
Using GIS to Estimate Population at Risk Because of Residence Proximity to Asbestos Processing Facilities in Colombia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
- -
- For the year 2005: population counts by five-year age groups for urban sections and rural sectors.
- -
- For the year 2018: population counts by five-year age groups for urban and rural sections.
- -
- Location of the asbestos facilities and the mine using satellite images integrated into a GIS via a web server and the creation of a point for each site.
- -
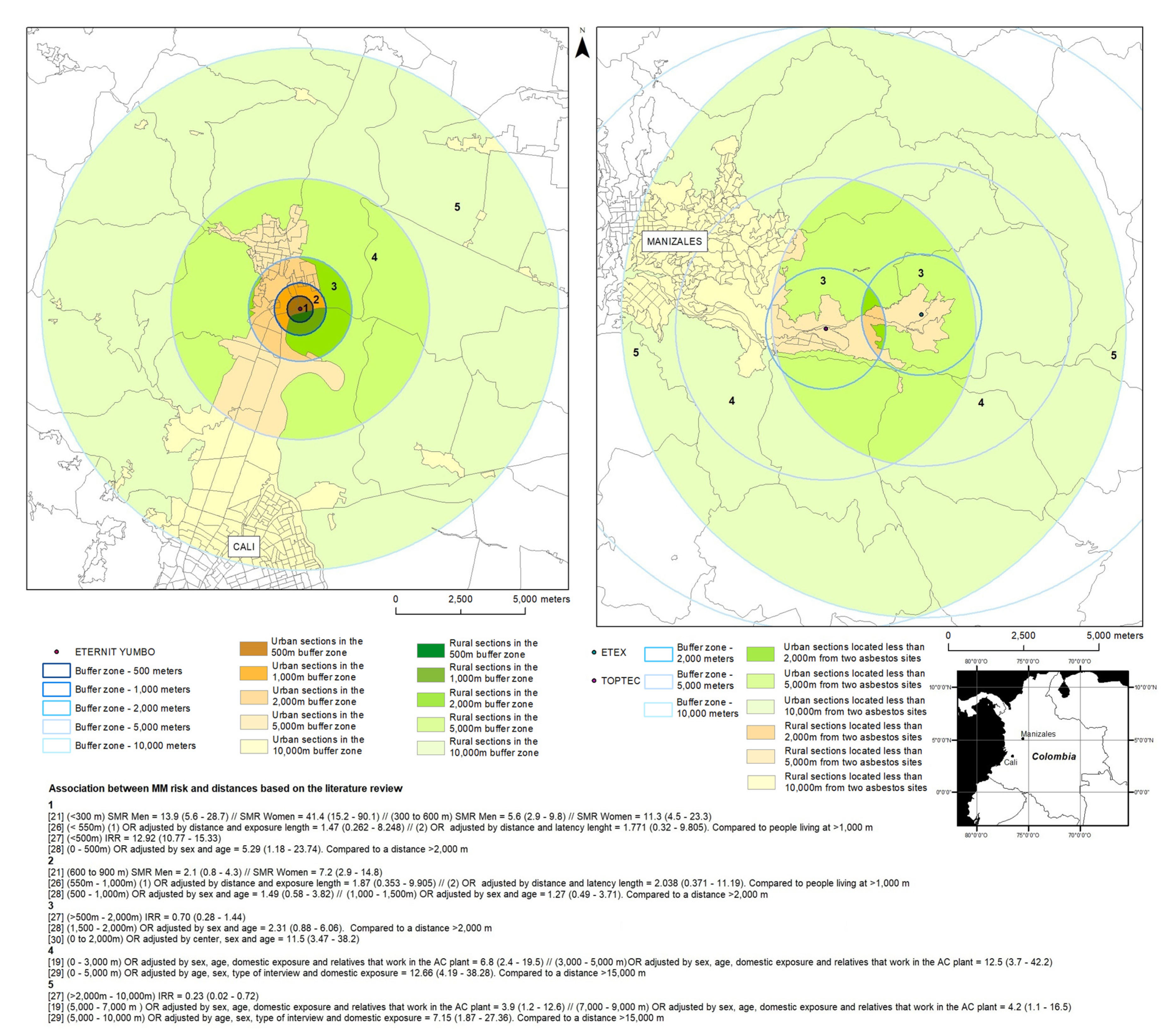
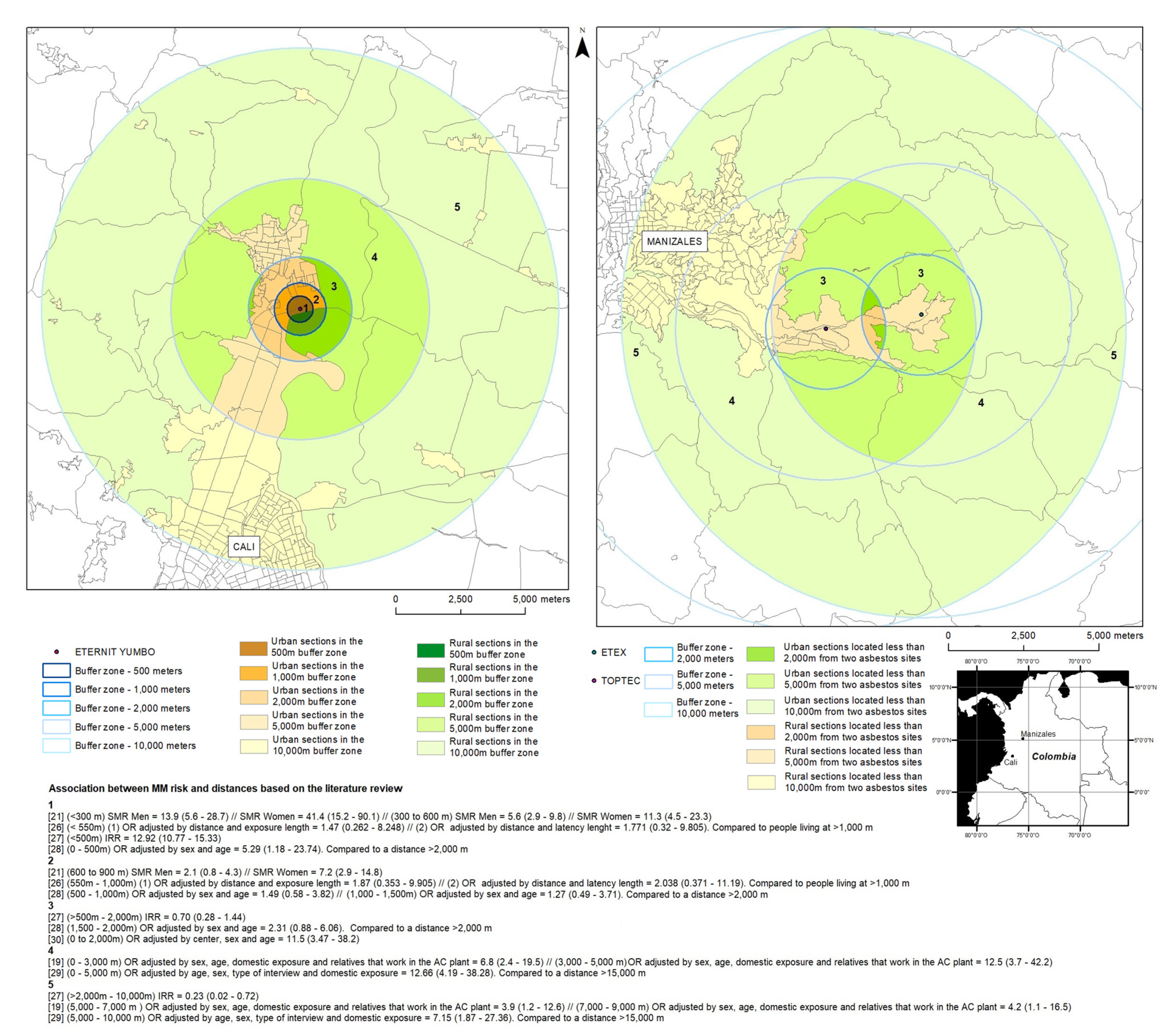
- Creation of buffer zones using the distances identified in the literature review.
- -
- Calculation of the individual area of the MGN polygons (area A).
- -
- Use of the “intersection” tool under Arcgis between each buffer zone and the polygons of the urban sections (2005 and 2018), rural sectors (2005), and rural sections (2018).
- -
- Calculation of the area of the polygons resulting from the intersection between the buffers and the MGN layers (area B).
- -
- Calculation of the ratio between area B and area A. This ratio was applied to the census populations in cases in which polygons of the MGN were not fully covered by a buffer.
- -
- Integration of the census data by table joining the DANE data and the “buffer/MGN polygons” intersection layers.
- -
- Exportation of the attribute tables in text format, followed by post-processing (i.e., the application of the ratio between area B to area A and the corresponding population), and estimation of the number of people residing there, categorized in five-year age groups, within the concentric radii surrounding the asbestos processing facilities and the mine. This procedure was done for both years 2005 and 2018. When fractional numbers were obtained for the population estimates, the value was rounded to the nearest integer, which may result in some slight differences in the calculations of row and column sums in the tables presented in the results.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ATSDR. Toxicological Profile for Asbestos. U.S. Department of Health and Human Services. Atlanta; 2001. Available online: http://www.atsdr.cdc.gov/toxprofiles/tp61.pdf (accessed on 3 November 2021).
- CDC. Asbestos Fibers and Other Elongate Mineral Particles: State of the Science and Roadmap for Research. Revised Edition. Curr. Intell. Bull. 2011, 62. Available online: https://www.cdc.gov/niosh/docs/2011-159/pdfs/2011-159.pdf (accessed on 3 November 2021).
- Campbell, W.J.; Blake, R.L.; Brown, L.L.; Cather, E.E.; Sjoberg, J.J. Selected Silicate Minerals and Their Asbestiform Varieties: Mineralogical Definitions and Identification-Characterization; Dept. of the Interior, Bureau of Mines: Washington, WA, USA, 1977.
- Virta, R.L. Asbestos: Geology, Mineralogy, Mining, and Uses by Open-File Report 02-149; US Department of the Interior, US Geological Survey: Washington, DC, USA, 2002; pp. 1–28. Available online: http://pubs.usgs.gov/of/2002/of02-149/of02-149.pdf (accessed on 3 November 2021).
- Ross, M.; Langer, A.M.; Nord, G.L.; Nolan, R.P.; Lee, R.J.; Van Orden, D.; Addison, J. The mineral nature of asbestos. Regul. Toxicol. Pharmacol. 2008, 52 (Suppl. 1), S26–S30. [Google Scholar] [CrossRef]
- Addison, J.; McConnell, E.E. A review of carcinogenicity studies of asbestos and non-asbestos tremolite and other amphiboles. Regul. Toxicol. Pharmacol. 2008, 52, S187–S199. [Google Scholar] [CrossRef] [PubMed]
- IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Asbestos (Chrysotile, Amosite, Crocidolite, Tremolite, Actinolite, and Anthophyllite). IARC Monogr.—Vol. 100C. 2012, pp. 219–294. Available online: http://monographs.iarc.fr/ENG/Monographs/vol100C/index.php (accessed on 3 November 2021).
- Kang, D.M.; Kim, J.E.; Kim, Y.K.; Lee, H.H.; Kim, S.Y. Occupational burden of Asbestos-related diseases in Korea, 1998–2013: Asbestosis, mesothelioma, lung Cancer, laryngeal Cancer, and ovarian Cancer. J. Korean Med. Sci. 2018, 33, e226. [Google Scholar] [CrossRef] [PubMed]
- Pasetto, R.; Terracini, B.; Marsili, D.; Comba, P. Occupational burden of asbestos-related cancer in Argentina, Brazil, Colombia and Mexico. Ann. Glob. Health 2014, 80, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Mirabelli, D.; Tunesi, S.; Terracini, B.; Magnani, C. Pleural mesothelioma and occupational and non-occupational asbestos exposure: A case-control study with quantitative risk assessment. Occup. Environ. Med. 2016, 73, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Carlin, D.J.; Larson, T.C.; Pfau, J.C.; Gavett, S.H.; Shukla, A.; Miller, A.; Hines, R. Current research and opportunities to address environmental asbestos exposures. Environ. Health Perspect 2015, 123, A194–A197. [Google Scholar] [CrossRef] [Green Version]
- Marsili, D.; Terracini, B.; Santana, V.S.; Ramos-Bonilla, J.P.; Pasetto, R.; Mazzeo, A.; Loomis, D.; Comba, P.; Algranti, E. Prevention of asbestos related disease in countries currently using asbestos. Int. J. Environ. Res. Public Health 2016, 13, 494. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.K.; Son, M.; Jin, Y.W.; Park, S.; Lee, W.J. Variations of lung cancer risk from asbestos exposure: Impact on estimation of population attributable fraction. Ind. Health 2013, 51, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, M.; Luce, D. The health impact of nonoccupational exposure to asbestos: What do we know? Eur. J. Cancer Prev. 2009, 18, 489–503. [Google Scholar] [CrossRef] [Green Version]
- IBAS. Current Asbestos Bans. 2021. Available online: http://ibasecretariat.org/alpha_ban_list.php (accessed on 20 January 2021).
- Congreso. Ley 1968 Por el cual se Prohíbe el uso de Asbesto en el Territorio Nacional y se Establecen Garantías de Proteccón a la Salud de los Colombianos. 2019. Available online: https://dapre.presidencia.gov.co/normativa/normativa/LEY%201968%20DEL%2011%20DE%20JULIO%20DE%202019.pdf (accessed on 15 April 2021).
- ILO-WHO. Outline for the Development of National Programmes for Elimination of Asbestos Related Diseases; ILO-WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Magnani, C.; Terracini, B.; Ivaldi, C.; Botta, M.; Mancini, A.; Andrion, A. Pleural malignant mesothelioma and non-occupational exposure to asbestos in Casale Monferrato, Italy. Occup. Environ. Med. 1995, 52, 362–367. [Google Scholar] [CrossRef]
- Maule, M.M.; Magnani, C.; Dalmasso, P.; Mirabelli, D.; Merletti, F.; Biggeri, A. Modeling mesothelioma risk associated with environmental asbestos exposure. Environ. Health Perspect. 2007, 115, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Kurumatani, N. Asbestos fiber concentration in the area surrounding a former asbestos cement plant and excess mesothelioma deaths in residents. Am. J. Ind. Med. 2009, 52, 790–798. [Google Scholar] [CrossRef]
- Kurumatani, N.; Kumagai, S. Mapping the risk of mesothelioma due to neighborhood asbestos exposure. Am. J. Respir. Crit. Care Med. 2008, 178, 624–629. [Google Scholar] [CrossRef]
- Musk, A.; Reid, A.; Olsen, N.; Hobbs, M.; Armstrong, B.; Franklin, P.; Hui, J.; Layman, L.; Merler, E.; Brims, F.; et al. The Wittenoom legacy. Int. J. Epidemiol. 2020, 49, 467–476. [Google Scholar] [CrossRef]
- Naik, S.; Lewin, M.; Young, R.; Dearwent, S.; Lee, R. Mortality from asbestos-associated disease in Libby, Montana 1979–2011. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 207–213. [Google Scholar] [CrossRef] [Green Version]
- DANE. Censos Nacionales de Población y Vivienda. 2020. Available online: http://systema59.dane.gov.co/bincol/rpwebengine.exe/PortalAction?lang=esp (accessed on 15 May 2021).
- DANE. Marco Geoestadistico Nacional—MGN. 2020. Available online: https://geoportal.dane.gov.co/servicios/descarga-y-metadatos/descarga-mgn-marco-geoestadistico-nacional/ (accessed on 15 May 2021).
- Vimercati, L.; Cavone, D.; Delfino, M.; Caputi, A.; De Maria, L.; Sponselli, S.; Corrado, V.; Ferri, G.; Serio, G. Asbestos Air Pollution: Description of a Mesothelioma Cluster Due to Residential Exposure from an Asbestos Cement Factory. Int. J. Environ. Res. Public Health 2020, 17, 2636. [Google Scholar] [CrossRef] [Green Version]
- Tarrés, J.; Albertí, C.; Martínez-Artés, X.; Abós-Herràndiz, R.; Rosell-Murphy, M.; García-Allas, I.; Krier, I.; Cantarell, G.; Gallego, M.; Canela-Soler, J.; et al. Pleural mesothelioma in relation to meteorological conditions and residential distance from an industrial source of asbestos. Occup. Environ. Med. 2013, 70, 588–590. [Google Scholar] [CrossRef]
- Musti, M.; Pollice, A.; Cavone, D.; Dragonieri, S.; Bilancia, M. The relationship between malignant mesothelioma and an asbestos cement plant environmental risk: A spatial case-control study in the city of Bari (Itali). Int. Arch. Occup. Environ. Health 2009, 82, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Airoldi, C.; Magnani, C.; Lazzarato, F.; Mirabelli, D.; Tunesi, S.; Ferrante, D. Environmental asbestos exposure and clustering of malignant mesothelioma in community: A spatial analysis in a population-based case–control study. Environ. Health 2021, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Magnani, C.; Agudo, A.; González, C.A.; Andrion, A.; Calleja, A.; Chellini, E.; Dalmasso, P.; Escolar, A.; Hernández, S.; Ivaldi, C.; et al. Multicentric study on malignant pleural mesothelioma and non-occupational exposure to asbestos. Br. J. Cancer 2000, 83, 104–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, B. Exposure to airborne amphibole structures and health risks: Libby, Montana. Regul. Toxicol. Pharmacol. 2008, 52, S97–S109. [Google Scholar] [CrossRef]
- Noonan, C.; Conway, K.; Landguth, E.; McNew, T.; Linker, L.; Pfau, J.; Black, B.; Szeinuk, J.; Flores, R. Multiple pathway asbestos exposure assessment for a Superfund community. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.; Nevill, M. Occupational and environmental mesotheliomas due to crocidolite mining activities in Wittenoom, Western Australia. Scand. J. Work Environ. Health 1995, 21, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Hansen, J.; De Klerk, N.H.; Musk, A.W.; Hobbs, M.S. Environmental exposure to crocidolite and mesothelioma: Exposure-response relationship. Am. J. Respir. Crit. Care Med. 1998, 157, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Kielkowski, D.; Nelson, G.; Rees, D. Risk of mesothelioma from exposure to crocidolite asbestos: A 1995 update of a South African mortality study. Occup. Environ. Med. 2000, 57, 563–567. [Google Scholar] [CrossRef]
- Braun, L.; Kisting, S. Asbestos-related disease in South Africa: The social production of an invisible epidemic. Am. J. Public Health 2006, 96, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Noonan, C. Environmental asbestos exposure and risk of mesothelioma. Ann. Transl. Med. 2017, 5, 234. [Google Scholar] [CrossRef] [Green Version]
- Datosmacro.com Colombia—Piramide de Población. 2020. Available online: https://datosmacro.expansion.com/demografia/estructura-poblacion/colombia (accessed on 15 February 2021).
- Ramos-Bonilla, J.P.; Cely-García, M.F.; Giraldo, M.; Comba, P.; Terracini, B.; Pasetto, R.; Marsili, D.; Ascoli, V.; Lysaniuk, B.; Rodríguez, M.C.; et al. An asbestos contaminated town in the vicinity of an asbestos-cement facility: The case study of Sibaté, Colombia. Environ. Res. 2019, 176, 108464. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, A.; Somigliana, A.; Gemmi, M.; Bernabeo, F.; Savoca, D.; Cavallo, D.; Bertazzi, P. Airborne concentrations of chrysotile asbestos in serpentine quarries and stone processing facilities in Valmalenco. Italy. Ann. Occup. Hyg. 2012, 56, 671–683. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.; Hwang, Y.; Choi, Y.; Kim, S.; Kim, Y. Monitoring and Simulating Environmental Asbestos Dispersion from a Textile Factory. Int. J. Environ. Res. Public Health 2018, 15, 1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, F.; Bihari, V.; Rastogi, S.; Ashquin, M.; Ahmad, I. Environmental health survey in asbestos cement sheets manufacturing industry. Indian J. Occup. Environ. Med. 2007, 11, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Written answer to request from Agencia Nacional de Minería Resumen Histórico de la Producción de “Fibra de Asbesto”. Respuesta No 20173210263811 de la ANM al Derecho de Petición 20175510216022. 2017.
- Written answer to request from Agencia Nacional de Minería Producción asbesto en el municipio de Campamento en el 2018. Respuesta No 20203210306581 de la ANM al Derecho de Petición 20201000569462. 2020.
- Semana La Polémica Mina Que Revivió en Antioquia. Recuperado el 3 de Agosto de 2020; Publicaciones Semana S.A.: Bogotá, Colombia, 7 October 2013. [Google Scholar]
- Counil, E.; Daniau, C.; Isnard, H. Étude de Santé Publique Autour D’une Ancienne Usine de Broyage D’amiante: Le Comptoir des Minéraux et Matières Premières à Aulnay-Sous-Bois (Seine-Saint-Denis)—Pollution Environnementale Entre 1938 et 1975: Impacts Sanitaires et Recommandations. 2007. Available online: https://www.santepubliquefrance.fr/regions/ile-de-france/documents/rapport-synthese/2007/etude-de-sante-publique-autour-d-une-ancienne-usine-de-broyage-d-amiante-le-comptoir-des-mineraux-et-matieres-premieres-a-aulnay-sous-bois-seine2 (accessed on 15 April 2021).
- Cely-García, M.F.; Lysaniuk, B.; Pasetto, R.; Ramos-Bonilla, J.P. The challenges of applying an Activity-Based Sampling methodology to estimate the cancer risk associated with asbestos contaminated landfilled zones. Environ. Res. 2020, 181, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lysaniuk, B.; Cely-García, M.; Mazzeo, A.; Marsili, D.; Pasetto, R.; Comba, P.; Ramos-Bonilla, J.P. Where are the landfilled zones? Use of historical geographic information and local spatial knowledge to determine the location of underground asbestos contamination in Sibaté (Colombia). Environ. Res. 2020, 191, 1–14. [Google Scholar] [CrossRef]
- Ministerio de Ambiente, Vivienda y Desarrollo Territorial. Decreto Número 4741 por el Cual se Reglamenta Parcialmente la Prevención y Manejo de los Residuos o Desechos Peligrosos Generados en el Marco de la Gestión Integral. 2005. Available online: http://www.ideam.gov.co/documents/51310/526371/Decreto+4741+2005+PREVENCION+Y+MANEJO+DE+REIDUOS+PELIGROSOS+GENERADOS+EN+GESTION+INTEGRAL.pdf/491df435-061e-4d27-b40f-c8b3afe25705 (accessed on 15 June 2021).
- Ministerio de Ambiente, Vivienda y Desarrollo Territorial. Resolución Número 1362 por la Cual se Establece los Requisitos y el Procedimiento para el Registro de Generadores de Residuos o Desechos Peligrosos, a que Hacen Referencia los Artículos 27° y 28° del Decreto 4741 del 30 de Diciembre de 2005. Available online: http://www.ideam.gov.co/documents/51310/526371/Resolucion+1362+2007++REQUISITOS+Y+PROCEDIMIENTOS+PARA+REG+DE+GENERADORES+DE+RESPEL.pdf/cdd6d851-013b-4bea-adf6-addec449f32b (accessed on 15 June 2021).
- Ministerio de Salud y Protección Social. Resolución Número 007 por la Cual se Adopta el Reglamento de Higiene y Seguridad del Crisotilo y Otras Fibras de Uso Similar. 2011. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/resolucion-007-2011.pdf (accessed on 15 June 2021).

{kind=link}
| Name | Municipality (and Department) | Type of Facility | Production | Starting Date |
|---|---|---|---|---|
| Eternit Colombiana SA | Sibaté (Cundinamarca) | Plant | Asbestos cement | 1942 |
| Eternit Atlántico SA | Barranquilla (Atlántico) | Plant | Asbestos cement | 1944 |
| Eternit Pacífico SA | Yumbo (Valle del Cauca) | Plant | Asbestos cement | 1944 |
| Incolbest SA | Bogotá (Bogotá DC) | Plant | Friction products | 1960 |
| Etex Colombia SA | Manizales (Caldas) | Plant | Asbestos cement | 1967 |
| Toptec SA | Manizales (Caldas) | Plant | Asbestos cement | 1982 |
| Minera Las Brisas | Campamento (Antioquia) | Mine | Chrysotile | 1980 |
| Article Reference | Asbestos-Related Diseases Studied | Sources of Environmental Exposure | Asbestos Type | Risk-Related Indicator | Relationship between Risk and Distance to the Plant | Observations | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <500 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | ||||||
| Vimercati et al., 2020 | Epithelioid mesothelioma | Asbestos cement plant | Amosite and crocidolite: 20%; chrysotile: 80% | (1) Adjusted risks of EM (OR) by distance and exposure length (2) Adjusted risks of EM (OR) by distance and latency length | (<550 m) (1) OR = 1.47 (0.262–8.248) // (2) OR = 1.771 (0.32–9.805). Compared to people living at >1000 m | (550–1000 m) (1) OR = 1.87 (0.353–9.905) // (2) OR = 2.038 (0.371–11.19). Compared to people living at >1000 m | Apulia Mesothelioma Registry. There is an exposure reconstruction. They looked at the records of 2236 cases between 1989 and 2019. The 71 cases analyzed were only environmentally exposed. The distance of 550–1000 m is a finding of the study, based on the living locations of the 71 cases. 3000 m was the largest distance that cases lived from the factory, but there was no risk estimate for 3000 m. | ||||
| Tarrés et al., 2012 | Malignant pleural mesothelioma | Asbestos cement plant | Amosite: 5%; crocidolite: 15%; chrysotile: 80% | Incidence rate ratio | (<500 m) IRR = 12.92 (10.77–15.33) | (>500–2000 m) IRR = 0.70 (0.28–1.44) | (>2000–10,000 m) IRR = 0.23 (0.02–0.72) | Clinical and epidemiological data were recorded for the 24 pleural mesothelioma cases. Places of residence were obtained from primary healthcare documentation. Concentric circles were used for the analysis. | |||
| Kurumatani, Kumagai, 2008 | Pleural and peritoneal mesotheliomas + pleural cancers (on death certificate) | Asbestos cement plant | Crocidolite and chrysotile | SMR | SMR Men (<300 m) = 13.9 (5.6–28.7) // SMR Women (<300 m) = 41.4 (15.2–90.1) | SMR Men (300 to 600 m) = 5.6 (2.9–9.8) // SMR Women (300 m to 600 m) = 11.3 (4.5–23.3) | SMR Men (600 to 900 m) = 2.1 (0.8–4.3) // SMR Women (600 m to 900 m) = 7.2 (2.9–14.8) | 90 cases. Distances were analyzed with 300 m increments. | |||
| Musti et al., 2009 | Malignant mesothelioma | Asbestos cement plant | Amosite: 5%; crocidolite: 15%; chrysotile: 80% | OR adjusted by sex and age | (0–500 m) OR = 5.29 (1.18–23.74). Compared to a distance of >2000 m | (500–1000 m) OR = 1.49 (0.58–3.82) // (1000–1500 m) OR = 1.27 (0.49–3.71). Compared to a distance of >2000 m | (1500–2000 m) OR = 2.31 (0.88–6.06). Compared to a distance of >2000 m | Case–control study. Regional Mesothelioma Register–Bari. 48 cases of malignant mesothelioma, non-occupationally exposed, and 273 controls. | |||
| Maule et al., 2007 | Malignant pleural mesothelioma | Asbestos cement plant | Crocidolite: 10%; “airborne emissions from the AC plant included both chrysotile and crocidolite fibers” | OR adjusted by sex, age, domestic exposure, and relatives that work in the AC plant | (0–3000 m ) OR = 6.8 (2.4–19.5) // (3000–5000 m) OR = 12.5 (3.7–42.2) | (5000–7000 m ) OR = 3.9 (1.2–12.6) // (7000–9000 m) OR = 4.2 (1.1–16.5) | Case–control study. 103 cases, 272 controls. Casale Monferrato. Piedmont Mesothelioma Registry. | ||||
| Airoldi et al., 2021 | Malignant pleural mesothelioma | Asbestos cement plant | Crocidolite: 10% | OR adjusted by age, sex, type of interview, and domestic exposure | (0–5000 m) OR = 12.66 (4.19–38.28). Compared to a distance of >15,000 m | (5000–10,000 m) OR = 7.15 (1.87–27.36). Compared to a distance of >15,000 m | Case–control study. 200 cases, 348 controls. Casale Monferrato. | ||||
| Magnani et al., 2000 | Malignant pleural mesothelioma | Asbestos cement plants; asbestos textiles, shipyards, or brakes factories | Unspecified | OR adjusted by center, sex, and age | “A high risk was observed for high probability of environmental exposure (11.5 (3.47–38.2))—that is, subjects who had lived for some time within 2000 m of a mine or asbestos facility” | Histologically confirmed cases. Exposure classification of cases. High risk of exposure (not disease). | |||||
| Age Groups (Years) | Incolbest—Bogotá | Eternit—Sibaté | Eternit—Yumbo | Eternit—Barranquilla | Las Brisas—Campamento | Toptec—Manizales | Colombit (Etex)—Manizales | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | |
| 0–4 | 354 | 1872 | 10,012 | 58,109 | 283,057 | 4 | 15 | 201 | 17,846 | 49,988 | 47 | 547 | 2203 | 5719 | 28,547 | 65 | 864 | 3339 | 33,099 | 134,411 | 0 | 0 | 0 | 35 | 303 | 308 | 911 | 1210 | 5733 | 24,391 | 20 | 53 | 93 | 1541 | 19,273 |
| 5–9 | 377 | 1963 | 11,008 | 61,771 | 312,962 | 4 | 16 | 251 | 20,294 | 57,551 | 55 | 667 | 2574 | 6580 | 32,572 | 68 | 873 | 3412 | 34,829 | 133,712 | 0 | 0 | 0 | 41 | 364 | 361 | 1108 | 1493 | 7058 | 28,602 | 28 | 73 | 116 | 1891 | 22,871 |
| 10–14 | 347 | 1779 | 10,207 | 56,974 | 300,387 | 4 | 17 | 229 | 19,992 | 56,800 | 66 | 667 | 2694 | 6832 | 33,313 | 79 | 992 | 3890 | 35,847 | 130,874 | 0 | 0 | 0 | 37 | 341 | 377 | 1134 | 1531 | 7944 | 32,080 | 28 | 71 | 119 | 1932 | 25,547 |
| 15–19 | 274 | 1580 | 9329 | 50,759 | 281,226 | 4 | 16 | 185 | 17,523 | 47,645 | 50 | 549 | 2303 | 6221 | 31,235 | 89 | 1071 | 4610 | 38,786 | 132,424 | 0 | 0 | 0 | 29 | 281 | 411 | 1278 | 1717 | 9194 | 33,149 | 25 | 69 | 112 | 2092 | 26,292 |
| 20–24 | 311 | 1929 | 10,605 | 55,085 | 316,058 | 6 | 20 | 196 | 18,379 | 46,706 | 50 | 567 | 2094 | 5840 | 31,754 | 89 | 1063 | 5294 | 43,047 | 137,290 | 0 | 0 | 0 | 18 | 187 | 468 | 1422 | 1918 | 10,407 | 33,886 | 19 | 53 | 91 | 2238 | 26,877 |
| 25–29 | 345 | 2066 | 10,354 | 55,095 | 307,855 | 3 | 10 | 149 | 14,911 | 40,169 | 41 | 493 | 1753 | 5267 | 29,665 | 171 | 1145 | 4376 | 36,814 | 119,697 | 0 | 0 | 0 | 15 | 146 | 470 | 1400 | 1799 | 7830 | 28,011 | 22 | 56 | 91 | 2117 | 21,967 |
| 30–34 | 395 | 1948 | 9573 | 51,653 | 274,411 | 2 | 8 | 153 | 12,857 | 36,185 | 37 | 453 | 1688 | 4891 | 26,811 | 67 | 812 | 3468 | 30,844 | 100,196 | 0 | 0 | 0 | 16 | 145 | 382 | 1149 | 1487 | 6659 | 24,052 | 23 | 57 | 86 | 1797 | 19,249 |
| 35–39 | 352 | 1725 | 9076 | 49,904 | 268,013 | 3 | 10 | 149 | 13,557 | 38,813 | 43 | 407 | 1720 | 4907 | 26,769 | 79 | 903 | 3760 | 31,586 | 100,699 | 0 | 0 | 0 | 13 | 154 | 377 | 1092 | 1459 | 7416 | 26,567 | 27 | 70 | 104 | 1834 | 21,088 |
| 40–44 | 279 | 1422 | 7855 | 45,254 | 253,778 | 2 | 9 | 130 | 12,994 | 36,783 | 46 | 410 | 1629 | 4653 | 25,562 | 82 | 956 | 3902 | 32,707 | 97,947 | 0 | 0 | 0 | 15 | 160 | 332 | 1032 | 1383 | 7478 | 26,752 | 22 | 62 | 98 | 1722 | 20,978 |
| 45–49 | 173 | 1013 | 6136 | 35,323 | 207,639 | 2 | 7 | 87 | 11,957 | 30,749 | 34 | 329 | 1247 | 3611 | 20,955 | 70 | 755 | 3458 | 28,280 | 80,426 | 0 | 0 | 0 | 12 | 140 | 349 | 1055 | 1413 | 6815 | 24,682 | 14 | 38 | 68 | 1668 | 18,980 |
| 50–54 | 131 | 831 | 4414 | 25,834 | 160,060 | 2 | 6 | 69 | 9077 | 22,995 | 21 | 251 | 928 | 2832 | 16,817 | 56 | 644 | 2823 | 23,416 | 63,545 | 0 | 0 | 0 | 12 | 115 | 345 | 1068 | 1392 | 5965 | 20,724 | 11 | 28 | 54 | 1601 | 15,981 |
| 55–59 | 83 | 673 | 3373 | 18,758 | 122,064 | 1 | 5 | 60 | 5768 | 15,313 | 15 | 190 | 669 | 2171 | 12,823 | 37 | 452 | 2124 | 18,723 | 48,676 | 0 | 0 | 0 | 8 | 87 | 280 | 851 | 1114 | 4716 | 15,988 | 8 | 23 | 42 | 1297 | 12,328 |
| 60–64 | 66 | 505 | 2428 | 13,081 | 89,080 | 1 | 3 | 48 | 3490 | 10,056 | 18 | 162 | 501 | 1581 | 9112 | 28 | 365 | 1555 | 13,875 | 34,896 | 0 | 0 | 0 | 9 | 83 | 173 | 554 | 718 | 3482 | 11,904 | 10 | 25 | 38 | 878 | 9256 |
| 65–69 | 45 | 305 | 1783 | 8923 | 63,725 | 1 | 4 | 51 | 2571 | 7701 | 9 | 118 | 460 | 1415 | 7429 | 22 | 292 | 1285 | 11,980 | 29,625 | 0 | 0 | 0 | 6 | 72 | 130 | 404 | 539 | 2773 | 9759 | 7 | 18 | 29 | 664 | 7664 |
| 70–74 | 35 | 202 | 1115 | 6061 | 46,247 | 0 | 2 | 34 | 1617 | 5389 | 7 | 84 | 321 | 1017 | 5363 | 22 | 243 | 1067 | 9286 | 22,328 | 0 | 0 | 0 | 3 | 64 | 89 | 281 | 371 | 2162 | 7652 | 5 | 13 | 21 | 452 | 5904 |
| 75–79 | 25 | 134 | 793 | 4305 | 32,006 | 0 | 2 | 16 | 1022 | 3171 | 5 | 47 | 191 | 714 | 3662 | 18 | 218 | 915 | 7769 | 17,031 | 0 | 0 | 0 | 3 | 37 | 59 | 203 | 268 | 1594 | 5643 | 2 | 4 | 9 | 313 | 4339 |
| 80+ | 15 | 118 | 704 | 3912 | 28,352 | 0 | 1 | 16 | 907 | 2640 | 5 | 43 | 184 | 689 | 3480 | 17 | 225 | 989 | 8546 | 17,953 | 0 | 0 | 0 | 3 | 45 | 52 | 169 | 232 | 1455 | 5067 | 2 | 5 | 9 | 276 | 3887 |
| TOTAL | 3606 | 20,065 | 108,768 | 600,803 | 3,346,920 | 40 | 150 | 2025 | 184,763 | 508,656 | 547 | 5985 | 23,161 | 64,938 | 345,868 | 1059 | 11,875 | 50,267 | 439,434 | 1,401,729 | 0 | 0 | 2 | 274 | 2724 | 4963 | 15,110 | 20,044 | 98,680 | 358,909 | 273 | 718 | 1178 | 24,312 | 282,479 |
| Age Groups (Years) | Incolbest—Bogotá | Eternit—Sibaté | Eternit—Yumbo | Eternit—Barranquilla | Las Brisas—Campamento | Toptec—Manizales | Colombit (Etex)—Manizales | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | |
| 0–4 | 364 | 1696 | 7518 | 43,828 | 217,519 | 1 | 3 | 163 | 20,621 | 68,139 | 30 | 359 | 1718 | 4717 | 16,713 | 62 | 556 | 2097 | 22,997 | 102,243 | 4 | 19 | 43 | 142 | 557 | 255 | 735 | 918 | 4949 | 19,201 | 10 | 26 | 32 | 1082 | 15,300 |
| 5–9 | 384 | 1781 | 8071 | 47,133 | 236,397 | 1 | 4 | 165 | 22,373 | 74,775 | 32 | 384 | 1839 | 5107 | 18,411 | 66 | 611 | 2181 | 23,962 | 106,250 | 7 | 30 | 69 | 215 | 800 | 278 | 818 | 1012 | 5377 | 21,197 | 14 | 38 | 48 | 1182 | 16,900 |
| 10–14 | 422 | 1832 | 8657 | 50,446 | 251,234 | 1 | 3 | 179 | 23,495 | 77,893 | 38 | 455 | 2163 | 5917 | 20,901 | 60 | 602 | 2210 | 25,173 | 108,512 | 8 | 35 | 84 | 269 | 949 | 318 | 948 | 1203 | 6092 | 24,504 | 20 | 48 | 59 | 1393 | 19,581 |
| 15–19 | 500 | 2124 | 9908 | 57,992 | 290,521 | 1 | 3 | 185 | 25,678 | 84,035 | 49 | 540 | 2390 | 6610 | 23,432 | 74 | 736 | 2806 | 29,569 | 121,016 | 7 | 32 | 75 | 251 | 940 | 380 | 1122 | 1425 | 7732 | 29,767 | 19 | 51 | 66 | 1670 | 23,560 |
| 20–24 | 612 | 2751 | 12,639 | 72,384 | 363,729 | 1 | 3 | 204 | 27,338 | 91,143 | 49 | 558 | 2533 | 7058 | 26,743 | 88 | 812 | 3166 | 32,150 | 124,179 | 7 | 31 | 64 | 176 | 699 | 442 | 1335 | 1716 | 9470 | 34,697 | 19 | 53 | 66 | 2004 | 27,635 |
| 25–29 | 602 | 2775 | 12,394 | 71,283 | 354,252 | 1 | 4 | 178 | 24,513 | 87,213 | 48 | 511 | 2396 | 6774 | 26,444 | 79 | 755 | 2950 | 30,751 | 119,170 | 7 | 30 | 60 | 153 | 601 | 382 | 1147 | 1464 | 8402 | 32,040 | 18 | 44 | 57 | 1710 | 25,327 |
| 30–34 | 537 | 2366 | 10,508 | 64,642 | 315,266 | 1 | 4 | 198 | 23,219 | 81,174 | 41 | 454 | 2073 | 5985 | 24,740 | 66 | 638 | 2561 | 28,352 | 108,759 | 3 | 15 | 34 | 126 | 554 | 378 | 1167 | 1469 | 7695 | 28,903 | 15 | 42 | 52 | 1694 | 22,690 |
| 35–39 | 498 | 2225 | 9583 | 61,954 | 299,604 | 1 | 4 | 181 | 22,280 | 74,720 | 34 | 444 | 2018 | 5920 | 24,664 | 60 | 666 | 2608 | 28,398 | 105,724 | 4 | 16 | 37 | 126 | 572 | 479 | 1355 | 1695 | 8207 | 29,191 | 20 | 47 | 57 | 1950 | 22,910 |
| 40–44 | 434 | 1846 | 8051 | 52,008 | 252,717 | 0 | 2 | 143 | 17,840 | 59,484 | 29 | 385 | 1719 | 5111 | 21,614 | 67 | 626 | 2313 | 24,079 | 87,861 | 4 | 18 | 40 | 123 | 453 | 388 | 1119 | 1419 | 7135 | 24,764 | 20 | 49 | 61 | 1667 | 19,698 |
| 45–49 | 418 | 1814 | 7912 | 48,521 | 239,694 | 1 | 2 | 125 | 16,610 | 55,145 | 29 | 357 | 1706 | 5097 | 21,363 | 60 | 605 | 2190 | 23,427 | 82,756 | 3 | 15 | 34 | 108 | 474 | 413 | 1135 | 1422 | 7447 | 26,039 | 20 | 48 | 58 | 1666 | 20,657 |
| 50–54 | 387 | 1643 | 7618 | 45,803 | 235,627 | 1 | 2 | 123 | 15,816 | 51,432 | 35 | 355 | 1686 | 5014 | 21,691 | 60 | 618 | 2480 | 25,432 | 83,722 | 3 | 14 | 32 | 96 | 430 | 387 | 1103 | 1401 | 7926 | 27,675 | 16 | 44 | 53 | 1650 | 21,779 |
| 55–59 | 271 | 1233 | 6129 | 37,785 | 202,030 | 1 | 3 | 100 | 13,587 | 43,038 | 34 | 322 | 1346 | 4131 | 19,152 | 58 | 583 | 2363 | 24,362 | 75,116 | 3 | 12 | 26 | 85 | 410 | 360 | 1065 | 1334 | 7529 | 26,288 | 10 | 29 | 37 | 1532 | 20,345 |
| 60–64 | 193 | 917 | 4589 | 27,429 | 151,308 | 0 | 2 | 67 | 10,926 | 32,412 | 24 | 248 | 1037 | 3311 | 15,599 | 47 | 480 | 1997 | 20,502 | 59,893 | 2 | 8 | 19 | 68 | 309 | 353 | 1027 | 1312 | 6612 | 22,510 | 8 | 21 | 27 | 1469 | 17,386 |
| 65–69 | 113 | 659 | 3187 | 18,836 | 109,189 | 0 | 1 | 47 | 7217 | 21,564 | 13 | 173 | 748 | 2416 | 11,707 | 28 | 332 | 1460 | 16,169 | 44,985 | 2 | 9 | 19 | 52 | 238 | 292 | 871 | 1095 | 5224 | 17,414 | 6 | 14 | 18 | 1218 | 13,484 |
| 70–74 | 78 | 515 | 2283 | 12,310 | 75,028 | 0 | 2 | 44 | 4263 | 13,396 | 11 | 130 | 531 | 1745 | 8710 | 24 | 268 | 1094 | 11,618 | 31,007 | 1 | 4 | 10 | 37 | 185 | 205 | 619 | 791 | 3812 | 12,660 | 7 | 17 | 19 | 897 | 9899 |
| 75–79 | 57 | 351 | 1532 | 8187 | 52,393 | 0 | 1 | 37 | 2605 | 8508 | 12 | 106 | 417 | 1257 | 6114 | 17 | 214 | 843 | 8850 | 22,602 | 1 | 4 | 7 | 22 | 143 | 133 | 407 | 514 | 2637 | 8796 | 5 | 13 | 17 | 594 | 6920 |
| 80–84 | 30 | 189 | 895 | 5070 | 34,419 | 0 | 0 | 19 | 1455 | 4963 | 4 | 60 | 237 | 830 | 4116 | 16 | 162 | 609 | 6366 | 15,388 | 0 | 1 | 4 | 16 | 95 | 80 | 228 | 288 | 1784 | 5935 | 4 | 10 | 12 | 341 | 4611 |
| 85–89 | 21 | 88 | 453 | 2575 | 18,572 | 0 | 0 | 9 | 755 | 2521 | 3 | 32 | 121 | 452 | 2152 | 10 | 96 | 376 | 3752 | 8729 | 0 | 1 | 1 | 6 | 44 | 38 | 116 | 155 | 1000 | 3312 | 2 | 5 | 6 | 179 | 2566 |
| 90–94 | 4 | 27 | 163 | 1035 | 7173 | 0 | 0 | 3 | 273 | 888 | 1 | 9 | 59 | 223 | 880 | 4 | 30 | 148 | 1733 | 3980 | 0 | 0 | 0 | 1 | 15 | 16 | 52 | 68 | 450 | 1378 | 0 | 1 | 1 | 74 | 1071 |
| 95–99 | 2 | 14 | 55 | 279 | 1893 | 0 | 0 | 1 | 68 | 243 | 0 | 4 | 16 | 54 | 226 | 1 | 14 | 56 | 559 | 1288 | 0 | 0 | 0 | 0 | 2 | 2 | 7 | 8 | 89 | 301 | 0 | 0 | 0 | 11 | 233 |
| 100+ | 1 | 4 | 15 | 118 | 762 | 0 | 0 | 0 | 47 | 150 | 0 | 0 | 4 | 17 | 66 | 0 | 5 | 20 | 243 | 536 | 0 | 0 | 0 | 0 | 1 | 1 | 3 | 3 | 29 | 88 | 0 | 0 | 0 | 4 | 65 |
| TOTAL | 5927 | 26,851 | 122,161 | 729,618 | 3,709,324 | 12 | 45 | 2172 | 280,981 | 932,838 | 516 | 5886 | 26,758 | 77,746 | 315,439 | 948 | 9409 | 36,527 | 388,444 | 1,413,714 | 66 | 292 | 658 | 2071 | 8472 | 5582 | 16,378 | 20,715 | 109,599 | 396,661 | 234 | 599 | 746 | 23,986 | 312,615 |
| Age Groups (Years) | ETEX and TOPTEC | INCOLBEST and ETERNIT SIBATE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | |
| 0–4 | N/A | N/A | 7 | 1456 | 19,240 | N/A | N/A | N/A | N/A | 3799 |
| 5–9 | N/A | N/A | 6 | 1800 | 22,840 | N/A | N/A | N/A | N/A | 4324 |
| 10–14 | N/A | N/A | 9 | 1839 | 25,513 | N/A | N/A | N/A | N/A | 4026 |
| 15–19 | N/A | N/A | 7 | 2006 | 26,263 | N/A | N/A | N/A | N/A | 3557 |
| 20–24 | N/A | N/A | 8 | 2170 | 26,854 | N/A | N/A | N/A | N/A | 3697 |
| 25–29 | N/A | N/A | 7 | 2050 | 21,941 | N/A | N/A | N/A | N/A | 3436 |
| 30–34 | N/A | N/A | 5 | 1740 | 19,230 | N/A | N/A | N/A | N/A | 3146 |
| 35–39 | N/A | N/A | 5 | 1768 | 21,062 | N/A | N/A | N/A | N/A | 3000 |
| 40–44 | N/A | N/A | 7 | 1661 | 20,957 | N/A | N/A | N/A | N/A | 2576 |
| 45–49 | N/A | N/A | 7 | 1614 | 18,961 | N/A | N/A | N/A | N/A | 1896 |
| 50–54 | N/A | N/A | 6 | 1552 | 15,965 | N/A | N/A | N/A | N/A | 1578 |
| 55–59 | N/A | N/A | 3 | 1261 | 12,318 | N/A | N/A | N/A | N/A | 1266 |
| 60–64 | N/A | N/A | 2 | 849 | 9249 | N/A | N/A | N/A | N/A | 916 |
| 65–69 | N/A | N/A | 2 | 640 | 7659 | N/A | N/A | N/A | N/A | 629 |
| 70–74 | N/A | N/A | 1 | 437 | 5901 | N/A | N/A | N/A | N/A | 408 |
| 75–79 | N/A | N/A | 1 | 303 | 4337 | N/A | N/A | N/A | N/A | 253 |
| 80+ | N/A | N/A | 1 | 268 | 3885 | N/A | N/A | N/A | N/A | 223 |
| TOTAL | N/A | N/A | 82 | 23,416 | 282,175 | N/A | N/A | N/A | N/A | 38,728 |
| Age Groups (Years) | ETEX and TOPTEC | INCOLBEST and ETERNIT SIBATE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m | |
| 0–4 | N/A | N/A | 2 | 1077 | 15,297 | N/A | N/A | N/A | N/A | 3661 |
| 5–9 | N/A | N/A | 3 | 1176 | 16,895 | N/A | N/A | N/A | N/A | 4070 |
| 10–14 | N/A | N/A | 5 | 1390 | 19,575 | N/A | N/A | N/A | N/A | 4170 |
| 15–19 | N/A | N/A | 6 | 1664 | 23,555 | N/A | N/A | N/A | N/A | 4624 |
| 20–24 | N/A | N/A | 4 | 1999 | 27,627 | N/A | N/A | N/A | N/A | 5256 |
| 25–29 | N/A | N/A | 4 | 1700 | 25,323 | N/A | N/A | N/A | N/A | 5144 |
| 30–34 | N/A | N/A | 3 | 1690 | 22,687 | N/A | N/A | N/A | N/A | 4411 |
| 35–39 | N/A | N/A | 4 | 1944 | 22,908 | N/A | N/A | N/A | N/A | 3926 |
| 40–44 | N/A | N/A | 5 | 1663 | 19,694 | N/A | N/A | N/A | N/A | 3337 |
| 45–49 | N/A | N/A | 3 | 1662 | 20,651 | N/A | N/A | N/A | N/A | 3142 |
| 50–54 | N/A | N/A | 2 | 1647 | 21,775 | N/A | N/A | N/A | N/A | 2840 |
| 55–59 | N/A | N/A | 3 | 1529 | 20,339 | N/A | N/A | N/A | N/A | 2260 |
| 60–64 | N/A | N/A | 2 | 1465 | 17,384 | N/A | N/A | N/A | N/A | 1650 |
| 65–69 | N/A | N/A | 2 | 1217 | 13,483 | N/A | N/A | N/A | N/A | 1258 |
| 70–74 | N/A | N/A | 1 | 896 | 9898 | N/A | N/A | N/A | N/A | 922 |
| 75–79 | N/A | N/A | 1 | 592 | 6920 | N/A | N/A | N/A | N/A | 578 |
| 80–84 | N/A | N/A | 1 | 339 | 4608 | N/A | N/A | N/A | N/A | 323 |
| 85–89 | N/A | N/A | 0 | 179 | 2565 | N/A | N/A | N/A | N/A | 180 |
| 90–94 | N/A | N/A | 0 | 74 | 1071 | N/A | N/A | N/A | N/A | 59 |
| 95–99 | N/A | N/A | 0 | 11 | 233 | N/A | N/A | N/A | N/A | 17 |
| 100+ | N/A | N/A | 0 | 4 | 65 | N/A | N/A | N/A | N/A | 2 |
| TOTAL | N/A | N/A | 51 | 23,916 | 312,554 | N/A | N/A | N/A | N/A | 51,831 |
| Year | 500 m | 1000 m | 2000 m | 5000 m | 10,000 m |
|---|---|---|---|---|---|
| 2005 | 10,489 | 53,904 | 205,363 | 1,389,788 | 5,926,382 |
| 2018 | 13,285 | 59,459 | 209,685 | 1,588,528 | 6,724,677 |
| Municipality | C450—Pleural Mesothelioma | C451—Mesothelioma of Peritoneum | C452—Mesothelioma of Pericardium | |||
|---|---|---|---|---|---|---|
| Females | Males | Females | Males | Females | Males | |
| Barranquilla | 38 | 25 | 52 | 15 | 45 | 19 |
| Bogotá | 97 | 163 | 56 | 11 | 4 | 5 |
| Campamento | - | - | - | - | - | - |
| Manizales | 3 | 6 | 6 | 1 | - | 1 |
| Sibaté | 5 | 16 | - | - | - | - |
| Yumbo | - | 3 | - | 1 | - | - |
| Total | 143 | 213 | 114 | 28 | 49 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lysaniuk, B.; Cely-García, M.F.; Giraldo, M.; Larrahondo, J.M.; Serrano-Calderón, L.M.; Guerrero-Bernal, J.C.; Briceno-Ayala, L.; Cruz Rodriguez, E.; Ramos-Bonilla, J.P. Using GIS to Estimate Population at Risk Because of Residence Proximity to Asbestos Processing Facilities in Colombia. Int. J. Environ. Res. Public Health 2021, 18, 13297. https://doi.org/10.3390/ijerph182413297
Lysaniuk B, Cely-García MF, Giraldo M, Larrahondo JM, Serrano-Calderón LM, Guerrero-Bernal JC, Briceno-Ayala L, Cruz Rodriguez E, Ramos-Bonilla JP. Using GIS to Estimate Population at Risk Because of Residence Proximity to Asbestos Processing Facilities in Colombia. International Journal of Environmental Research and Public Health. 2021; 18(24):13297. https://doi.org/10.3390/ijerph182413297
Chicago/Turabian StyleLysaniuk, Benjamin, María Fernanda Cely-García, Margarita Giraldo, Joan M. Larrahondo, Laura Marcela Serrano-Calderón, Juan Carlos Guerrero-Bernal, Leonardo Briceno-Ayala, Esteban Cruz Rodriguez, and Juan Pablo Ramos-Bonilla. 2021. "Using GIS to Estimate Population at Risk Because of Residence Proximity to Asbestos Processing Facilities in Colombia" International Journal of Environmental Research and Public Health 18, no. 24: 13297. https://doi.org/10.3390/ijerph182413297
APA StyleLysaniuk, B., Cely-García, M. F., Giraldo, M., Larrahondo, J. M., Serrano-Calderón, L. M., Guerrero-Bernal, J. C., Briceno-Ayala, L., Cruz Rodriguez, E., & Ramos-Bonilla, J. P. (2021). Using GIS to Estimate Population at Risk Because of Residence Proximity to Asbestos Processing Facilities in Colombia. International Journal of Environmental Research and Public Health, 18(24), 13297. https://doi.org/10.3390/ijerph182413297