



Association of Workplace Culture of Health and Employee Emotional Wellbeing



Abstract
1. Introduction
2. Methods
2.1. Participants and Data Collection
2.2. Measures
2.2.1. Workplace Culture of Health (COH) Scale
2.2.2. Stress
2.2.3. Depression
2.2.4. Biometric Screening Data
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Differences by Gender and Job Class
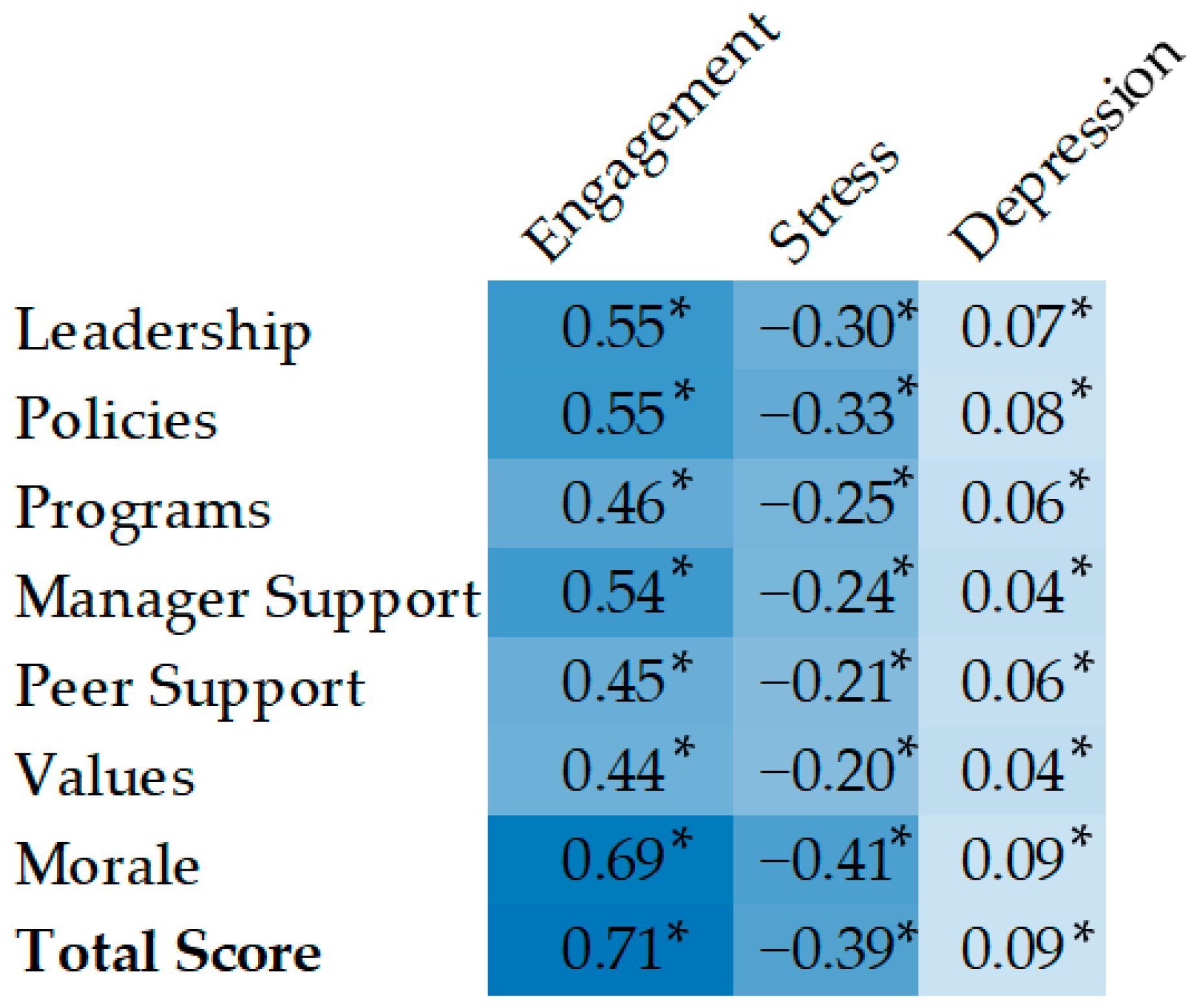
3.3. Correlations
3.4. Regression Models Predicting Workplace COH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Total Sample | Female | Male | Non-Supervisor | Supervisor | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | n = 6235 | n = 4007 | n = 2228 | n = 5023 | n = 1212 | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age | 45.02 | 11.45 | 45.31 | 11.56 | 44.48 | 11.23 | 44.54 | 11.7 | 46.98 | 10.13 |
| Workplace COH | ||||||||||
| Total Score | 73.86 | 12.94 | 73.43 | 13.03 | 74.64 | 12.74 | 73.59 | 13.10 | 74.99 | 12.19 |
| Leadership | 76.87 | 17.85 | 76.28 | 18.07 | 77.94 | 17.40 | 76.51 | 18.00 | 78.38 | 17.13 |
| Policies | 77.59 | 16.94 | 76.82 | 17.17 | 78.97 | 16.41 | 77.37 | 17.02 | 78.48 | 16.57 |
| Programs | 74.47 | 17.47 | 74.16 | 17.65 | 75.04 | 17.14 | 74.63 | 17.27 | 73.79 | 18.26 |
| Supervisor Support | 76.89 | 18.23 | 76.59 | 18.24 | 77.42 | 18.20 | 76.74 | 18.43 | 77.48 | 17.36 |
| Peer Support | 74.47 | 16.11 | 74.98 | 16.27 | 73.55 | 15.78 | 74.18 | 16.37 | 75.65 | 14.94 |
| Values | 76.63 | 16.66 | 76.81 | 16.55 | 76.31 | 16.85 | 76.33 | 16.84 | 77.85 | 15.82 |
| Morale | 70.13 | 13.92 | 69.48 | 14.08 | 71.31 | 13.55 | 69.68 | 14.21 | 72.00 | 12.51 |
| Engagement | 81.20 | 13.64 | 80.91 | 13.45 | 81.73 | 13.96 | 80.56 | 13.82 | 83.87 | 12.49 |
| Health & Biometrics | ||||||||||
| Stress | 5.47 | 2.60 | 5.61 | 2.57 | 5.21 | 2.63 | 5.33 | 2.61 | 6.02 | 2.46 |
| Depression | 96.87 | 13.82 | 96.64 | 14.18 | 97.27 | 13.12 | 96.62 | 14.42 | 97.88 | 10.92 |
| BMI | 29.20 | 6.81 | 29.15 | 7.33 | 29.35 | 5.80 | 29.27 | 6.94 | 29.00 | 6.32 |
| Systolic | 120.20 | 13.27 | 118.28 | 13.15 | 123.31 | 12.75 | 119.95 | 13.12 | 120.60 | 13.68 |
| Diastolic | 77.02 | 8.82 | 76.34 | 8.87 | 78.23 | 8.74 | 76.97 | 8.87 | 77.20 | 8.89 |
| Pulse Pressure | 43.18 | 9.92 | 41.95 | 9.80 | 45.08 | 9.61 | 42.99 | 9.74 | 43.40 | 10.29 |
| Glucose | 96.64 | 23.49 | 95.73 | 23.35 | 100.10 | 25.41 | 97.28 | 24.71 | 97.35 | 21.97 |
| Non-HDL | 130.14 | 38.92 | 126.74 | 37.50 | 135.97 | 40.21 | 130.00 | 38.87 | 130.18 | 38.22 |
Appendix B
| Variable | R2 | F | p | df | b | β | SE | t | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Engagement | 0.51 | 281.1 | <0.001 | (23, 6211) | ||||||
| COH Score | 74.83 | 0.71 | 0.02 | 47.23 | 0.000 | |||||
| Gender | 0.00 | 0.01 | 0.03 | 0.27 | 0.787 | |||||
| Job Class | 0.02 | 0.16 | 0.03 | 5.89 | 0.000 | |||||
| Age | 0.00 | −0.01 | 0.01 | −0.71 | 0.475 | |||||
| BMI | 0.00 | −0.01 | 0.02 | −0.77 | 0.444 | |||||
| Pulse Pressure | 0.00 | 0.00 | 0.01 | 0.32 | 0.748 | |||||
| Glucose | 0.00 | 0.00 | 0.02 | −0.21 | 0.831 | |||||
| Non HDL | 0.00 | −0.01 | 0.01 | −1.15 | 0.249 | |||||
| Org 1 | 4.42 | 0.32 | 0.15 | 2.23 | 0.026 | |||||
| Org 2 | 1.36 | 0.10 | 0.05 | 1.84 | 0.066 | |||||
| Org 3 | 1.58 | 0.12 | 0.06 | 1.82 | 0.069 | |||||
| Org 4 | 2.72 | 0.20 | 0.06 | 3.50 | 0.000 | |||||
| Org 5 | 1.29 | 0.09 | 0.07 | 1.32 | 0.187 | |||||
| Org 6 | 1.23 | 0.09 | 0.05 | 1.80 | 0.071 | |||||
| Org 7 | 2.98 | 0.22 | 0.16 | 1.35 | 0.176 | |||||
| Org 8 | 0.81 | 0.06 | 0.07 | 0.84 | 0.402 | |||||
| Org 9 | 1.49 | 0.11 | 0.12 | 0.87 | 0.382 | |||||
| Org 10 | 1.35 | 0.10 | 0.06 | 1.71 | 0.087 | |||||
| Org 11 | −6.07 | −0.44 | 0.05 | −8.19 | 0.000 | |||||
| Org 12 | 3.29 | 0.24 | 0.39 | 0.61 | 0.539 | |||||
| Org 13 | 2.69 | 0.20 | 0.09 | 2.23 | 0.026 | |||||
| Org 14 | 3.64 | 0.27 | 0.08 | 3.17 | 0.002 | |||||
| Org 15 | 4.21 | 0.31 | 0.06 | 4.89 | 0.000 | |||||
| Stress | 0.20 | 65.63 | <0.001 | (23, 6211) | ||||||
| COH Score | −0.08 | −0.4 | 0.02 | −27 | 0.000 | |||||
| Gender | −0.32 | −0.1 | 0.03 | −4.4 | 0.000 | |||||
| Job Class | 0.95 | 0.37 | 0.03 | 13.5 | 0.000 | |||||
| Age | −0.01 | −0 | 0.01 | −3 | 0.003 | |||||
| BMI | 0.00 | −0 | 0.02 | −0.2 | 0.824 | |||||
| Pulse Pressure | 0.00 | −0 | 0.01 | −0.5 | 0.587 | |||||
| Glucose | 0.00 | −0 | 0.02 | −0.2 | 0.804 | |||||
| Non HDL | 0.00 | 0 | 0.01 | 0.05 | 0.959 | |||||
| Org 1 | −0.93 | −0.4 | 0.15 | −2.5 | 0.014 | |||||
| Org 2 | −0.46 | −0.2 | 0.05 | −3.2 | 0.001 | |||||
| Org 3 | 0.03 | 0.01 | 0.06 | 0.16 | 0.875 | |||||
| Org 4 | −0.73 | −0.3 | 0.06 | −5 | 0.000 | |||||
| Org 5 | −0.47 | −0.2 | 0.07 | −2.5 | 0.011 | |||||
| Org 6 | 0.02 | 0.01 | 0.05 | 0.14 | 0.887 | |||||
| Org 7 | −0.06 | −0 | 0.16 | −0.1 | 0.890 | |||||
| Org 8 | 0.27 | 0.1 | 0.07 | 1.47 | 0.141 | |||||
| Org 9 | 0.19 | 0.07 | 0.12 | 0.59 | 0.553 | |||||
| Org 10 | −0.82 | −0.3 | 0.06 | −5.5 | 0.000 | |||||
| Org 11 | 0.82 | 0.32 | 0.05 | 5.81 | 0.000 | |||||
| Org 12 | 0.34 | 0.13 | 0.39 | 0.34 | 0.737 | |||||
| Org 13 | −0.76 | −0.3 | 0.09 | −3.3 | 0.001 | |||||
| Org 14 | −1.34 | −0.5 | 0.08 | −6.1 | 0.000 | |||||
| Org 15 | −0.85 | −0.3 | 0.06 | −5.2 | 0.000 | |||||
| Depression | 0.02 | 5.25 | <0.001 | (23, 6211) | ||||||
| COH Score | 0.08 | 0.08 | 0.02 | 5.05 | 0.000 | |||||
| Gender | 0.38 | 0.03 | 0.03 | 0.97 | 0.330 | |||||
| Job Class | 1.03 | 0.07 | 0.03 | 2.75 | 0.006 | |||||
| Age | 0.06 | 0.05 | 0.01 | 3.45 | 0.001 | |||||
| BMI | −0.08 | −0 | 0.02 | −2.5 | 0.014 | |||||
| Pulse Pressure | 0.02 | 0.02 | 0.01 | 1.15 | 0.250 | |||||
| Glucose | −0.03 | −0.1 | 0.02 | −3.1 | 0.002 | |||||
| Non HDL | 0.00 | −0 | 0.01 | −0.4 | 0.701 | |||||
| Org 1 | −1.52 | −0.1 | 0.15 | −0.8 | 0.449 | |||||
| Org 2 | −0.58 | −0 | 0.05 | −0.8 | 0.443 | |||||
| Org 3 | −1.34 | −0.1 | 0.06 | −1.5 | 0.130 | |||||
| Org 4 | −2.24 | −0.2 | 0.06 | −2.8 | 0.004 | |||||
| Org 5 | −1.95 | −0.1 | 0.07 | −2 | 0.049 | |||||
| Org 6 | −1.31 | −0.1 | 0.05 | −1.9 | 0.058 | |||||
| Org 7 | −4.10 | −0.3 | 0.16 | −1.8 | 0.066 | |||||
| Org 8 | −1.92 | −0.1 | 0.07 | −2 | 0.049 | |||||
| Org 9 | 0.27 | 0.02 | 0.12 | 0.16 | 0.875 | |||||
| Org 10 | −0.86 | −0.1 | 0.06 | −1.1 | 0.282 | |||||
| Org 11 | 1.63 | 0.12 | 0.05 | 2.18 | 0.029 | |||||
| Org 12 | −3.14 | −0.2 | 0.39 | −0.6 | 0.563 | |||||
| Org 13 | −2.79 | −0.2 | 0.09 | −2.3 | 0.022 | |||||
| Org 14 | −1.73 | −0.1 | 0.08 | −1.5 | 0.137 | |||||
| Org 15 | 0.38 | 0.03 | 0.06 | 0.44 | 0.661 | |||||
References
- Ogata, A.J.N. A Global View of Health and Well-Being. Am. J. Health Promot. 2019, 33, 621–622. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, K.; Anas, J. It’s a New Era for Mental Health at Work. Harvard Business Review, 4 October 2021. [Google Scholar]
- Daly, M.; Sutin, A.R.; Robinson, E. Depression Reported by US Adults in 2017–2018 and March and April 2020. J. Affect. Disord. 2021, 278, 131–135. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. Stress in America 2021: A National Mental Health Crisis; American Psychological Association: Washington, DC, USA, 2021. [Google Scholar]
- Linnan, L.A.; Cluff, L.; Lang, J.E.; Penne, M.; Leff, M.S. Results of the Workplace Health in America Survey. Am. J. Health Promot. 2019, 33, 652–665. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Henke, R.M.; Tabrizi, M.; Pelletier, K.R.; Loeppke, R.; Ballard, D.W.; Grossmeier, J.; Anderson, D.R.; Yach, D.; Kelly, R.K.; et al. Do Workplace Health Promotion (Wellness) Programs Work? J. Occup. Environ. Med. 2014, 56, 927–934. [Google Scholar] [CrossRef]
- Flynn, J.P.; Gascon, G.; Doyle, S.; Matson Koffman, D.M.; Saringer, C.; Grossmeier, J.; Tivnan, V.; Terry, P. Supporting a Culture of Health in the Workplace: A Review of Evidence-Based Elements. Am. J. Health Promot. 2018, 32, 1755–1788. [Google Scholar] [CrossRef]
- Aldana, S.G.; Anderson, D.R.; Adams, T.B.; Whitmer, R.W.; Merrill, R.M.; George, V.; Noyce, J. A Review of the Knowledge Base on Healthy Worksite Culture. J. Occup. Environ. Med. 2012, 54, 414–419. [Google Scholar] [CrossRef]
- Safeer, R.; Allen, J. Defining a Culture of Health in the Workplace. J. Occup. Environ. Med. 2019, 61, 863–867. [Google Scholar] [CrossRef]
- Kwon, Y.; Marzec, M.; Edington, D. Development and Validity of a Scale to Measure Workplace Culture of Health. J. Occup. Environ. Med. 2015, 57, 571–577. [Google Scholar] [CrossRef]
- Lee, B.; Bendixsen, C.; Liebman, A.; Gallagher, S. Using the Socio-Ecological Model to Frame Agricultural Safety and Health Interventions. J. Agromed. 2017, 22, 298–303. [Google Scholar] [CrossRef]
- Terry, P.E. Workplace Health Promotion Is Growing Up but Confusion Remains About What Constitutes a Comprehensive Approach. Am. J. Health Promot. 2019, 33, 845–849. [Google Scholar] [CrossRef]
- American College of Occupational and Environmental Medicine; American Council on Exercise; American Heart Association; Bravo Wellness; Health Enhancement Research Organization; HealthFitness; HealthPartners; Healthways; Interactive Health; Johnson & Johnson Services Inc.; et al. A Response to Proposed Equal Employment Opportunity Commission Regulations on Employer-Sponsored Health, Safety, and Well-Being Initiatives. J. Occup. Environ. Med. 2016, 58, e103–e110. [Google Scholar] [CrossRef]
- Hentges, M.; Pilot, E. Making It “Work”: Mothers’ Perceptions of Workplace Breastfeeding and Pumping at Dutch Universities. Int. Breastfeed. J. 2021, 16, 87. [Google Scholar] [CrossRef]
- Kwon, Y.; Marzec, M.L. Does Worksite Culture of Health (CoH) Matter to Employees? Empirical Evidence Using Job-Related Metrics. J. Occup. Environ. Med. 2016, 58, 448–454. [Google Scholar] [CrossRef]
- Nekula, P.; Koob, C. Associations between Culture of Health and Employee Engagement in Social Enterprises: A Cross-Sectional Study. PLoS ONE 2021, 16, e0245276. [Google Scholar] [CrossRef]
- Grossmeier, J.; Castle, P.H.; Pitts, J.S.; Saringer, C.; Jenkins, K.R.; Imboden, M.T.; Mangen, D.J.; Johnson, S.S.; Noeldner, S.P.; Mason, S.T. Workplace Well-Being Factors That Predict Employee Participation, Health and Medical Cost Impact, and Perceived Support. Am. J. Health Promot. 2020, 34, 349–358. [Google Scholar] [CrossRef]
- Goetzel, R.Z.; Fabius, R.; Roemer, E.C.; Kent, K.B.; Berko, J.; Head, M.A.; Henke, R.M. The Stock Performance of American Companies Investing in a Culture of Health. Am. J. Health Promot. 2019, 33, 439–447. [Google Scholar] [CrossRef]
- Henke, R.M.; Head, M.A.; Kent, K.B.; Goetzel, R.Z.; Roemer, E.C.; McCleary, K. Improvements in an Organization’s Culture of Health Reduces Workers’ Health Risk Profile and Health Care Utilization. J. Occup. Environ. Med. 2019, 61, 96–101. [Google Scholar] [CrossRef]
- Chang, Y.-T.; Tsai, F.-J.; Yeh, C.-Y.; Chen, R.-Y. From Cognition to Behavior: Associations of Workplace Health Culture and Workplace Health Promotion Performance with Personal Healthy Lifestyles. Front. Public Health 2021, 9, 745846. [Google Scholar] [CrossRef]
- Laing, S.S.; Jones, S.M.W. Anxiety and Depression Mediate the Relationship between Perceived Workplace Health Support and Presenteeism: A Cross-Sectional Analysis. J. Occup. Environ. Med. 2016, 58, 1144–1149. [Google Scholar] [CrossRef]
- Jia, Y.; Gao, J.; Dai, J.; Zheng, P.; Fu, H. Associations between Health Culture, Health Behaviors, and Health-Related Outcomes: A Cross-Sectional Study. PLoS ONE 2017, 12, e0178644. [Google Scholar] [CrossRef]
- Kwon, Y.; Marzec, M.L. Unpacking the Associations Between Perceived Cultural Support and Employee Health: The Approach of Social Capital. J. Occup. Environ. Med. 2019, 61, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P. Gender Differences in Stress and Coping Styles. Personal. Individ. Differ. 2004, 37, 1401–1415. [Google Scholar] [CrossRef]
- Kessler, R.C.; Walters, E.E.; Forthofer, M.S. The Social Consequences of Psychiatric Disorders, III: Probability of Marital Stability. AJP 1998, 155, 1092–1096. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Kroenke, K.; Gräfe, K. Detecting and Monitoring Depression with a Two-Item Questionnaire (PHQ-2). J. Psychosom. Res. 2005, 58, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P. A Guide to Econometrics; John Wiley & Sons: Hoboken, NJ, USA, 2008; ISBN 978-1-4051-8257-7. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage: Newcastle upon Tyne, UK, 2013; ISBN 1-4462-7458-6. [Google Scholar]
- Flatt, C.; Jacobs, R.L. Principle Assumptions of Regression Analysis: Testing, Techniques, and Statistical Reporting of Imperfect Data Sets. Adv. Dev. Hum. Resour. 2019, 21, 484–502. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2022. [Google Scholar]
- Marzec, M. Measuring Subcultures and Leveraging Data to Optimize Well-Being Initiatives. Am. J. Health Promot. 2018, 32, 1817–1820. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000; ISBN 978-92-4-120894-9.
- American Diabetes Association. Checking Your Blood Glucose. LivingWithDiabetes > TreatmentandCare>. 2015. Available online: http://www.diabetes.org (accessed on 3 August 2011).
- Verdecchia, P. Reference Values for Ambulatory Blood Pressure and Self-Measured Blood Pressure Based on Prospective Outcome Data. Blood Press. Monit. 2001, 6, 323–327. [Google Scholar] [CrossRef]
- Cholesterol Levels: What You Need to Know. Available online: https://medlineplus.gov/cholesterollevelswhatyouneedtoknow.html (accessed on 26 April 2022).
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The Measurement of Work Engagement With a Short Questionnaire: A Cross-National Study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Peterson, M. What Men and Women Value at Work: Implications for Workplace Health. Gend. Med. 2004, 1, 106–124. [Google Scholar] [CrossRef]
- Weeden, K.A.; Cha, Y.; Bucca, M. Long Work Hours, Part-Time Work, and Trends in the Gender Gap in Pay, the Motherhood Wage Penalty, and the Fatherhood Wage Premium. RSF Russell Sage Found. J. Soc. Sci. 2016, 2, 71–102. [Google Scholar] [CrossRef]
- Hamm, M.D. An Examination of the Potential Mediating Effect of Employee Health Risk Status on the Relationship between Organizational Health Culture and Employee Engagement. Ph.D. Thesis, Grand Canyon Univerisy, Phoenix, AZ, USA, ProQuest Information & Learning, Ann Arbor, MI, USA, 2018. [Google Scholar]
- Pahn, J.; Yang, Y. Factors Associated with Cardiovascular Disease Prevention Behavior Among Office Workers Based on an Ecological Model. Sage Open 2021, 11, 21582440211004163. [Google Scholar] [CrossRef]
- Crimmins, T.J.; Halberg, J. Measuring Success in Creating a “Culture of Health”. J. Occup. Environ. Med. 2009, 51, 351–355. [Google Scholar] [CrossRef]
- Hall, M.E.; Bergman, R.J.; Nivens, S. Worksite Health Promotion Program Participation: A Study to Examine the Determinants of Participation. Health Promot. Pract. 2014, 15, 768–776. [Google Scholar] [CrossRef]
- Lin, Y.-W.; Lin, Y.-Y. A Multilevel Model of Organizational Health Culture and the Effectiveness of Health Promotion. Am. J. Health Promot. 2014, 29, e53–e63. [Google Scholar] [CrossRef]

| Female | Male | |||||||
|---|---|---|---|---|---|---|---|---|
| (n = 4007) | (n = 2228) | |||||||
| Mean | SD | Mean | SD | t | df | p | d | |
| COH Score | 73.43 | 13.03 | 74.64 | 12.74 | −3.58 | 4691 | <0.001 | 0.09 |
| Engagement | 80.91 | 13.45 | 81.73 | 13.96 | −2.24 | 4460 | 0.025 | 0.06 |
| Stress | 5.61 | 2.57 | 5.21 | 2.63 | 5.70 | 4512 | <0.001 | 0.15 |
| Depression | 96.64 | 14.18 | 97.27 | 13.12 | −1.78 | 4908 | 0.07 | 0.05 |
| Non-Supervisor | Supervisor | |||||||
|---|---|---|---|---|---|---|---|---|
| (n = 5023) | (n = 1212) | |||||||
| Mean | SD | Mean | SD | t | df | p | d | |
| COH Score | 73.59 | 13.10 | 74.99 | 12.19 | −3.58 | 4691 | <0.001 | 0.09 |
| Engagement | 80.56 | 13.82 | 83.87 | 12.49 | −2.24 | 4460 | 0.025 | 0.06 |
| Stress | 5.33 | 2.61 | 6.02 | 2.46 | 5.70 | 4512 | <0.001 | 0.15 |
| Depression | 96.62 | 14.42 | 97.88 | 10.92 | −1.78 | 4908 | 0.07 | 0.05 |
| Variable | R2 | F | p | df | β | SE | t | p | |
|---|---|---|---|---|---|---|---|---|---|
| Engagement | 0.51 | 281.1 | <0.001 | (23, 6211) | |||||
| COH Score | 0.71 | 0.01 | 77.89 | <0.001 | |||||
| Gender | 0.01 | 0.02 | 0.37 | 0.711 | |||||
| Job Class | 0.16 | 0.02 | 6.94 | <0.001 | |||||
| Age | −0.01 | 0.01 | −1.02 | 0.306 | |||||
| BMI | −0.01 | 0.01 | −1.34 | 0.181 | |||||
| Pulse Pressure | 0.00 | 0.01 | 0.46 | 0.648 | |||||
| Glucose | 0.00 | 0.01 | −0.44 | 0.658 | |||||
| Non HDL | −0.01 | 0.01 | −1.53 | 0.127 | |||||
| Stress | 0.20 | 65.63 | <0.001 | (23, 6211) | |||||
| COH Score | −0.40 | 0.01 | −34.43 | <0.001 | |||||
| Gender | −0.12 | 0.03 | −4.72 | <0.001 | |||||
| Job Class | 0.37 | 0.03 | 12.45 | <0.001 | |||||
| Age | −0.04 | 0.01 | −3.36 | <0.001 | |||||
| BMI | 0.00 | 0.01 | −0.30 | 0.761 | |||||
| Pulse Pressure | −0.01 | 0.01 | −0.60 | 0.547 | |||||
| Glucose | 0.00 | 0.01 | −0.40 | 0.687 | |||||
| Non HDL | 0.00 | 0.01 | 0.05 | 0.957 | |||||
| Depression | 0.02 | 5.25 | <0.001 | (23, 6211) | |||||
| COH Score | 0.08 | 0.01 | 5.89 | <0.001 | |||||
| Gender | 0.03 | 0.03 | 0.95 | 0.345 | |||||
| Job Class | 0.07 | 0.03 | 2.30 | 0.02 | |||||
| Age | 0.05 | 0.01 | 3.49 | <0.001 | |||||
| BMI | −0.04 | 0.01 | −3.03 | <0.001 | |||||
| Pulse Pressure | 0.02 | 0.01 | 1.15 | 0.249 | |||||
| Glucose | −0.06 | 0.01 | −4.48 | <0.001 | |||||
| Non HDL | 0.00 | 0.01 | −0.36 | 0.719 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marenus, M.W.; Marzec, M.; Chen, W. Association of Workplace Culture of Health and Employee Emotional Wellbeing. Int. J. Environ. Res. Public Health 2022, 19, 12318. https://doi.org/10.3390/ijerph191912318
Marenus MW, Marzec M, Chen W. Association of Workplace Culture of Health and Employee Emotional Wellbeing. International Journal of Environmental Research and Public Health. 2022; 19(19):12318. https://doi.org/10.3390/ijerph191912318
Chicago/Turabian StyleMarenus, Michele Wolf, Mary Marzec, and Weiyun Chen. 2022. "Association of Workplace Culture of Health and Employee Emotional Wellbeing" International Journal of Environmental Research and Public Health 19, no. 19: 12318. https://doi.org/10.3390/ijerph191912318
APA StyleMarenus, M. W., Marzec, M., & Chen, W. (2022). Association of Workplace Culture of Health and Employee Emotional Wellbeing. International Journal of Environmental Research and Public Health, 19(19), 12318. https://doi.org/10.3390/ijerph191912318