The Effects of Temperament on Depression According to the Schema Model: A Scoping Review



Abstract
1. Introduction
1.1. About Depression
1.2. Psychological Treatments for Depression
1.3. New Therapeutic Approaches to Depression
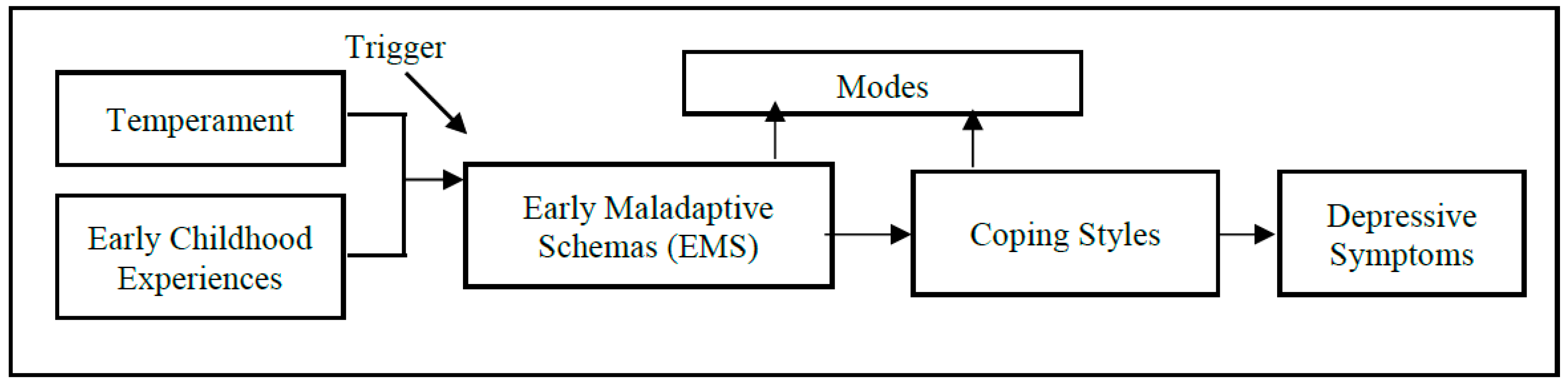
1.4. About the Schema Model
2. Scoping Review
2.1. Objectives and Questions
2.1.1. Objectives
2.1.2. Questions
2.2. Inclusion and Exclusion Criteria
2.2.1. Types of Participants
2.2.2. Concept
2.2.3. Context
2.2.4. Outcome
2.2.5. Types of Sources
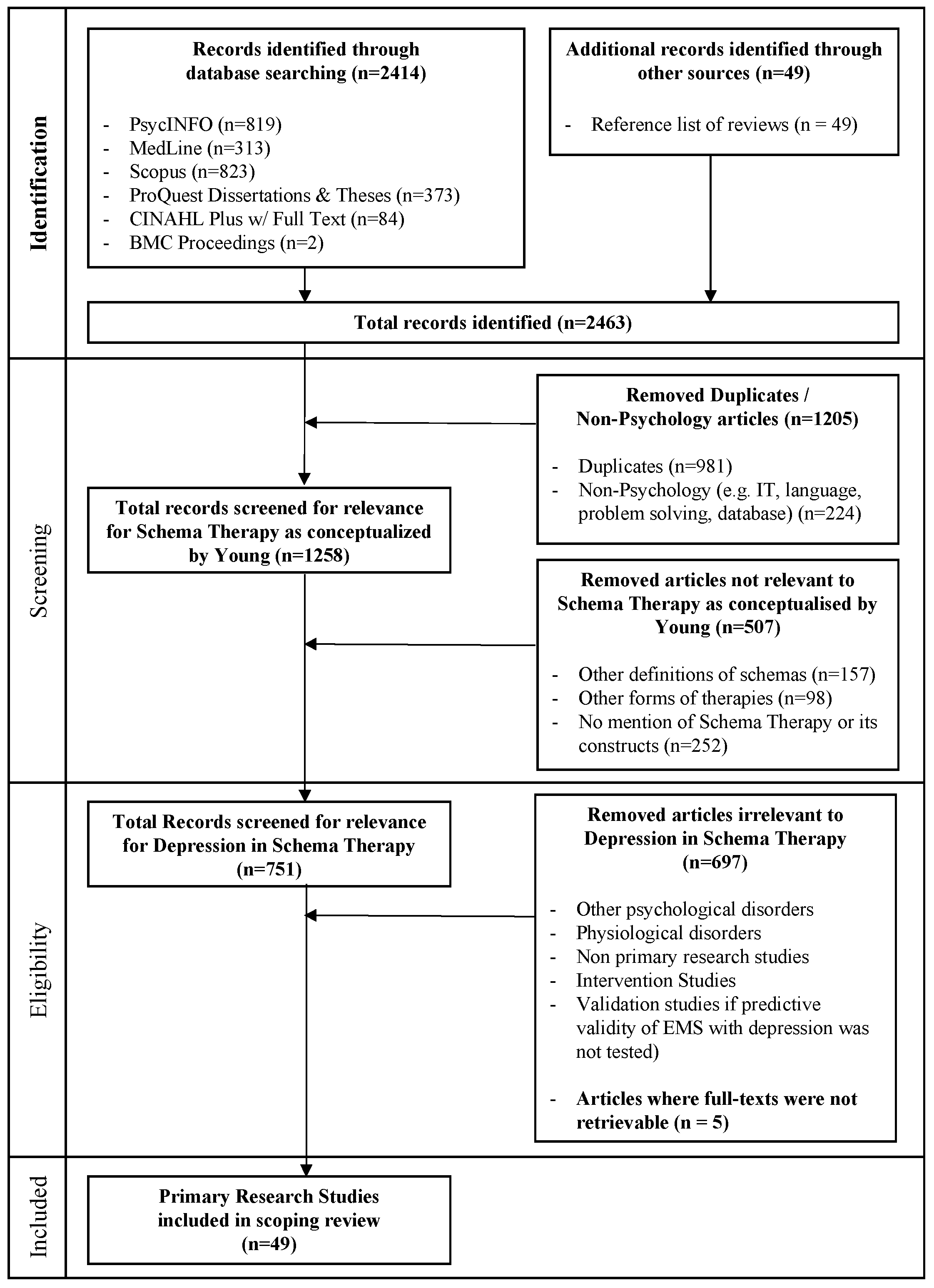
2.3. Search Strategy
2.3.1. Pre-Identification Stage
2.3.2. Identification Stage
2.3.3. Screening Stage
2.3.4. Eligibility Stage
2.3.5. Final Screening Stage
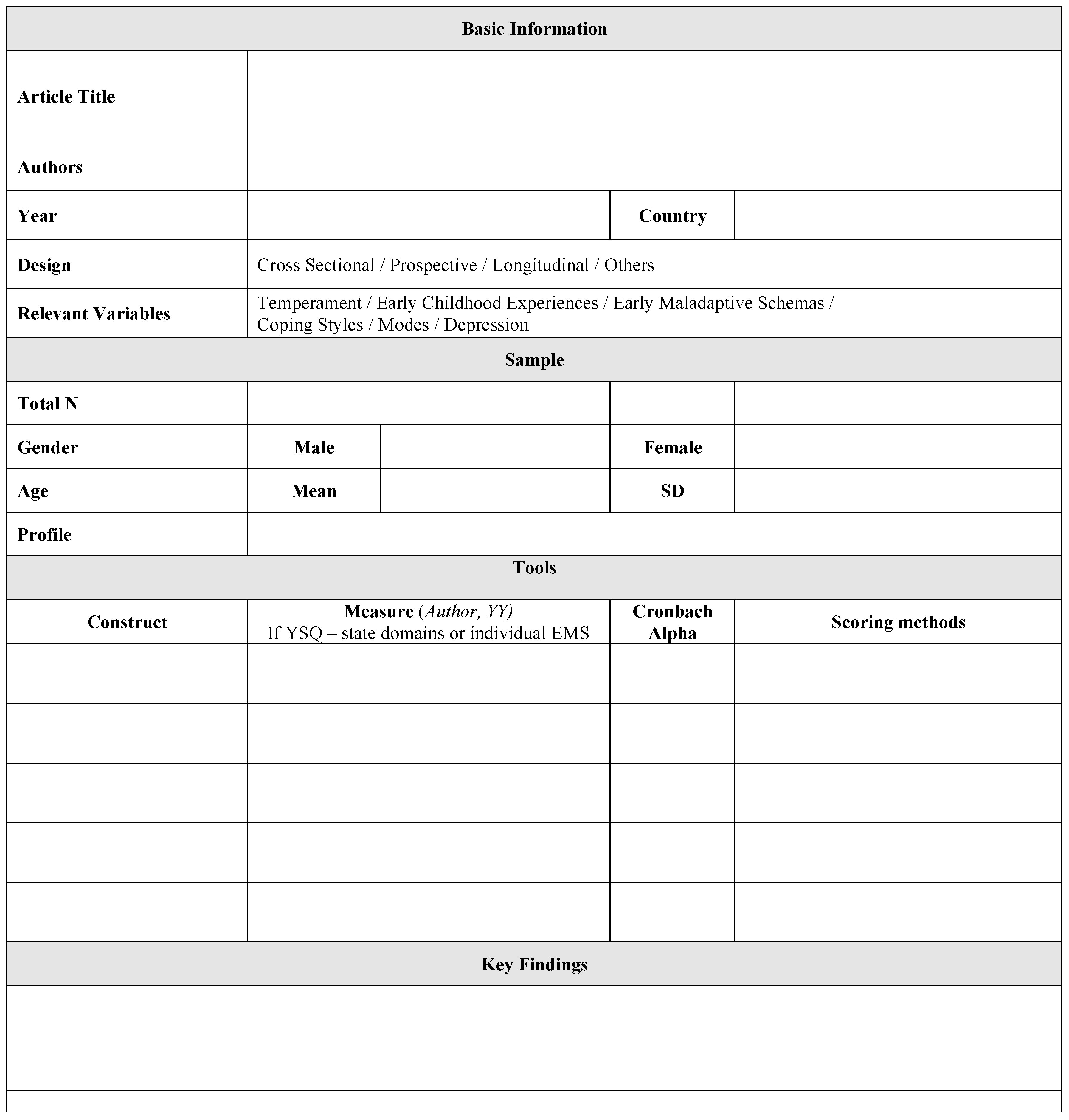
2.4. Data Extraction Process
3. Results of Scoping Review—Temperament
3.1. Overview
3.2. Findings in Relation to ST and Depression
Muris (2006). Maladaptive schemas, perceived parental behaviors, big five personality factors, and psychopathological symptoms in non-clinical adolescents.[31]
Halvorsen et al. (2009). Early maladaptive schemas, temperament and character traits in a mixed adult sample.[34]
Jesinoski (2010) Negative childhood experiences, temperament and negative affectivity among undergraduates.[33]
Balsamo (2013). Personality and depression among undergraduates.[36]
Calvete (2014). Neuroticism, emotional abuse, early maladaptive schemas, and depressive symptoms among adolescents.[30]
3.3. Overall Findings of Existing Research
3.3.1. Neuroticism
3.3.2. Harm Avoidance, Self-Directedness, and Cooperativeness
3.3.3. Ruled out Variables
4. An Examination of the Two Models
4.1. The Five Factor Model (FFM)
4.2. Psychobiological Model of Personality (PBM)
4.3. Overall Suitabaility to Assess Temperament
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. What Is Depression? Available online: https://www.psychiatry.org/patients-families/depression/what-is-depression (accessed on 1 May 2018).
- World Health Organisation. Depression and other Common Mental Health Disorders Global Health Estimates. Available online: http://www.who.int/news-room/fact-sheets/detail/depression (accessed on 1 May 2018).
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Depression in adults: Recognition and Management. Available online: https://www.nice.org.uk/guidance/cg90/chapter/2-Research-recommendations (accessed on 23 May 2018).
- Anxiety and Depression Association of American. Clinical Practice Review for Major Depressive Disorder. Available online: https://adaa.org/resources-professionals/practice-guidelines-mdd (accessed on 22 May 2018).
- Shea, M.T.; Elkin, I.; Imber, S.D.; Sotsky, S.M.; Watkins, J.T.; Collins, J.F.; Pilkonis, P.A. Course of depressive symptoms over follow-up: Findings from the National Institute of Mental Health Treatment of Depression Collaborative Research Program. Arch. Gen. Psychiatry 1992, 49, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Smit, F.; Bohlmeijer, E.; Hollon, S.D.; Andersson, G. Efficacy of cognitive-behavioural therapy and other psychological treatments for adult depression: Meta-analytic study of publication bias. Br. J. Psychiatry 2010, 196, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Roy, K.; Eyers, K. Cognitive behavior therapy for depression? Choose horses for courses. Am. J. Psychiatry 2003, 160, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. Cognitive Therapy of Depression, 1st ed.; Guilford Press: New York, NY, USA, 1979; ISBN 0898629195. [Google Scholar]
- Clark, D.A. Perceived limitations of standard cognitive therapy: A consideration of efforts to revise Beck’s theory and therapy. J. Cogn. Psychother. 1995, 9, 153. [Google Scholar]
- Hawke, L.D.; Provencher, M.D. Schema theory and schema therapy in mood and anxiety disorders: A review. J. Cogn. Psychother. 2011, 25, 257. [Google Scholar] [CrossRef]
- Clark, D.A.; Beck, A.T. Scientific Foundations of Cognitive Theory and Therapy of Depression, 1st ed.; John Wiley & Sons: New York, NY, USA, 1999; ISBN 0471189707. [Google Scholar]
- Young, J.E. Cognitive Therapy for Personality Disorders: A Schema-focused Approach, 3rd ed.; Professional Resource Press/Professional Resource Exchange: Sarasota, FL, USA, 1994; ISBN 1568870477. [Google Scholar]
- Young, J.E.; Klosko, J.S.; Weishaar, M.E. Schema Therapy: A Practitioner's Guide, 1st ed.; Guilford Press: New York, NY, USA, 2003; ISBN 1593853726. [Google Scholar]
- Ainsworth, M.S.; Bowlby, J. An ethological approach to personality development. Am. Psychol. 1991, 46, 333. [Google Scholar] [CrossRef]
- Greenberg, J. Object Relations in Psychoanalytic Theory, 1st ed.; Harvard University Press: Cambridge, UK, 1983; ISBN 0674629752. [Google Scholar]
- Balsamo, M.; Carlucci, L.; Murdock, K.; Saggino, A. The Mediating Role of Early Maladaptive Schemas in the Relation between Co-rumination and Depression in Young Adults. PLoS ONE 2015, e0140177. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, L.; D’Ambrosio, I.; Innamorati, M.; Saggino, A.; Balsamo, M. Co-rumination, anxiety, and maladaptive cognitive schemas: When friendship can hurt. Psychol. Res. Behav. Manag. 2018, 11, 133. [Google Scholar] [CrossRef] [PubMed]
- Jacob, G.A.; Arntz, A. Schema therapy for personality disorders—A review. Int. J. Cogn. Ther. 2013, 6, 171–185. [Google Scholar] [CrossRef]
- Masley, S.A.; Gillanders, D.T.; Simpson, S.G.; Taylor, M.A. A systematic review of the evidence base for schema therapy. Cogn. Behav. Ther. 2012, 41, 185–202. [Google Scholar] [CrossRef] [PubMed]
- Crilly, T.; Jashapara, A.; Ferlie, E. Research Utilisation and Knowledge Mobilisation: A Scoping Review of the Literature. Available online: https://repository.royalholloway.ac.uk/file/b8101c3b-4572-c3ea-57ea-73b46830629f/9/Jashapara_Research_utilisation_2010.pdf (accessed on 11 June 2018).
- De Chavez, A.C.; Backett-Milburn, K.; Parry, O.; Platt, S. Understanding and researching wellbeing: Its usage in different disciplines and potential for health research and health promotion. Health Educ. J. 2005, 64, 70–87. [Google Scholar] [CrossRef]
- Decaria, J.; Sharp, C.; Petrella, R. Scoping review report: Obesity in older adults. Int. J. Obes. 2012, 36, 1141. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, Australia, 2015. [Google Scholar]
- Fischer, T.D.; Smout, M.F.; Delfabbro, P.H. The relationship between psychological flexibility, early maladaptive schemas, perceived parenting and psychopathology. J. Context. Behav. Sci. 2016, 5, 169–177. [Google Scholar] [CrossRef]
- Yigit, I.; Erden, G. The Mediating Role of Early Maladaptive Schemas in the Relationship between Childhood Abuse Experiences and Psychological Wellbeing. Turk Psikoloji Dergisi 2015, 30, 47–63. [Google Scholar]
- Goldberg, L.R. An alternative “description of personality”: The big-five factor structure. J. Personal. Soc. Psychol. 1990, 59, 1216. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Przybeck, T.R.; Svrakic, D.M.; Wetzel, R.D. The Temperament and Character Inventory (TCI): A Guide to Its Development and Use. Available online: https://www.researchgate.net/profile/Robert_Cloninger/publication/264329741_TCI-Guide_to_Its_Development_and_Use/links/53d8ec870cf2e38c6331c2ee/TCI-Guide-to-Its-Development-and-Use.pdf (accessed on 1 May 2018).
- Barbaranelli, C.; Caprara, G.V.; Rabasca, A.; Pastorelli, C. A questionnaire for measuring the Big Five in late childhood. Personal. Individ. Differ. 2003, 34, 645–664. [Google Scholar] [CrossRef]
- Calvete, E. Emotional abuse as a predictor of early maladaptive schemas in adolescents: Contributions to the development of depressive and social anxiety symptoms. Child Abuse Negl. 2014, 38, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Muris, P. Maladaptive schemas in non-clinical adolescents: Relations to perceived parental rearing behaviours, big five personality factors and psychopathological symptoms. Clin. Psychol. Psychother. 2006, 13, 405–413. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. NEO PI-R Professional Manual, 1st ed.; Psychological Assessment Resources Inc.: Lutz, FL, USA, 1992; ISBN 9789997924452. [Google Scholar]
- Jesinoski, M.S. Young’s Schema Theory: Exploring the Direct and Indirect Links between Negative Childhood Experiences and Temperament to Negative Affectivity in Adulthood. Ph.D. Thesis, Utah State University, Logan, UT, USA, 2010. [Google Scholar]
- Halvorsen, M.; Wang, C.E.; Richter, J.; Myrland, I.; Pedersen, S.K.; Eisemann, M.; Waterloo, K. Early maladaptive schemas, temperament and character traits in clinically depressed and previously depressed subjects. Clin. Psychol. Psychother. 2009, 16, 394–407. [Google Scholar] [CrossRef] [PubMed]
- Cloninger, C.R. The Temperament and Character Inventory-Revised; Centre for Psychobiology of Personality Washington University: St Louis, MO, USA, 1999. [Google Scholar]
- Balsamo, M. Personality and depression: Evidence for a possible mediating role for anger trait in the relationship between cooperativeness and depression. Compr. Psychiatry 2013, 54, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kagan, J.; Reznick, J.S.; Snidman, N. Biological bases of childhood shyness. Science 1988, 240, 167–171. [Google Scholar] [CrossRef] [PubMed]
- McCrae, R.R.; Costa, P.T., Jr. A five-factor theory of personality. Handb. Personal. Theory Res. 1999, 2, 139–153. [Google Scholar]
- Tupes, E.C.; Christal, R.E. Recurrent personality factors based on trait ratings. J. Personal. 1992, 60, 225–251. [Google Scholar] [CrossRef]
- Saucier, G. Effects of variable selection on the factor structure of person descriptors. J. Personal. Soc. Psychol. 1997, 73, 1296. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. Personality in adulthood: A six-year longitudinal study of self-reports and spouse ratings on the NEO Personality Inventory. J. Personal. Soc. Psychol. 1988, 54, 853. [Google Scholar] [CrossRef]
- Lanning, K. Dimensionality of observer ratings on the California Adult Q-set. J. Personal. Soc. Psychol. 1994, 67, 151. [Google Scholar] [CrossRef]
- Clark, L.A.; Livesley, W.J. Two Approaches to Identifying the Dimensions of Personality Disorder: Convergence on the Five-factor Model; American Psychological Association: Washington, DC, USA, 2002. [Google Scholar]
- Jang, K.L.; McCrae, R.R.; Angleitner, A.; Riemann, R.; Livesley, W.J. Heritability of facet-level traits in a cross-cultural twin sample: Support for a hierarchical model of personality. J. Personal. Soc. Psychol. 1998, 74, 1556. [Google Scholar] [CrossRef]
- Yamagata, S.; Suzuki, A.; Ando, J.; Ono, Y.; Kijima, N.; Yoshimura, K.; Ostendorf, F.; Angleitner, A.; Riemann, R.; Spinath, F.M. Is the genetic structure of human personality universal? A cross-cultural twin study from North America, Europe, and Asia. J. Personal. Soc. Psychol. 2006, 90, 987. [Google Scholar] [CrossRef] [PubMed]
- Molfese, V.J.; Molfese, D.L.; McCrae, R.R. Stability of temperament in childhood: Laboratory infant assessment to parent report at seven years. In Temperament and Personality Development across the Life Span, 1st ed.; Psychology Press: London, UK, 2000; pp. 95–130. [Google Scholar]
- Roberts, B.W.; DelVecchio, W.F. The rank-order consistency of personality traits from childhood to old age: A quantitative review of longitudinal studies. Psychol. Bull. 2000, 126, 3. [Google Scholar] [CrossRef] [PubMed]
- Rothbart, M.K.; Ahadi, S.A.; Evans, D.E. Temperament and personality: Origins and outcomes. J. Personal. Soc. Psychol. 2000, 78, 122. [Google Scholar] [CrossRef]
- Eysenck, H.J. Intelligence assessment: A theoretical and experimental approach. Br. J. Educ. Psychol. 1967, 37, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Eysneck, H.; Eysneck, M. Personality and individual differences. In A Natural Science Approach, 1st ed.; Plenum Press: New York, NY, USA; Singapore, 1985; ISBN 0306418444. [Google Scholar]
- McNaughton, N.; Gray, J.A. Anxiolytic action on the behavioural inhibition system implies multiple types of arousal contribute to anxiety. J. Affect. Disord. 2000, 61, 161–176. [Google Scholar] [CrossRef]
- Ormel, J.; Jeronimus, B.F.; Kotov, R.; Riese, H.; Bos, E.H.; Hankin, B.; Rosmalen, J.G.; Oldehinkel, A.J. Neuroticism and common mental disorders: Meaning and utility of a complex relationship. Clin. Psychol. Rev. 2013, 33, 686–697. [Google Scholar] [CrossRef] [PubMed]
- Lahey, B.B. Public health significance of neuroticism. Am. Psychol. 2009, 64, 241. [Google Scholar] [CrossRef] [PubMed]
- Pervin, L.A.; John, O.P. Handbook of Personality: Theory and Research; Elsevier: New York, NY, USA, 1999. [Google Scholar]
- Josefsson, K.; Cloninger, C.R.; Hintsanen, M.; Jokela, M.; Pulkki-Raback, L.; Keltkangas-Jarvinen, L. Associations of personality profiles with various aspects of well-being: A population–based study. J. Affect. Disord. 2011, 133, 265–273. [Google Scholar] [PubMed]
- Miettunen, J.; Lauronen, E.; Kantojärvi, L.; Veijola, J.; Joukamaa, M. Inter-correlations between Cloninger’s temperament dimensions—A meta-analysis. Psychiatry Res. 2008, 160, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Atalay, H.; Akbaş, N.B.; Zahmacıoğlu, O.; Kılıç, E.Z.; Göktuna, Z. Are early maladaptive schemas, temperament and character dimensions correlated. Open J. Psychiatry 2013, 3, 206. [Google Scholar] [CrossRef]
- Farmer, R.F.; Goldberg, L.R. Brain modules, personality layers, planes of being, spiral structures, and the equally implausible distinction between TCI-R “temperament” and “character” scales: Reply to Cloninger. Psychol. Assess. 2008, 20, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.L.; Svrakic, D.M.; Przybeck, T.R.; Cloninger, R.C. The relationship of personality to mood and anxiety states: A dimensional approach. J. Psychiatry. Res. 1992, 26, 197–211. [Google Scholar] [CrossRef]
- Strakowski, S.M.; Faedda, G.L.; Tohen, M.; Goodwin, D.C.; Stoll, A.L. Possible affective-state dependence of the Tridimensional Personality Questionnaire in first-episode psychosis. Psychiatry Res. 1992, 41, 215–226. [Google Scholar] [CrossRef]
- Joffe, R.T.; Bagby, R.M.; Levitt, A.J.; Regan, J.J.; Parker, J.D. The Tridimensional Personality Questionnaire in major depression. Am. J. Psychiatry 1993, 150, 959–960. [Google Scholar] [PubMed]
- Joyce, P.R.; Mulder, R.T.; Cloninger, C.R. Temperament predicts clomipramine and desipramine response in major depression. J. Affect. Disord. 1994, 30, 35–46. [Google Scholar] [CrossRef]
- Svrakic, D.M.; Przybeck, T.R.; Cloninger, C.R. Mood states and personality traits. J. Affect. Disord. 1992, 24, 217–226. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Are Articles Relevant to SM [13,14]? | |
|---|---|
| Articles Containing the Following Terms Are | |
| Likely to Be Relevant | Unlikely to Be Relevant |
| (Other Definitions of Schemas)
|
(Other Therapies)
| |
(Others)
| |
| (If there were no mention of Schema Therapy and its related constructs in article’s title and/or abstract) | |
| Are Articles Relevant to Pathways to Depression within ST [13,14]? | |
|---|---|
| Articles Containing the Following Terms Are | |
| Likely to Be Relevant | Unlikely to Be Relevant |
|
|
| Construct | Model | Tool/Author/Year | Studies |
|---|---|---|---|
| Temperament | Five Factor Model | Big Five Questionnaire—Children (BFQ-C) [29] | Calvete, 2014 [30]; Muris, 2006 [31] |
| Five Factor Model | Neuroticism Extraversion Openness—Personality Inventory—Revised (NEO-PI-R) [32] | Jesinoski, 2010 [33] | |
| Temperament & Character | Psychobiological Model of Personality | Temperament & Character Inventory (TCI) [28] | Halvorsen et al., 2009 [34] |
| Psychobiological Model of Personality | Temperament & Character Inventory—Revised (TCI-R) [35] | Balsamo, 2013 [36] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, C.R.; Barlas, J.; Ho, R.C.M. The Effects of Temperament on Depression According to the Schema Model: A Scoping Review. Int. J. Environ. Res. Public Health 2018, 15, 1231. https://doi.org/10.3390/ijerph15061231
Lim CR, Barlas J, Ho RCM. The Effects of Temperament on Depression According to the Schema Model: A Scoping Review. International Journal of Environmental Research and Public Health. 2018; 15(6):1231. https://doi.org/10.3390/ijerph15061231
Chicago/Turabian StyleLim, Charmaine Ruling, Joanna Barlas, and Roger Chun Man Ho. 2018. "The Effects of Temperament on Depression According to the Schema Model: A Scoping Review" International Journal of Environmental Research and Public Health 15, no. 6: 1231. https://doi.org/10.3390/ijerph15061231
APA StyleLim, C. R., Barlas, J., & Ho, R. C. M. (2018). The Effects of Temperament on Depression According to the Schema Model: A Scoping Review. International Journal of Environmental Research and Public Health, 15(6), 1231. https://doi.org/10.3390/ijerph15061231