S.; Schmidt, T.; Nielsen, J.V.; Troelsen, J.; Schipperijn, J. Will the children use it?—A RE-AIM evaluation of a local public open space intervention involving children from a deprived neighbourhood. Evaluation Program Plan. 2019, 77, 101706. [Google Scholar] [CrossRef]
- Razani, N.; Hills, N.K.; Thompson, D.; Rutherford, G.W. The Association of Knowledge, Attitudes and Access with Park Use before and after a Park-Prescription Intervention for Low-Income Families in the U.S. Int. J. Environ. Res. Public Health 2020, 17, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fair, M.L.; Kaczynski, A.T.; Hughey, S.M.; Besenyi, G.M.; Powers, A.R. An Initiative to Facilitate Park Usage, Discovery, and Physical Activity Among Children and Adolescents in Greenville County, South Carolina, 2014. Prev. Chronic Dis. 2017, 14, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balcázar, H.G.; de Heer, H.D.; Thomas, S.W.; Redelfs, A.; Rosenthal, E.L.; Burgos, X.; Duarte, M.O. Promotoras Can Facilitate Use of Recreational Community Resources. Health Promot. Pr. 2015, 17, 343–352. [Google Scholar] [CrossRef]
- Copeland, J.L.; Currie, C.; Walker, A.; Mason, E.; Willoughby, T.N.; Amson, A. Fitness Equipment in Public Parks: Frequency of Use and Community Perceptions in a Small Urban Centre. J. Phys. Act. Health 2017, 14, 344–352. [Google Scholar] [CrossRef]
- Kubota, A.; Matsushita, M.; Smith, B.J.; Sugiyama, T.; Arao, T. The impact of a new exercise facility on physical activity at the community level: A non-randomized panel study in Japan. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Droomers, M.; Jongeneel-Grimen, B.; Kramer, D.; de Vries, S.; Kremers, S.; Bruggink, J.-W.; van Oers, H.; Kunst, A.E.; Stronks, K. The impact of intervening in green space in Dutch deprived neighbourhoods on physical activity and general health: Results from the quasi-experimental URBAN40 study. J. Epidemiology Community Health 2015, 70, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller-Riemenschneider, F.; Petrunoff, N.; Yao, J.; Ng, A.; Sia, A.; Ramiah, A.; Wong, M.; Han, J.; Tai, B.C.; Uijtdewilligen, L. Effectiveness of prescribing physical activity in parks to improve health and wellbeing - the park prescription randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13, e0192921. [Google Scholar] [CrossRef] [Green Version]
- Gagliardi, C.; Pillemer, K.; Gambella, E.; Piccinini, F.; Fabbietti, P. Benefits for Older People Engaged in Environmental Volunteering and Socializing Activities in City Parks: Preliminary Results of a Program in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3772. [Google Scholar] [CrossRef]
- Cohen, D.A.; Sehgal, A.; Williamson, S.; Marsh, T.; Golinelli, D.; McKenzie, T.L. New Recreational Facilities for the Young and the Old in Los Angeles: Policy and Programming Implications. J. Public Health Policy 2009, 30, S248–S263. [Google Scholar] [CrossRef]
- Cohen, D.A.; Marsh, T.; Williamson, S.; Derose, K.P.; Martinez, H.; Setodji, C.; McKenzie, T.L. Parks and physical activity: Why are some parks used more than others? Prev. Med. 2010, 50, S9–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, D.A.; Marsh, T.; Williamson, S.; Golinelli, D.; McKenzie, T.L. Impact and cost-effectiveness of family Fitness Zones: A natural experiment in urban public parks. Health Place 2012, 18, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.; Han, B.; Derose, K.; Williamson, S.; Marsh, T.; Raaen, L.; McKenzie, T.L. The Paradox of Parks in Low-Income Areas. Environ. Behav. 2016, 48, 230–245. [Google Scholar] [CrossRef]
- Foster, S.; Giles-Corti, B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. Prev. Med. 2008, 47, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Han, B.; Isacoff, J.; Shulaker, B.; Williamson, S.; Marsh, T.; McKenzie, T.L.; Weir, M.; Bhatia, R. Impact of Park Renovations on Park Use and Park-Based Physical Activity. J. Phys. Act. Health 2015, 12, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Schultz, C.L.; Stanis, S.A.W.; Sayers, S.P.; Thombs, L.A.; Thomas, I.M. A longitudinal examination of improved access on park use and physical activity in a low-income and majority African American neighborhood park. Prev. Med. 2017, 95, S95–S100. [Google Scholar] [CrossRef]
- Tester, J.; Baker, R. Making the playfields even: Evaluating the impact of an environmental intervention on park use and physical activity. Prev. Med. 2009, 48, 316–320. [Google Scholar] [CrossRef]
- Richardson, A.S.; Ghosh-Dastidar, M.; Collins, R.L.; Hunter, G.P.; Troxel, W.M.; Colabianchi, N.; Cohen, D.A.; Dubowitz, T. Improved Street Walkability, Incivilities, and Esthetics Are Associated with Greater Park Use in Two Low-Income Neighborhoods. J. Urban Health 2020, 97, 204–212. [Google Scholar] [CrossRef]
- Han, B.; Cohen, D.A.; Derose, K.P.; Marsh, T.; Williamson, S.; Loy, S. Effectiveness of a free exercise program in a neighborhood park. Prev. Med. Rep. 2015, 2, 255–258. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.A.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; Raaen, L.; McKenzie, T.L. Promoting physical activity in high-poverty neighborhood parks: A cluster randomized controlled trial. Soc. Sci. Med. 2017, 186, 130–138. [Google Scholar] [CrossRef]
- Torres, A.; Díaz, M.P.; Hayat, M.J.; Lyn, R.; Pratt, M.; Salvo, D.; Sarmiento, O.L. Assessing the effect of physical activity classes in public spaces on leisure-time physical activity: “Al Ritmo de las Comunidades” A natural experiment in Bogota, Colombia. Prev. Med. 2017, 103, S51–S58. [Google Scholar] [CrossRef]
- Hoffman, J.; Frerichs, L.; Story, M.; Jones, J.; Gaskin, K.; Apple, A.; Skinner, A.; Armstrong, S. An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial. Pediatrics 2018, 141, e20171444. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.A.; Marsh, T.; Williamson, S.; Han, B.; Derose, K.P.; Golinelli, D.; McKenzie, T.L. The Potential for Pocket Parks to Increase Physical Activity. Am. J. Health Promot. 2014, 28, S19–S26. [Google Scholar] [CrossRef] [Green Version]
- Dobbinson, S.; Simmons, J.; Chamberlain, J.; MacInnis, R.J.; Salmon, J.; Staiger, P.K.; Wakefield, M.; Veitch, J. Examining Health-Related Effects of Refurbishment to Parks in a Lower Socioeconomic Area: The ShadePlus Natural Experiment. Int. J. Environ. Res. Public Heal. 2020, 17, 6102. [Google Scholar] [CrossRef]
- Middle, I. Between a dog and a green space: Applying ecosystem services theory to explore the human benefits of off-the-leash dog parks. Landsc. Res. 2019, 45, 81–94. [Google Scholar] [CrossRef]
- Pearson, A.L.; Pfeiffer, K.A.; Gardiner, J.; Horton, T.; Buxton, R.T.; Hunter, R.F.; Breeze, V.; McDade, T. Study of active neighborhoods in Detroit (StAND): Study protocol for a natural experiment evaluating the health benefits of ecological restoration of parks. BMC Public Heal. 2020, 20, 638. [Google Scholar] [CrossRef] [PubMed]
- Schoffman, D.E.; Kaczynski, A.T.; Forthofer, M.; Wilcox, S.; Hutto, B.; Child, S.T.; Hughey, S.M. Longitudinal associations with changes in outdoor recreation area use for physical activity during a community-based intervention. Prev. Med. 2015, 78, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Austin, G.; Duncan, M.J.; Bell, T. Codesigning Parks for Increasing Park Visits and Physical Activity in a Low-Socioeconomic Community: The Active By Community Design Experience. Health Promot. Pract. 2020, 22, 338–348. [Google Scholar] [CrossRef]
- Banda, J.A.; Hooker, S.; Wilcox, S.; Colabianchi, N.; Kaczynski, A.T.; Hussey, J. The Effects of a Park Awareness Campaign on Rural Park Use and Physical Activity. J. Public Health Manag. Pract. 2017, 23, e25–e28. [Google Scholar] [CrossRef]
- Jansson, A.; Lubans, D.; Smith, J.; Duncan, M.; Bauman, A.; Attia, J.; Robards, S.; Plotnikoff, R. Integrating Smartphone Technology, Social Support and The Outdoor Built Environment to Promote Community-Based Aerobic And Resistance-Based Physical Activity: Rationale And Study Protocol For The ‘Ecofit’ Randomized Controlled Trial. Contemp. Clin. Trials Commun. 2019, 16, 100457. [Google Scholar] [CrossRef]
- Benton, J.S.; Anderson, J.; Hunter, R.F.; French, D.P. The effect of changing the built environment on physical activity: A quantitative review of the risk of bias in natural experiments. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocarro, J.N.; Floyd, M.F.; Smith, W.R.; Edwards, M.B.; Schultz, C.L.; Baran, P.; Moore, R.A.; Cosco, N.; Suau, L.J. Social and Environmental Factors Related to Boys’ and Girls’ Park-Based Physical Activity. Prev. Chronic Dis. 2015, 12, E97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehner, C.M.; Brownson, R.C.; Allen, D.; Gramann, J.; Behrens, T.K.; Floyd, M.F.; Leahy, J.; Liddle, J.B.; Smaldone, D.; Spain, D.D.; et al. Parks Promoting Physical Activity: Synthesis of Findings from Interventions in Seven National Parks. J. Phys. Act. Health 2010, 7, S67–S81. [Google Scholar] [CrossRef] [PubMed]
- Kaczynski, A.T.; Stanis, S.A.W.; Hipp, J.A. Point-of-decision prompts for increasing park-based physical activity: A crowdsource analysis. Prev. Med. 2014, 69, 87–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpe, P.A.; Burroughs, E.L.; Granner, M.L.; Wilcox, S.; Hutto, B.E.; Bryant, C.A.; Peck, L.; Pekuri, L. Impact of a Community-Based Prevention Marketing Intervention to Promote Physical Activity Among Middle-Aged Women. Health Educ. Behav. 2009, 37, 403–423. [Google Scholar] [CrossRef]
- Buller, D.B.; English, D.R.; Buller, M.K.; Simmons, J.; Chamberlain, J.A.; Wakefield, M.; Dobbinson, S. Shade Sails and Passive Recreation in Public Parks of Melbourne and Denver: A Randomized Intervention. Am. J. Public Health 2017, 107, 1869–1875. [Google Scholar] [CrossRef]
- Lal, A.; Moodie, M.; Abbott, G.; Carver, A.; Salmon, J.; Giles-Corti, B.; Timperio, A.; Veitch, J. The impact of a park refurbishment in a low socioeconomic area on physical activity: A cost-effectiveness study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Veitch, J.; Ball, K.; Crawford, D.; Abbott, G.R.; Salmon, J. Park Improvements and Park Activity. Am. J. Prev. Med. 2012, 42, 616–619. [Google Scholar] [CrossRef] [Green Version]
- Roemmich, J.N.; Beeler, J.E.; Johnson, L. A microenvironment approach to reducing sedentary time and increasing physical activity of children and adults at a playground. Prev. Med. 2014, 62, 108–112. [Google Scholar] [CrossRef]
- Slater, S.; Pugach, O.; Lin, W.; Bontu, A. If You Build It Will They Come? Does Involving Community Groups in Playground Renovations Affect Park Utilization and Physical Activity? Environ. Behav. 2016, 48, 246–265. [Google Scholar] [CrossRef]
- Sami, M.; Smith, M.; Ogunseitan, O.A. Changes in Physical Activity after Installation of a Fitness Zone in a Community Park. Prev. Chronic Dis. 2018, 15, E101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sami, M.; Smith, M.; Ogunseitan, O.A. Placement of Outdoor Exercise Equipment and Physical Activity: A Quasi-Experimental Study in Two Parks in Southern California. Int. J. Environ. Res. Public Health 2020, 17, 2605. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country/Region | Number of Studies |
|---|---|
| USA | 33 |
| Australia | 16 |
| Canada | 3 |
| Singapore | 2 |
| Colombia | 2 |
| Japan | 1 |
| Netherlands | 1 |
| Denmark | 1 |
| Italy | 1 |
| Belgium | 1 |
| England | 1 |
| Scotland | 1 |
| New Zealand | 1 |
| Total | 64 |
| Study Design | Number of Studies |
|---|---|
| Randomised controlled trial | 12 |
| Quasi-experimental pre–post evaluation design with a comparison group | 27 |
| Quasi-experimental pre–post evaluation design without a parallel comparison group | 14 |
| Case study | 3 |
| Systematic reviews | 4 |
| Population of Interest | Number of Studies |
|---|---|
| Whole population | 28 |
| Children | 6 |
| Adults | 7 |
| Low-income families | 12 |
| Older people | 2 |
| Women | 2 |
| Adolescents | 2 |
| Youths | 1 |
| Impact of Intervention | Park Prescription Intervention–D1 | Increasing Safe Access to Parks–S5 | Play-Grounds–S9 | Park Renovation/Renewal/Redesign–S2 | Education and Campaign –D2 | Physical Activity Program–S7 | Park Facilities Install-ation-S1 | Non-Physical Activity Program–S8 | Outdoor Gym Installation/Fitness Area–S4 | Involving Community Stakeholders–D5 |
|---|---|---|---|---|---|---|---|---|---|---|
| Positively statistically significant | 3 (60%) | 3 (60%) | 4 (50%) | 5 (46%) | 3 (43%) | 9 (41%) | 6 (38%) | 2 (34%) | 4 (27%) | 1 (20%) |
| Negatively statistically significant | 0 (0%) | 0 (0%) | 1 (13%) | 0 (0%) | 1 (14%) | 0 (0%) | 2 (12%) | 0 (0%) | 1 (7%) | 0 (0%) |
| Mixed | 0 | 0 | 0 (0%) | 2 (18%) | 1 (14%) | 3 (14%) | 2 (13%) | 2 (33%) | 3 (20%) | 1 (20%) |
| Not significant | 0 | 0 | 1 (12%) | 0 (0%) | 0 (0%) | 3 (14%) | 2 (12%) | 0 (0%) | 3 (20%) | 1 (20%) |
| No result provided | 2 (40%) | 2 (40%) | 2 (25%) | 4 (36%) | 2 (29%) | 7 (31%) | 4 (25%) | 2 (33%) | 4 (26%) | 2 (40%) |
| Total | 5 | 5 | 8 | 11 | 7 | 22 | 16 | 6 | 15 | 5 |
| Risk of Bias Judgement | Critical | Serious | Moderate | Low |
|---|---|---|---|---|
| Bias due to confounding effects | 2 | 27 | 10 | 5 |
| Bias in selection of study participants | 2 | 30 | 4 | 8 |
| Bias in measurement of interventions | 0 | 7 | 9 | 28 |
| Bias due to departures from intended interventions | 0 | 0 | 0 | 44 |
| Bias due to missing data | 1 | 31 | 4 | 8 |
| Bias in measurement of outcomes | 0 | 16 | 20 | 8 |
| Bias in selection of the reported results | 0 | 0 | 25 | 19 |
| Overall bias | 14 | 24 | 5 | 1 |
| Risk of Bias Judgement | Critical | Serious | Moderate | Low |
|---|---|---|---|---|
| Bias due to confounding effects | 0 | 1 | 2 | 3 |
| Bias in selection of study participants | 0 | 0 | 1 | 5 |
| Bias in measurement of interventions | 0 | 0 | 0 | 6 |
| Bias due to departures from intended interventions | 0 | 0 | 0 | 6 |
| Bias due to missing data | 0 | 1 | 2 | 3 |
| Bias in measurement of outcomes | 0 | 1 | 2 | 3 |
| Bias in selection of the reported results | 0 | 0 | 1 | 5 |
| Overall bias | 0 | 1 | 4 | 1 |
| Outcome Number of Studies | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall GRADE Score |
|---|---|---|---|---|---|---|
| Engagement in MVPA (32) | Very serious (−2) | Serious (−1) | Serious (−1) | Serious (−1) | Unlikely | Very low |
| Increased attendance of parks (18) | Very serious (−2) | Serious (−1) | No important indirectness | Serious (−1) | Likely (−1) | Very low |
| Increased physical activity (METs) (17) | Very serious (−2) | Serious (−1) | No important indirectness | No important imprecision | Likely (−1) | Very low |
| Increased number of visit per person (10) | Very serious (−2) | No important inconsistency | No important indirectness | No important imprecision | Likely (−1) | Very low |
| Increased time spent in parks per person (8) | Very serious (−2) | Very serious (−2) | No important indirectness | No important imprecision | Unlikely | Very low |
| Participation in the more intensive category of physical activity (6) | Very serious (−2) | Serious (−1) | No important indirectness | No important imprecision | Likely (−1) | Very low |
| The number of physically inactive visitors (5) | Serious (−1) | Serious (−1) | Serious (−1) | No important imprecision | Unlikely | Very low |
| Increased use of the installed area (5) | Very serious (−2) | No important inconsistency | No important indirectness | Serious (−1) | Likely (−1) | Very low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, Y.; Wheeler, S.A.; Zuo, A. The Effectiveness of Interventions to Increase Participation and Physical Activities in Parks: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2022, 19, 12590. https://doi.org/10.3390/ijerph191912590
Xu Y, Wheeler SA, Zuo A. The Effectiveness of Interventions to Increase Participation and Physical Activities in Parks: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2022; 19(19):12590. https://doi.org/10.3390/ijerph191912590
Chicago/Turabian StyleXu, Ying, Sarah Ann Wheeler, and Alec Zuo. 2022. "The Effectiveness of Interventions to Increase Participation and Physical Activities in Parks: A Systematic Review of the Literature" International Journal of Environmental Research and Public Health 19, no. 19: 12590. https://doi.org/10.3390/ijerph191912590
APA StyleXu, Y., Wheeler, S. A., & Zuo, A. (2022). The Effectiveness of Interventions to Increase Participation and Physical Activities in Parks: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 19(19), 12590. https://doi.org/10.3390/ijerph191912590