
How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Translation and Cultural Adaptation
2.2. Testing Measurement Properties
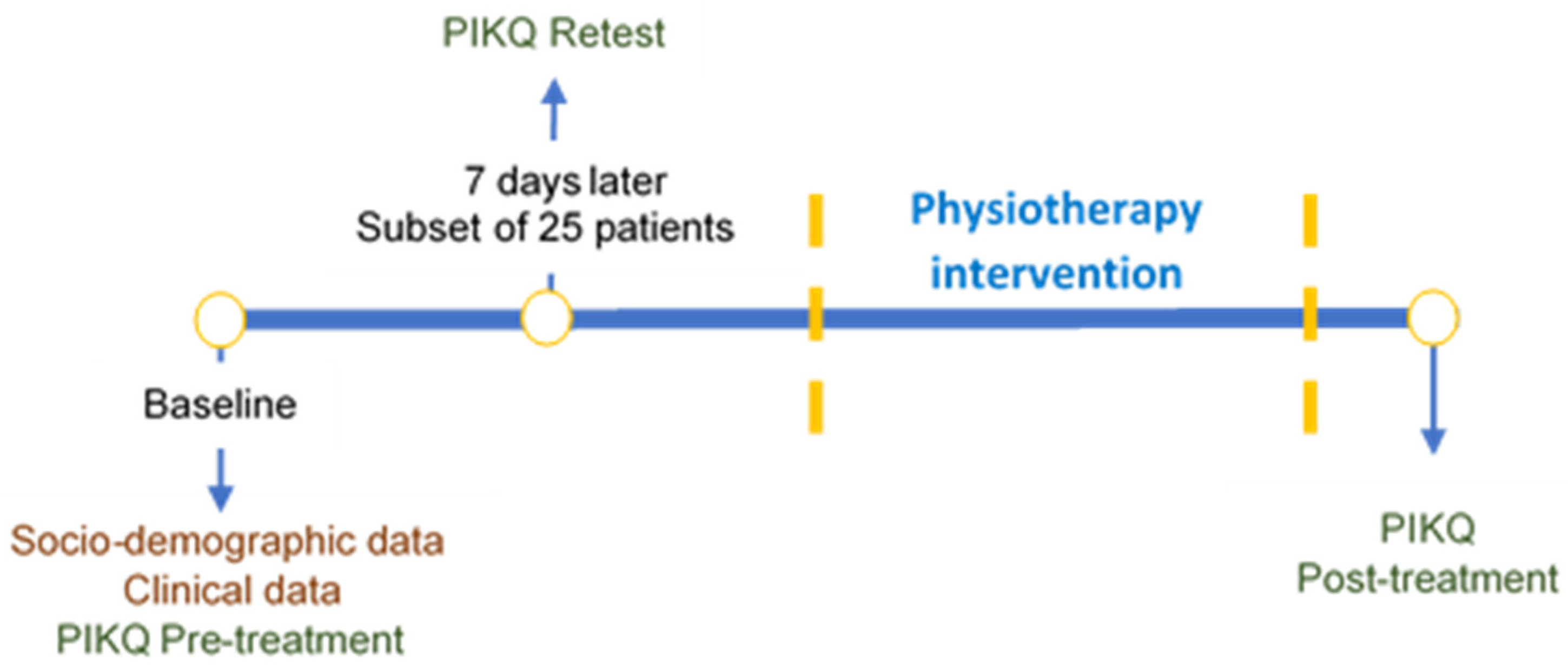
2.2.1. Participants and Procedure
2.2.2. Demographic Data and PIKQ Score Determination
2.2.3. Data Analysis
2.3. Development of the Real Practical Cases
3. Results
3.1. Translation and Cultural Adaptation
3.2. Measurement Properties of the Spanish PIKQ
3.2.1. Characteristics of Participants, Interpretability, and Feasibility of PIKQ
3.2.2. Validity
3.2.3. Reliability
3.2.4. Responsiveness
3.3. Practical Cases Proposal
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weber, A.M.; Abrams, P.; Brubaker, L.; Cundiff, G.; Davis, G.; Dmochowski, R.R. The standardization of termi-nology for researchers in female pelvic floor disorders. Int. Urogynecology J. 2001, 12, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, I.; Barber, M.D.; Burgio, K.L.; Kenton, K.; Meikle, S.; Schaffer, J.; Spino, C.; Whitehead, W.E.; Wu, J.; Brody, D.J. Prevalence of symptomatic pelvic floor disorders in US women. JAMA 2008, 300, 1311. [Google Scholar] [CrossRef]
- Wu, J.M.; Vaughan, C.P.; Goode, P.S.; Redden, D.T.; Burgio, K.L.; Richter, H.E.; Markland, A.D. Prevalence and Trends of Symptomatic Pelvic Floor Disorders in U.S. Women. Obstet. Gynecol. 2014, 123, 141–148. [Google Scholar] [CrossRef]
- Jundt, K.; Peschers, U.; Kentenich, H. The Investigation and Treatment of Female Pelvic Floor Dysfunction. Dtsch. Aerzteblatt Online 2015, 112, 564–574. [Google Scholar] [CrossRef]
- Huang, A.J.; Brown, J.S.; Kanaya, A.M.; Creasman, J.M.; Ragins, A.I.; Eeden, S.K.V.D.; Thom, D.H. Quality-of-Life Impact and Treatment of Urinary Incontinence in Ethnically Diverse Older Women. Arch. Intern. Med. 2006, 166, 2000. [Google Scholar] [CrossRef]
- Jelovsek, J.E.; Barber, M.D. Women seeking treatment for advanced pelvic organ prolapse have decreased body image and quality of life. Am. J. Obstet. Gynecol. 2006, 194, 1455–1461. [Google Scholar] [CrossRef]
- Milsom, I.; Altman, D.; Lapitan, M.C.; Nelson, R.; Sillén, U.; Thom, D. Epidemiology of urinary (UI) and faecal (FI) in-continence and pelvic organ prolapse (POP). In Incontinence, 4th International Consultation on Incontinence; Abrams, P., Cardozo, L., Khoury, S., Eds.; Health Publication Ltd.: Paris, France, 2009; pp. 37–111. [Google Scholar]
- Rizk, D.E.E.; Shaheen, H.; Thomas, L.; Dunn, E.; Hassan, M.Y. The Prevalence and Determinants of Health Care-Seeking Behavior for Urinary Incontinence in United Arab Emirates Women. Int. Urogynecology J. 1999, 10, 160–165. [Google Scholar] [CrossRef]
- Minassian, V.A.; Drutz, H.P.; Al-Badr, A. Urinary incontinence as a worldwide problem. Int. J. Gynecol. Obstet. 2003, 82, 327–338. [Google Scholar] [CrossRef]
- Liebergall-Wischnitzer, M.; Cnaan, T.; Hochner, H.; Paltiel, O. Self-reported Prevalence of and Knowledge About Urinary Incontinence Among Community-Dwelling Israeli Women of Child-Bearing Age. J. Woundostomy Cont. Nurs. 2015, 42, 401–406. [Google Scholar] [CrossRef]
- Sampselle, C.M.; Messer, K.L.; Seng, J.S.; Raghunathan, T.E.; Hines, S.H.; Diokno, A.C. Learning outcomes of a group be-havioral modification program to prevent urinary incontinence. Int. Urogynecology J. 2005, 16, 441–446. [Google Scholar] [CrossRef]
- World Health Organization. Therapeutic Patient Education: Continuing Education Programmes for Health Care Providers in The Field of Prevention of Chronic Diseases; World Health Organization: Copenhagen, Denmark, 1998. [Google Scholar]
- Alewijnse, D.; Mesters, I.E.; Metsemakers, J.F.; van den Borne Bart, H.W. Program development for promoting adher-ence during and after exercise therapy for urinary incontinence. Patient Educ. Couns. 2002, 48, 147–160. [Google Scholar] [CrossRef]
- Geoffrion, R.; Robert, M.; Ross, S.; Van Heerden, D.; Neustaedter, G.; Tang, S.; Milne, J. Evaluating patient learning after an educational program for women with incontinence and pelvic organ prolapse. Int. Urogynecology J. 2009, 20, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- McFall, S.L.; Yerkes, A.M.; Cowan, L.D. Outcomes of a small group educational intervention for urinary incontinence: Episodes of incontinence and other urinary symptoms. J. Aging Health 2000, 12, 250–267. [Google Scholar] [CrossRef]
- Shah, A.D.; Shott, S.; Kohli, N.; Wu, J.M.; Catlin, S.; Hoyte, L. Do racial differences in knowledge about urogynecologic issues exist? Int. Urogynecology J. 2008, 19, 1371–1378. [Google Scholar] [CrossRef]
- Whitford, H.M.; Alder, B.; Jones, M. A cross-sectional study of knowledge and practice of pelvic floor exercises dur-ing pregnancy and associated symptoms of stress urinary incontinence in North-East Scotland. Midwifery 2007, 23, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Rizk, D.E.; El-Safty, M.M. Female pelvic floor dysfunction in the Middle East: A tale of three factors—culture, reli-gion and socialization of health role stereotypes. Int. Urogynecology J. 2006, 17, 436–438. [Google Scholar] [CrossRef]
- Shah, A.D.; Massagli, M.P.; Kohli, N.; Rajan, S.S.; Braaten, K.P.; Hoyte, L. A reliable, valid instrument to assess patient knowledge about urinary incontinence and pelvic organ prolapse. Int. Urogynecology J. 2008, 19, 1283–1289. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: Oxford, UK, 2015; pp. 9, 12, 131, 159, 230–231. [Google Scholar]
- Rothman, M.; Burke, L.; Erickson, P.; Leidy, N.K.; Patrick, D.L.; Petrie, C.D. Use of Existing Patient-Reported Outcome (PRO) Instruments and Their Modification: The ISPOR Good Research Practices for Evaluating and Documenting Content Validity for the Use of Existing Instruments and Their Modification PRO Task Force Report. Value Health 2009, 12, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached interna-tional consensus on taxonomy, terminology, and definitions of measurement properties for health-related pa-tient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef]
- Davidson, M.; Keating, J. Patient-reported outcome measures (PROMs): How should I interpret reports of meas-urement properties? A practical guide for clinicians and researchers who are not biostatisticians. Br. J. Sports Med. 2014, 48, 792–796. [Google Scholar] [CrossRef] [PubMed]
- De Andrade, R.L.; Bø, K.; Antonio, F.I.; Driusso, P.; Mateus-Vasconcelos, E.C.L.; Ramos, S. An education program about pelvic floor muscles improved women’s knowledge but not pelvic floor muscle function, urinary inconti-nence or sexual function: A randomised trial. J. Physiother. 2018, 64, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.L.; Ryan, C.G.; Martin, D.J. Pain neurophysiology education for the management of individuals with chronic low back pain: A systematic review and meta-analysis. Man. Ther. 2011, 16, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The Effect of Neuroscience Education on Pain, Disability, Anxiety, and Stress in Chronic Musculoskeletal Pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef]
- Gagnayre, R.; Marchand, C.; Pinosa, C.; Brun, M.; Billot, D.; Iguemane, J. Approche conceptuelle d’un dispositif d’évaluation pédagogique du patient. Pédagogie Médicale 2006, 7, 31–42. [Google Scholar] [CrossRef][Green Version]
- Toprak Celenay, S.; Akbayrak, T.; Kaya, S.; Ekici, G.; Beksac, S. Validity and reliability of the Turkish version of the Pelvic Floor Distress Inventory-20. Int. Urogynecology J. 2012, 23, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.Y.; Chowdhury, H.R.; Qusar, M.; Hafez, M.A. Cross cultural adaptation & psychometric validation of re-search instruments: A methodological review. J. Behav. Health 2016, 5, 129–136. [Google Scholar]
- Chen, C.C.G.; Cox, J.T.; Yuan, C.; Thomaier, L.; Dutta, S. Knowledge of pelvic floor disorders in women seeking prima-ry care: A cross-sectional study. BMC Fam. Pract. 2019, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mandimika, C.L.; Murk, W.; McPencow, A.M.; Lake, A.; Wedderburn, T.; Collier, C.H.; Connell, K.A.; Guess, M.K. Knowledge of pelvic floor disorders in a population of community-dwelling women. Am. J. Obstet. Gynecol. 2014, 210, 165.e1–165.e9. [Google Scholar] [CrossRef]
- Van Der Vleuten Cees, P.M.; Schuwirth, L.W. Assessing professional competence: From methods to programmes. Med. Educ. 2005, 39, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Janssen-Noordman, A.; Merriënboer, J.J.; Van der Vleuten Cees, P.M.; Scherpbier, A.J. Design of integrated practice for learning professional competences. Med. Teach. 2006, 28, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Husted, J.A.; Cook, R.J.; Farewell, V.T.; Gladman, D.D. Methods for assessing responsiveness: A critical review and recommendations. J. Clin. Epidemiol. 2000, 53, 459–468. [Google Scholar] [CrossRef]
- Barber, M.D.; Walters, M.D.; Cundiff, G.W.; PESSRI Trial Group. Responsiveness of the Pelvic Floor Distress Inventory (PFDI) and Pelvic Floor Impact Questionnaire (PFIQ) in women undergoing vaginal surgery and pessary treatment for pelvic organ prolapse. Obs. Gynecol. 2006, 194, 1492–1498. [Google Scholar]


{kind=link}
| Competences | Dimensions |
|---|---|
| Identify, analyze | Identify and analyze the significant elements, summarize and integrate the different parts, organize the elements and the connection among them, deduce some ideas and/or results and provide some conclusions. |
| Decision making | Apply systematic methods to make decisions, compile and analyze data to take the most suitable decision, show certainty, be consistent with the solution adopted, collaborate with other on taking decisions. |
| Communicate needs | Intonation and volume, level of preparation of exposition, gestures and body language, clarity of exposure, ability to answer questions, speech clarity, structure, and sequence within the speech. |
| Problem-solving | Define the problem, identify strategies, propose solutions/hypotheses, evaluate potential solutions, implement solutions, evaluate results. |
| Know how to manage | Identify the different resources, access resources, use resources efficiently, assess the suitability of resources based on the results. |
| Patients Group (n = 147) | Experts Group (n = 128) | |
|---|---|---|
| Age, years. (SD) | 38.57 (8.21) | 24.18 (7.59) |
| Education level: | ||
| Primary School | 16 (10.9) | 0 (0) |
| High School | 49 (33.3) | 0 (0) |
| College or University | 82 (55.8) | 127 (100) |
| Occupational Status | ||
| Unemployed | 30 (20.4) | 0 (0) |
| Employed | 115 (78.2) | 28 (22) |
| Student | 2 (1.4) | 100 (78) |
| Incomes | ||
| <EUR 12,000/year | 12 (8.2) | 28 (22) |
| EUR 12,000–24,000/year | 52 (35.4) | - |
| EUR 24,000–36,000/year | 35 (23.8) | 100 (78) |
| EUR 36,000–48,000/year | 29 (19.7) | - |
| >EUR 48,000 | 19 (12.9) | - |
| Vaginal delivery: | ||
| None | 7 (4.8) | 120 (93.7) |
| One | 92 (62.6) | 5 (3.9) |
| Two | 40 (27.2) | 2 (1.5) |
| Three or more | 8 (5.4) | 1 (0.7) |
| Cesarean | 11 (7.5) | 1 (0.7) |
| Menopause | 18 (12.2) | 2 (1.5) |
| Urogynecological symptoms | ||
| SUI | 57 (38.7) | - |
| UUI | 17 (11.5) | - |
| POP | 12 (8.2) | - |
| Effect Size (95%CI) | SRM (95%CI) | ||||
|---|---|---|---|---|---|
| Patients (n = 147) | PIKQ-IU | 8.99 (2.05) | 11.24 (0.66) | 1.09 (0.95–1.2) | 1.16 (1.01–1.32) |
| PIKQ-POP | 7.15 (2.79) | 10.38 (0.53) | 1.16 (0.99–1.34) | 1.15 (0.99–1.33) | |
| Experts (n = 128) | PIKQ-IU | 11.92 (0.27) | - | - | - |
| PIKQ-POP | 11.96 (0.23) | - | - | - |
| SEM | SDCind | SDCgroup | ICC (95%CI) | |||
|---|---|---|---|---|---|---|
| PIKQ-IU | 8.56 (2.02) | 8.52 (2.04) | 0.15 | 0.42 | 0.017 | 0.995 (0.989–0.998) |
| PIKQ-POP | 7.04 (2.56) | 7.04 (2.42) | 0.37 | 1.03 | 0.04 | 0.977 (0.951–0.990) |
| Session | Topic | Contents | Learning Tools | Activities | Assessment Tools |
|---|---|---|---|---|---|
| 1 | What do you know about PFD? | - Knowledge about the PFD symptoms and treatment options. - Beliefs about causes and evolution of PFD - Possible resources and self-efficacy facing a PFD | - Exploratory motivational interview - PIKQ - Real practical cases | - To fill in the PIKQ - To detect the PFD symptoms, the risk factors, and the treatment options of each real practical case | - PIKQ & real practical cases rubric are discussed - The notes of the contents in a notebook are requested and reviewed |
| 2 | Why PF is important? | - PF anatomy - Where PFM are - PFM function - What PFD are - Risk factors of PFD | - Anatomical prints - Pelvic bones and muscles anatomical model - Small ball | - To identify the boundaries and parts of the PF - To spatially locate the PFM in a picture and in themselves - To relate structures to functions, risk factors, and PFD | - A drawing of the PF anatomy is requested - A task of connecting anatomical structures with different functions is requested |
| 3 | How to contract the PFM correctly? | - Visualization of self PFM contraction - How to contract PFM - How to perform PFM exercises - Identifying her own PFD risk factors | - Ultrasound images of the PF and PFM contraction - Ultrasound biofeedback - Physiotherapist manual and auditory feedback - PFD risk factors sheet | - To understand the correct movement of the PFM - To watch and sense the correct contraction of the PFM - To contract the PFM in supine and sitting positions - To identify unwanted contraction of muscles close to the PFM - To fill in the PFD risk factors sheet at home. | - To review recordings of PFM contractions and identify the correct ones is requested - PFM contraction is assessed through vaginal palpation and transabdominal ultrasound - A diary of the PFM contractions practice is requested - The PFD risk factors sheet is discussed |
| 4 | How to relax the PFM and empty your bladder adequately? What are your voiding routines? | - Coordination between PFM and breathing - How to relax PFM - Urinary, defecatory and liquid intake patient habits | - Anatomical prints - Physiotherapist manual and auditory feedback - Motor imagery - Voiding and intake diary | - To try to contract the PFM when breathing out - To try to relax the PFM when breathing in - To fill in the voiding and intake diary during three consecutive days | - On-site test on PFM contraction and relaxation - The voiding and intake diary is requested and saved for later review |
| 5 | How important is the position of the pelvis? | - Pelvis positions during PFM exercises - Pelvis position during daily tasks - Pelvis position during micturition and defecation | - Anatomical prints - Pelvic bones and muscles anatomical model - Swiss ball | - To identify and practice the neutral pelvic position and the anterior and posterior pelvic tilt sitting and standing - To deduce which pelvic alignment assists each excretory process | - On-site test on pelvic alignment |
| 6 | What is the role of the PFM in intra-abdominal pressure? | - Coordination between PFM and abdominal muscles - Knack maneuver - How to lift weight | - Anatomical prints - Ultrasound biofeedback - A mirror - A light weight | - To contract the PFM and deep abdominal muscles when breathing out - To practice the PFM contraction before and during coughing and head lifting - To practice the knack when lifting a weight | - Ultrasound checking - A diary of the knack maneuver practice is requested |
| 7 | What are the best habits for the pelvic floor? | - Voiding ideal frequency - Infection prevention - Use of vaginal weight devices - Role of the pelvic floor in sexual intercourse | - Anatomical prints - A balloon - Vaginal weights | - To analyze the voiding frequency - To understand how the detrusor muscle and the PFM work - To list tips to avoid urine infections and improve sexual practice - To understand the use and guidelines for the use of vaginal devices | - To answer a short test about bladder function - To prepare your own “do’s and dont’s” as purposes to improve |
| 8 | What have I learned? | - All the contents of the program (session 1 to 7) | - Exploratory motivational interview - PIKQ - Real practical cases - Anatomical prints | - To fill in the PIKQ again - To detect the PFD symptoms, the risk factors, and the treatment options of each real practical case - To propose therapeutic resources to improve a PFD | - PIKQ & rubric of real practical cases are discussed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Sánchez, B.; Arranz-Martín, B.; Navarro-Brazález, B.; Vergara-Pérez, F.; Bailón-Cerezo, J.; Torres-Lacomba, M. How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders. Int. J. Environ. Res. Public Health 2021, 18, 2377. https://doi.org/10.3390/ijerph18052377
Sánchez-Sánchez B, Arranz-Martín B, Navarro-Brazález B, Vergara-Pérez F, Bailón-Cerezo J, Torres-Lacomba M. How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders. International Journal of Environmental Research and Public Health. 2021; 18(5):2377. https://doi.org/10.3390/ijerph18052377
Chicago/Turabian StyleSánchez-Sánchez, Beatriz, Beatriz Arranz-Martín, Beatriz Navarro-Brazález, Fernando Vergara-Pérez, Javier Bailón-Cerezo, and María Torres-Lacomba. 2021. "How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders" International Journal of Environmental Research and Public Health 18, no. 5: 2377. https://doi.org/10.3390/ijerph18052377
APA StyleSánchez-Sánchez, B., Arranz-Martín, B., Navarro-Brazález, B., Vergara-Pérez, F., Bailón-Cerezo, J., & Torres-Lacomba, M. (2021). How Do We Assess Patient Skills in a Competence-Based Program? Assessment of Patient Competences Using the Spanish Version of the Prolapse and Incontinence Knowledge Questionnaire and Real Practical Cases in Women with Pelvic Floor Disorders. International Journal of Environmental Research and Public Health, 18(5), 2377. https://doi.org/10.3390/ijerph18052377