

Using Artificial Neural Network Models (ANNs) to Identify Patients with Idiopathic Normal Pressure Hydrocephalus (INPH) and Alzheimer Dementia (AD): Clinical Psychological Features and Differential Diagnosis

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
- -
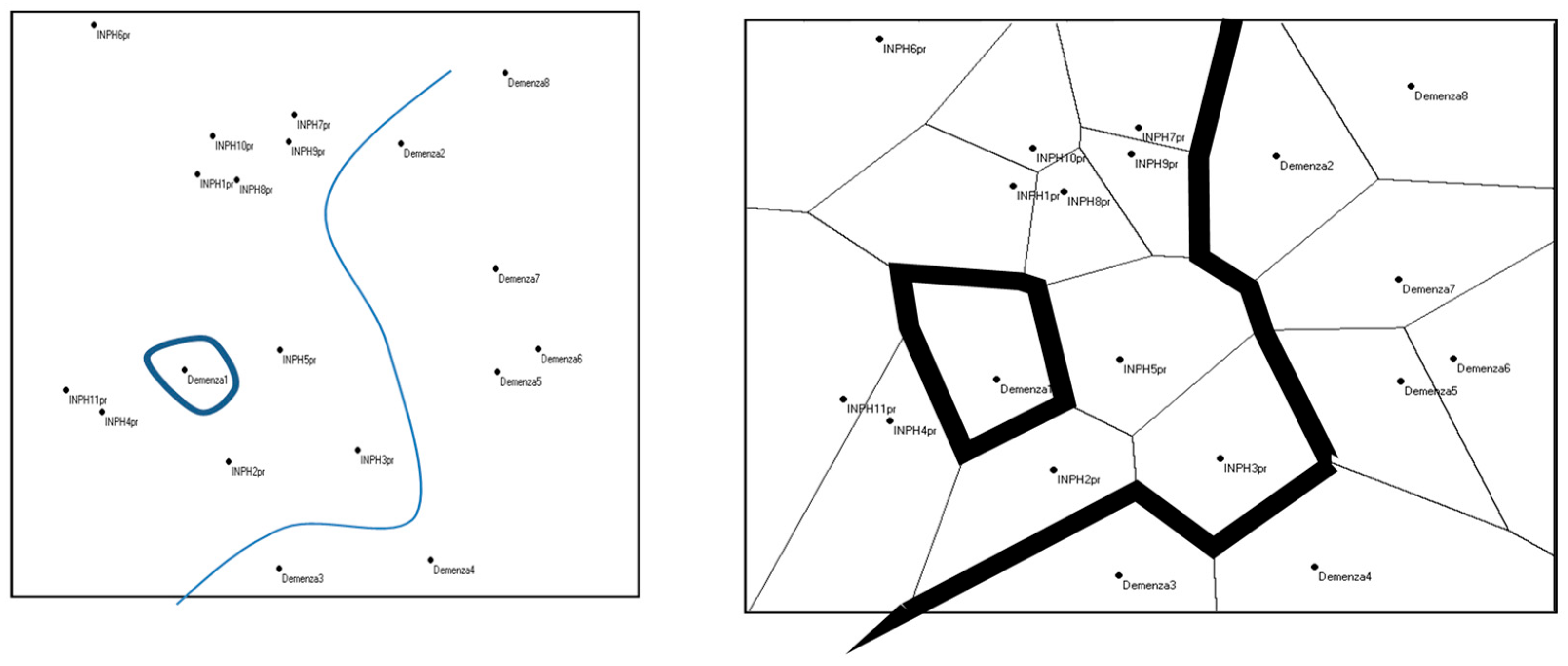
- Populations: This is a Multi-Dimensional Scaling algorithm that projects the observed individuals on a bi-dimensional plane with coordinates X and Y [51];
- -
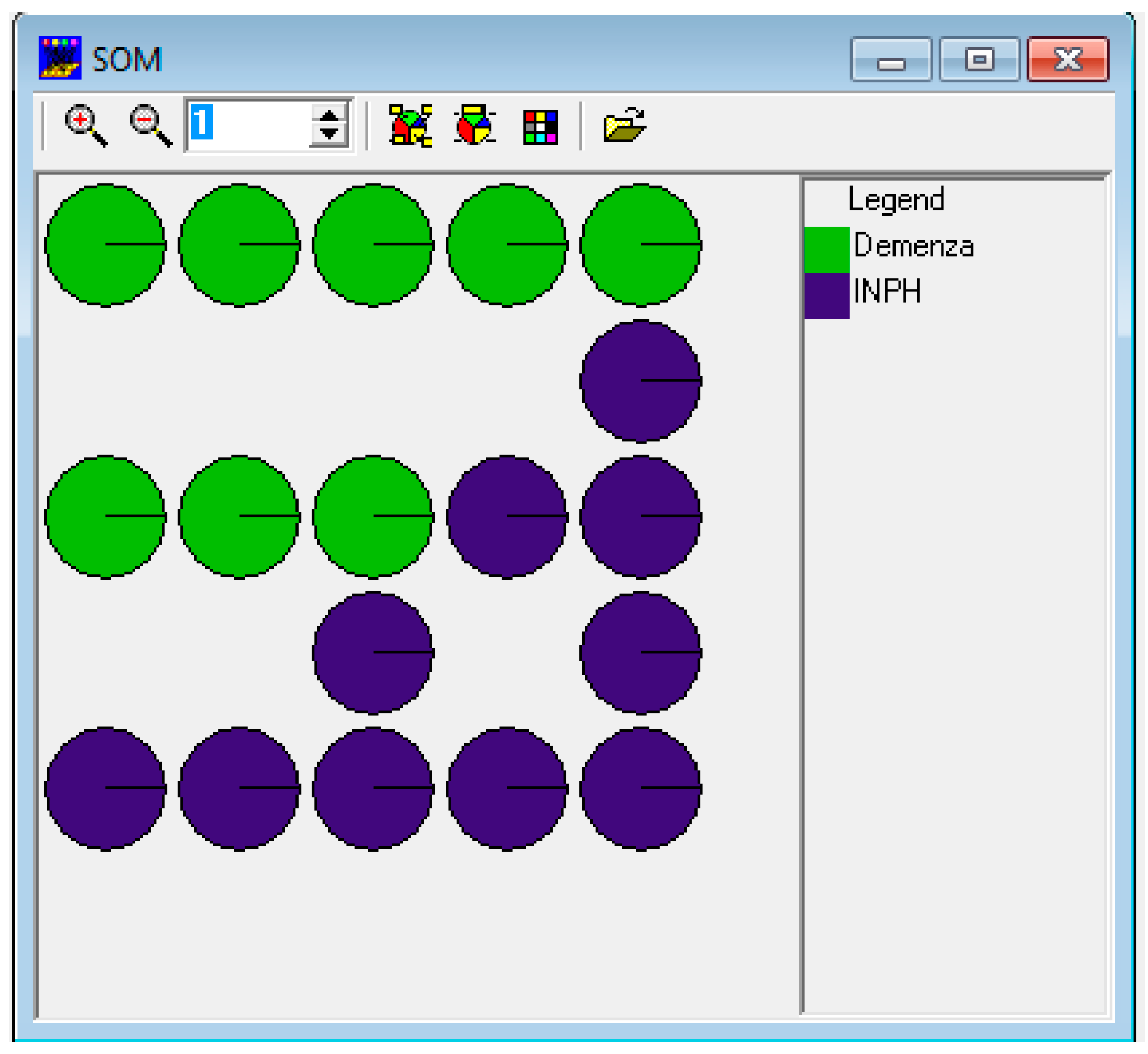
- Self-Organizing Map (SOM): This is an example of an unsupervised neural network, clustering the observed individuals and focusing on input variables on a bi-dimensional matrix [52];
- -
3. Results
3.1. Results with Populations
3.2. Results with SOM Algorithm
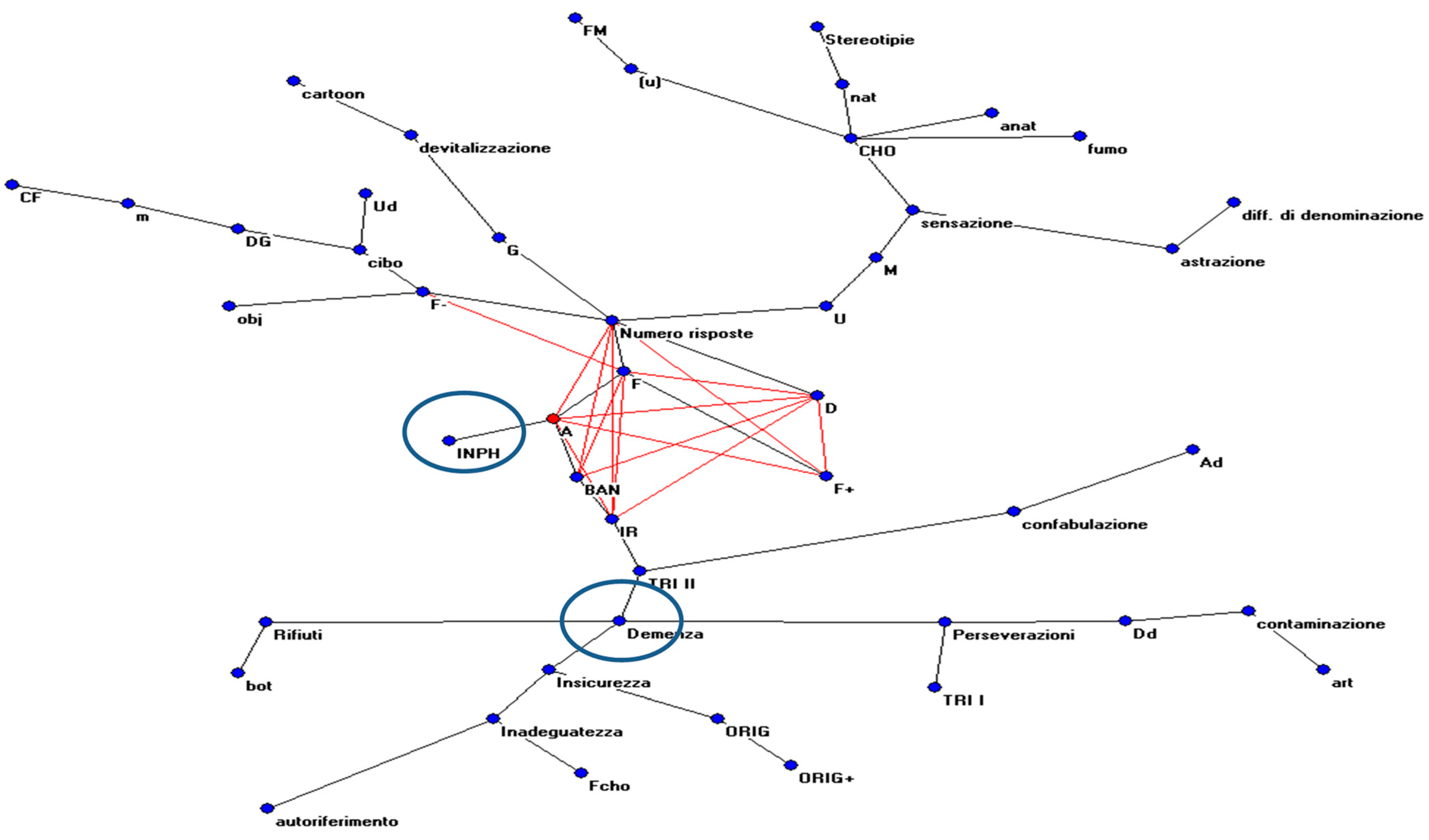
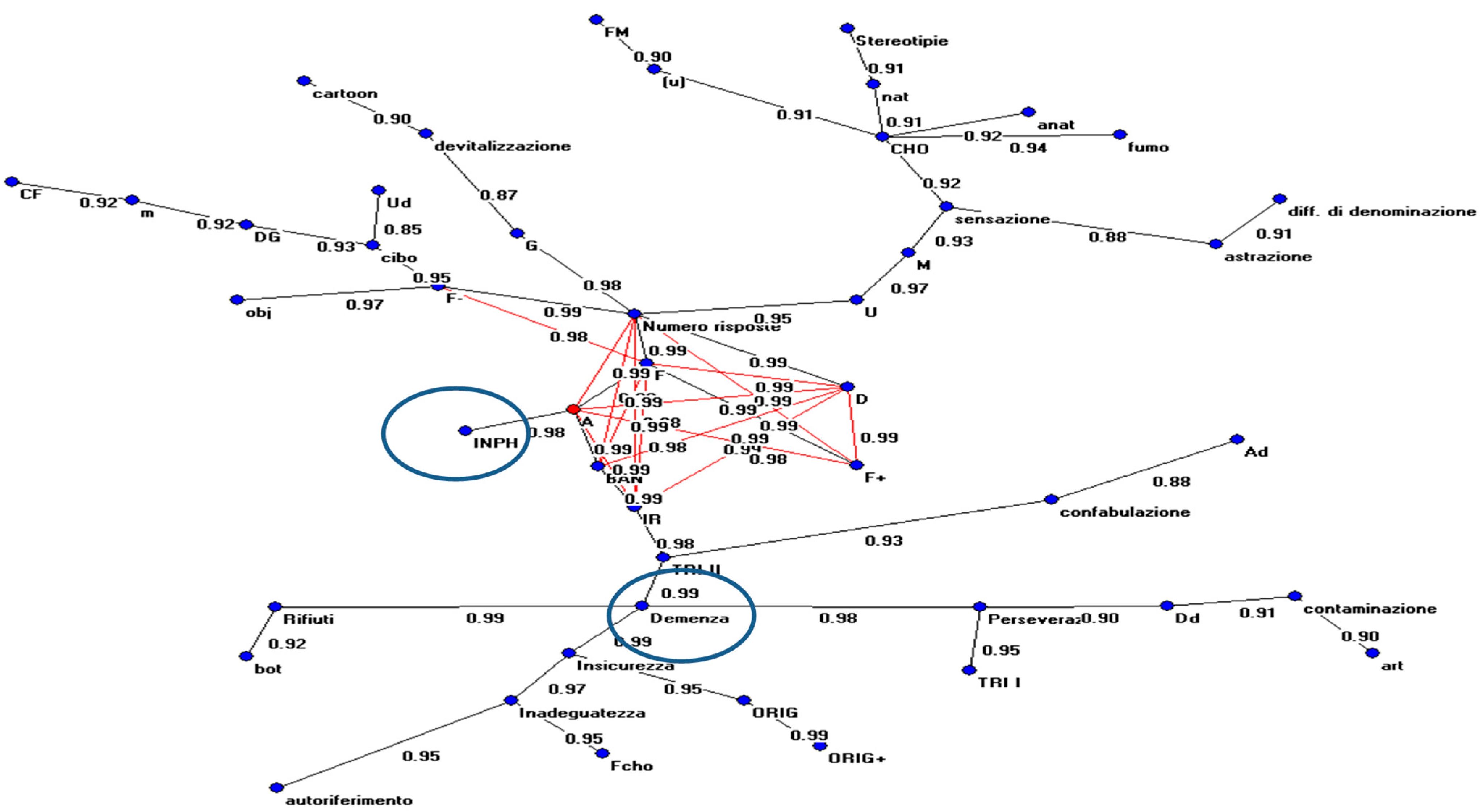
3.3. Results with AutoCM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Notes About the Methodology Used
Appendix A.1. Analysis Through Populations
Appendix A.2. Analysis Through the SOM
- It performs the classification of the input vectors on the basis of their vector similarity and assigns them to a class.
- It creates a prototypical model of the classes with the same cardinality (number of variables) as the input vector.
- It provides a measurement, expressed as a numerical value, of the distance/proximity of the various classes.
- It creates a relational map of the various classes, placing each class on the map itself.
- It provides a measurement of the distance/proximity that exists between the input vectors from the class they belong to and between the input vectors and other classes.
Appendix A.3. Analysis Through AutoCM
References
- Xiao, H.; Hu, F.; Ding, J.; Ye, Z. Cognitive impairment in idiopathic normal pressure hydrocephalus. Neurosci. Bull. 2022, 38, 1085–1096. [Google Scholar] [CrossRef] [PubMed]
- Fife, T.D. Clinical features of normal pressure hydrocephalus. Barrow Q. 2003, 19, 10–15. [Google Scholar]
- Clarfield, A.M. The reversible dementias: Do they reverse? Ann. Intern. Med. 1988, 109, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Klinge, P.; Marmarou, A.; Bergsneider, M.; Relkin, N.; Black, P.M. Outcome of shunting in idiopathic normal-pressure hydrocephalus and the value of outcome assessment in shunted patients. Neurosurgery 2005, 57, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Duinkerke, A.; Williams, M.A.; Rigamonti, D.; Hillis, A.E. Cognitive recovery in idiopathic normal pressure hydrocephalus after shunt. Cogn. Behav. Neurol. 2004, 17, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; McGirt, M.J.; Woodworth, G.; Heidler, J.; Rigamonti, D.; Hillis, A.E.; Williams, M.A. Baseline neuropsychological profile and cognitive response to cerebrospinal fluid shunting for idiopathic normal pressure hydrocephalus. Dement. Geriatr. Cogn. Disord. 2005, 20, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Sindorio, C.; Abbritti, R.V.; Raffa, G.; Priola, S.M.; Germanò, A.; Visocchi, M.; Quattropani, M.C. Neuropsychological Assessment in the Differential Diagnosis of Idiopathic Normal Pressure Hydrocephalus. An Important Tool for the Maintenance and Restoration of Neuronal and Neuropsychological Functions. Acta. Neurochir. Suppl. 2017, 124, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Holodny, A.I.; Waxman, R.; George, A.E.; Rusinek, H.; Kalnin, A.J.; Leon, M.d. MR differential diagnosis of normal-pressure hydrocephalus and Alzheimer disease: Significance of perihippocampal fissures. Am. J. Neuroradiol. 1998, 19, 813–819. [Google Scholar] [PubMed] [PubMed Central]
- Laurent, M.S. Normal pressure hydrocephalus in geriatric medicine: A challenge. J. Geriatr. Psychiatry Neurol. 1988, 1, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Gallia, G.L.; Rigamonti, D.; Williams, M.A. The diagnosis and treatment of idiopathic normal pressure hydrocephalus. Nat. Clin. Pr. Neurol. 2006, 2, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Siraj, S. An overview of normal pressure hydrocephalus and its importance: How much do we really know? J. Am. Med. Dir. Assoc. 2011, 12, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Shprecher, D.; Schwalb, J.; Kurlan, R. Normal Pressure Hydrocephalus: Diagnosis and Treatment. Curr. Neurol. Neurosci. Rep. 2008, 8, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Grossman, H.; Bergmann, C.; Parker, S. Dementia: A brief review. Mt. Sinai. J. Med. 2006, 73, 985–992. [Google Scholar] [PubMed]
- Kiefer, M.; Unterberg, A. The differential diagnosis and treatment of normal-pressure hydrocephalus. Dtsch. Arztebl. Int. 2012, 109, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, R.V.; Nanda, A. Implanted ventricular shunts in the United States: The billion-dollar-a-year cost of hydrocephalus treatment. Neurosurgery 2005, 56, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Vacca, V. Diagnosis and Treatment of Idiopathic Normal Pressure Hydrocephalus. J. Neurosci. Nurs. 2007, 39, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Factora, R.; Luciano, M. Normal pressure hydrocephalus: Diagnosis and new approaches to treatment. Clin. Geriatr. Med. 2006, 22, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Marmarou, A.; Bergsneider, M.; Klinge, P.; Relkin, N.; Black, P.M. The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery 2005, 57, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Krauss, J.K.; Halve, B. Normal pressure hydrocephalus: Survey on contemporary diagnostic algorithms and therapeutic decision-making in clinical practice. Acta. Neurochir. 2004, 146, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Di Ieva, A.; Valli, M.; Cusimano, M.D. Distinguishing Alzheimer’s disease from normal pressure hydrocephalus: A search for MRI biomarkers. J. Alzheimers. Dis. 2014, 38, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Pickard, J.D.; Spiegelhalter, D.; Czosnyka, M. Health economics and the search for shunt-responsive symptomatic hydrocephalus in the elderly. J. Neurosurg. 2006, 105, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Sharkey, P.; van Doren, D.; Thomas, G.; Rigamonti, D. Influence of shunt surgery on healthcare expenditures of elderly fee-for-service Medicare beneficiaries with hydrocephalus. J. Neurosurg. 2007, 107, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Kazui, H.; Mori, E.; Hashimoto, M.; Ishikawa, M.; Hirono, N.; Takeda, M. Effect of Shunt Operation on Idiopathic Normal Pressure Hydrocephalus Patients in Reducing Caregiver Burden: Evidence from Sinphoni. Dement. Geriatr. Cogn. Disord 2011, 31, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Barison, F.; Tognazzo, D.P. Il Rorschach Fenomenologico; Franco Angeli: Milano, Italy, 1982. [Google Scholar]
- Mihura, J.L.; Jowers, C.E.; Dumitrascu, N.; van den Hurk, A.W.V.; Keddy, P.J. The specific uses of the Rorschach in clinical practice. Rorschachiana 2022, 43, 14–35. [Google Scholar] [CrossRef]
- Tognazzo, D.P. Il Metodo Rorschach; Giunti: Firenze, Italy, 1994. [Google Scholar]
- Acklin, M.W. Some contributions of cognitive science to the Rorschach test. Rorschachiana 1994, 19, 129–145. [Google Scholar] [CrossRef]
- Weiner, I.B. Using the Rorschach properly in practice and research. J. Clin. Psychol. 2000, 56, 435–438, discussion 441–448. [Google Scholar] [CrossRef]
- Smith, S.R.; Bistis, K.; Zahka, N.E.; Blais, M.A. Perceptual-organizational characteristics of the Rorschach task. Clin. Neuropsychol. 2007, 21, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Schott, G.D. Revisiting the Rorschach inkblots: From iconography and psychology to neuroscience. J. Neurol. Neurosurg. Psychiatry 2014, 85, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Insùa, A.M.; Loza, S.M. Psychometric patterns of the Rorschach of healthy elderly persons and patients with suspected dementia. Percept. Mot. Ski. 1986, 63, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Perry, W.; Potterat, E.; Auslander, L.; Kaplan, E.; Jeste, D. A Neuropsychological approach to the Rorschach in patients with Dementia of the Alzheimer Type. Assessment 1996, 3, 351–363. [Google Scholar] [CrossRef]
- Makoto, S.; Nishio, Y.; Kanno, S.; Uchiyama, M.; Hayashi, A.; Takagi, M.; Kikuchi, H.; Yamasaki, H.; Shimomura, T.; Iizuka, O.; et al. Cognitive profile of Idiopathic Normal pressure Hydrocephalus. Extra Dement. Geriatr. Cogn. Disord. 2011, 1, 202–211. [Google Scholar] [CrossRef]
- Sànchez, H.S. Rorschach y la psicobiología de la personalidad. Univ. Psychol. 2016, 15, 15–39. [Google Scholar] [CrossRef]
- Cockrell, J.R.; Folstein, M.F. Mini-mental state examination. In Principles and Practice of Geriatric Psychiatry, 2nd ed.; Sadavoy, J., Lazarus, L.W., Jarvik, L.F., Eds.; John Wiley & Sons: Chichester, UK, 2002; pp. 140–141. [Google Scholar] [CrossRef]
- Rorschach, H. Psychodiagnostics: A Diagnostic Test Based on Perception; Reading Read Books: Virginia Beach, VA, USA, 2011. [Google Scholar]
- Schachtel, E.G. Experiential Foundations of Rorschach’s Test; Analytic Press: Hillsdale, NJ, USA, 2001. [Google Scholar]
- Groth-Marnat, G. Handbook of Psychological Assessment; John Wiley & Sons: New York, NY, USA, 2003. [Google Scholar]
- Pelto, J.; Pelto, G.H. Anthropological Research: The Structure of Inquiry; Cambridge University Press: Cambridge, UK, 1996. [Google Scholar]
- Malmgren, H. Rorschach’s idea of a “movement” response in the light of recent philosophy and psychology of perception. Rorschachiana 2000, 24, 1–27. [Google Scholar] [CrossRef]
- Kron, A.; Cohen, A.; Benziman, H.; Ben-Shakha, G. What is it that color determinants determine? The relation between the Rorschach inkblot method and cognitive object-recognition processes. J. Pers. Assess. 2009, 91, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Giromini, L.; Porcelli, P.; Viglione, D.J.; Parolin, L.; Pineda, J.A. The feeling of movement: EEG evidence for mirroring activity during the observations of static, ambiguous stimuli in the Rorschach cards. Biol. Psychol. 2010, 85, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Malone, J.C.; Stein, M.B.; Slavin-Mulford, J.; Bello, I.; Sinclair, S.J.; Blais, M.A. Seeing red: Affect modulation and chromatic color responses on the Rorschach. Bull. Menninger. Clin. 2013, 77, 70–93. [Google Scholar] [CrossRef] [PubMed]
- Insùa, A.M.; Loza, S.M. Evaluation of Piotrowsky’s organic signs in the Rorschach test of patients with an early stage of dementia. Acta. Psiquiatr. Psicol. Am. Lat. 1988, 34, 243–250. [Google Scholar] [PubMed]
- Zillmer, E.A.; Perry, W. Cognitive-neuropsychological abilities and related psychological disturbance: A factor model of Neuropsychological, Rorschach and MMPI indices. Psychol. Assess 1996, 3, 209–224. [Google Scholar] [CrossRef]
- Piotrowski, C. The Rorschach in research on neurocognitive dysfunction: An historical overview, 1936–2016. SIS J. Proj. Psychol. Ment. Health. 2018, 25, 44–53. [Google Scholar]
- Acklin, M.W.; Decato, C.M. Piotrowski’s enduring contributions to the Rorschach: A review of Perceptanalysis. J. Personal. Assess Dec. 1993, 61, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Acklin, M.W.; Wu-Holt, P. Contributions of cognitive science to the Rorschach Technique: Cognitive and neuropsychological correlates of the response process. J. Pers. Assess. 1996, 67, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Kimoto, A.; Iseki, E.; Ota, K.; Murayama, N.; Sato, K.; Ogura, N.; Arai, H. Differences in responses to the Rorschach test between patients with dementia with Lewy bodies and Alzheimer’s disease from the perspective of visuoperceptual impairment. Psychiatry Res. 2017, 257, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Massini, G.; Terzi, S.; Buscema, P.M. Population Algorithm: A New Method of Multi-Dimensional Scaling. In Data Mining Applications Using Artificial Adaptive Systems; Tastle, W.J., Ed.; Springer Science+Business Media: New York, NY, USA, 2013; Chapter 3; pp. 63–74. [Google Scholar] [CrossRef]
- Kohonen, T. Self-Organizing Maps. Series in Information Sciences; Springer: Heidelberg, Germany, 1995; Volume 30. [Google Scholar]
- Buscema, P.M. A general presentation of Artificial Neural Networks in Substance Use & Misuse. Int. J. Addict. 1997, 32, 97–112. [Google Scholar]
- Buscema, P.M.; Massini, G.; Breda, M.; Lodwick, W.A.; Newman, F.; Asadi-Zeydabadi, M. Artificial Adaptive Systems Using Auto Contractive Maps: Theory, Applications and Extensions; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Buscema, P.M.; Lodwick, W.A.; Massini, G.; Sacco, P.L.; Asadi-Zeydabadi, M.; Newman, F.; Petritoli, R.; Marco Breda, M. AI: A Broad and a Different Perspective; Springer Briefs in Applied Sciences and Technology. Computational Intelligence; Springer: Cham, Switzerland, 2025. [Google Scholar] [CrossRef]
- Ogata, Y.; Ozaki, A.; Ota, M.; Oka, Y.; Nishida, N.; Tabu, H.; Sato, N.; Hanakawa, T. Interhemispheric resting-state functional connectivity predicts severity of idiopathic normal pressure hydrocephalus. Front. Neurosci. 2017, 11, 470. [Google Scholar] [CrossRef] [PubMed]
- Singh, A. An artificial bee colony algorithm for the leaf-constrained minimum spanning tree problem. Appl. Soft Comput. 2009, 9, 625–631. [Google Scholar] [CrossRef]
- Graham, R.L.; Hell, P. On the history of the minimum spanning tree problem. Ann. Hist. Comput. 1985, 7, 43–57. [Google Scholar] [CrossRef]
- Grygorash, O.; Zhou, Y.; Jorgensen, Z. Minimum spanning tree based clustering algorithms. In Proceedings of the 2006 18th IEEE International Conference on Tools with Artificial Intelligence (ICTAI’06), Arlington, VA, USA, 13–15 November 2006; IEEE: New York, NY, USA, 2006; pp. 73–81. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|
| Age | 76.11 | 7.32 | 59 | 88 |
| Age > 75 | 0.58 | 0.51 | 0 | 1 |
| Gender (1 = female; 0 = male) | 0.58 | 0.51 | 0 | 1 |
| Compulsory education | 0.63 | 0.50 | 0 | 1 |
| Married (1 = yes; 0 = no) | 0.89 | 0.32 | 0 | 1 |
| Number of answers | 10.32 | 3.83 | 4 | 18 |
| MMSE total score | 17.89 | 5.15 | 8 | 27 |
| Localization: | ||||
| Global (G) | 5.42 | 2.81 | 1 | 13 |
| Details (D) | 4.58 | 3.06 | 0 | 10 |
| Little details (Dd) | 0.11 | 0.32 | 0 | 1 |
| Details → global (DG) | 0.21 | 0.71 | 0 | 1 |
| Determinants: | ||||
| F (shape) | 8.53 | 4.14 | 2 | 16 |
| F+ (positive shape) | 5.63 | 3.20 | 1 | 12 |
| F− (negative shape) | 2.89 | 2.21 | 0 | 8 |
| M (Human kinesthetic activity) | 0.74 | 0.73 | 0 | 3 |
| FM (Animal kinesthetic activity) | 0.74 | 1.24 | 0 | 4 |
| m (inanimate movement) | 0.05 | 0.23 | 0 | 1 |
| CF (color and shame) | 0.05 | 0.23 | 0 | 1 |
| FCho (diffuse shading) | 0.11 | 0.32 | 0 | 1 |
| Cho (pure shading) | 0.05 | 0.23 | 0 | 1 |
| Contents: | ||||
| A (animals) | 5.84 | 2.59 | 0 | 10 |
| Ad (animal details) | 0.47 | 1.02 | 0 | 4 |
| H (human) | 1.26 | 1.48 | 0 | 5 |
| (h) (fantastic human) | 0.11 | 0.32 | 0 | 1 |
| Hd human details | 0.37 | 0.83 | 0 | 3 |
| Obj object | 0.95 | 1.31 | 0 | 4 |
| Cibo food | 0.16 | 0.37 | 0 | 1 |
| Nat nature | 0.11 | 0.32 | 0 | 1 |
| Botanic | 0.58 | 0.96 | 0 | 3 |
| Anatomical | 0.32 | 0.75 | 0 | 3 |
| Smoke | 0.05 | 0.23 | 0 | 1 |
| Cartoon | 0.11 | 0.32 | 0 | 1 |
| Art | 0.11 | 0.32 | 0 | 1 |
| Popular | 2.21 | 1.17 | 0 | 4 |
| Original | 0.11 | 0.32 | 0 | 1 |
| TRI I (Erleibniss typus I) | 1.74 | 0.99 | 1 | 3 |
| TRI II (Erleibniss typus II) | 2.16 | 0.96 | 1 | 3 |
| IR (reality index) | 3.58 | 1.80 | 0 | 6 |
| Particular phenomena | ||||
| Perseveration | 0.37 | 0.50 | 0 | 1 |
| Inadequacy | 0.21 | 0.42 | 0 | 1 |
| Insecurity | 0.26 | 0.45 | 0 | 1 |
| Stereotyped | 0.05 | 0.23 | 0 | 1 |
| Refuse | 0.63 | 0.50 | 0 | 1 |
| Confabulation | 0.21 | 0.42 | 0 | 1 |
| Abstraction | 0.05 | 0.23 | 0 | 1 |
| Contamination | 0.05 | 0.23 | 0 | 1 |
| Difficulty of naming | 0.05 | 0.23 | 0 | 1 |
| Self-reference | 0.11 | 0.32 | 0 | 1 |
| Devitalization | 0.11 | 0.32 | 0 | 1 |
| Sensation | 0.11 | 0.32 | 0 | 1 |
| Caso | Numero Risposte | G | D | Dd | DG | F | F+ | F− | M | FM | m | CF | Fcho | CHO | BAN | ORIG | ORIG+ | A | Ad | U | (u) | Ud | Obj | Cibo | Nat | Bot | Anat | Fumo | Cartoon | Art | IR | TRI I | TRI II | Perseverazioni | Inadeguatezza | Insicurezza | Stereotipie | Rifiuti | Confabulazione | Astrazione | Contaminazione | Diff. Denominazione | Autoriferimento | Devitalizzazione | Sensazione |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Demenza 1 | 8 | 8 | 0 | 0 | 0 | 8 | 5 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 3 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 2 | 7 | 2 | 5 | 0 | 0 | 5 | 1 | 4 | 1 | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 5 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 4 | 1 | 3 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 3 | 10 | 4 | 3 | 0 | 3 | 8 | 3 | 5 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 | 0 | 0 | 0 | 2 | 4 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 2 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 4 | 15 | 7 | 8 | 0 | 0 | 14 | 12 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 4 | 1 | 1 | 9 | 0 | 3 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 5 | 1 | 3 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 5 | 9 | 1 | 7 | 1 | 0 | 9 | 7 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 5 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 3 | 3 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 6 | 13 | 3 | 9 | 0 | 1 | 11 | 8 | 3 | 1 | 0 | 0 | 0 | 1 | 0 | 3 | 1 | 1 | 7 | 1 | 2 | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 0 | 0 | 4 | 1 | 2 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Demenza 7 | 8 | 2 | 6 | 0 | 0 | 7 | 7 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 3 | 0 | 2 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 1 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Demenza 8 | 7 | 5 | 2 | 0 | 0 | 4 | 2 | 2 | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 1 | 3 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 |
| INPH 1 pr | 10 | 7 | 3 | 0 | 0 | 6 | 5 | 1 | 0 | 4 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 9 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 2 pr | 13 | 5 | 8 | 0 | 0 | 13 | 7 | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 7 | 4 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 6 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 3 pr | 13 | 6 | 7 | 0 | 0 | 13 | 10 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 5 | 3 | 3 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 4 pr | 16 | 13 | 3 | 0 | 0 | 15 | 7 | 8 | 1 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 6 | 1 | 2 | 0 | 1 | 3 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 6 | 1 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| INPH 5 pr | 7 | 7 | 0 | 0 | 0 | 7 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 3 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 6 pr | 12 | 7 | 5 | 0 | 0 | 7 | 3 | 4 | 1 | 3 | 0 | 0 | 0 | 1 | 3 | 0 | 0 | 6 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 3 | 1 | 0 | 0 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| INPH 7 pr | 4 | 3 | 1 | 0 | 0 | 2 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 8 pr | 11 | 6 | 5 | 0 | 0 | 8 | 4 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 9 pr | 4 | 3 | 1 | 0 | 0 | 2 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 10 pr | 11 | 7 | 4 | 0 | 0 | 7 | 4 | 3 | 1 | 3 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 7 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| INPH 11 pr | 18 | 7 | 10 | 1 | 0 | 16 | 11 | 5 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 9 | 0 | 4 | 1 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Caso | Numero Risposte | G | D | Dd | DG | F | F+ | F− | M | FM | m | CF | Fcho | CHO | BAN | ORIG | ORIG+ | A | Ad | U | (u) | Ud | Obj | Cibo | Nat | Bot | Anat | Fumo | Cartoon | Art | IR | TRI I | TRI II | Perseverazioni | Inadeguatezza | Insicurezza | Stereotipie | Rifiuti | Confabulazione | Astrazione | Contaminazione | Diff. Di Denominazione | Autoriferimento | Devitalizzazione | Sensazione |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Demenza 1 | 8 | 8 | 0 | 0 | 0 | 8 | 5 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 3 | 3 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 2 | 7 | 2 | 5 | 0 | 0 | 5 | 1 | 4 | 1 | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 5 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 4 | 1 | 3 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 3 | 10 | 4 | 3 | 0 | 3 | 8 | 3 | 5 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 3 | 0 | 0 | 0 | 2 | 4 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 2 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 4 | 15 | 7 | 8 | 0 | 0 | 14 | 12 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 4 | 1 | 1 | 9 | 0 | 3 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 5 | 1 | 3 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 5 | 9 | 1 | 7 | 1 | 0 | 9 | 7 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 5 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 3 | 3 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Demenza 6 | 13 | 3 | 9 | 0 | 1 | 11 | 8 | 3 | 1 | 0 | 0 | 0 | 1 | 0 | 3 | 1 | 1 | 7 | 1 | 2 | 0 | 0 | 0 | 1 | 0 | 2 | 0 | 0 | 0 | 0 | 4 | 1 | 2 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Demenza 7 | 8 | 2 | 6 | 0 | 0 | 7 | 7 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 3 | 0 | 2 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 1 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| Demenza 8 | 7 | 5 | 2 | 0 | 0 | 4 | 2 | 2 | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 5 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 2 | 1 | 3 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 |
| INPH 1 pr | 10 | 7 | 3 | 0 | 0 | 6 | 5 | 1 | 0 | 4 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 9 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 2 pr | 13 | 5 | 8 | 0 | 0 | 13 | 7 | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 7 | 4 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 6 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 3 pr | 13 | 6 | 7 | 0 | 0 | 13 | 10 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 5 | 3 | 3 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 4 pr | 16 | 13 | 3 | 0 | 0 | 15 | 7 | 8 | 1 | 0 | 0 | 0 | 0 | 0 | 4 | 0 | 0 | 6 | 1 | 2 | 0 | 1 | 3 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 6 | 1 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| INPH 5 pr | 7 | 7 | 0 | 0 | 0 | 7 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 3 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 6 pr | 12 | 7 | 5 | 0 | 0 | 7 | 3 | 4 | 1 | 3 | 0 | 0 | 0 | 1 | 3 | 0 | 0 | 6 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 3 | 1 | 0 | 0 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| INPH 7 pr | 4 | 3 | 1 | 0 | 0 | 2 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | |
| INPH 8 pr | 11 | 6 | 5 | 0 | 0 | 8 | 4 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 9 pr | 4 | 3 | 1 | 0 | 0 | 2 | 2 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 3 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| INPH 10 pr | 11 | 7 | 4 | 0 | 0 | 7 | 4 | 3 | 1 | 3 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 7 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 4 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| INPH 11 pr | 18 | 7 | 10 | 1 | 0 | 16 | 11 | 5 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 9 | 0 | 4 | 1 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gitto, L.; Mento, C.; Massini, G.; Buscema, P.M.; Raffa, G.; Germanò, A.F.; Quattropani, M.C.A. Using Artificial Neural Network Models (ANNs) to Identify Patients with Idiopathic Normal Pressure Hydrocephalus (INPH) and Alzheimer Dementia (AD): Clinical Psychological Features and Differential Diagnosis. Medicina 2025, 61, 1332. https://doi.org/10.3390/medicina61081332
Gitto L, Mento C, Massini G, Buscema PM, Raffa G, Germanò AF, Quattropani MCA. Using Artificial Neural Network Models (ANNs) to Identify Patients with Idiopathic Normal Pressure Hydrocephalus (INPH) and Alzheimer Dementia (AD): Clinical Psychological Features and Differential Diagnosis. Medicina. 2025; 61(8):1332. https://doi.org/10.3390/medicina61081332
Chicago/Turabian StyleGitto, Lara, Carmela Mento, Giulia Massini, Paolo Massimo Buscema, Giovanni Raffa, Antonio Francesco Germanò, and Maria Catena Ausilia Quattropani. 2025. "Using Artificial Neural Network Models (ANNs) to Identify Patients with Idiopathic Normal Pressure Hydrocephalus (INPH) and Alzheimer Dementia (AD): Clinical Psychological Features and Differential Diagnosis" Medicina 61, no. 8: 1332. https://doi.org/10.3390/medicina61081332
APA StyleGitto, L., Mento, C., Massini, G., Buscema, P. M., Raffa, G., Germanò, A. F., & Quattropani, M. C. A. (2025). Using Artificial Neural Network Models (ANNs) to Identify Patients with Idiopathic Normal Pressure Hydrocephalus (INPH) and Alzheimer Dementia (AD): Clinical Psychological Features and Differential Diagnosis. Medicina, 61(8), 1332. https://doi.org/10.3390/medicina61081332