Oral Health Problems and Utilization of Dental Services among Spanish and Immigrant Children and Adolescents



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Socio-Economic and Demographic Variables
3.2. Utilization of Dental Services and Oral Health Problems
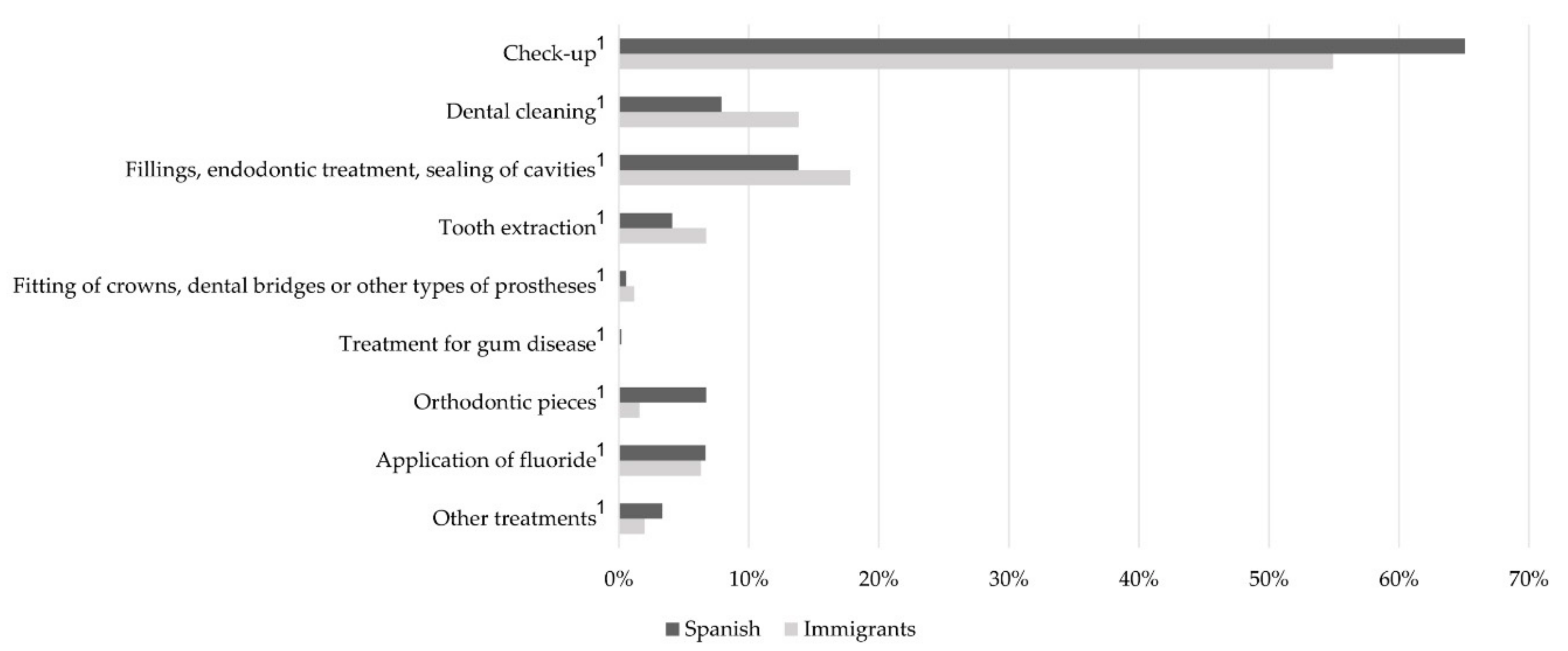
3.3. Type of Dental Treatment Received
3.4. Association between Socioeconomic and Demographic Variables and Utilization of Dental Services
3.5. Association between Socioeconomic and Demographic Variables and the Presence of Dental Health Problems
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Muñoz Pino, N.; Vives Cases, C.; Agudelo Suárez, A.A.; Ronda Pérez, E. Comparing oral health services use in the Spanish and immigrant working population. J. Immigr. Health 2018, 22, 809–815. [Google Scholar] [CrossRef]
- Bravo, M.; San Martín, L.; Casals, E.; Eaton, K.; Widström, E. The healthcare system and the provision of oral healthcare in European Union member states. Part 2: Spain. Br. Dent. J. 2015, 219, 547–551. [Google Scholar] [CrossRef]
- Tchicaya, A.; Lorentz, N. Socioeconomic inequalities in the non-use of dental care in Europe. Int. J. Equity Health 2014, 13, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Reda, S.M.; Krois, J.; Reda, S.F.; Thomson, W.M.; Schwendicke, F. The impact of demographic, health-related and social factors on dental services utilization: Systematic review and meta-analysis. J. Dent. 2018, 75, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Eurostat: Population without the Citizenship of the Reporting Country. Available online: https://ec.europa.eu/eurostat/tgm/graph.do?tab=graph&plugin=1&language=en&pcode=tps00157&toolbox=type (accessed on 6 December 2019).
- Reda, S.F.; Reda, S.M.; Thomson, W.M.; Schwendicke, F. Inequality in utilization of dental services: A systematic review and meta-analysis. Am. J. Public Health 2018, 108, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Valcárcel Soria, R.; Somacarrera Pérez, M.L. Estado de salud oral de los niños inmigrantes en España. Odontol. Pediatr. 2016, 24, 194–206. [Google Scholar]
- Ghasemianpour, M.; Bakhshandeh, S.; Shirvani, A.; Emadi, N.; Samadzadeh, H.; Fatemi, N.M.; Ghasemian, A. Dental caries experience and socio-economic status among Iranian children: A multilevel analysis. BMC Public Health 2019, 19, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Foster Page, L.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Babo Soares, L.F.; Allen, P.; Bettiol, S.; Crocombe, L. The association of socioeconomic status and dental caries experience in children in Dili, Timor-Leste. Asia Pac. J. Public Health 2016, 28, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.-C.A.; Hakeberg, M.; Petzold, M.; Östberg, A.-L. Demographic factors and dental health of Swedish children and adolescents. Acta Odontol. Scand. 2016, 74, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Font Ribera, L.; García Continente, X.; Davó Blanes, M.C.; Ariza, C.; Díez, E.; García Calvente, M.M.; Maroto, G.; Suárez, M.; Rajmil, L.; Grupo de Determinantes Sociales de la Sociedad Española de Epidemiología. El estudio de las desigualdades sociales en la salud infantil y adolescente en España. Gac. Sanit. 2014, 28, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Encuesta Nacional de Salud de España 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm (accessed on 13 September 2019).
- Plan de Salud Bucodental del Ministerio de Sanidad y Política Social. Gobierno de España. Available online: http://www.mscbs.gob.es/campannas/campanas08/bucoDental/medidas_salud_bucodental.html (accessed on 1 October 2019).
- Domingo Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C. Propuestas de clase social neoweberiana y neomarxista a partir de la Clasificación Nacional de Ocupaciones 2011. Gac. Sanit. 2014, 28, 316–325. [Google Scholar] [CrossRef]
- El-Yousfi, S.; Jones, K.; White, S.; Marshman, Z. A rapid review of barriers to oral healthcare for vulnerable people. Br. Dent. J. 2019, 227, 143–151. [Google Scholar] [CrossRef]
- Markkula, N.; Cabieses, B.; Lehti, V.; Uphoff, E.; Astorga, S.; Stutzin, F. Use of health services among international migrant children—A systematic review. Glob. Health 2018, 14, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Ley Orgánica 4/2000, de 11 de Enero, Sobre Derechos y Libertades de los Extranjeros en España y su Integración Social. Available online: https://www.boe.es/buscar/pdf/2000/BOE-A-2000-544-consolidado.pdf (accessed on 12 November 2019).
- Xu, M.; Yuan, C.; Sun, X.; Cheng, M.; Xie, Y.; Si, Y. Oral health service utilization patterns among preschool children in Beijing, China. BMC Oral Health 2018, 18, 31–39. [Google Scholar] [CrossRef]
- Tapias Ledesma, M.A.; Hernández Barrera, V.; Carrasco Garrido, P.; Gil de Miguel, A.; Esteban y Peña, M.; Jiménez Garcia, R. Use of dental care and prevalence of caries among immigrant and Spanish-born children. ASDC J. Dent. Child. 2011, 78, 36–42. [Google Scholar]
- Finlayson, T.L.; Asgari, P.; Dougherty, E.; Tadese, B.K.; Stamm, N.; Nunez Alvarez, A. Child, caregiver, and family factors associated with child dental utilization among Mexican migrant families in California. Community Dent. Health 2018, 35, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Bhagavatula, P.; Xiang, Q.; Szabo, A.; Eichmiller, F.; Kuthy, R.A.; Okunseri, C.E. Rural-urban differences in dental service use among children enrolled in a private dental insurance plan in Wisconsin: Analysis of administrative data. BMC Oral Health 2012, 12, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Irvin, K.; Fahim, F.; Alshehri, S.; Kitsantas, P. Family structure and children’s unmet health-care needs. J. Child. Health Care 2018, 22, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.-H.; Kim, M.-H.; Ryu, J.-I. Inequalities in oral health among adolescents in Gangneung, South Korea. BMC Oral Health 2018, 18, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Mamai Homata, E.; Koletsi Kounari, H.; Margaritis, V. Gender differences in oral health status and behavior of Greek dental students: A meta-analysis of 1981, 2000, and 2010 data. J. Int. Soc. Prev. Community Dent. 2016, 6, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Tadakamadla, J.; Kroon, J.; Johnson, N.W. Impact of parent-related factors on dental caries in the permanent dentition of 6–12-year-old children: A systematic review. J. Dent. 2016, 46, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bright, M.A.; Alford, S.M.; Hinojosa, M.S.; Knapp, C.; Fernandez Baca, D.E. Adverse childhood experiences and dental health in children and adolescents. Community Dent. Oral Epidemiol. 2015, 43, 193–199. [Google Scholar] [CrossRef]
- Kumar, S.; Tadakamadla, J.; Zimmer Gembeck, M.J.; Kroon, J.; Lalloo, R.; Johnson, N.W. Parenting practices and children’s dental caries experience: A structural equation modelling approach. Community Dent. Oral Epidemiol. 2017, 45, 552–558. [Google Scholar] [CrossRef]
- Rouxel, P.; Chandola, T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent. Oral Epidemiol. 2018, 46, 426–434. [Google Scholar] [CrossRef]
- Hall Scullin, E.; Goldthorpe, J.; Milsom, K.; Tickle, M. A qualitative study of the views of adolescents on their caries risk and prevention behaviours. BMC Oral Health 2015, 15, 141–150. [Google Scholar] [CrossRef]
- Almerich Torres, T.; Montiel Company, J.M.; Bellot Arcís, C.; Almerich Silla, J.M. Relationship between caries, body mass index and social class in Spanish children. Gac. Sanit. 2017, 31, 499–504. [Google Scholar] [CrossRef][Green Version]
- Kumar, S.; Tadakamadla, J.; Duraiswamy, P.; Kulkarni, S. Dental caries and its socio-behavioral predictors—An exploratory cross-sectional study. J. Clin. Pediatr. Dent. 2016, 40, 186–192. [Google Scholar] [CrossRef]
- Veiga, N.; Pereira, C.; Amaral, O. Prevalence and determinants of dental caries in Portuguese children. Procedia Soc. Behav. Sci. 2015, 171, 995–1002. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Spanish (n = 4315) n (%) | Immigrants (n = 253) n (%) | p-Value |
|---|---|---|---|
| Time since the last visit to the dentist, stomatologist or dental hygienist | |||
| ≤12 months | 2786 (64.57) | 122 (48.22) | <0.001 |
| >12 months | 1529 (35.43) | 131 (51.78) | |
| Do you have caries? | |||
| Yes | 401 (9.29) | 47 (18.58) | <0.001 |
| No | 3914 (90.71) | 206 (81.42) | |
| Do you have any teeth/molars with fillings or capped teeth? | |||
| Yes | 1093 (25.33) | 62 (24.51) | 0.75 |
| No | 3222 (74.67) | 191 (75.49) | |
| Do your gums bleed spontaneously or when you brush your teeth? | |||
| Yes | 180 (4.17) | 14 (5.53) | 0.6 |
| No | 4135 (95.83) | 239 (94.47) |
| Spanish (n = 4315) | Immigrants (n = 253) | |||||
|---|---|---|---|---|---|---|
| n (%) | OR (CI 95%) | ORa (CI 95%) | n (%) | OR (CI 95%) | ORa (CI 95%) | |
| Total | 1529 (35.43) | 131 (51.78) | ||||
| Gender | ||||||
| Male | 811 (53.04) | Reference | Reference | 77 (58.78) | Reference | Reference |
| Female | 718 (46.96) | 0.89 (0.79–1.01) | 0.94 (0.82–1.08) | 54 (41.22) | 0.66 (0.40–1.08) | 0.60 (0.35–1.03) |
| Age | ||||||
| 3–6 years old | 812 (53.11) | Reference | Reference | 59 (45.04) | Reference | Reference |
| 7–10 years old | 409 (26.75) | 0.18 (0.15–0.21) 1 | 0.17 (0.15–0.20) 1 | 45 (34.35) | 0.35 (0.19–0.66) 1 | 0.31 (0.15–0.64) 1 |
| 11–14 years old | 308 (20.14) | 0.16 (0.14–0.20) 1 | 0.15 (0.13–0.18) 1 | 27 (20.61) | 0.21 (0.11–0.42) 1 | 0.19 (0.09–0.41) 1 |
| Size of town of residence | ||||||
| <10,000 inhab | 305 (19.95) | Reference | Reference | 17 (12.98) | Reference | Reference |
| 10,000–100,000 inhab | 658 (43.03) | 1.04 (0.89–1.25) | 1.09 (0.91–1.32) | 83 (63.36) | 1.44 (0.20–2.07) | 1.01 (0.36–2.79) |
| >100,000 inhab | 566 (37.02) | 1.05 (0.79–1.11) | 1.11 (0.92–1.34) | 31 (23.66) | 1.58 (0.22–2.57) | 1.89 (0.29–2.74) |
| Type of household | ||||||
| Couple | 1204 (78.74) | Reference | Reference | 101 (77.10) | Reference | Reference |
| Father or mother | 146 (9.55) | 0.76 (0.62–1.94) | 0.67 (0.54–1.84) | 19 (14.50) | 1.39 (0.65–2.97) | 1.57 (0.69–3.55) |
| Other type of household | 179 (11.71) | 0.99 (0.82–1.22) | 0.93 (0.75–1.15) | 11 (8.40) | 0.80 (0.34–1.88) | 0.68 (0.28–1.68) |
| Social class | ||||||
| Upper | 316 (20.67) | Reference | Reference | 8 (6.11) | Reference | Reference |
| Middle | 491 (32.11) | 1.12 (1.05–1.20) 1 | 1.16 (1.11–1.23) 1 | 21 (16.03) | 1.58 (1.30–2.53) 1 | 1.13 (1.35–3.63) 1 |
| Lower | 722 (47.22) | 1.34 (1.14–1.58) 1 | 1.59 (1.33–1.90) 1 | 102 (77.86) | 1.80 (1.69–4.68) 1 | 2.42 (1.84–2.97) 2 |
| Spanish (n = 4315) | Immigrants (n = 253) | |||||
|---|---|---|---|---|---|---|
| n (%) | OR (CI 95%) | ORa (CI 95%) | n (%) | OR (CI 95%) | ORa (CI 95%) | |
| Total | 1342 (31.10) | 92 (36.36) | ||||
| Gender | ||||||
| Male | 668 (49.78) | Reference | Reference | 51 (55.43) | Reference | Reference |
| Female | 674 (50.22) | 1.08 (0.96–1.24) | 1.04 (0.91–1.19) | 41 (44.57) | 0.89 (0.54–1.50) | 0.94 (0.54–1.64) |
| Age | ||||||
| 3–6 years old | 163 (12.15) | Reference | Reference | 13 (14.13) | Reference | Reference |
| 7–10 years old | 527 (39.27) | 2.29 (1.52–2.32) 1 | 2.27 (1.52–2.47) 1 | 35 (38.04) | 2.53 (1.65–2.64) 1 | 2.36 (1.62–2.88) 1 |
| 11–14 years old | 652 (48.58) | 2.29 (1.55–2.41) 1 | 2.36 (1.57–2.53) 1 | 44 (47.83) | 2.58 (1.93–2.78) 1 | 2.14 (1.62–2.30) 1 |
| Size of town of residence | ||||||
| <10,000 inhab | 291 (21.68) | Reference | Reference | 7 (7.61) | Reference | Reference |
| 10,000–100,000 inhab | 543 (40.46) | 0.85 (0.52–0.97) 2 | 0.84 (0.43–0.91) 2 | 61 (66.30) | 1.41 (0.56–1.57) | 0.45 (0.15–1.38) |
| >100,000 inhab | 508 (37.85) | 0.79 (0.72–0.92) 2 | 0.77 (0.64–0.93) 2 | 24 (26.09) | 1.93 (0.69–2.35) | 0.83 (0.25–1.79) |
| Type of household | ||||||
| Couple | 1.056 (78.69) | Reference | Reference | 73 (79.35) | Reference | Reference |
| Father or mother | 145 (10.80) | 0.92 (0.75–1.13) | 0.98 (0.79–1.21) | 13 (14.13) | 1.16 (0.54–2.49) | 1.12 (0.49–2.56) |
| Other type of household | 141 (10.51) | 0.86 (0.70–1.06) | 0.89 (0.72–1.11) | 6 (6.52) | 0.57 (0.22–1.49) | 0.62 (0.22–1.73) |
| Social class | ||||||
| Upper | 277 (20.64) | Reference | Reference | 4 (4.35) | Reference | Reference |
| Middle | 450 (33.53) | 1.08 (0.90–1.29) | 1.08 (0.90–1.29) | 63 (68.48) | 2.02 (0.64–2.34) | 1.60 (0.48–2.33) |
| Lower | 615 (45.83) | 1.26 (1.06–1.49) 2 | 1.18 (0.99–1.41) 2 | 25 (27.17) | 3.23 (1.95–4.01) 2 | 2.55 (1.70–3.31) 2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Portero de la Cruz, S.; Cebrino, J. Oral Health Problems and Utilization of Dental Services among Spanish and Immigrant Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 738. https://doi.org/10.3390/ijerph17030738
Portero de la Cruz S, Cebrino J. Oral Health Problems and Utilization of Dental Services among Spanish and Immigrant Children and Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(3):738. https://doi.org/10.3390/ijerph17030738
Chicago/Turabian StylePortero de la Cruz, Silvia, and Jesús Cebrino. 2020. "Oral Health Problems and Utilization of Dental Services among Spanish and Immigrant Children and Adolescents" International Journal of Environmental Research and Public Health 17, no. 3: 738. https://doi.org/10.3390/ijerph17030738
APA StylePortero de la Cruz, S., & Cebrino, J. (2020). Oral Health Problems and Utilization of Dental Services among Spanish and Immigrant Children and Adolescents. International Journal of Environmental Research and Public Health, 17(3), 738. https://doi.org/10.3390/ijerph17030738