


Concerted Model of Healthcare for Awá Indigenous of Nariño, Colombia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
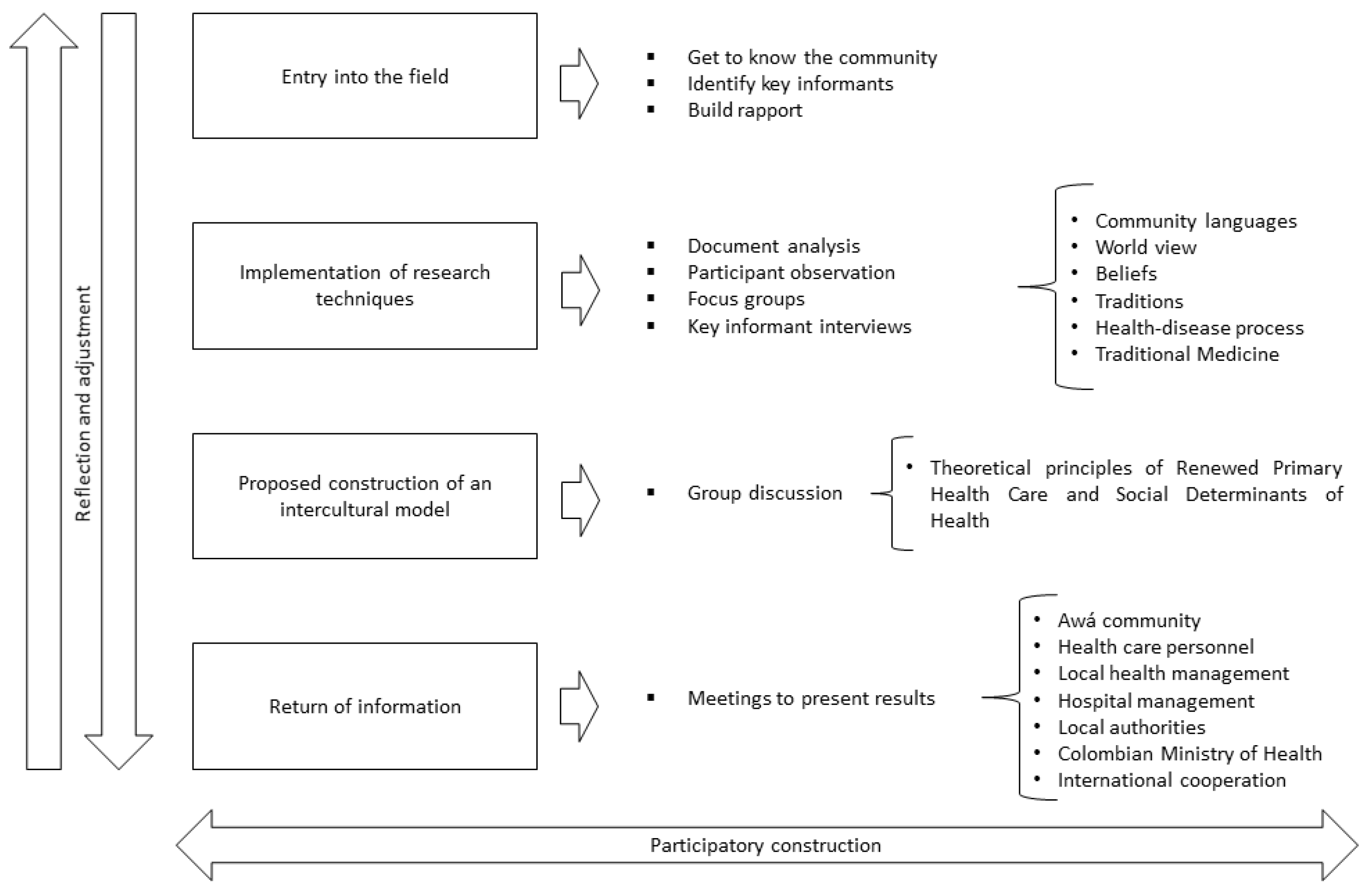
2.1. Design
2.2. Participants
2.3. Data Collection Techniques
2.3.1. Analysis of Documents
2.3.2. Participant Observation
2.3.3. Interviews with Key Informants
2.3.4. Focus Groups
2.3.5. Group Discussion
2.4. Procedure
2.5. Analysis of the Information
2.6. Ethical Considerations
3. Results
3.1. General Context of the Awá Community
3.1.1. Geographic Location
3.1.2. Demographic Aspects and Social Organization
3.2. The “Katsa Su”, the Awá’s Concept of Land
3.3. Social Determinants of Health (SDH) for the Awá
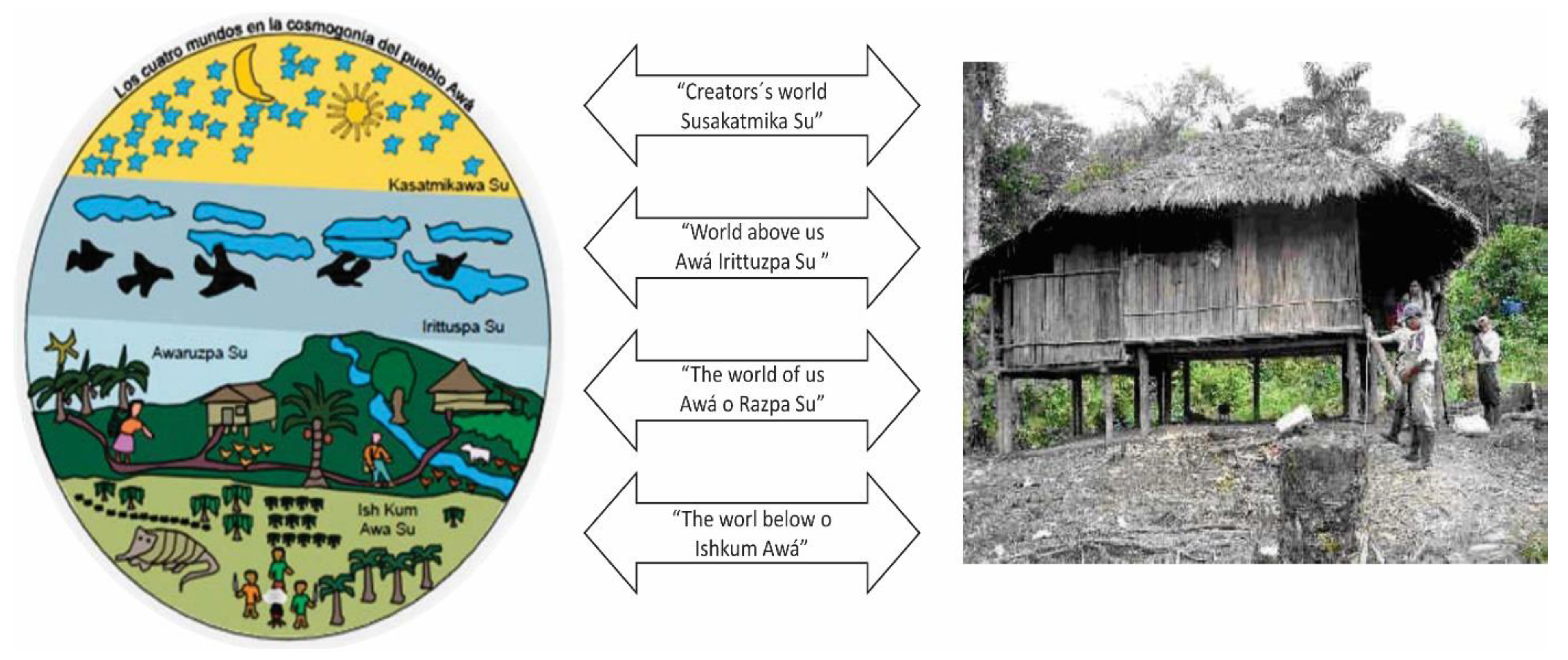
- (1)
- The land: the central focus of their worldview of life and health is ancestral land, which is “material and spiritual” and supports their beliefs, uses and customs, particularly the belief in the existence of the “four physical and spiritual worlds” that govern their behavior and social and cultural relations and reflects a deep relationship with nature. For the Awá, the supra material conception of land has its equivalence and representation in the construction and layout of their homes.
- (2)
- The mountains and jungles: the location of their sacred sites, which are inhabited by the spirits of their ancestors, reflecting the Awá’s intense cultural relationship with “mother earth.” The natural resources, forests, jungles and plants, as well as the wild animals that provide them sustenance and food security and sovereignty, are key to the Awá’s “Law of Origin”, which is based on the principle of “taking just what is needed from nature” to survive, without requiring more.
- (3)
- Traditional medicine: with its beliefs, wisdom and ancestral knowledge and “the traditional physicians and their ongoing relationship with ancestral spirits”, which explain the uses, customs, behaviors and cultural practices related to health and make it possible to prevent, treat, purify and cure spiritual illnesses. In traditional medicine, a disease can be triggered by the influence of factors that are external to a person, such as plants or nature spirits, as well as by internal factors related to the spiritual dimension of the person. The latter is crucial to healing. Generally, it can be said that spiritual illnesses fall within culture-bound syndromes [11].
- (4)
- Food security and sovereignty: the land permits and provides unlimited resources and sources of ancestral food, such that families freely moving through the mountains and jungles without restriction is guaranteed for planting, harvesting, hunting, fishing and eating for the security and physical preservation of the Awá.
3.4. Concerted Intercultural Health Care Model
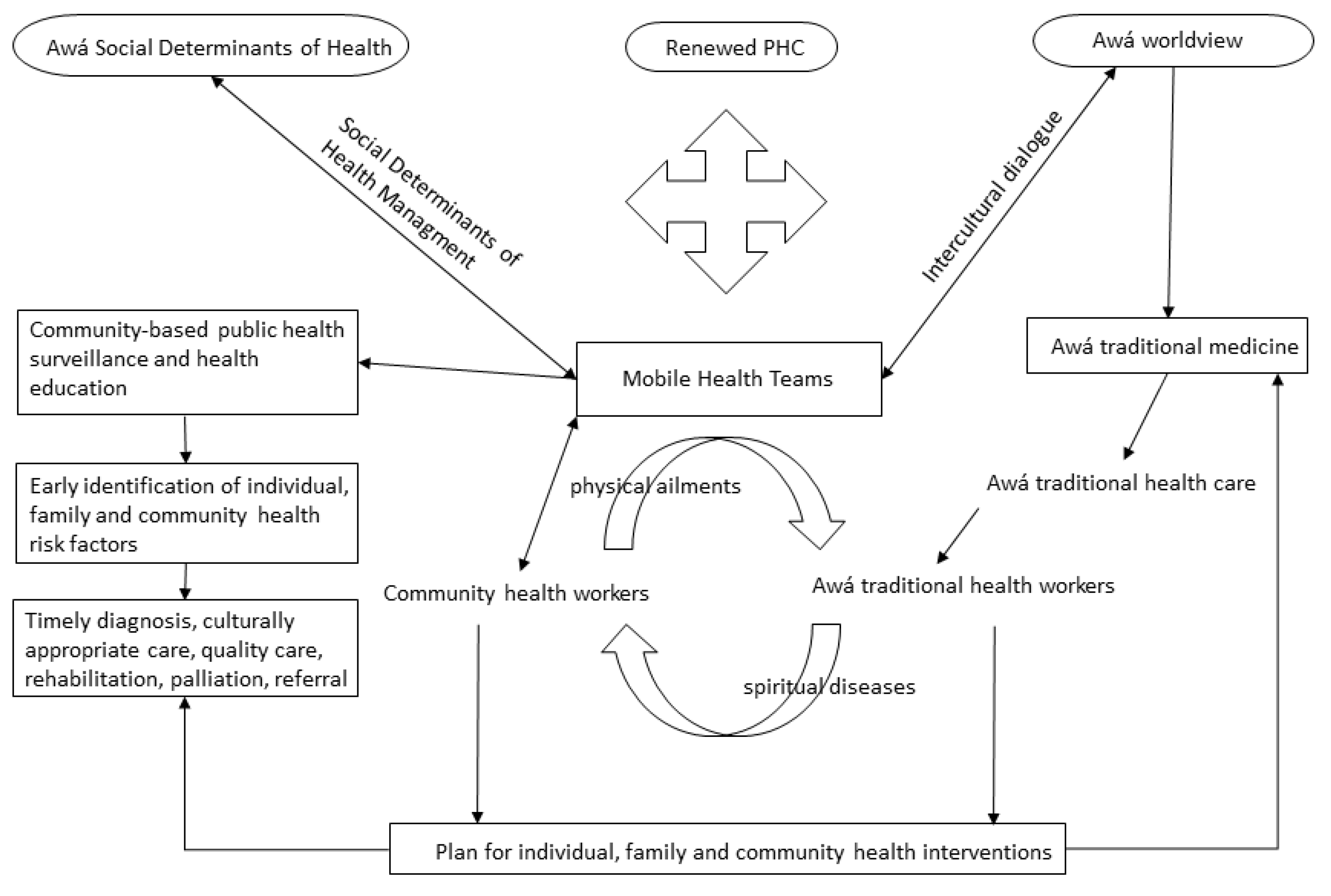
- The creation of an Indigenous Health Services Provider Institution (IPSI in Spanish) to organize, administer and operate intercultural health care for the Ricaurte Awá community, with its administrative and service headquarters in the municipal capital and outpatient health care services offered by Western and traditional physicians. This proposal includes at least seven Mobile Health Teams (MHTs) made up of family physicians, dentists, nurses, nursing aides or public health workers, health promoters and environmental sanitation promoters working in coordination with traditional Awá medicine practitioners (prior meetings would ensure both a common language and shared goals). These units would be permanently and strategically located in seven communal territories throughout the Awá territory and be open 24 h/day, 7 days/week and 20 days/month (with a 10-day rest period). They would play a strong role in health promotion and disease prevention, in the search for and early detection of individual, family and community risk factors for health, in intervention in those factors and the provision of low-complexity extramural medical care.
- The MHTs would be trained and be able to solve problems. Their operations in the Awá territory would be logistically autonomous, and they would also handle medical and obstetric emergencies, or when necessary, stabilize and refer patients to second- or third-level complexity services without negatively affecting the health care that the local hospital should continue to provide, which would continue to be the referral hospital for primary care. At the same time, the Awá would continue to receive health services from traditional practitioners in close coordination with the MHTs. The Awá families would be the first link in the community’s participation in health, with activities related to self-care, community-based public health surveillance, referrals and counter-referrals of patients, basic sanitation, and health promotion and prevention.
- The progressive conversion of the Ricaurte hospital into a second-level hospital is proposed through the implementation of the human resources, technology and facilities needed to address not only general low-complexity medical needs but also medium-complexity cases. To this end, basic medical surgical specialties would be provided, including pediatrics, internal medicine, gynecology, obstetrics, general surgery and anesthesia to treat basic medical and surgical cases for children, women and adults, and thereby minimize referral of patients to other cities. Subsequently, the MHTs would be strengthened by family physicians who would provide needed medical care, thereby expanding and improving problem-solving capacity directly in the field and in the local hospital, and through this action preventing displacement of the Awá. This also prevents their feeling of being uprooted when they are referred from their territory to the local hospital or other institutions in the service network, as these spaces are very foreign to them and where, generally, they are far from their relatives and friends.
- The intercultural appropriateness of all institutional health programs at the local hospital and the institutions in the network is envisioned to be in accordance with the Awá community’s worldview of life and health. This process would be a product of intercultural dialogue on health—an “exchange of knowledge” that enables taking concerted actions that effectively impact the current health situation of the Awá population. The proposal also includes appropriate physical spaces, food and accommodations, as well as traditional physicians who offer health care in the health institutions and are dedicated to “spiritual” care and assisting Awá patients who require hospitalization. This would undoubtedly contribute to successfully treating cultural illnesses that are specific to the Awá population, or “spiritual and physical” illnesses.
- It is proposed that housing be made available in the municipal capital of Ricaurte for Indigenous patients who are referred to the local hospital from the most remote communal territories and for their families and companions so that they have a dignified place to stay and take meals during patient visits and hospitalizations. This would also be used by postpartum women to get the rest they need during at least their first few days on the diet that the Awá women are accustomed to eating after childbirth. This would mitigate the negative effects of the institution’s decision to discharge women the day after childbirth and avoid the medical and cultural implications of the mother and child taking a long trip back home, which often requires traveling for more than two days in difficult climate conditions and along the poor roads that are typical of the region.
- Ongoing support for traditional Awá medicine is proposed through the training of new traditional physicians and midwives by providing support or incentives for the work of traditional health agents through modalities such as “food for work” or “food for training” programs, which have been implemented in the past by international cooperation agencies in the region, such as the United Nations World Food Programme [12]. This type of support can also be applied for promoting community medicinal gardens.
- The participants proposed that the traditional and civil authorities in the municipality of Ricaurte, the department of Nariño, national authorities and international cooperation agencies work together to solve the serious problems in the Awá territory with the ongoing humanitarian situation and armed conflict, through urgent humanitarian demining of the territory, suspending current and future large-scale mining and forest exploitation, stopping aerial glyphosate spraying of mountains and jungles, taking concerted efforts to develop and implement options to replace and end the use of illegal crops, carrying out appropriate, adapted, concerted and sustainable community development projects that ensure food security and sovereignty in accordance with their uses and customs, implementing environmentally sustainable alternatives for supplying safe water, and appropriately disposing of excrement and solid and liquid wastes.
- Lastly, the Awá community proposed support and capacity-building for their traditional medicine agents, incentives for cultivating medicinal plants for the rituals, uses, practices and customs of their health culture, meetings and dialogues for the exchange of knowledge, and coordination with Western medicine, particularly with the proposed mobile teams.
3.5. Characteristics of the Model and Operational Strategies
- (1)
- Concerted efforts through ongoing dialogue about the knowledge of Western and traditional Awá medicine; dialogue based on recognition, respect and mutual coordination.
- (2)
- Community participation in health through the social mobilization of Awá families and communities, intercultural adaptation of health education on self-care and disease prevention, community-based public health surveillance, and establishing an intercultural dialogue between Western and traditional medicine.
- (3)
- Intersectorality: Institutional, sectoral, intersectoral, community and cross-sectoral coordination for an integrated SDH approach.
- (4)
- Reorienting institutional health services according to the social, cultural and geographic needs of the municipality and the Awá territory.
- (5)
- Intercultural appropriateness of institutional health programs and services through ongoing intercultural dialogue between the two medicines and health cultures.
- (6)
- Ongoing education for Mobile Health Teams and the community, and capacity-building, training and exchange of knowledge for the institutions and the community. This includes training Awá people as health technicians, technologists and professionals for subsequent community service and ownership of their health processes.
- (7)
- Health sector advocacy of programs, projects, plans and policies that lead to improving the health situation of the Awá population.
- (8)
- Strengthening institutions to expand coverage, services, technologies and facilities in the service network, including telecommunication, communication and information technologies for improving the problem-solving capacity of the MHTs in Awá territories.
- (9)
- Ongoing planning and evaluation for organizing services, managing health risks, providing quality care, ensuring the sustainability of the model, accomplishing concrete processes, achieving health impact goals, improving the quality of health and consequently contributing to the physical and cultural preservation of the Awá population in Ricaurte Nariño, Colombia. The integrated model can be seen in Figure 3.
4. Discussion
5. Conclusions
6. Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colombia Ministry of Health and Social Protection. Análisis de Situación de Salud Colombia 2014; (PDF) A S I S Análisis de Situación de Salud COLOMBIA 2014|ADRIANA GUEVARA-Academia.edu; Colombia Ministry of Health and Social Protection: Bogotá, Colombia, 2014. [Google Scholar]
- CODHES Consultoría para los Derechos Humanos y el Desplazamiento. ¿Consolidación de qué? Informe sobre desplazamiento, conflicto armado y derechos humanos en Colombia en 2010. Boletín Informativo. 2011, 77. [Google Scholar]
- Colombia’s Constitutional Court Sentencia T- 025 de 2004. Autos 004 de 2009. 382 de 2010. 174 de 2011 y 173 de 2011.
- Municipality of Ricaurte Nariño. Análisis de Situación de Salud; ASIS de Ricaurte Nariño: Nariño, Colombia, 2013. [Google Scholar]
- McKay, S. Participatory Action Research, Community-Based. In The Encyclopedia of Peace Psychology, 1st ed.; Christie, D.J., Ed.; Wiley Online Library: Hoboken, NJ, USA, 2011. [Google Scholar] [CrossRef]
- Valdez, Z. Etnografía crítica. Surgimiento y repercusiones. Rev. Comun. 2012, 33, 16–24. [Google Scholar]
- Guber, R. La Etnografía Método, Campo y Reflexividad; Siglo Veintiuno Editores: Buenos Aires, Argentina, 2016. [Google Scholar]
- Barcia, M.; De Pena, L.; Giménez, S.; Morosi, C.; Toledo, S. Consentimiento informado comunitario en investigación con seres humanos. An. Fac. Med. (Univ. Repúb. Urug.) 2017, 4 (Suppl. S2), 7–15. [Google Scholar]
- National Statistics Department of Colombia. Estimaciones y Proyecciones de Población de 1985–2020. Proyecciones de población. Available online: dane.gov.co (accessed on 11 July 2022).
- Republic of Colombia; Congreso de la República. Diario Oficial. Constitución Política Nacional. 1991; Constitucion-Politica-Colombia-1991.pdf. Available online: corteconstitucional.gov.co (accessed on 11 July 2022).
- Portilla-Rodríguez, S.P.; Madroñero, O.; Getia, P.E. Sistema médico tradicional-ancestral en el territorio de los Pastos Resguardo Indígena de Túquerres-Narino, Colombia. Cienc. Intercult. 2016, 19, 66–80. [Google Scholar] [CrossRef]
- World Food Programme. Colombia. Colombia | World Food Programme. Available online: wfp.org (accessed on 11 July 2022).
- Corso, M.; DeSouza, A.; Brunton, G.; Yu, H.; Cancelliere, C.; Mior, S.; Taylor-Vaisey, A.; MacLeod-Beaver, K.; Côté, P. Integrating Indigenous healing practices within collaborative care models in primary healthcare in Canada: A rapid scoping review. BMJ Open 2022, 12, e059323. [Google Scholar] [CrossRef]
- PAHO/WHO. La Renovación de la Atención Primaria en Salud en las Américas; Documento de posición de la OPS/OMS; OPS. La Renovación de la Atención Primaria de Salud en las Américas: Washintong, DC, USA, 2007; Available online: paho.org (accessed on 11 July 2022).
- Davy, C.; Harfield, S.; McArthur, A.; Munn, Z.; Brown, A. Access to primary health care services for Indigenous peoples: A framework synthesis. Int. J. Equity Health 2016, 15, 163. [Google Scholar] [CrossRef]
- Pelcastre-Villafuerte, B.; Meneses-Navarro, S.; Ruelas-González, G.; Reyes-Morales, H.; Amaya-Castellanos, A.; Taboada, A. Aging in rural, Indigenous communities: An intercultural and participatory healthcare approach in Mexico. Ethn. Health 2017, 22, 610–630. [Google Scholar] [CrossRef]
- Harfield, S.; Davy, C.; McArthur, A.; Munn, Z.; Brown, A.; Brown, N. Characteristics of Indigenous primary health care service delivery models: A systematic scoping review. Glob. Health 2018, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud; Dirección General de Promoción de la Salud; Unidad de Salud Comunitaria y Movilización Social. Guía de Desarrollo Comunitario en Proyectos de Salud-DESCOM SALUD; Editorial Euro Express: La Paz, Bolivia, 2019. [Google Scholar]
- Langdon, E. Salud indígena en Brasil: Pluralismo médico y autoatención. Desacatos 2018, 58, 8–15. [Google Scholar] [CrossRef]
- Alban-Meneses, C.J.; Icaza, V.M.S.; Alban, C.L.M. La salud en los pueblos indígenas: Atención primaria e interculturalidad. Rev. Minerva Investig. Científica 2020, 1, 23–34. [Google Scholar] [CrossRef]
- ILO. Convenio 169 Sobre Pueblos Indígenas y Tribales en Países Independientes. 1989. Ley169_modificado. Available online: www.gob.mx (accessed on 11 July 2022).
- United Nations. Declaración de las Naciones Unidas Sobre los Derechos de los Pueblos Indígenas. 2008. DRIPS_es.pdf. Available online: un.org (accessed on 11 July 2022).
- Chino, M.; DeBruyn, L. Building True Capacity: Indigenous Models for Indigenous Communities. Commentary. Am. J. Public Health 2006, 96, 596–599. [Google Scholar] [CrossRef] [PubMed]
- Cochran, P.; Marshall, C.; Garcia-Dowing, C.; Kendall, E.; Cook, D.; McCubbin, L.; Gover, R.M. Indigenous Ways of Knowing: Implications for Participatory Research and Community. Am. J. Public Health 2011, 98, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Kryzanowski, J.A.; McIntyre, L. A Holistic Model for the Selection of Environmental Assessment Indicators to Assess the Impact of Industrialization on Indigenous Health. Can. J. Public Health 2011, 102, 112–117. [Google Scholar] [CrossRef]
- Gibson, O.; Lisy, K.; Davy, C.; Aromataris, E.; Kite, E.; Lockwood, C.; Riitano, D.; McBride, K.; Brown, A. Enablers and barriers to the implementation of primary health care interventions for Indigenous people with chronic diseases: A systematic review. Implement. Sci. 2015, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Dawson, A.; Harfield, S.; Davy, C.; Baker, A.; Kite, E.; Aitken, G.; Morey, K.; Braunack-Mayer, A.; Brown, A. Aboriginal community-controlled aged care: Principles, practices and actions to integrate with primary health care. Prim. Health Care Res. Dev. 2021, 22, E50. [Google Scholar] [CrossRef] [PubMed]
- Urrego-Rodríguez, J.H. Indigenous struggles for an own and intercultural fundamental right to health in Colombia. Saúde Debate 2020, 44 (Suppl. S1), 79–90. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Role | Number | Sex (Female/Male) | Age | Communal Territory | Distance to Municipal Capital (Walking) |
|---|---|---|---|---|---|
| Traditional authorities: governors, other members of councils | 5 | 5 M | 42–65 | Pialapí, Nulpes Medio, Alto, Pueblo Viejo, Gualcalá, Vegas | 12–24 h |
| Midwives (males) | 3 | 3 M | 34–58 | Nulpes, Pueblo Viejo | 18 h |
| Healers | 3 | 1 F, 2 M | 45–62 | Gualcalá | 24 h |
| Pregnant women | 2 | 2 F | 23, 35 | Nulpes | 18 h |
| Wise elder | 1 | 1 M | 88 | Pueblo Viejo | 14 h |
| Leaders and representatives | 2 | 2 M | 33, 42 | Vegas, Integrado M | 8–12 h |
| Other Indigenous from communal territories | 2 | 1 F, 1 M | 27, 53 | Guaduales; Milagrosa | 18 h |
| “[Awá Women] Feel a Lack of Trust, Embarrassment When Being Examined, Looked at or Touched by Western Physicians” “the Food They Give [in the] Hospital Is Not Good, Upset the Stomach, They Don’t Like It (Midwife from the Pueblo Viejo Communal Territory) |
| “[to get health care we have to] stay up until four in the morning and stand in line to get a number” |
| “it takes several days for someone who is sick to be treated [in the] hospital” |
| “the hospital discharges Awá women who recently give birth the day after the birth, so they go home, regardless of their having to walk many hours on foot after childbirth” |
| “medical attention at the Ricaurte hospital in the communal territories is at most a one-week visit or less per year” |
| “…we need a group of doctors or a health team that rotates from here to there, that visits the Awá families weekly, sees the mom, the dad, the children, sees what their housing is like, the water, that comes back again and visits all the three hundred plus families in this communal territory and is permanently around the community. But this health group should of course also include the traditional physicians from here, where the midwife can provide care, other Awá traditional doctors of ours, be made up of Western medicine with a doctor, nurse, health technician, sanitation, and have functions in the community, so if tomorrow a health problem presents itself we find that health team in the communal territory, they provide us with medical care and also with a traditional physician and in that way the Awá family begins to be protected, to be cared for by a health team, given guidance, vaccinations, prenatal care if the father gives his permission, examine someone who is coughing, collect phlegm for tuberculosis, that there be health care like we have never had in the communal territories, but health care through our concerted efforts, then the community understands that what we are going to do now is see how health care is going to be for us Awá” (interview with a member of the communal territory) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casas Cruz, H.M.; Pelcastre-Villafuerte, B.E.; Arenas-Monreal, L.; Ruiz-Rodríguez, M. Concerted Model of Healthcare for Awá Indigenous of Nariño, Colombia. Int. J. Environ. Res. Public Health 2022, 19, 12250. https://doi.org/10.3390/ijerph191912250
Casas Cruz HM, Pelcastre-Villafuerte BE, Arenas-Monreal L, Ruiz-Rodríguez M. Concerted Model of Healthcare for Awá Indigenous of Nariño, Colombia. International Journal of Environmental Research and Public Health. 2022; 19(19):12250. https://doi.org/10.3390/ijerph191912250
Chicago/Turabian StyleCasas Cruz, Harold Mauricio, Blanca Estela Pelcastre-Villafuerte, Luz Arenas-Monreal, and Myriam Ruiz-Rodríguez. 2022. "Concerted Model of Healthcare for Awá Indigenous of Nariño, Colombia" International Journal of Environmental Research and Public Health 19, no. 19: 12250. https://doi.org/10.3390/ijerph191912250
APA StyleCasas Cruz, H. M., Pelcastre-Villafuerte, B. E., Arenas-Monreal, L., & Ruiz-Rodríguez, M. (2022). Concerted Model of Healthcare for Awá Indigenous of Nariño, Colombia. International Journal of Environmental Research and Public Health, 19(19), 12250. https://doi.org/10.3390/ijerph191912250