
Barriers and Facilitators to Artificial Intelligence Implementation in Diabetes Management from Healthcare Workers’ Perspective: A Scoping Review

 ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
1.1. Prevalence of Diabetes and Social Impact
1.2. Use of Devices and Technology in Diabetes Management
1.3. Study Aims
- What are the barriers and facilitators to the use of AI by healthcare professionals in the management of diabetes?
- Which quantitative and qualitative insights, as perceived by healthcare professionals, can most effectively inform the bottom-up implementation of AI in diabetes care?
2. Materials and Methods
2.1. Study Design and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
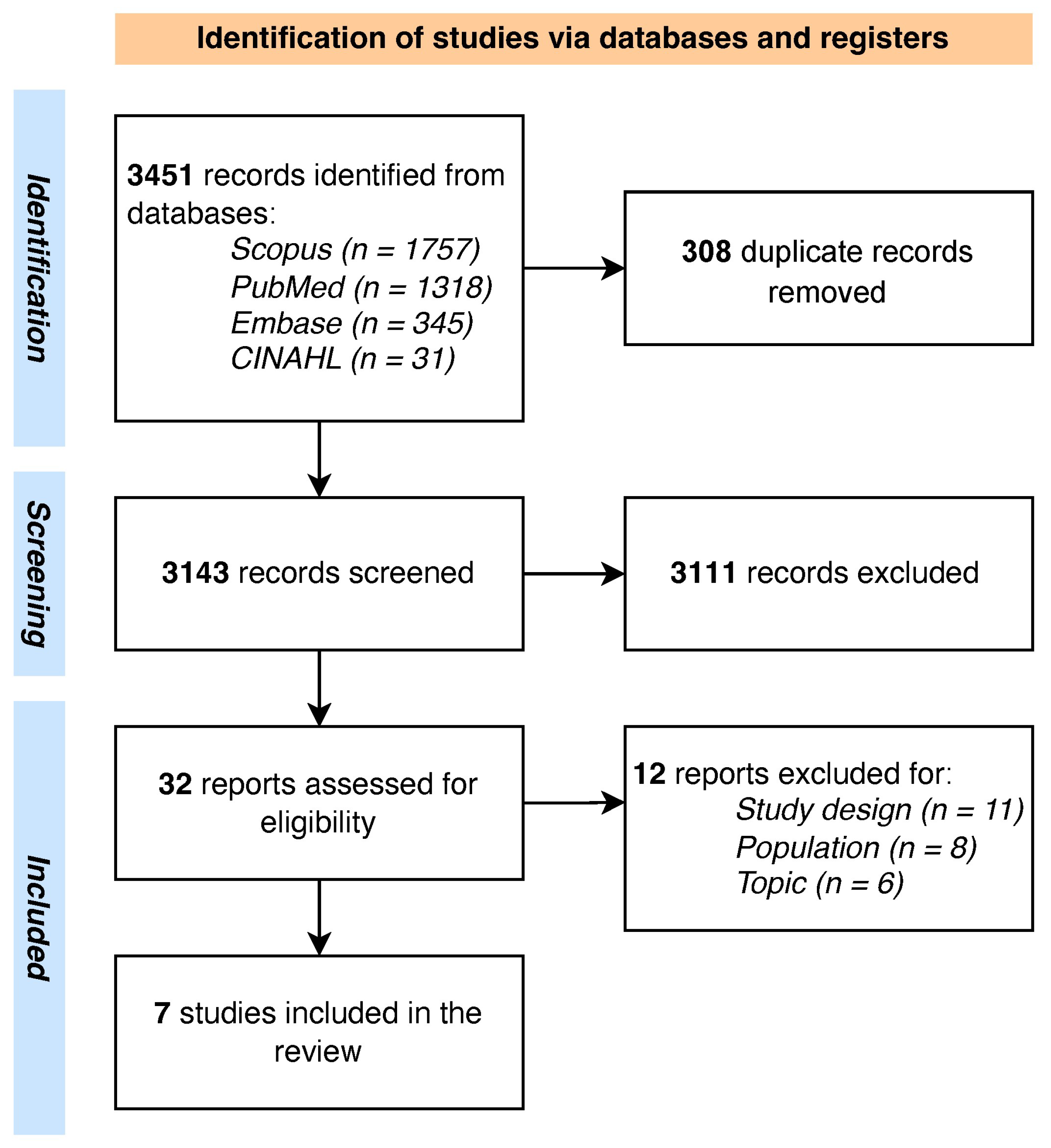
2.4. Study Selection Process
2.5. Data Extraction and Quality Appraisal
2.6. Conceptual and Analytical Framework
2.7. Synthesis of the Results
3. Results

{kind=link}
{kind=link}
| Study | Country | Study Design | Setting | Sample Size (N, % Female) | AI Type |
|---|---|---|---|---|---|
| Held et al., 2022 [51] | Germany | Qualitative | Primary care | 24 (42) | Smartphone-based and AI-supported diagnosis tools for the screening of diabetic retinopathy |
| Liao et al., 2024 [52] | China | Qualitative | Hospital and community healthcare center | 40 (42.5) | AI-assisted system for diabetic retinopathy screening |
| Petersen et al., 2024 [53] | Denmark | Qualitative | Hospital | 18 (61) | AI-assisted system for diabetic retinopathy screening |
| Romero et al., 2019 [55] | United States | Mixed -methods | Primary care outpatient clinics | 83 (N/A) | AI-powered clinical decision support system for identifying diabetes patients at risk of poor glycemic control |
| Roy et al., 2024 [54] | India | Cross-sectional | Physicians in clinical practice | 202 (N/A) | AI-based diabetes diagnostic interventions |
| Wahlich et al., 2024 [57] | United Kingdom | Qualitative | Hospital and community healthcare center | 98 (N/A) | AI-assisted system for diabetic retinopathy screening |
| Wewetzer et al., 2023 [56] | Germany | Cross-sectional | Primary care | 209 (107) | AI-assisted system for diabetic retinopathy screening |
3.1. Quality Appraisal
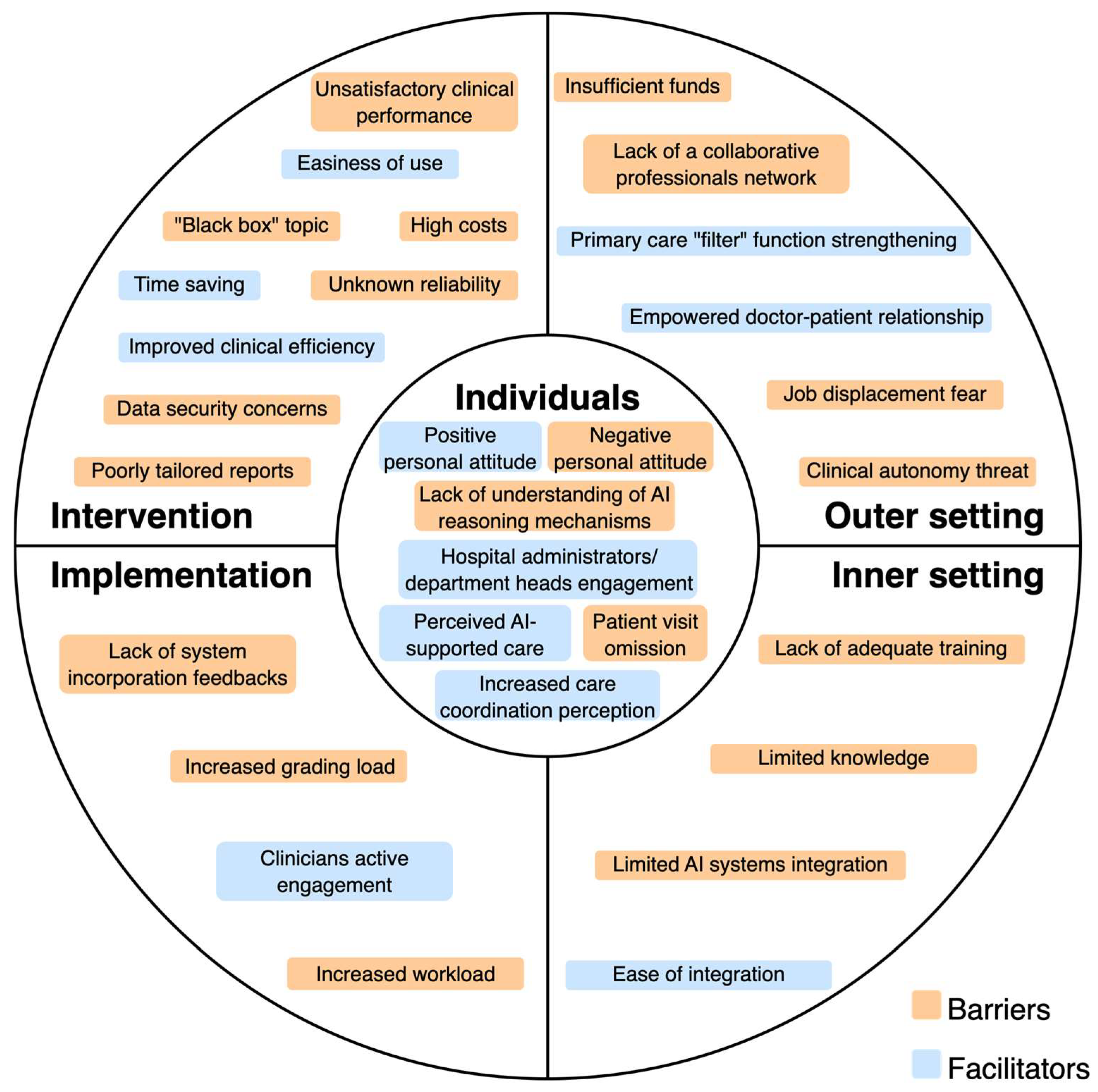
3.2. Barriers and Facilitators Identified According to the CFIR Framework
3.2.1. Individuals Domain
3.2.2. Intervention Domain
3.2.3. Implementation Process Domain
3.2.4. Inner Setting Domain
3.2.5. Outer Setting Domain
4. Discussion
4.1. Innovation, Effectiveness, and Trust in Technology
4.2. Equity and Sustainability: AI Costs, Access, and Integration
4.3. Healthcare System and Multilevel Governance
4.4. Training, Digital Literacy, and Empowerment
4.5. Opportunities for Public Health
4.6. Barriers and Facilitators in a Bottom-Up Perspective
4.7. A Public Health View on AI in Clinical Practice
4.8. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| IDF | International Diabetes Foundation |
| T2D | Type 2 Diabetes |
| T1D | Type 1 Diabetes |
| CGM | Continuous Glucose Monitoring |
| IP | Insulin Pump |
| MDI | Multiple Daily Injection |
| ML | Machine Learning |
| DL | Deep Learning |
| PRISMA-ScR | Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews |
| OSF | Open Science Foundation |
| PCC | Population, Concept, Context |
| JBI | Joanna Briggs Institute |
| MMAT | Mixed-Methods Appraisal Tool |
| CFIR | Consolidated Framework for Implementation Research |
| SD | Standard Deviation |
| SWIM | Synthesis Without Meta-Analysis |
| GP | General Practitioner |
| WHO | World Health Organization |
| EU | European Union |
References
- Aschner, P.; Karuranga, S.; James, S.; Simmons, D.; Basit, A.; Shaw, J.E.; Wild, S.H.; Ogurtsova, K.; Saeedi, P. The International Diabetes Federation’s Guide for Diabetes Epidemiological Studies. Diabetes Res. Clin. Pract. 2021, 172, 108630. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Diabetes—Fact Sheets. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 13 June 2025).
- Chen, X.; Zhang, L.; Chen, W. Global, Regional, and National Burdens of Type 1 and Type 2 Diabetes Mellitus in Adolescents from 1990 to 2021, with Forecasts to 2030: A Systematic Analysis of the Global Burden of Disease Study 2021. BMC Med. 2025, 23, 48. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th Edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.; Le, L.K.-D.; Ananthapavan, J.; Gao, L.; Dunstan, D.W.; Moodie, M. Economics of Sedentary Behaviour: A Systematic Review of Cost of Illness, Cost-Effectiveness, and Return on Investment Studies. Prev. Med. 2022, 156, 106964. [Google Scholar] [CrossRef]
- Alkaf, B.; Blakemore, A.I.; Järvelin, M.-R.; Lessan, N. Secondary Analyses of Global Datasets: Do Obesity and Physical Activity Explain Variation in Diabetes Risk across Populations? Int. J. Obes. 2021, 45, 944–956. [Google Scholar] [CrossRef]
- Komuro, K.; Kaneko, H.; Komuro, J.; Suzuki, Y.; Okada, A.; Mizuno, A.; Fujiu, K.; Takeda, N.; Morita, H.; Node, K.; et al. Differences in the Association of Lifestyle-Related Modifiable Risk Factors with Incident Cardiovascular Disease between Individuals with and without Diabetes. Eur. J. Prev. Cardiol. 2025, 32, 376–383. [Google Scholar] [CrossRef]
- Chimoriya, R.; Rana, K.; Adhikari, J.; Aitken, S.J.; Poudel, P.; Baral, A.; Rawal, L.; Piya, M.K. The Association of Physical Activity With Overweight/Obesity and Type 2 Diabetes in Nepalese Adults: Evidence From a Nationwide Non-Communicable Disease Risk Factor Survey. Obes. Sci. Pract. 2025, 11, e70046. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità Giornata Mondiale Diabete: Dalla Prevalenza All’accesso Alle Cure, I Numeri Della Sorveglianza Passi. Available online: https://www.iss.it/-/giornata-mondiale-diabete-da-prevalenza-ad-accesso-cure-i-numeri-del-sistema-passi (accessed on 13 June 2025).
- Istituto Nazionale di Statistica Il Diabete in Italia. Available online: https://www.istat.it/it/files/2017/07/REPORT_DIABETE.pdf (accessed on 13 June 2025).
- Jiang, Y.; Hu, J.; Chen, F.; Liu, B.; Wei, M.; Xia, W.; Yan, Y.; Xie, J.; Du, S.; Tian, X.; et al. Comprehensive Systematic Review and Meta-Analysis of Risk Factors for Childhood Obesity in China and Future Intervention Strategies. Lancet Reg. Health-West. Pac. 2025, 58, 101553. [Google Scholar] [CrossRef]
- Blanken, C.P.S.; Bayer, S.; Buchner Carro, S.; Hauner, H.; Holzapfel, C. Associations Between TCF7L2, PPARγ, and KCNJ11 Genotypes and Insulin Response to an Oral Glucose Tolerance Test: A Systematic Review. Mol. Nutr. Food Res. 2025, 69, e202400561. [Google Scholar] [CrossRef]
- Wang, Y.; Cao, P.; Liu, F.; Chen, Y.; Xie, J.; Bai, B.; Liu, Q.; Ma, H.; Geng, Q. Gender Differences in Unhealthy Lifestyle Behaviors among Adults with Diabetes in the United States between 1999 and 2018. IJERPH 2022, 19, 16412. [Google Scholar] [CrossRef]
- Teck, J. Diabetes-Associated Comorbidities. Prim. Care Clin. Off. Pract. 2022, 49, 275–286. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Holloway, S.; Polya, R.; Sloan, R.; Zhang, L.; Gregg, E.W.; Harrison, K.; Elvidge, J.; Jonsson, P.; Porter, T. Variations in Comorbidity Burden in People with Type 2 Diabetes over Disease Duration: A Population-Based Analysis of Real World Evidence. eClinicalMedicine 2022, 52, 101584. [Google Scholar] [CrossRef]
- Yu, M.G.; Gordin, D.; Fu, J.; Park, K.; Li, Q.; King, G.L. Protective Factors and the Pathogenesis of Complications in Diabetes. Endocr. Rev. 2024, 45, 227–252. [Google Scholar] [CrossRef] [PubMed]
- Bech, A.A.; Madsen, M.D.; Kvist, A.V.; Vestergaard, P.; Rasmussen, N.H. Diabetes Complications and Comorbidities as Risk Factors for MACE in People with Type 2 Diabetes and Their Development over Time: A Danish Registry-Based Case–Control Study. J. Diabetes 2025, 17, e70076. [Google Scholar] [CrossRef] [PubMed]
- Henney, A.E.; Gillespie, C.S.; Alam, U.; Hydes, T.J.; Boyland, E.; Cuthbertson, D.J. Ultra-processed Food and Non-communicable Diseases in the United Kingdom: A Narrative Review and Thematic Synthesis of Literature. Obes. Rev. 2024, 25, e13682. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Khandpur, N.; Desjardins, C.; Wang, L.; Monteiro, C.A.; Rossato, S.L.; Fung, T.T.; Manson, J.E.; Willett, W.C.; Rimm, E.B.; et al. Ultra-Processed Food Consumption and Risk of Type 2 Diabetes: Three Large Prospective U.S. Cohort Studies. Diabetes Care 2023, 46, 1335–1344. [Google Scholar] [CrossRef]
- Dai, W.; Albrecht, S.S. Sitting Time and Its Interaction With Physical Activity in Relation to All-Cause and Heart Disease Mortality in U.S. Adults with Diabetes. Diabetes Care 2024, 47, 1764–1768. [Google Scholar] [CrossRef]
- Rafiei, S.K.S.; Fateh, F.; Arab, M.; Espanlo, M.; Dahaghin, S.; Gilavand, H.K.; Shahrokhi, M.; Fallahi, M.S.; Zardast, Z.; Ansari, A.; et al. Weight Change and the Risk of Micro and Macro Vascular Complications of Diabetes: A Systematic Review. MJMS 2024, 31, 18–31. [Google Scholar] [CrossRef]
- Costa Hoffmeister, M.; Hammel Lovison, V.; Priesnitz Friedrich, E.; Da Costa Rodrigues, T. Ambulatory Blood Pressure Monitoring and Vascular Complications in Patients with Type 1 Diabetes Mellitus—Systematic Review and Meta-Analysis of Observational Studies. Diabetes Res. Clin. Pract. 2024, 217, 111873. [Google Scholar] [CrossRef]
- Perais, J.; Agarwal, R.; Evans, J.R.; Loveman, E.; Colquitt, J.L.; Owens, D.; Hogg, R.E.; Lawrenson, J.G.; Takwoingi, Y.; Lois, N. Prognostic Factors for the Development and Progression of Proliferative Diabetic Retinopathy in People with Diabetic Retinopathy. Cochrane Database Syst. Rev. 2023, 2023, CD013775. [Google Scholar] [CrossRef]
- Cangelosi, G.; Grappasonni, I.; Nguyen, C.T.T.; Acito, M.; Pantanetti, P.; Benni, A.; Petrelli, F. Mediterranean Diet (MedDiet) and Lifestyle Medicine (LM) for Support and Care of Patients with Type II Diabetes in the COVID-19 Era: A Cross-Observational Study. Acta Biomed. Atenei Parm. 2023, 94, e2023189. [Google Scholar] [CrossRef]
- Kanbour, S.; Ageeb, R.A.; Malik, R.A.; Abu-Raddad, L.J. Impact of Bodyweight Loss on Type 2 Diabetes Remission: A Systematic Review and Meta-Regression Analysis of Randomised Controlled Trials. Lancet Diabetes Endocrinol. 2025, 13, 294–306. [Google Scholar] [CrossRef]
- Petrelli, F.; Cangelosi, G.; Scuri, S.; Cuc Thi Thu, N.; Debernardi, G.; Benni, A.; Vesprini, A.; Rocchi, R.; De Carolis, C.; Pantanetti, P.; et al. Food Knowledge of Patients at the First Access to a Diabetology Center: Food Knowledge of Patients at the First Access to a Diabetology Center. Acta Biomed. Atenei Parm. 2020, 91, 160–164. [Google Scholar] [CrossRef]
- Aljawarneh, Y.M.; Wardell, D.W.; Wood, G.L.; Rozmus, C.L. A Systematic Review of Physical Activity and Exercise on Physiological and Biochemical Outcomes in Children and Adolescents with Type 1 Diabetes. J. Nurs. Scholarsh. 2019, 51, 337–345. [Google Scholar] [CrossRef]
- Steiman De Visser, H.; Fast, I.; Brunton, N.; Arevalo, E.; Askin, N.; Rabbani, R.; Abou-Setta, A.M.; McGavock, J. Cardiorespiratory Fitness and Physical Activity in Pediatric Diabetes: A Systemic Review and Meta-Analysis. JAMA Netw. Open 2024, 7, e240235. [Google Scholar] [CrossRef]
- Santos, L. The Impact of Nutrition and Lifestyle Modification on Health. Eur. J. Intern. Med. 2022, 97, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Amerkamp, J.; Benli, S.; Isenmann, E.; Brinkmann, C. Optimizing the Lifestyle of Patients with Type 2 Diabetes Mellitus—Systematic Review on the Effects of Combined Diet-and-Exercise Interventions. Nutr. Metab. Cardiovasc. Dis. 2025, 35, 103746. [Google Scholar] [CrossRef] [PubMed]
- Mannoubi, C.; Kairy, D.; Menezes, K.V.; Desroches, S.; Layani, G.; Vachon, B. The Key Digital Tool Features of Complex Telehealth Interventions Used for Type 2 Diabetes Self-Management and Monitoring with Health Professional Involvement: Scoping Review. JMIR Med. Inf. 2024, 12, e46699. [Google Scholar] [CrossRef] [PubMed]
- Jancev, M.; Vissers, T.A.C.M.; Visseren, F.L.J.; Van Bon, A.C.; Serné, E.H.; DeVries, J.H.; De Valk, H.W.; Van Sloten, T.T. Continuous Glucose Monitoring in Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetologia 2024, 67, 798–810. [Google Scholar] [CrossRef]
- Ferreira, R.O.M.; Trevisan, T.; Pasqualotto, E.; Chavez, M.P.; Marques, B.F.; Lamounier, R.N.; Van De Sande-Lee, S. Continuous Glucose Monitoring Systems in Noninsulin-Treated People with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Diabetes Technol. Ther. 2024, 26, 252–262. [Google Scholar] [CrossRef]
- Saetang, T.; Greeviroj, P.; Thavaraputta, S.; Santisitthanon, P.; Houngngam, N.; Laichuthai, N. The Effectiveness of Telemonitoring and Integrated Personalized Diabetes Management in People with Insulin-treated Type 2 Diabetes Mellitus. Diabetes Obes. Metab. 2024, 26, 5233–5238. [Google Scholar] [CrossRef] [PubMed]
- Kiran, M.; Xie, Y.; Anjum, N.; Ball, G.; Pierscionek, B.; Russell, D. Machine Learning and Artificial Intelligence in Type 2 Diabetes Prediction: A Comprehensive 33-Year Bibliometric and Literature Analysis. Front. Digit. Health 2025, 7, 1557467. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Tian, D.; Zhao, X.; Zhang, L.; Xu, Y.; Lu, X.; Chen, Y. Evolutionary Patterns and Research Frontiers of Artificial Intelligence in Age-Related Macular Degeneration: A Bibliometric Analysis. Quant. Imaging Med. Surg. 2025, 15, 813–830. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Bee, Y.M.; Lim, C.C.; Sabanayagam, C.; Yim-Lui Cheung, C.; Wong, T.Y.; Ting, D.S.W.; Lim, L.-L.; Li, H.; He, M.; et al. Use of Artificial Intelligence with Retinal Imaging in Screening for Diabetes-Associated Complications: Systematic Review. eClinicalMedicine 2025, 81, 103089. [Google Scholar] [CrossRef]
- Elmotia, K.; Abouyaala, O.; Bougrine, S.; Ouahidi, M.L. Effectiveness of AI-Driven Interventions in Glycemic Control: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Prim. Care Diabetes 2025, 19, 345–354. [Google Scholar] [CrossRef]
- Yismaw, M.B.; Tafere, C.; Tefera, B.B.; Demsie, D.G.; Feyisa, K.; Addisu, Z.D.; Zeleke, T.K.; Siraj, E.A.; Worku, M.C.; Berihun, F. Artificial Intelligence Based Predictive Tools for Identifying Type 2 Diabetes Patients at High Risk of Treatment Non-Adherence: A Systematic Review. Int. J. Med. Inform. 2025, 198, 105858. [Google Scholar] [CrossRef]
- Usman, T.M.; Saheed, Y.K.; Nsang, A.; Ajibesin, A.; Rakshit, S. A Systematic Literature Review of Machine Learning Based Risk Prediction Models for Diabetic Retinopathy Progression. Artif. Intell. Med. 2023, 143, 102617. [Google Scholar] [CrossRef]
- Khokhar, P.B.; Gravino, C.; Palomba, F. Advances in Artificial Intelligence for Diabetes Prediction: Insights from a Systematic Literature Review. Artif. Intell. Med. 2025, 164, 103132. [Google Scholar] [CrossRef]
- Senot, C.; Chandrasekaran, A.; Ward, P.T. Role of Bottom-Up Decision Processes in Improving the Quality of Health Care Delivery: A Contingency Perspective. Prod. Oper. Manag. 2016, 25, 458–476. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Pollock, D.; Peters, M.D.J.; Khalil, H.; McInerney, P.; Alexander, L.; Tricco, A.C.; Evans, C.; De Moraes, É.B.; Godfrey, C.M.; Pieper, D.; et al. Recommendations for the Extraction, Analysis, and Presentation of Results in Scoping Reviews. JBI Evid. Synth. 2023, 21, 520–532. [Google Scholar] [CrossRef]
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative Research Synthesis: Methodological Guidance for Systematic Reviewers Utilizing Meta-Aggregation. Int. J. Evid.-Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: North Adelaide, Australia, 2017. [Google Scholar]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) Version 2018 for Information Professionals and Researchers. EFI 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Camp, S.; Legge, T. Simulation as a Tool for Clinical Remediation: An Integrative Review. Clin. Simul. Nurs. 2018, 16, 48–61. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering Implementation of Health Services Research Findings into Practice: A Consolidated Framework for Advancing Implementation Science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without Meta-Analysis (SWiM) in Systematic Reviews: Reporting Guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef]
- Held, L.A.; Wewetzer, L.; Steinhäuser, J. Determinants of the Implementation of an Artificial Intelligence-Supported Device for the Screening of Diabetic Retinopathy in Primary Care—A Qualitative Study. Health Inform. J. 2022, 28, 14604582221112816. [Google Scholar] [CrossRef]
- Liao, X.; Yao, C.; Jin, F.; Zhang, J.; Liu, L. Barriers and Facilitators to Implementing Imaging-Based Diagnostic Artificial Intelligence-Assisted Decision-Making Software in Hospitals in China: A Qualitative Study Using the Updated Consolidated Framework for Implementation Research. BMJ Open 2024, 14, e084398. [Google Scholar] [CrossRef]
- Petersen, G.B.; Joensen, L.E.; Kristensen, J.K.; Vorum, H.; Byberg, S.; Fangel, M.V.; Cleal, B. How to Improve Attendance for Diabetic Retinopathy Screening: Ideas and Perspectives From People with Type 2 Diabetes and Health-Care Professionals. Can. J. Diabetes 2024, 49, 121–127. [Google Scholar] [CrossRef]
- Roy, M.; Jamwal, M.; Vasudeva, S.; Singh, M. Physicians Behavioural Intentions towards AI-Based Diabetes Diagnostic Interventions in India. J. Public Health 2024. [Google Scholar] [CrossRef]
- Romero-Brufau, S.; Wyatt, K.D.; Boyum, P.; Mickelson, M.; Moore, M.; Cognetta-Rieke, C. A Lesson in Implementation: A Pre-Post Study of Providers’ Experience with Artificial Intelligence-Based Clinical Decision Support. Int. J. Med. Inform. 2020, 137, 104072. [Google Scholar] [CrossRef]
- Wewetzer, L.; Held, L.A.; Goetz, K.; Steinhäuser, J. Determinants of the Implementation of Artificial Intelligence-Based Screening for Diabetic Retinopathy-a Cross-Sectional Study with General Practitioners in Germany. Digit. Health 2023, 9, 20552076231176644. [Google Scholar] [CrossRef]
- Wahlich, C.; Chandrasekaran, L.; Chaudhry, U.A.R.; Willis, K.; Chambers, R.; Bolter, L.; Anderson, J.; Shakespeare, R.; Olvera-Barrios, A.; Fajtl, J.; et al. Patient and Practitioner Perceptions around Use of Artificial Intelligence within the English NHS Diabetic Eye Screening Programme. Diabetes Res. Clin. Pract. 2025, 219, 111964. [Google Scholar] [CrossRef]
- Lucero-Prisno, D.E.; Shomuyiwa, D.O.; Kouwenhoven, M.B.N.; Dorji, T.; Odey, G.O.; Miranda, A.V.; Ogunkola, I.O.; Adebisi, Y.A.; Huang, J.; Xu, L.; et al. Top 10 Public Health Challenges to Track in 2023: Shifting Focus beyond a Global Pandemic. Public Health Chall. 2023, 2, e86. [Google Scholar] [CrossRef] [PubMed]
- Lucero-Prisno, D.E.; Shomuyiwa, D.O.; Kouwenhoven, M.B.N.; Dorji, T.; Adebisi, Y.A.; Odey, G.O.; George, N.S.; Ajayi, O.T.; Ekerin, O.; Manirambona, E.; et al. Top 10 Public Health Challenges for 2024: Charting a New Direction for Global Health Security. Public Health Chall. 2025, 4, e70022. [Google Scholar] [CrossRef]
- Balasubramaniam, N.; Kauppinen, M.; Rannisto, A.; Hiekkanen, K.; Kujala, S. Transparency and Explainability of AI Systems: From Ethical Guidelines to Requirements. Inf. Softw. Technol. 2023, 159, 107197. [Google Scholar] [CrossRef]
- Rajesh, A.E.; Davidson, O.Q.; Lee, C.S.; Lee, A.Y. Artificial Intelligence and Diabetic Retinopathy: AI Framework, Prospective Studies, Head-to-Head Validation, and Cost-Effectiveness. Diabetes Care 2023, 46, 1728–1739. [Google Scholar] [CrossRef]
- Hasan, S.U.; Siddiqui, M.A.R. Diagnostic Accuracy of Smartphone-Based Artificial Intelligence Systems for Detecting Diabetic Retinopathy: A Systematic Review and Meta-Analysis. Diabetes Res. Clin. Pract. 2023, 205, 110943. [Google Scholar] [CrossRef] [PubMed]
- Jha, D.; Durak, G.; Das, A.; Sanjotra, J.; Susladkar, O.; Sarkar, S.; Rauniyar, A.; Kumar Tomar, N.; Peng, L.; Li, S.; et al. Ethical Framework for Responsible Foundational Models in Medical Imaging. Front. Med. 2025, 12, 1544501. [Google Scholar] [CrossRef]
- European Commission Regulation (EU) 2024/1689 of the European Parliament and of the Council of 13 June 2024 Laying down Harmonised Rules on Artificial Intelligence and Amending Regulations (EC) No 300/2008, (EU) No 167/2013, (EU) No 168/2013, (EU) 2018/858, (EU) 2018/1139 and (EU) 2019/2144 and Directives 2014/90/EU, (EU) 2016/797 and (EU) 2020/1828 (Artificial Intelligence Act) (Text with EEA Relevance) 2024. Available online: https://eur-lex.europa.eu/eli/reg/2024/1689/oj/eng (accessed on 28 July 2025).
- Ahmad, Z.; Rahim, S.; Zubair, M.; Abdul-Ghafar, J. Artificial Intelligence (AI) in Medicine, Current Applications and Future Role with Special Emphasis on Its Potential and Promise in Pathology: Present and Future Impact, Obstacles Including Costs and Acceptance among Pathologists, Practical and Philosophical Considerations. A Comprehensive Review. Diagn. Pathol. 2021, 16, 24. [Google Scholar] [CrossRef]
- Wilkinson, D.; Savulescu, J. Cost-Equivalence and Pluralism in Publicly-Funded Health-Care Systems. Health Care Anal. 2018, 26, 287–309. [Google Scholar] [CrossRef]
- World Health Organization Ethics and Governance of Artificial Intelligence for Health. WHO Guidance. Available online: https://www.who.int/publications/i/item/9789240029200 (accessed on 5 June 2025).
- Walker, D.M.; Tarver, W.L.; Jonnalagadda, P.; Ranbom, L.; Ford, E.W.; Rahurkar, S. Perspectives on Challenges and Opportunities for Interoperability: Findings From Key Informant Interviews with Stakeholders in Ohio. JMIR Med. Inf. 2023, 11, e43848. [Google Scholar] [CrossRef]
- Garabedian, P.; Kain, J.; Emani, S.; Singleton, S.; Rozenblum, R.; Samal, L.; Mueller, S. User Requirements and Conceptual Design for an Electronic Data Platform for Interhospital Transfer Between Acute Care Hospitals: User-Centered Design Study. JMIR Hum. Factors 2025, 12, e67884. [Google Scholar] [CrossRef] [PubMed]
- United Nations Sustainable Development Goals. Available online: https://sdgs.un.org/goals (accessed on 21 July 2025).
- Gordon, D.; McKay, S.; Marchildon, G.; Bhatia, R.S.; Shaw, J. Collaborative Governance for Integrated Care: Insights from a Policy Stakeholder Dialogue. Int. J. Integr. Care 2020, 20, 3. [Google Scholar] [CrossRef]
- Faijue, D.D.; Segui, A.O.; Shringarpure, K.; Razavi, A.; Hasan, N.; Dar, O.; Manikam, L. Constructing a One Health Governance Architecture: A Systematic Review and Analysis of Governance Mechanisms for One Health. Eur. J. Public Health 2024, 34, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.K.; Doerr, M.; Schmit, C.D. AI Governance: A Challenge for Public Health. JMIR Public Health Surveill. 2024, 10, e58358. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Savage, C.; Nair, M.; Larsson, I.; Svedberg, P.; Nygren, J.M. Artificial Intelligence Applications in Health Care Practice: Scoping Review. J Med. Internet Res. 2022, 24, e40238. [Google Scholar] [CrossRef]
- Hassan, M.; Kushniruk, A.; Borycki, E. Barriers to and Facilitators of Artificial Intelligence Adoption in Health Care: Scoping Review. JMIR Hum Factors 2024, 11, e48633. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Wherton, J.; Papoutsi, C.; Lynch, J.; Hughes, G.; A’Court, C.; Hinder, S.; Fahy, N.; Procter, R.; Shaw, S. Beyond Adoption: A New Framework for Theorizing and Evaluating Nonadoption, Abandonment, and Challenges to the Scale-Up, Spread, and Sustainability of Health and Care Technologies. J Med. Internet Res. 2017, 19, e367. [Google Scholar] [CrossRef]
- Ahmed, M.I.; Spooner, B.; Isherwood, J.; Lane, M.; Orrock, E.; Dennison, A. A Systematic Review of the Barriers to the Implementation of Artificial Intelligence in Healthcare. Cureus 2023, 15, e46454. [Google Scholar] [CrossRef]
- Han, S.; Kang, H.S.; Gimber, P.; Lim, S. Nursing Students’ Perceptions and Use of Generative Artificial Intelligence in Nursing Education. Nurs. Rep. 2025, 15, 68. [Google Scholar] [CrossRef]
- Chew, B.-H.; Ngiam, K.Y. Artificial Intelligence Tool Development: What Clinicians Need to Know? BMC Med. 2025, 23, 244. [Google Scholar] [CrossRef]
- Alowais, S.A.; Alghamdi, S.S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A.I.; Almohareb, S.N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.A.; et al. Revolutionizing Healthcare: The Role of Artificial Intelligence in Clinical Practice. BMC Med. Educ. 2023, 23, 689. [Google Scholar] [CrossRef]
- Singh, K.; Prabhu, A.; Kaur, N. The Impact and Role of Artificial Intelligence (AI) in Healthcare: Systematic Review. CTMC 2025, 25. [Google Scholar] [CrossRef]
- Aravazhi, P.S.; Gunasekaran, P.; Benjamin, N.Z.Y.; Thai, A.; Chandrasekar, K.K.; Kolanu, N.D.; Prajjwal, P.; Tekuru, Y.; Brito, L.V.; Inban, P. The Integration of Artificial Intelligence into Clinical Medicine: Trends, Challenges, and Future Directions. Dis.-a-Mon. 2025, 71, 101882. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, N.K.; Galvão, C.; Santos, J.W.; Del Pino, C.; Pinto, E.P.; Barbosa, C.; Massmann, D.; Mambrini, R.; Galvão, L.; Terem, E.; et al. Worldwide AI Ethics: A Review of 200 Guidelines and Recommendations for AI Governance. Patterns 2023, 4, 100857. [Google Scholar] [CrossRef]
- Ratti, M.; Ceriotti, D.; Rescinito, R.; Bibi, R.; Panella, M. Does Robotic Assisted Technique Improve Patient Utility in Total Knee Arthroplasty? A Comparative Retrospective Cohort Study. Healthcare 2024, 12, 1650. [Google Scholar] [CrossRef] [PubMed]
- Uwimana, A.; Gnecco, G.; Riccaboni, M. Artificial Intelligence for Breast Cancer Detection and Its Health Technology Assessment: A Scoping Review. Comput. Biol. Med. 2025, 184, 109391. [Google Scholar] [CrossRef] [PubMed]
- Sguanci, M.; Mancin, S.; Gazzelloni, A.; Diamanti, O.; Ferrara, G.; Morales Palomares, S.; Parozzi, M.; Petrelli, F.; Cangelosi, G. The Internet of Things in the Nutritional Management of Patients with Chronic Neurological Cognitive Impairment: A Scoping Review. Healthcare 2024, 13, 23. [Google Scholar] [CrossRef]
- Sguanci, M.; Palomares, S.M.; Cangelosi, G.; Petrelli, F.; Sandri, E.; Ferrara, G.; Mancin, S. Artificial Intelligence in the Management of Malnutrition in Cancer Patients: A Systematic Review. Adv. Nutr. 2025, 16, 100438. [Google Scholar] [CrossRef]
- Hosain, M.N.; Kwak, Y.-S.; Lee, J.; Choi, H.; Park, J.; Kim, J. IoT-Enabled Biosensors for Real-Time Monitoring and Early Detection of Chronic Diseases. Phys. Act. Nutr. 2024, 28, 60–69. [Google Scholar] [CrossRef]
- Pantanetti, P.; Cangelosi, G.; Morales Palomares, S.; Ferrara, G.; Biondini, F.; Mancin, S.; Caggianelli, G.; Parozzi, M.; Sguanci, M.; Petrelli, F. Real-World Life Analysis of a Continuous Glucose Monitoring and Smart Insulin Pen System in Type 1 Diabetes: A Cohort Study. Diabetology 2025, 6, 7. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network Global. Burden of Disease Study 2021 (GBD 2021) Results. 2024. Available online: https://www.healthdata.org/sites/default/files/2024-05/GBD_2021_Booklet_FINAL_2024.05.16.pdf (accessed on 5 June 2025).
- Subramanian, M.; Wojtusciszyn, A.; Favre, L.; Boughorbel, S.; Shan, J.; Letaief, K.B.; Pitteloud, N.; Chouchane, L. Precision Medicine in the Era of Artificial Intelligence: Implications in Chronic Disease Management. J. Transl. Med. 2020, 18, 472. [Google Scholar] [CrossRef] [PubMed]
- Shao, H.; Shi, L.; Lin, Y.; Fonseca, V. Using Modern Risk Engines and Machine Learning/Artificial Intelligence to Predict Diabetes Complications: A Focus on the BRAVO Model. J. Diabetes Its Complicat. 2022, 36, 108316. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.B.; Fahim, C.; Garad, Y.; Presseau, J.; Hoens, A.M.; Braimoh, J.; Duncan, D.; Bruyn-Martin, L.; Straus, S.E. Developing the Intersectionality Supplemented Consolidated Framework for Implementation Research (CFIR) and Tools for Intersectionality Considerations. BMC Med. Res. Methodol. 2023, 23, 262. [Google Scholar] [CrossRef]
- Wienert, J.; Zeeb, H. Implementing Health Apps for Digital Public Health—An Implementation Science Approach Adopting the Consolidated Framework for Implementation Research. Front. Public Health 2021, 9, 610237. [Google Scholar] [CrossRef]
- Scanzera, A.C.; Beversluis, C.; Potharazu, A.V.; Bai, P.; Leifer, A.; Cole, E.; Du, D.Y.; Musick, H.; Chan, R.V.P. Planning an Artificial Intelligence Diabetic Retinopathy Screening Program: A Human-Centered Design Approach. Front. Med. 2023, 10, 1198228. [Google Scholar] [CrossRef]
- Pan, M.; Li, R.; Wei, J.; Peng, H.; Hu, Z.; Xiong, Y.; Li, N.; Guo, Y.; Gu, W.; Liu, H. Application of Artificial Intelligence in the Health Management of Chronic Disease: Bibliometric Analysis. Front. Med. 2025, 11, 1506641. [Google Scholar] [CrossRef]
- Serin, O.; Yıldırım, B.F.; Duman, F.; Ercorumlu, K.; Yavas, R.; Tasar, M.A.; Celik, M. Physician Perspectives on Artificial Intelligence in Healthcare: A Cross-Sectional Study of Child-Focused Care in a Turkish Tertiary Hospital. Int. J. Med. Inform. 2025, 203, 106003. [Google Scholar] [CrossRef]
- Gumus, E.; Alan, H. Perspectives of Physicians, Nurses, and Patients on the Use of Artificial Intelligence and Robotic Nurses in Healthcare. Int. Nurs. Rev. 2025, 72, e70017. [Google Scholar] [CrossRef]
- Vanamali, D.R.; Gara, H.K.; Dronamraju, V.A.C. Evaluation of Knowledge, Attitudes, and Practices among Healthcare Professionals toward Role of Artificial Intelligence in Healthcare. J. Assoc. Phys. India 2025, 73, e6–e12. [Google Scholar]
- Singareddy, S.; Sn, V.P.; Jaramillo, A.P.; Yasir, M.; Iyer, N.; Hussein, S.; Nath, T.S. Artificial Intelligence and Its Role in the Management of Chronic Medical Conditions: A Systematic Review. Cureus 2023, 15, e46066. [Google Scholar] [CrossRef]
- Nair, P.M.; Silwal, K.; Kodali, P.B.; Fogawat, K.; Binna, S.; Sharma, H.; Tewani, G.R. Impact of Holistic, Patient-Centric Yoga & Naturopathy-Based Lifestyle Modification Program in Patients with Musculoskeletal Disorders: A Quasi-Experimental Study. Adv. Integr. Med. 2023, 10, 184–189. [Google Scholar] [CrossRef]
- Baines, R.; Bradwell, H.; Edwards, K.; Stevens, S.; Prime, S.; Tredinnick-Rowe, J.; Sibley, M.; Chatterjee, A. Meaningful Patient and Public Involvement in Digital Health Innovation, Implementation and Evaluation: A Systematic Review. Health Expect. 2022, 25, 1232–1245. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Berenbrok, L.A.; Snader, L.; Soh, Y.H.; Kumar, V.K.; Javed, M.A.; Bates, D.W.; Sorce, L.R.; Kane-Gill, S.L. Facilitators and Barriers to Interacting with Clinical Decision Support in the ICU: A Mixed-Methods Approach. Crit. Care Explor. 2023, 5, e0967. [Google Scholar] [CrossRef] [PubMed]
- Scuri, S.; Tesauro, M.; Petrelli, F.; Argento, N.; Damasco, G.; Cangelosi, G.; Nguyen, C.T.T.; Savva, D.; Grappasonni, I. Use of an Online Platform to Evaluate the Impact of Social Distancing Measures on Psycho-Physical Well-Being in the COVID-19 Era. IJERPH 2022, 19, 6805. [Google Scholar] [CrossRef] [PubMed]
- Trinh, S.; Skoll, D.; Saxon, L.A. Health Care 2025: How Consumer-Facing Devices Change Health Management and Delivery. J. Med. Internet Res. 2025, 27, e60766. [Google Scholar] [CrossRef]
- Awad, A.; Trenfield, S.J.; Pollard, T.D.; Ong, J.J.; Elbadawi, M.; McCoubrey, L.E.; Goyanes, A.; Gaisford, S.; Basit, A.W. Connected Healthcare: Improving Patient Care Using Digital Health Technologies. Adv. Drug. Deliv. Rev. 2021, 178, 113958. [Google Scholar] [CrossRef]
- Neborachko, M.; Pkhakadze, A.; Vlasenko, I. Current Trends of Digital Solutions for Diabetes Management. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2997–3003. [Google Scholar] [CrossRef]
- Yang, J.; Amrollahi, A.; Marrone, M. Harnessing the Potential of Artificial Intelligence: Affordances, Constraints, and Strategic Implications for Professional Services. J. Strateg. Inf. Syst. 2024, 33, 101864. [Google Scholar] [CrossRef]
- Castiello, T. The Benefits and Challenges of Digitally-Enabled Cardiology. Br. J. Hosp. Med. 2025, 86, 1–6. [Google Scholar] [CrossRef]
- Warraich, H.J.; Tazbaz, T.; Califf, R.M. FDA Perspective on the Regulation of Artificial Intelligence in Health Care and Biomedicine. JAMA 2025, 333, 241. [Google Scholar] [CrossRef]
- Geukes Foppen, R.J.; Gioia, V.; Gupta, S.; Johnson, C.L.; Giantsidis, J.; Papademetris, M. Methodology for Safe and Secure AI in Diabetes Management. J. Diabetes Sci. Technol. 2025, 19, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Gundlack, J.; Negash, S.; Thiel, C.; Buch, C.; Schildmann, J.; Unverzagt, S.; Mikolajczyk, R.; Frese, T.; PEAK Consortium. Artificial Intelligence in Medical Care—Patients’ Perceptions on Caregiving Relationships and Ethics: A Qualitative Study. Health Expect. 2025, 28, e70216. [Google Scholar] [CrossRef] [PubMed]
- Gundlack, J.; Thiel, C.; Negash, S.; Buch, C.; Apfelbacher, T.; Denny, K.; Christoph, J.; Mikolajczyk, R.; Unverzagt, S.; Frese, T. Patients’ Perceptions of Artificial Intelligence Acceptance, Challenges, and Use in Medical Care: Qualitative Study. J. Med. Internet Res. 2025, 27, e70487. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, K.; Okhai, R.; Neely, S.R. Public Perceptions of Artificial Intelligence in Healthcare: Ethical Concerns and Opportunities for Patient-Centered Care. BMC Med. Ethics 2024, 25, 74. [Google Scholar] [CrossRef]
- Alsaleh, A. The Impact of Technological Advancement on Culture and Society. Sci. Rep. 2024, 14, 32140. [Google Scholar] [CrossRef]
- Fatoum, H.; Hanna, S.; Halamka, J.D.; Sicker, D.C.; Spangenberg, P.; Hashmi, S.K. Blockchain Integration With Digital Technology and the Future of Health Care Ecosystems: Systematic Review. J. Med. Internet Res. 2021, 23, e19846. [Google Scholar] [CrossRef]
- Xie, Y.; Zhai, Y.; Lu, G. Evolution of Artificial Intelligence in Healthcare: A 30-Year Bibliometric Study. Front. Med. 2025, 11, 1505692. [Google Scholar] [CrossRef]
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Studies involving healthcare professionals (principally doctors, nurses, specialists, technicians) who manage diabetes with AI. | Studies that do not involve healthcare workers. |
| Concept | Studies exploring the adoption and implementation of AI in managing diabetes, such as monitoring systems, diagnostics, predictive therapy, and personalized patient management. AI technologies extended in ML or DL use. | Studies that address AI in non-healthcare contexts or those unrelated to managing diabetes; technological interventions that do not use AI, ML or DL. |
| Context | Barriers and obstacles perceived from healthcare workers in adopting AI (e.g., technological difficulties, cultural challenges, insufficient training, resistance to change). Facilitators and enabling factors from healthcare workers in terms of AI adoption (e.g., organizational support, training, technology accessibility, evidence of effectiveness). | Studies that do not explore barriers or facilitators in AI adoption by healthcare workers; research that only addresses clinical outcomes of diabetes treatment without focusing on perception, implementation science, and attitude. |
| Study | Checklist | Overall Quality |
|---|---|---|
| Held et al., 2022 [51] | JBI for qualitative studies | Medium |
| Liao et al., 2024 [52] | JBI for qualitative studies | Excellent |
| Petersen et al., 2024 [53] | JBI for qualitative studies | High |
| Romero et al., 2019 [55] | MMAT | High |
| Roy et al., 2024 [54] | JBI for analytical cross-sectional studies | Low |
| Wahlich et al., 2024 [57] | JBI for qualitative studies | Medium |
| Wewetzer et al., 2023 [56] | JBI for analytical cross-sectional studies | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cangelosi, G.; Conti, A.; Caggianelli, G.; Panella, M.; Petrelli, F.; Mancin, S.; Ratti, M.; Masini, A. Barriers and Facilitators to Artificial Intelligence Implementation in Diabetes Management from Healthcare Workers’ Perspective: A Scoping Review. Medicina 2025, 61, 1403. https://doi.org/10.3390/medicina61081403
Cangelosi G, Conti A, Caggianelli G, Panella M, Petrelli F, Mancin S, Ratti M, Masini A. Barriers and Facilitators to Artificial Intelligence Implementation in Diabetes Management from Healthcare Workers’ Perspective: A Scoping Review. Medicina. 2025; 61(8):1403. https://doi.org/10.3390/medicina61081403
Chicago/Turabian StyleCangelosi, Giovanni, Andrea Conti, Gabriele Caggianelli, Massimiliano Panella, Fabio Petrelli, Stefano Mancin, Matteo Ratti, and Alice Masini. 2025. "Barriers and Facilitators to Artificial Intelligence Implementation in Diabetes Management from Healthcare Workers’ Perspective: A Scoping Review" Medicina 61, no. 8: 1403. https://doi.org/10.3390/medicina61081403
APA StyleCangelosi, G., Conti, A., Caggianelli, G., Panella, M., Petrelli, F., Mancin, S., Ratti, M., & Masini, A. (2025). Barriers and Facilitators to Artificial Intelligence Implementation in Diabetes Management from Healthcare Workers’ Perspective: A Scoping Review. Medicina, 61(8), 1403. https://doi.org/10.3390/medicina61081403